

Phase IIa Clinical Biomarker Trial of Dietary Arginine Restriction and Aspirin in Colorectal Cancer Patients
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
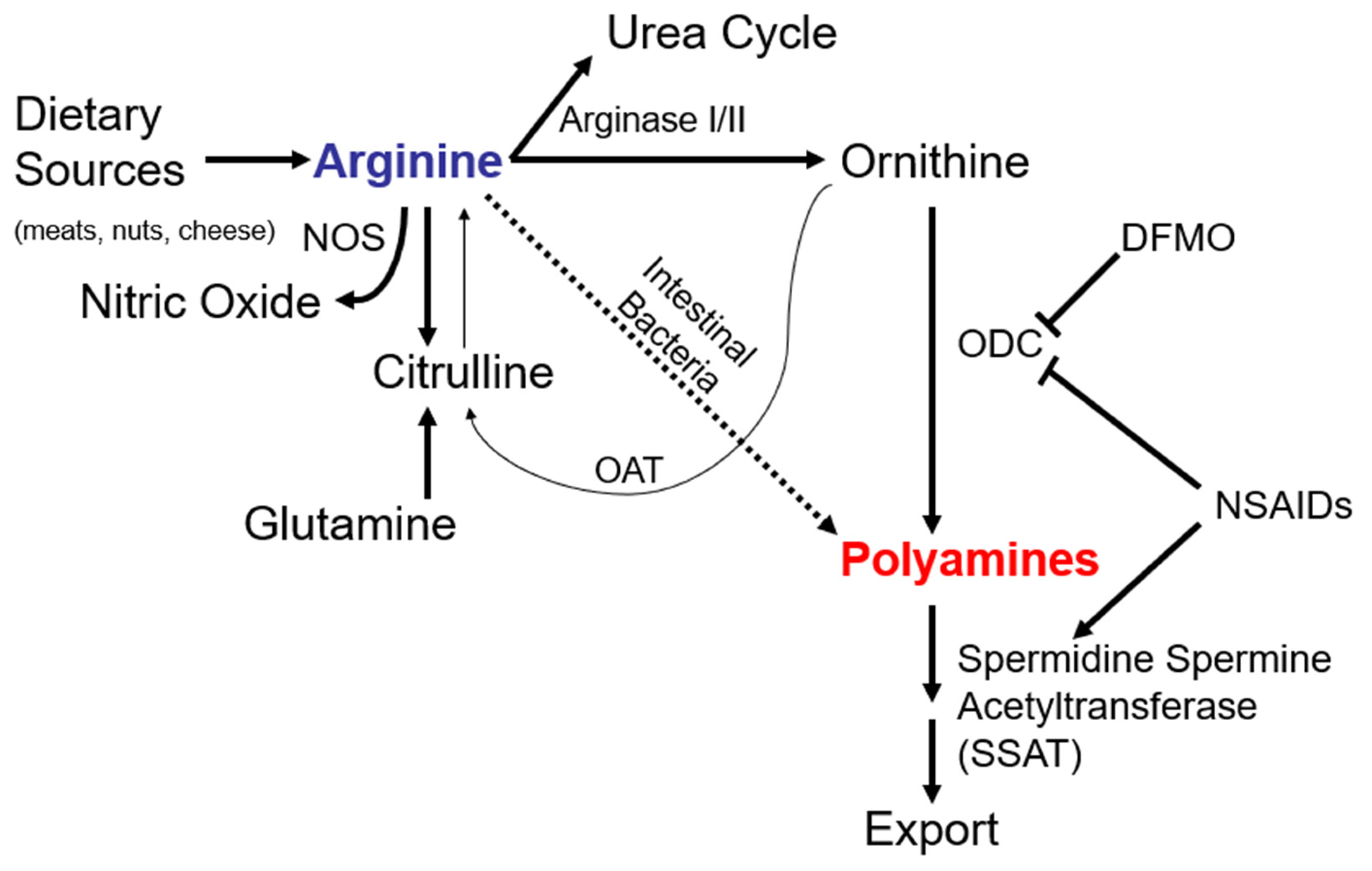
1. Introduction
2. Methods
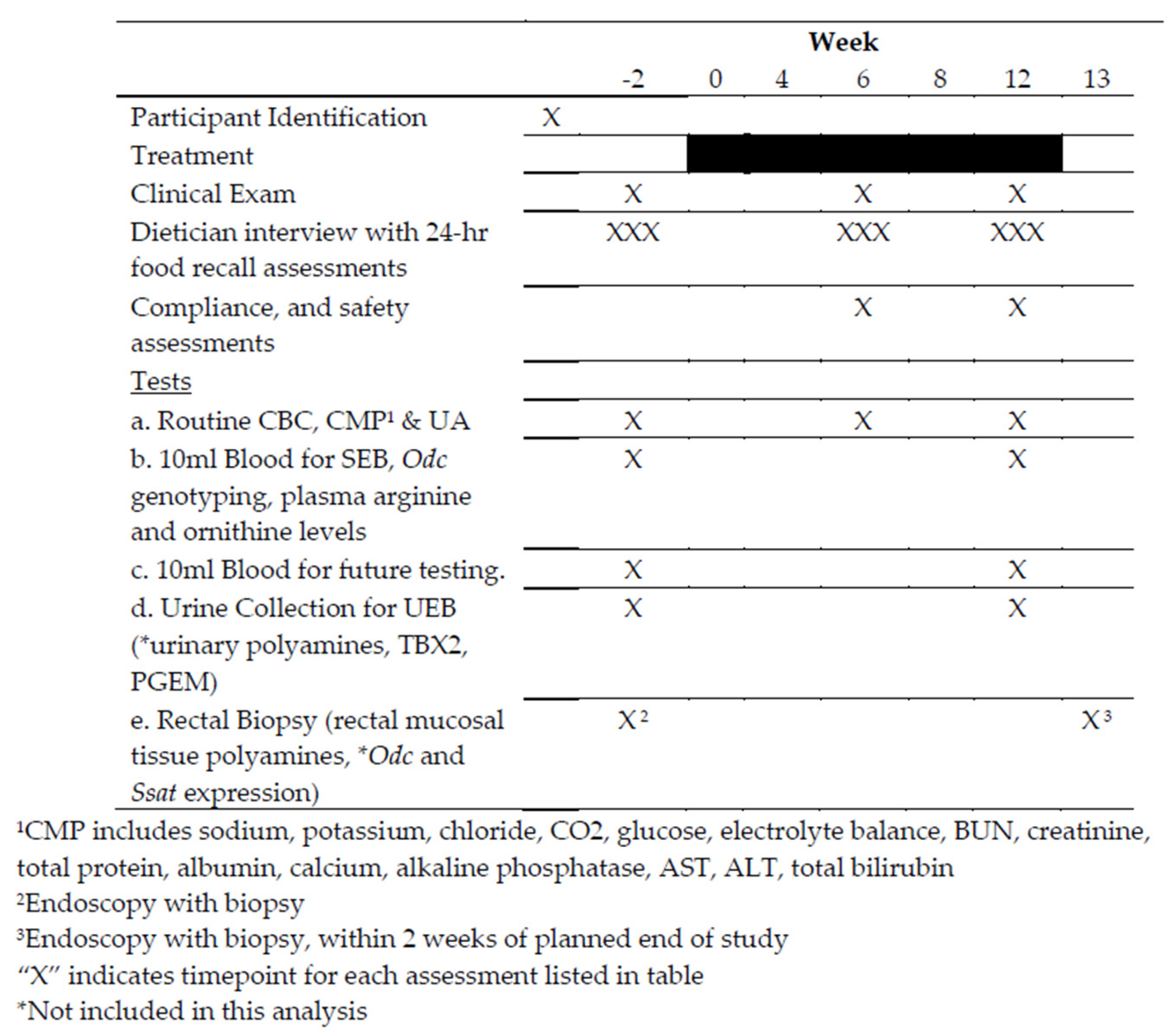
2.1. Study Design
2.2. Eligibility Criteria
2.3. Intervention and On-Study Assessments
2.4. Clinical Evaluation
2.5. Statistical Analyses
2.6. Ethical Considerations & Data Monitoring
3. Results
3.1. Demographics
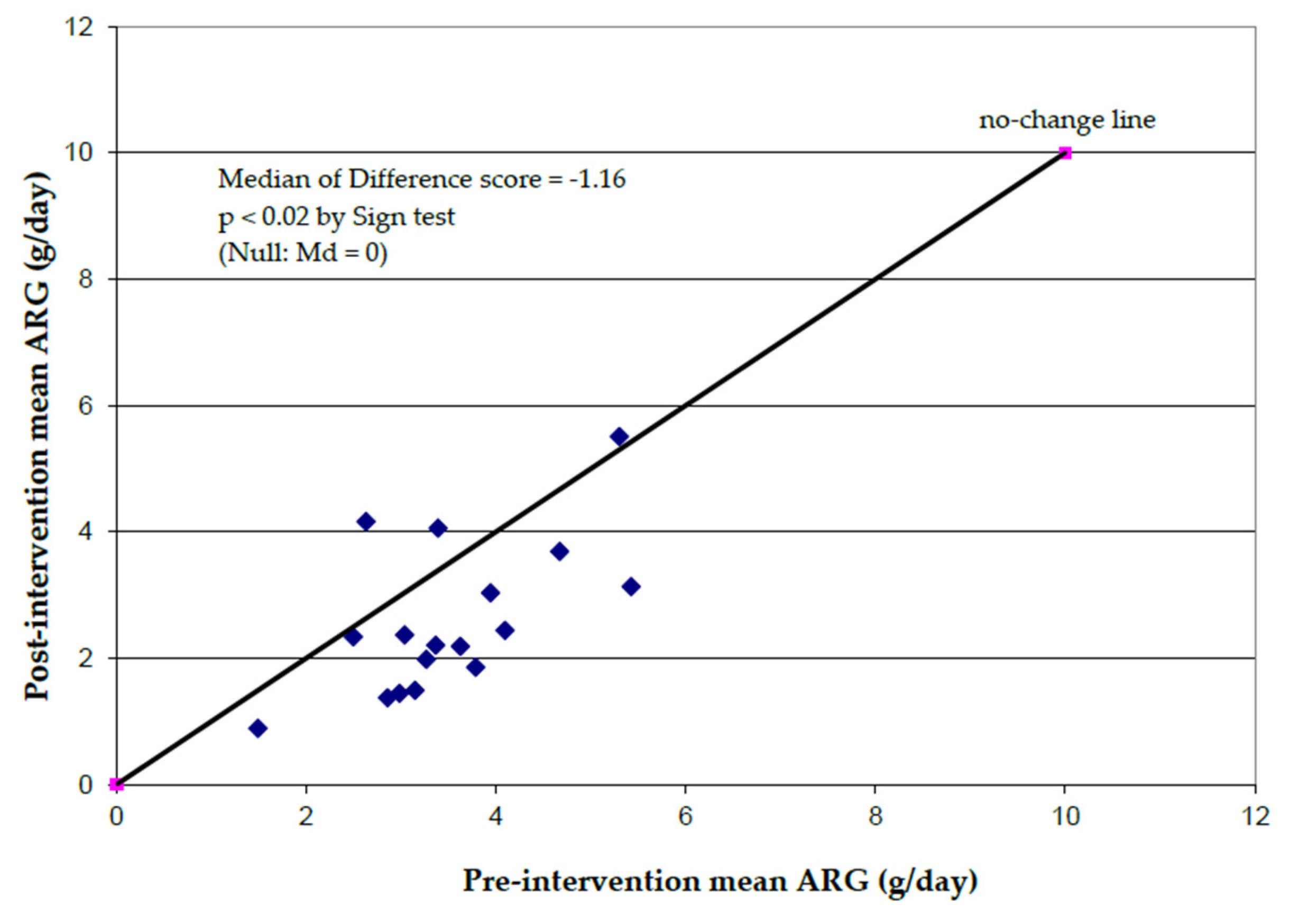
3.2. Dietary Analyses
3.3. Plasma Arginine, Plasma Ornithine Levels
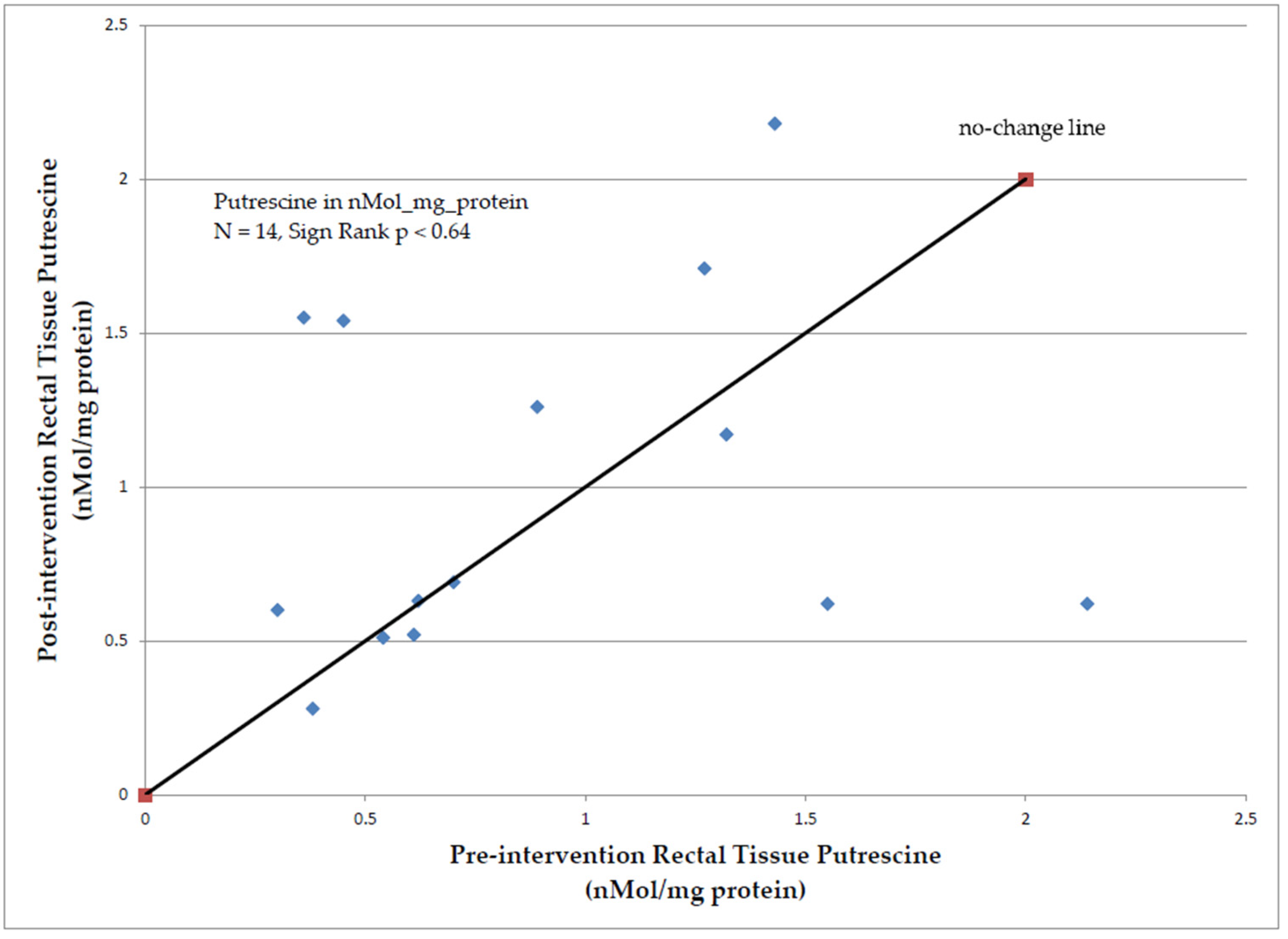
3.4. Rectal Tissue Polyamine Analysis
3.5. Adverse Events
3.6. Quality of Life/Psychosocial Telephone Counseling (PTC) Intervention
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Chu, D.Z.; Chansky, K.; Alberts, D.S.; Meyskens, F.L., Jr.; Fenoglio-Preiser, C.M.; Rivkin, S.E.; Mills, G.M.; Giguere, J.K.; Goodman, G.E.; Abbruzzese, J.L.; et al. Adenoma recurrences after resection of colorectal carcinoma: Results from the Southwest Oncology Group 9041 calcium chemoprevention pilot study. Ann. Surg. Oncol. 2003, 10, 870–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, M.E.; Baron, J.A.; Lieberman, D.A.; Schatzkin, A.; Lanza, E.; Winawer, S.J.; Zauber, A.G.; Jiang, R.; Ahnen, D.J.; Bond, J.H.; et al. A pooled analysis of advanced colorectal neoplasia diagnoses after colonoscopic polypectomy. Gastroenterology 2009, 136, 832–841. [Google Scholar] [CrossRef] [Green Version]
- Sargent, D.J.; Patiyil, S.; Yothers, G.; Haller, D.G.; Gray, R.; Benedetti, J.; Buyse, M.; Labianca, R.; Seitz, J.F.; O’Callaghan, C.J.; et al. End points for colon cancer adjuvant trials: Observations and recommendations based on individual patient data from 20,898 patients enrolled onto 18 randomized trials from the ACCENT Group. J. Clin. Oncol. 2007, 25, 4569–4574. [Google Scholar] [CrossRef] [PubMed]
- Fultz, K.E.; Gerner, E.W. APC-dependent regulation of ornithine decarboxylase in human colon tumor cells. Mol. Carcinog. 2002, 34, 10–18. [Google Scholar] [CrossRef]
- Erdman, S.H.; Ignatenko, N.A.; Powell, M.B.; Blohm-Mangone, K.A.; Holubec, H.; Guillen-Rodriguez, J.M.; Gerner, E.W. APC-dependent changes in expression of genes influencing polyamine metabolism, and consequences for gastrointestinal carcinogenesis, in the Min mouse. Carcinogenesis 1999, 20, 1709–1713. [Google Scholar] [CrossRef] [Green Version]
- Meyskens, F.L., Jr.; McLaren, C.E.; Pelot, D.; Fujikawa-Brooks, S.; Carpenter, P.M.; Hawk, E.; Kelloff, G.; Lawson, M.J.; Kidao, J.; McCracken, J.; et al. Difluoromethylornithine plus sulindac for the prevention of sporadic colorectal adenomas: A randomized placebo-controlled, double-blind trial. Cancer Prev. Res. 2008, 1, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Holbert, C.E.; Cullen, M.T.; Casero, R.A., Jr.; Stewart, T.M. Polyamines in cancer: Integrating organismal metabolism and antitumour immunity. Nat. Rev. Cancer 2022, 22, 467–480. [Google Scholar] [CrossRef]
- Venho, B.; Voutilainen, S.; Valkonen, V.P.; Virtanen, J.; Lakka, T.A.; Rissanen, T.H.; Ovaskainen, M.L.; Laitinen, M.; Salonen, J.T. Arginine intake, blood pressure, and the incidence of acute coronary events in men: The Kuopio Ischaemic Heart Disease Risk Factor Study. Am. J. Clin. Nutr. 2002, 76, 359–364. [Google Scholar] [CrossRef] [Green Version]
- FoodData Central, U.S. Department of Agriculture, Agricultural Research Service. Available online: https://fdc.nal.usda.gov/index.html (accessed on 2 February 2023).
- Giovannucci, E.; Willett, W.C. Dietary factors and risk of colon cancer. Ann. Med. 1994, 26, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Ambs, S.; Merriam, W.G.; Bennett, W.P.; Felley-Bosco, E.; Ogunfusika, M.O.; Oser, S.M.; Klein, S.; Shields, P.G.; Billiar, T.R.; Harris, C.C. Frequent nitric oxide synthase-2 expression in human colon adenomas: Implication for tumor angiogenesis and colon cancer progression. Cancer Res. 1998, 58, 334–341. [Google Scholar] [PubMed]
- Escribano, M.; Molero, L.; Lopez-Farre, A.; Abarrategui, C.; Carrasco, C.; Garcia-Mendez, A.; Manzarbeitia, F.; Martin, M.J.; Vazquez, M.; Sanchez-Fayos, P.; et al. Aspirin inhibits endothelial nitric oxide synthase (eNOS) and Flk-1 (vascular endothelial growth factor receptor-2) prior to rat colon tumour development. Clin. Sci. 2004, 106, 83–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, M.; Fukuda, K.; Ohata, T.; Sugimura, T.; Wakabayashi, K. Increased expression of inducible and endothelial constitutive nitric oxide synthases in rat colon tumors induced by azoxymethane. Cancer Res. 1997, 57, 1233–1237. [Google Scholar]
- Ahn, B.; Ohshima, H. Suppression of intestinal polyposis in Apc(Min/+) mice by inhibiting nitric oxide production. Cancer Res. 2001, 61, 8357–8360. [Google Scholar]
- Yerushalmi, H.F.; Besselsen, D.G.; Ignatenko, N.A.; Blohm-Mangone, K.A.; Padilla-Torres, J.L.; Stringer, D.E.; Cui, H.; Holubec, H.; Payne, C.M.; Gerner, E.W. The role of NO synthases in arginine-dependent small intestinal and colonic carcinogenesis. Mol. Carcinog. 2006, 45, 93–105. [Google Scholar] [CrossRef]
- Zell, J.A.; Ignatenko, N.A.; Yerushalmi, H.F.; Ziogas, A.; Besselsen, D.G.; Gerner, E.W.; Anton-Culver, H. Risk and risk reduction involving arginine intake and meat consumption in colorectal tumorigenesis and survival. Int. J. Cancer 2007, 120, 459–468. [Google Scholar] [CrossRef] [Green Version]
- Zell, J.A.; Ziogas, A.; Bernstein, L.; Clarke, C.A.; Deapen, D.; Largent, J.A.; Neuhausen, S.L.; Stram, D.O.; Ursin, G.; Anton-Culver, H. Meat consumption, nonsteroidal anti-inflammatory drug use, and mortality among colorectal cancer patients in the California Teachers Study. Cancer Prev. Res. 2010, 3, 865–875. [Google Scholar] [CrossRef] [Green Version]
- Bardocz, S.; Duguid, T.J.; Brown, D.S.; Grant, G.; Pusztai, A.; White, A.; Ralph, A. The importance of dietary polyamines in cell regeneration and growth. Br. J. Nutr. 1995, 73, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Kaiser-Kupfer, M.I.; Caruso, R.C.; Valle, D. Gyrate atrophy of the choroid and retina: Further experience with long-term reduction of ornithine levels in children. Arch. Ophthalmol. 2002, 120, 146–153. [Google Scholar] [CrossRef] [Green Version]
- Kaiser-Kupfer, M.I.; Caruso, R.C.; Valle, D.; Reed, G.F. Use of an arginine-restricted diet to slow progression of visual loss in patients with gyrate atrophy. Arch. Ophthalmol. 2004, 122, 982–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyskens, F.L., Jr.; Gerner, E.W.; Emerson, S.; Pelot, D.; Durbin, T.; Doyle, K.; Lagerberg, W. Effect of alpha-difluoromethylornithine on rectal mucosal levels of polyamines in a randomized, double-blinded trial for colon cancer prevention. J. Natl. Cancer Inst. 1998, 90, 1212–1218. [Google Scholar] [CrossRef] [Green Version]
- Seiler, N.; Knodgen, B. High-performance liquid chromatographic procedure for the simultaneous determination of the natural polyamines and their monoacetyl derivatives. J. Chromatogr. 1980, 221, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Kelloff, G.J.; Lippman, S.M.; Dannenberg, A.J.; Sigman, C.C.; Pearce, H.L.; Reid, B.J.; Szabo, E.; Jordan, V.C.; Spitz, M.R.; Mills, G.B.; et al. Progress in chemoprevention drug development: The promise of molecular biomarkers for prevention of intraepithelial neoplasia and cancer—A plan to move forward. Clin. Cancer Res. 2006, 12, 3661–3697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, P.A.; Wertheim, B.C.; Zell, J.A.; Chen, W.P.; McLaren, C.E.; LaFleur, B.J.; Meyskens, F.L.; Gerner, E.W. Levels of rectal mucosal polyamines and prostaglandin E2 predict ability of DFMO and sulindac to prevent colorectal adenoma. Gastroenterology 2010, 139, 797–805. [Google Scholar] [CrossRef] [Green Version]
- Simoneau, A.R.; Gerner, E.W.; Phung, M.; McLaren, C.E.; Meyskens, F.L., Jr. Alpha-difluoromethylornithine and polyamine levels in the human prostate: Results of a phase IIa trial. J. Natl. Cancer Inst. 2001, 93, 57–59. [Google Scholar] [CrossRef] [Green Version]
- Ignatenko, N.A.; Besselsen, D.G.; Stringer, D.E.; Blohm-Mangone, K.A.; Cui, H.; Gerner, E.W. Combination chemoprevention of intestinal carcinogenesis in a murine model of familial adenomatous polyposis. Nutr. Cancer 2008, 60 (Suppl. S1), 30–35. [Google Scholar] [CrossRef]
- Baron, J.A.; Cole, B.F.; Sandler, R.S.; Haile, R.W.; Ahnen, D.; Bresalier, R.; McKeown-Eyssen, G.; Summers, R.W.; Rothstein, R.; Burke, C.A.; et al. A randomized trial of aspirin to prevent colorectal adenomas. N. Engl. J. Med. 2003, 348, 891–899. [Google Scholar] [CrossRef]
- Sandler, R.S.; Halabi, S.; Baron, J.A.; Budinger, S.; Paskett, E.; Keresztes, R.; Petrelli, N.; Pipas, J.M.; Karp, D.D.; Loprinzi, C.L.; et al. A randomized trial of aspirin to prevent colorectal adenomas in patients with previous colorectal cancer. N. Engl. J. Med. 2003, 348, 883–890. [Google Scholar] [CrossRef]
- Steinbach, G.; Lynch, P.M.; Phillips, R.K.; Wallace, M.H.; Hawk, E.; Gordon, G.B.; Wakabayashi, N.; Saunders, B.; Shen, Y.; Fujimura, T.; et al. The effect of celecoxib, a cyclooxygenase-2 inhibitor, in familial adenomatous polyposis. N. Engl. J. Med. 2000, 342, 1946–1952. [Google Scholar] [CrossRef]
- Chan, A.T.; Giovannucci, E.L.; Schernhammer, E.S.; Colditz, G.A.; Hunter, D.J.; Willett, W.C.; Fuchs, C.S. A prospective study of aspirin use and the risk for colorectal adenoma. Ann. Intern. Med. 2004, 140, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Asano, T.K.; McLeod, R.S. Nonsteroidal anti-inflammatory drugs and aspirin for the prevention of colorectal adenomas and cancer: A systematic review. Dis. Colon Rectum 2004, 47, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.T.; Giovannucci, E.L.; Meyerhardt, J.A.; Schernhammer, E.S.; Curhan, G.C.; Fuchs, C.S. Long-term use of aspirin and nonsteroidal anti-inflammatory drugs and risk of colorectal cancer. JAMA 2005, 294, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Mahipal, A.; Anderson, K.E.; Limburg, P.J.; Folsom, A.R. Nonsteroidal anti-inflammatory drugs and subsite-specific colorectal cancer incidence in the Iowa women’s health study. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 1785–1790. [Google Scholar] [CrossRef] [Green Version]
- Arber, N.; Eagle, C.J.; Spicak, J.; Racz, I.; Dite, P.; Hajer, J.; Zavoral, M.; Lechuga, M.J.; Gerletti, P.; Tang, J.; et al. Celecoxib for the prevention of colorectal adenomatous polyps. N. Engl. J. Med. 2006, 355, 885–895. [Google Scholar] [CrossRef] [Green Version]
- Bertagnolli, M.M.; Eagle, C.J.; Zauber, A.G.; Redston, M.; Solomon, S.D.; Kim, K.; Tang, J.; Rosenstein, R.B.; Wittes, J.; Corle, D.; et al. Celecoxib for the prevention of sporadic colorectal adenomas. N. Engl. J. Med. 2006, 355, 873–884. [Google Scholar] [CrossRef] [PubMed]
- Force, U.S.P.S.T.; Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Chelmow, D.; Coker, T.R.; Davis, E.M.; Donahue, K.E.; Jaen, C.R.; et al. Aspirin Use to Prevent Cardiovascular Disease: US Preventive Services Task Force Recommendation Statement. JAMA 2022, 327, 1577–1584. [Google Scholar] [CrossRef]
- Nelson, E.L.; Wenzel, L.B.; Osann, K.; Dogan-Ates, A.; Chantana, N.; Reina-Patton, A.; Laust, A.K.; Nishimoto, K.P.; Chicz-DeMet, A.; du Pont, N.; et al. Stress, immunity, and cervical cancer: Biobehavioral outcomes of a randomized clinical trial [corrected]. Clin. Cancer Res. 2008, 14, 2111–2118. [Google Scholar] [CrossRef] [Green Version]
- Osann, K.; Wilford, J.; Wenzel, L.; Hsieh, S.; Tucker, J.A.; Wahi, A.; Monk, B.J.; Nelson, E.L. Relationship between social support, quality of life, and Th2 cytokines in a biobehavioral cancer survivorship trial. Support. Care Cancer 2019, 27, 3301–3310. [Google Scholar] [CrossRef] [Green Version]
- Zell, J.A.; McLaren, C.E.; Chen, W.P.; Thompson, P.A.; Gerner, E.W.; Meyskens, F.L. Ornithine decarboxylase-1 polymorphism, chemoprevention with eflornithine and sulindac, and outcomes among colorectal adenoma patients. J. Natl. Cancer Inst. 2010, 102, 1513–1516. [Google Scholar] [CrossRef] [Green Version]
- Zell, J.A.; Ziogas, A.; Ignatenko, N.; Honda, J.; Qu, N.; Bobbs, A.S.; Neuhausen, S.L.; Gerner, E.W.; Anton-Culver, H. Associations of a polymorphism in the ornithine decarboxylase gene with colorectal cancer survival. Clin. Cancer Res. 2009, 15, 6208–6216. [Google Scholar] [CrossRef] [Green Version]
- Zell, J.A.; Lin, B.S.; Ziogas, A.; Anton-Culver, H. Meat consumption, ornithine decarboxylase gene polymorphism, and outcomes after colorectal cancer diagnosis. J. Carcinog. 2012, 11, 17. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Fang, Y.J.; Abulimiti, A.; Yang, X.; Li, L.; Liu, K.Y.; Zhang, X.; Feng, X.L.; Chen, Y.M.; Zhang, C.X. Dietary Polyamines Intake and Risk of Colorectal Cancer: A Case-Control Study. Nutrients 2020, 12, 3575. [Google Scholar] [CrossRef]
- Vargas, A.J.; Ashbeck, E.L.; Wertheim, B.C.; Wallace, R.B.; Neuhouser, M.L.; Thomson, C.A.; Thompson, P.A. Dietary polyamine intake and colorectal cancer risk in postmenopausal women. Am. J. Clin. Nutr. 2015, 102, 411–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, C.A.; Dekker, E.; Lynch, P.; Samadder, N.J.; Balaguer, F.; Huneburg, R.; Burn, J.; Castells, A.; Gallinger, S.; Lim, R.; et al. Eflornithine plus Sulindac for Prevention of Progression in Familial Adenomatous Polyposis. N. Engl. J. Med. 2020, 383, 1028–1039. [Google Scholar] [CrossRef] [PubMed]
- Balaguer, F.; Stoffel, E.M.; Burke, C.A.; Dekker, E.; Samadder, N.J.; Van Cutsem, E.; Lynch, P.M.; Wise, P.E.; Huneburg, R.; Lim, R.M.; et al. Combination of Sulindac and Eflornithine Delays the Need for Lower Gastrointestinal Surgery in Patients With Familial Adenomatous Polyposis: Post Hoc Analysis of a Randomized Clinical Trial. Dis. Colon Rectum 2022, 65, 536–545. [Google Scholar] [CrossRef]
- Meyerhardt, J.A.; Shi, Q.; Fuchs, C.S.; Meyer, J.; Niedzwiecki, D.; Zemla, T.; Kumthekar, P.; Guthrie, K.A.; Couture, F.; Kuebler, P.; et al. Effect of Celecoxib vs Placebo Added to Standard Adjuvant Therapy on Disease-Free Survival Among Patients With Stage III Colon Cancer: The CALGB/SWOG 80702 (Alliance) Randomized Clinical Trial. JAMA 2021, 325, 1277–1286. [Google Scholar] [CrossRef]
- Cheng, E.; Shi, Q.; Shields, A.F.; Nixon, A.B.; Shergill, A.P.; Ma, C.; Guthrie, K.A.; Couture, F.; Kuebler, P.; Kumar, P.; et al. Association of Inflammatory Biomarkers With Survival Among Patients With Stage III Colon Cancer. JAMA Oncol. 2023, 9, 404. [Google Scholar] [CrossRef]
- Zell, J.; You, Y.N.; Boughey, J.C. PACES trial: Evaluating the effectiveness of eflornithine and sulindac in preventing colon adenomas. Bull. Am. Coll. Surg. 2015, 100, 70–71. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 20) | ||
|---|---|---|
| Gender | Male | 13 (65%) |
| Female | 7 (35%) | |
| Mean Age | Male | 62.1 y (12.3) |
| Female | 51.7 y (6.9) | |
| Total | 58.1 y (11.6) | |
| Race | Asian | 8 (40%) |
| White | 12 (60%) | |
| Ethnicity | Hispanic | 1 (5%) |
| White | 19 (95%) | |
| Tumor Subsite Location | Cecum | 1 (4.8%) |
| Transverse | 1 (4.8%) | |
| Sigmoid | 5 (23.8%) | |
| Rectosigmoid | 4 (19%) | |
| Rectum | 6 (28.6%) | |
| Colorectum-NOS | 3 (15%) | |
| AJCC Stage | I | 4 (19%) |
| IIA | 4 (19%) | |
| IIIA | 3 (14.3%) | |
| IIIB | 8 (38.1%) | |
| IIIC | 1 (4.8%) | |
| Tumor Grade | Well-Differentiated (Gr 1) | 3 (15%) |
| Moderately Differentiated (Gr 2) | 10 (50%) | |
| Poorly Differentiated (Gr 3) | 1 (5%) | |
| Missing | 6 (30%) | |
| Odc Genotype | AA | 4 (20%) |
| AG | 7 (35%) | |
| GG | 9 (45%) | |
| Randomized to PTC Intervention? | Yes No | 8 (40%) 7 (35%) |
| N/A | 5 (25%) |
| Variable | N | Mean | Median | Std Dev | Minimum | Maximum |
|---|---|---|---|---|---|---|
| Carbohydrate (g) Baseline Midpoint End of Study | 20 17 17 | 216.5 210.1 189.7 | 200.4 193.9 182.5 | 101.4 105.9 58.0 | 97.2 74.9 75.0 | 518.9 563.9 298.1 |
| Fiber (g) Baseline Midpoint End of Study | 20 17 17 | 18.0 18.5 17.4 | 18.4 16.5 16.1 | 7.3 10.5 6.4 | 6.6 5.6 7.0 | 31.8 48.2 33.1 |
| Fat (g) Baseline Midpoint End of Study | 20 17 17 | 56.5 51.4 49.2 | 49.8 52.4 48.2 | 29.6 32.9 19.0 | 16.7 17.6 14.8 | 160.4 154.6 79.8 |
| Protein (g) Baseline Midpoint End of Study | 20 17 17 | 65.4 55.9 53.5 | 62.9 54.3 49.4 | 20.9 20.5 20.3 | 27.8 27.8 16.7 | 118.7 112.4 92.7 |
| Energy (kcal) Baseline Midpoint End of Study | 20 17 17 | 1625.5 1515.7 1409.8 | 1595.1 1388.4 1445.1 | 682.2 766.7 401.9 | 661.4 630.0 508.4 | 3925.5 4090.4 2255.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zell, J.A.; Taylor, T.H.; Albers, C.G.; Carmichael, J.C.; McLaren, C.E.; Wenzel, L.; Stamos, M.J. Phase IIa Clinical Biomarker Trial of Dietary Arginine Restriction and Aspirin in Colorectal Cancer Patients. Cancers 2023, 15, 2103. https://doi.org/10.3390/cancers15072103
Zell JA, Taylor TH, Albers CG, Carmichael JC, McLaren CE, Wenzel L, Stamos MJ. Phase IIa Clinical Biomarker Trial of Dietary Arginine Restriction and Aspirin in Colorectal Cancer Patients. Cancers. 2023; 15(7):2103. https://doi.org/10.3390/cancers15072103
Chicago/Turabian StyleZell, Jason A., Thomas H. Taylor, C. Gregory Albers, Joseph C. Carmichael, Christine E. McLaren, Lari Wenzel, and Michael J. Stamos. 2023. "Phase IIa Clinical Biomarker Trial of Dietary Arginine Restriction and Aspirin in Colorectal Cancer Patients" Cancers 15, no. 7: 2103. https://doi.org/10.3390/cancers15072103
APA StyleZell, J. A., Taylor, T. H., Albers, C. G., Carmichael, J. C., McLaren, C. E., Wenzel, L., & Stamos, M. J. (2023). Phase IIa Clinical Biomarker Trial of Dietary Arginine Restriction and Aspirin in Colorectal Cancer Patients. Cancers, 15(7), 2103. https://doi.org/10.3390/cancers15072103