

Predictors for Survival of Patients with Squamous Cell Carcinoma of Unknown Primary in the Head and Neck Region
 , , , , , ,
, , , , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
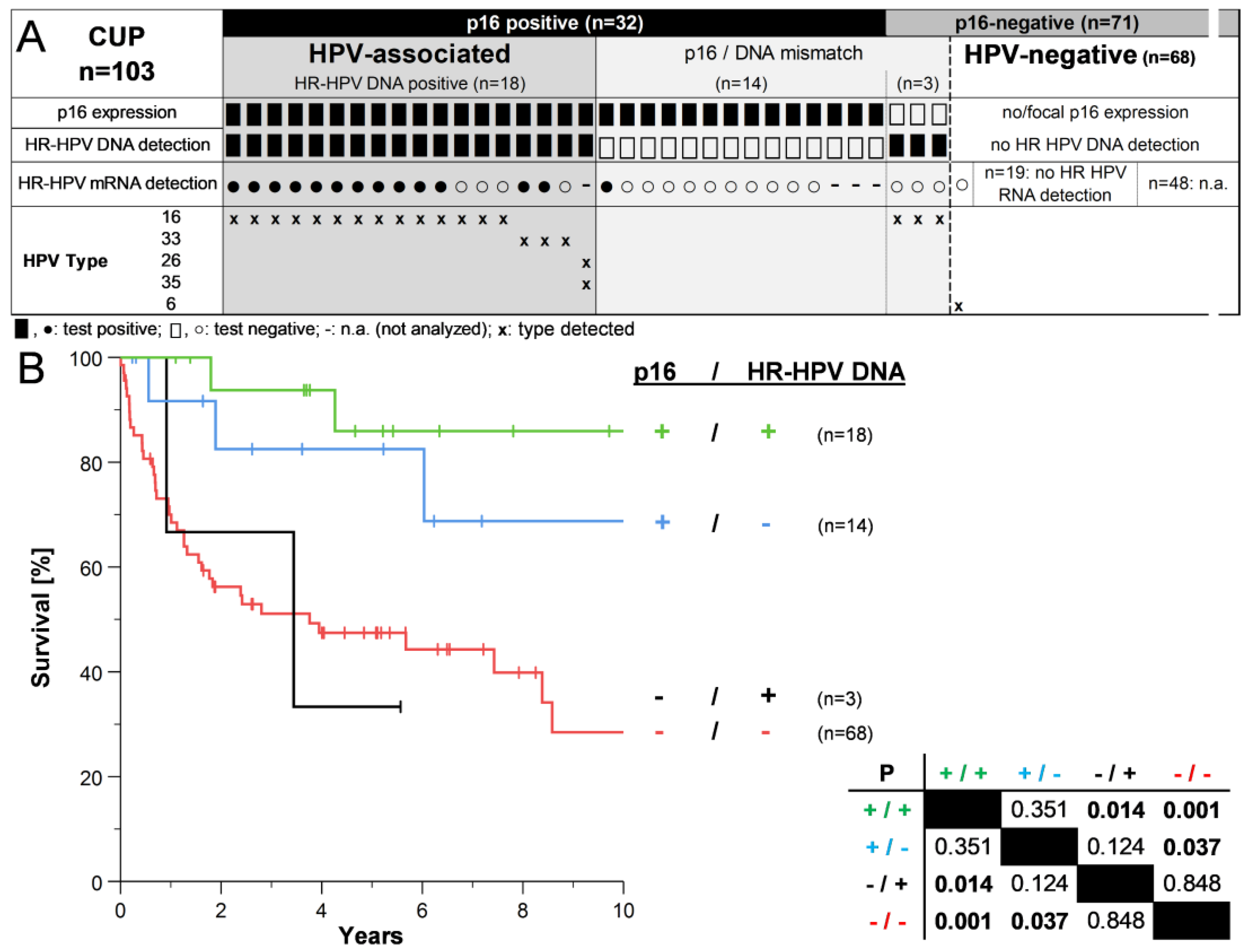
3.1. Descriptive Analysis of CUPHNSCC according to p16 Status
3.2. HPV Status in CUPHNSCC and Survival of Patients
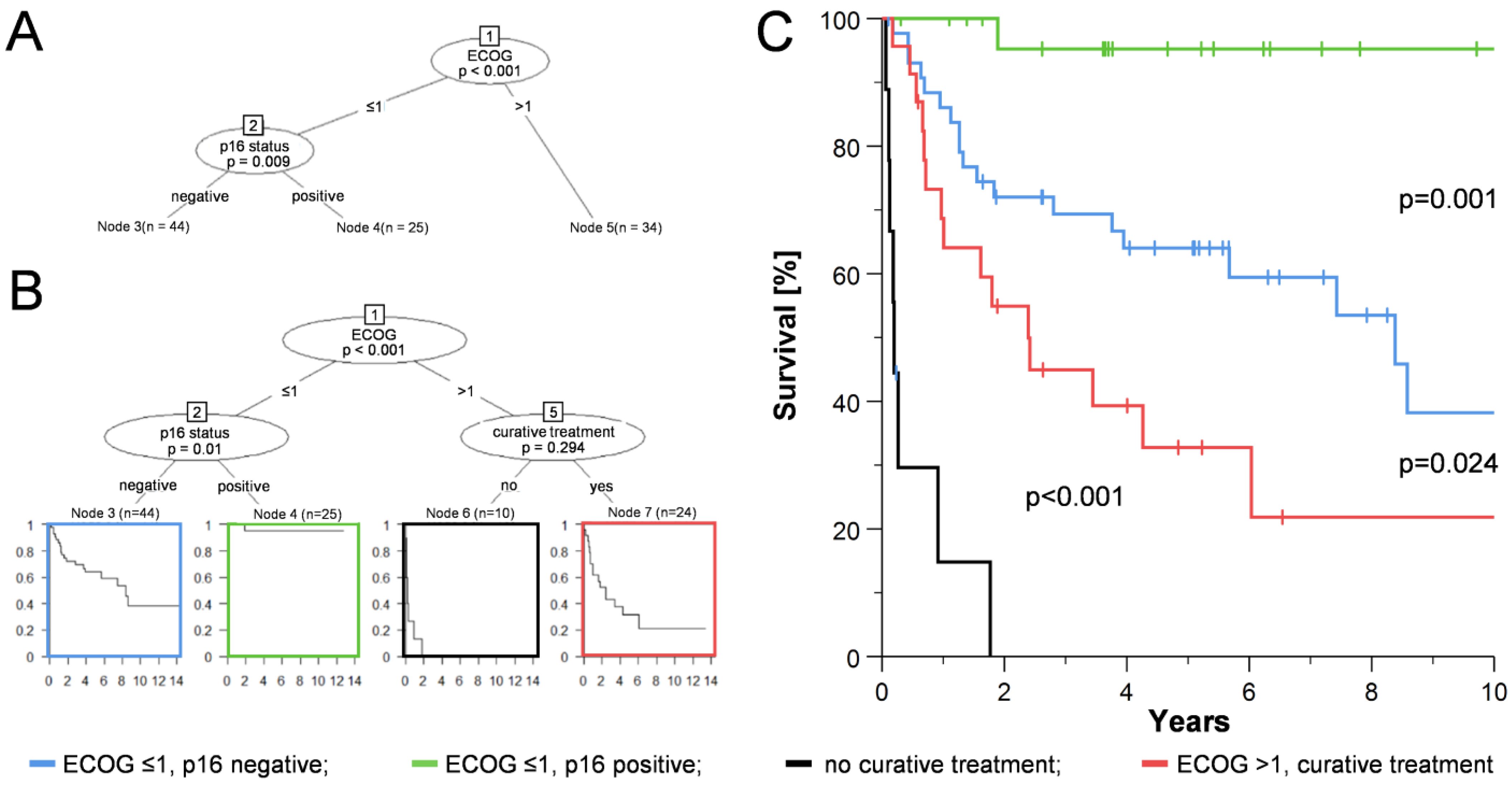
3.3. Development of a Risk Model for CUPHNSCC by Recursive Partitioning Analysis (RPA)
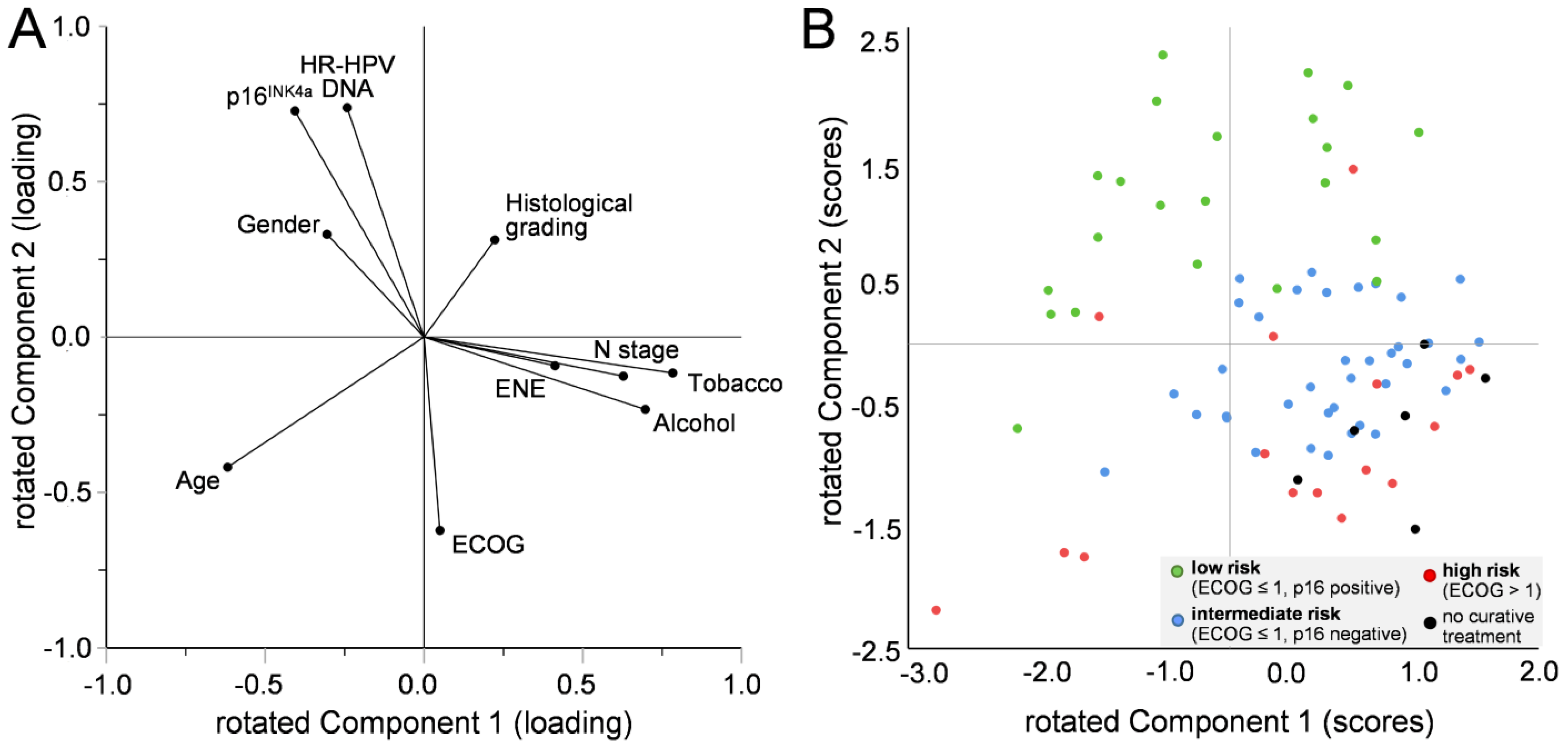
3.4. Correlation of Factors Affecting the Formation of the Risk Model in Patients with CUPHNSCC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Issing, W.J.; Taleban, B.; Tauber, S. Diagnosis and management of carcinoma of unknown primary in the head and neck. Eur. Arch. Otorhinolaryngol. 2003, 260, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Regelink, G.; Brouwer, J.; de Bree, R.; Pruim, J.; van der Laan, B.F.; Vaalburg, W.; Hoekstra, O.S.; Comans, E.F.; Vissink, A.; Leemans, C.R.; et al. Detection of unknown primary tumours and distant metastases in patients with cervical metastases: Value of FDG-PET versus conventional modalities. Eur. J. Nucl. Med. Mol. Imaging 2002, 29, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Arosio, A.D.; Pignataro, L.; Gaini, R.M.; Garavello, W. Neck lymph node metastases from unknown primary. Cancer Treat. Rev. 2017, 53, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, R. Distribution of cervical lymph node metastases from squamous cell carcinoma of the upper respiratory and digestive tracts. Cancer 1972, 29, 1446–1449. [Google Scholar] [CrossRef] [PubMed]
- Robbins, K.T.; Shaha, A.R.; Medina, J.E.; Califano, J.A.; Wolf, G.T.; Ferlito, A.; Som, P.M.; Day, T.A.; Committee for Neck Dissection Classification, A.H.; Neck, S. Consensus statement on the classification and terminology of neck dissection. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 536–538. [Google Scholar] [CrossRef] [Green Version]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [Green Version]
- Wittekindt, C.; Wagner, S.; Bushnak, A.; Prigge, E.S.; von Knebel Doeberitz, M.; Wurdemann, N.; Bernhardt, K.; Pons-Kuhnemann, J.; Maulbecker-Armstrong, C.; Klussmann, J.P. Increasing Incidence rates of Oropharyngeal Squamous Cell Carcinoma in Germany and Significance of Disease Burden Attributed to Human Papillomavirus. Cancer PRev. Res. 2019, 12, 375–382. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, A.K.; Engels, E.A.; Pfeiffer, R.M.; Hernandez, B.Y.; Xiao, W.; Kim, E.; Jiang, B.; Goodman, M.T.; Sibug-Saber, M.; Cozen, W.; et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J. Clin. Oncol. 2011, 29, 4294–4301. [Google Scholar] [CrossRef]
- Boeker, R.; Stromberger, C.; Heiland, M.; Beck-Broichsitter, B.; Hofmann, V.M.; Neumann, K.; Ochsenreither, S.; Olze, H.; Dommerich, S.; Piwonski, I.; et al. Carcinoma of Unknown Primary and the 8th Edition TNM Classification for Head and Neck Cancer. Laryngoscope 2021, 131, E2534–E2542. [Google Scholar] [CrossRef]
- Schroeder, L.; Pring, M.; Ingarfield, K.; Pawlita, M.; Leary, S.D.; Thomas, S.J.; Waylen, A.; Waterboer, T.; Ness, A.R. HPV driven squamous cell head and neck cancer of unknown primary is likely to be HPV driven squamous cell oropharyngeal cancer. Oral Oncol. 2020, 107, 104721. [Google Scholar] [CrossRef]
- Ren, J.; Yang, W.; Su, J.; Ren, X.; Fazelzad, R.; Albert, T.; Habbous, S.; Goldstein, D.P.; de Almeida, J.R.; Hansen, A.; et al. Human papillomavirus and p16 immunostaining, prevalence and prognosis of squamous carcinoma of unknown primary in the head and neck region. Int. J. Cancer 2019, 145, 1465–1474. [Google Scholar] [CrossRef]
- American Joint Committee on, C. AJCC Cancer Staging Manual, 8th ed.; Corrected at 3rd Printing ed.; Amin, M.B., Greene, F.L., Edge, S.B., Eds.; AJCC, American Joint Committee on Cancer: Chicago, IL, USA, 2017. [Google Scholar]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tan, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Rietbergen, M.M.; Witte, B.I.; Velazquez, E.R.; Snijders, P.J.; Bloemena, E.; Speel, E.J.; Brakenhoff, R.H.; Kremer, B.; Lambin, P.; Leemans, C.R. Different prognostic models for different patient populations: Validation of a new prognostic model for patients with oropharyngeal cancer in Western Europe. Br. J. Cancer 2015, 112, 1733–1736. [Google Scholar] [CrossRef] [Green Version]
- Velazquez, E.R.; Hoebers, F.; Aerts, H.J.; Rietbergen, M.M.; Brakenhoff, R.H.; Leemans, R.C.; Speel, E.J.; Straetmans, J.; Kremer, B.; Lambin, P. Externally validated HPV-based prognostic nomogram for oropharyngeal carcinoma patients yields more accurate predictions than TNM staging. Radiother. Oncol. 2014, 113, 324–330. [Google Scholar] [CrossRef] [Green Version]
- Wagner, S.; Wittekindt, C.; Sharma, S.J.; Wuerdemann, N.; Juttner, T.; Reuschenbach, M.; Prigge, E.S.; von Knebel Doeberitz, M.; Gattenlohner, S.; Burkhardt, E.; et al. Human papillomavirus association is the most important predictor for surgically treated patients with oropharyngeal cancer. Br. J. Cancer 2017, 116, 1604–1611. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, L.; Boscolo-Rizzo, P.; Dal Cin, E.; Romeo, S.; Baboci, L.; Dyckhoff, G.; Hess, J.; Lucena-Porcel, C.; Byl, A.; Becker, N.; et al. Human papillomavirus as prognostic marker with rising prevalence in neck squamous cell carcinoma of unknown primary: A retrospective multicentre study. Eur. J. Cancer 2017, 74, 73–81. [Google Scholar] [CrossRef]
- Dixon, P.R.; Au, M.; Hosni, A.; Perez-Ordonez, B.; Weinreb, I.; Xu, W.; Song, Y.; Huang, S.H.; O’Sullivan, B.; Goldstein, D.P.; et al. Impact of p16 expression, nodal status, and smoking on oncologic outcomes of patients with head and neck unknown primary squamous cell carcinoma. Head Neck 2016, 38, 1347–1353. [Google Scholar] [CrossRef]
- Cheraghlou, S.; Torabi, S.J.; Husain, Z.A.; Otremba, M.D.; Osborn, H.A.; Mehra, S.; Yarbrough, W.G.; Burtness, B.A.; Judson, B.L. HPV status in unknown primary head and neck cancer: Prognosis and treatment outcomes. Laryngoscope 2019, 129, 684–691. [Google Scholar] [CrossRef]
- Gillison, M.L.; Trotti, A.M.; Harris, J.; Eisbruch, A.; Harari, P.M.; Adelstein, D.J.; Jordan, R.C.K.; Zhao, W.; Sturgis, E.M.; Burtness, B.; et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): A randomised, multicentre, non-inferiority trial. Lancet 2019, 393, 40–50. [Google Scholar] [CrossRef]
- Mehanna, H.; Robinson, M.; Hartley, A.; Kong, A.; Foran, B.; Fulton-Lieuw, T.; Dalby, M.; Mistry, P.; Sen, M.; O’Toole, L.; et al. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): An open-label randomised controlled phase 3 trial. Lancet 2019, 393, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Patel, R.R.; Ludmir, E.B.; Augustyn, A.; Zaorsky, N.G.; Lehrer, E.J.; Ryali, R.; Trifiletti, D.M.; Adeberg, S.; Amini, A.; Verma, V. De-intensification of therapy in human papillomavirus associated oropharyngeal cancer: A systematic review of prospective trials. Oral Oncol. 2020, 103, 104608. [Google Scholar] [CrossRef] [PubMed]
- Mirghani, H.; Blanchard, P. Treatment de-escalation for HPV-driven oropharyngeal cancer: Where do we stand? Clin. Transl. Radiat. Oncol. 2018, 8, 4–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boscolo-Rizzo, P.; Pawlita, M.; Holzinger, D. From HPV-positive towards HPV-driven oropharyngeal squamous cell carcinomas. Cancer Treat. Rev. 2016, 42, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Nauta, I.H.; Rietbergen, M.M.; van Bokhoven, A.; Bloemena, E.; Lissenberg-Witte, B.I.; Heideman, D.A.M.; Baatenburg de Jong, R.J.; Brakenhoff, R.H.; Leemans, C.R. Evaluation of the eighth TNM classification on p16-positive oropharyngeal squamous cell carcinomas in the Netherlands and the importance of additional HPV DNA testing. Ann. Oncol. 2018, 29, 1273–1279. [Google Scholar] [CrossRef]
- Prigge, E.S.; Arbyn, M.; von Knebel Doeberitz, M.; Reuschenbach, M. Diagnostic accuracy of p16(INK4a) immunohistochemistry in oropharyngeal squamous cell carcinomas: A systematic review and meta-analysis. Int. J. Cancer 2017, 140, 1186–1198. [Google Scholar] [CrossRef] [Green Version]
- Wagner, S.; Prigge, E.S.; Wuerdemann, N.; Reder, H.; Bushnak, A.; Sharma, S.J.; Obermueller, T.; von Knebel Doeberitz, M.; Dreyer, T.; Gattenlohner, S.; et al. Evaluation of p16(INK4a) expression as a single marker to select patients with HPV-driven oropharyngeal cancers for treatment de-escalation. Br. J. Cancer 2020, 123, 1114–1122. [Google Scholar] [CrossRef]
- Hotelling, H. Relations Between Two Sets of Variates. Biometrika 1936, 28, 321–377. [Google Scholar] [CrossRef]
- Pearson, K.L., III. On lines and planes of closest fit to systems of points in space. Lond. Edinb. Dublin Philos. Mag. J. Sci. 1901, 2, 559–572. [Google Scholar] [CrossRef] [Green Version]
- Sobin, L.H.; Wittekind, C. (Eds.) TNM Classification of Malignant Tumours, 6th Edition (UICC), 6th ed.; Wiley-Liss: New York, NY, USA, 2002. [Google Scholar]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. (Eds.) TNM Classification of Malignant Tumours, 7th Edition (UICC), 7th ed.; Wiley-Blackwell: Chichester, UK; Hoboken, NJ, USA, 2010. [Google Scholar]
- Pindborg, J.J. (Ed.) Histological Typing of Cancer and Precancer of the Oral Mucosa, 2nd ed.; Springer: Berlin/Heidelberg, Germany; New York, NY, USA; Barcelona, Spain; Budapest, Hungary; Hong Kong; London, UK; Milan, Italy; Paris, France; Santa Clara, CA, USA; Singapore; Tokyo, Japan, 1997; pp. X, 87 S. [Google Scholar]
- Prigge, E.S.; Toth, C.; Dyckhoff, G.; Wagner, S.; Muller, F.; Wittekindt, C.; Freier, K.; Plinkert, P.; Hoffmann, J.; Vinokurova, S.; et al. p16(INK4a)/Ki-67 co-expression specifically identifies transformed cells in the head and neck region. Int. J. Cancer 2015, 136, 1589–1599. [Google Scholar] [CrossRef]
- Halec, G.; Schmitt, M.; Dondog, B.; Sharkhuu, E.; Wentzensen, N.; Gheit, T.; Tommasino, M.; Kommoss, F.; Bosch, F.X.; Franceschi, S.; et al. Biological activity of probable/possible high-risk human papillomavirus types in cervical cancer. Int. J. Cancer 2013, 132, 63–71. [Google Scholar] [CrossRef]
- Hothorn, T.; Zeileis, A. partykit: A Modular Toolkit for Recursive Partytioning in R. J. Mach. Learn. Res. 2015, 16, 3905–3909. [Google Scholar]
- Straetmans, J.; Vent, J.; Lacko, M.; Speel, E.J.; Huebbers, C.; Semrau, R.; Hoebers, F.; Mujagic, Z.; Klussmann, J.P.; Preuss, S.F.; et al. Management of neck metastases of unknown primary origin united in two European centers. Eur. Arch. Otorhinolaryngol. 2015, 272, 195–205. [Google Scholar] [CrossRef]
- Jensen, D.H.; Hedback, N.; Specht, L.; Hogdall, E.; Andersen, E.; Therkildsen, M.H.; Friis-Hansen, L.; Norrild, B.; von Buchwald, C. Human papillomavirus in head and neck squamous cell carcinoma of unknown primary is a common event and a strong predictor of survival. PLoS ONE 2014, 9, e110456. [Google Scholar] [CrossRef]
- Tribius, S.; Hoffmann, A.S.; Bastrop, S.; Gorogh, T.; Haag, J.; Rocken, C.; Clauditz, T.; Grob, T.; Wilczak, W.; Tennstedt, P.; et al. HPV status in patients with head and neck of carcinoma of unknown primary site: HPV, tobacco smoking, and outcome. Oral Oncol. 2012, 48, 1178–1184. [Google Scholar] [CrossRef]
- Schroeder, L.; Wichmann, G.; Willner, M.; Michel, A.; Wiesenfarth, M.; Flechtenmacher, C.; Gradistanac, T.; Pawlita, M.; Dietz, A.; Waterboer, T.; et al. Antibodies against human papillomaviruses as diagnostic and prognostic biomarker in patients with neck squamous cell carcinoma from unknown primary tumor. Int. J. Cancer 2018, 142, 1361–1368. [Google Scholar] [CrossRef] [Green Version]
- Ilmarinen, T.; Auvinen, E.; Hiltunen-Back, E.; Ranki, A.; Aaltonen, L.M.; Pitkaranta, A. Transmission of human papillomavirus DNA from patient to surgical masks, gloves and oral mucosa of medical personnel during treatment of laryngeal papillomas and genital warts. Eur. Arch. Otorhinolaryngol. 2012, 269, 2367–2371. [Google Scholar] [CrossRef]
- Wang, Y.; Tian, Y.; Lin, J.; Chen, L.; Wang, L.; Hao, P.; Han, R.; Ying, M.; Li, X.; Tang, X. Assessment of p16 expression and HPV infection in adenoid cystic carcinoma of the lacrimal gland. Mol. Vis. 2018, 24, 143–152. [Google Scholar]
- Antony, V.M.; Kakkar, A.; Sikka, K.; Thakar, A.; Deo, S.V.S.; Bishop, J.A.; Jain, D. p16 Immunoexpression in sinonasal and nasopharyngeal adenoid cystic carcinomas: A potential pitfall in ruling out HPV-related multiphenotypic sinonasal carcinoma. Histopathology 2020, 77, 989–993. [Google Scholar] [CrossRef]
- Stagner, A.M.; Afrogheh, A.H.; Jakobiec, F.A.; Iacob, C.E.; Grossniklaus, H.E.; Deshpande, V.; Maske, C.; Hiss, D.C.; Faquin, W.C. p16 Expression Is Not a Surrogate Marker for High-Risk Human Papillomavirus Infection in Periocular Sebaceous Carcinoma. Am. J. OphthalMol. 2016, 170, 168–175. [Google Scholar] [CrossRef]
- George, M.; Smith, A.; Sabesan, S.; Ranmuthugala, G. Physical Comorbidities and Their Relationship with Cancer Treatment and Its Outcomes in Older Adult Populations: Systematic Review. JMIR Cancer 2021, 7, e26425. [Google Scholar] [CrossRef]
- Maltoni, R.; Ravaioli, S.; Bronte, G.; Mazza, M.; Cerchione, C.; Massa, I.; Balzi, W.; Cortesi, M.; Zanoni, M.; Bravaccini, S. Chronological age or biological age: What drives the choice of adjuvant treatment in elderly breast cancer patients? Transl. Oncol. 2022, 15, 101300. [Google Scholar] [CrossRef] [PubMed]
- Amr, S.; Ioffe, D.; Suzuki, I.; Mehra, R.; Cullen, K.; Goloubeva, O. Treatment modalities, adverse events, and survival outcomes in older patients with head and neck squamous cell carcinoma. Head Neck 2021, 43, 3935–3945. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, T.L.; Edge, S.B.; Kossoff, E.B.; Groman, A.; Wilding, G.E.; Ademuyiwa, F.O.; Levine, E.G.; Watroba, N.; Ngamphaiboon, N. Factors affecting the delivery of adjuvant/neoadjuvant chemotherapy in older women with breast cancer. J. Geriatr. Oncol. 2012, 3, 320–328. [Google Scholar] [CrossRef]
- Rassy, E.; Nicolai, P.; Pavlidis, N. Comprehensive management of HPV-related squamous cell carcinoma of the head and neck of unknown primary. Head Neck 2019, 41, 3700–3711. [Google Scholar] [CrossRef]
- Sivars, L.; Tani, E.; Nasman, A.; Ramqvist, T.; Munck-Wikland, E.; Dalianis, T. Human Papillomavirus as a Diagnostic and Prognostic Tool in Cancer of Unknown Primary in the Head and Neck Region. Anticancer. Res. 2016, 36, 487–493. [Google Scholar]
- Strojan, P.; Ferlito, A.; Medina, J.E.; Woolgar, J.A.; Rinaldo, A.; Robbins, K.T.; Fagan, J.J.; Mendenhall, W.M.; Paleri, V.; Silver, C.E.; et al. Contemporary management of lymph node metastases from an unknown primary to the neck: I. A review of diagnostic approaches. Head Neck 2013, 35, 123–132. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total | p16-Positive | p16-Negative | p | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Total | 103 | 100 | 32 | 31 | 71 | 69 | N/A | |
| Gender | Male | 78 | 76 | 21 | 66 | 57 | 80 | 0.108 |
| Female | 25 | 24 | 11 | 34 | 14 | 20 | ||
| Age (years) | Median | 62.9 | 62.0 | 63.0 | 0.847 # | |||
| Minimum | 32.2 | 47.0 | 32.2 | N/A | ||||
| Maximum | 95.2 | 84.9 | 95.2 | N/A | ||||
| Sampling period | 2000 to 2009 | 50 | 49 | 15 | 47 | 35 | 49 | 0.820 |
| 2010 to 2018 | 53 | 51 | 17 | 53 | 36 | 51 | ||
| N stage | 1 | 11 | 11 | 3 | 9 | 8 | 11 | 0.168 |
| 2a | 15 | 15 | 7 | 22 | 8 | 11 | ||
| 2b | 48 | 47 | 18 | 56 | 30 | 43 | ||
| 2c | 5 | 5 | 1 | 3 | 4 | 6 | ||
| 3 | 23 | 22 | 3 | 9 | 20 | 29 | ||
| unknown | 1 | 1 | - | 1 | ||||
| N stage (dichotomized) | 1–2b | 74 | 73 | 28 | 88 | 46 | 66 | 0.022 |
| >2b | 28 | 27 | 4 | 13 | 24 | 34 | ||
| Extranodal extension (ENE) | No | 35 | 34 | 15 | 58 | 20 | 33 | 0.035 |
| Yes | 51 | 50 | 11 | 42 | 40 | 67 | ||
| unknown | 17 | 17 | 6 | 11 | ||||
| Tobacco | Non-smokers | 25 | 24 | 13 | 43 | 12 | 18 | 0.007 |
| Smokers | 73 | 71 | 17 | 57 | 56 | 82 | ||
| unknown | 5 | 5 | 2 | 3 | ||||
| Alcohol | Non-drinkers | 55 | 53 | 24 | 77 | 31 | 45 | 0.003 |
| Drinkers | 45 | 44 | 7 | 23 | 38 | 55 | ||
| unknown | 3 | 3 | 1 | 2 | ||||
| ECOG | 0 | 16 | 16 | 7 | 22 | 9 | 13 | 0.469 |
| 1 | 53 | 51 | 18 | 56 | 35 | 49 | ||
| 2 | 26 | 25 | 6 | 19 | 20 | 28 | ||
| 3 | 7 | 7 | 1 | 3 | 6 | 8 | ||
| 4 | 1 | 1 | 0 | 0 | 1 | 1 | ||
| ECOG (dichotomized) | 0–1 | 69 | 67 | 25 | 78 | 44 | 62 | 0.107 |
| >1 | 34 | 33 | 7 | 22 | 27 | 38 | ||
| Histological grading | ||||||||
| low/intermediate | 1–2 | 38 | 37 | 8 | 25 | 30 | 43 | 0.083 |
| high grade | >2 | 64 | 62 | 24 | 75 | 40 | 57 | |
| unknown | 1 | 1 | - | 1 | ||||
| Treatment intension | Palliative | 13 | 13 | 1 | 3 | 12 | 17 | 0.057 * |
| Curative | 88 | 85 | 31 | 97 | 57 | 83 | ||
| unknown | 2 | 2 | - | 2 | ||||
| Curative treatment (% based on n = 88) | Surgery only | 8 | 9 | 2 | 7 | 6 | 11 | 0.730 |
| Surgery + RT | 35 | 40 | 13 | 43 | 22 | 39 | ||
| Surgery + RCT | 37 | 42 | 12 | 40 | 25 | 44 | ||
| RT only | 3 | 3 | 2 | 7 | 1 | 2 | ||
| RCT only | 4 | 5 | 1 | 3 | 3 | 5 | ||
| unknown | 1 | 1 | 1 | - | ||||
| Median follow-up (years) | 2.8 | 5.3 | 1.9 | N/A | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, S.; Langer, C.; Wuerdemann, N.; Reiser, S.; Abing, H.; Pons-Kühnemann, J.; Prigge, E.-S.; von Knebel Doeberitz, M.; Gattenlöhner, S.; Waterboer, T.; et al. Predictors for Survival of Patients with Squamous Cell Carcinoma of Unknown Primary in the Head and Neck Region. Cancers 2023, 15, 2167. https://doi.org/10.3390/cancers15072167
Wagner S, Langer C, Wuerdemann N, Reiser S, Abing H, Pons-Kühnemann J, Prigge E-S, von Knebel Doeberitz M, Gattenlöhner S, Waterboer T, et al. Predictors for Survival of Patients with Squamous Cell Carcinoma of Unknown Primary in the Head and Neck Region. Cancers. 2023; 15(7):2167. https://doi.org/10.3390/cancers15072167
Chicago/Turabian StyleWagner, Steffen, Christine Langer, Nora Wuerdemann, Susanne Reiser, Helen Abing, Jörn Pons-Kühnemann, Elena-Sophie Prigge, Magnus von Knebel Doeberitz, Stefan Gattenlöhner, Tim Waterboer, and et al. 2023. "Predictors for Survival of Patients with Squamous Cell Carcinoma of Unknown Primary in the Head and Neck Region" Cancers 15, no. 7: 2167. https://doi.org/10.3390/cancers15072167
APA StyleWagner, S., Langer, C., Wuerdemann, N., Reiser, S., Abing, H., Pons-Kühnemann, J., Prigge, E. -S., von Knebel Doeberitz, M., Gattenlöhner, S., Waterboer, T., Schroeder, L., Arens, C., Klussmann, J. P., & Wittekindt, C. (2023). Predictors for Survival of Patients with Squamous Cell Carcinoma of Unknown Primary in the Head and Neck Region. Cancers, 15(7), 2167. https://doi.org/10.3390/cancers15072167