


TP53 and/or BRCA1 Mutations Based on CtDNA Analysis as Prognostic Biomarkers for Primary Triple-Negative Breast Cancer
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Circulating Tumor DNA Extraction
2.3. Circulating Tumor DNA Sequencing
2.4. Statistical Analysis
3. Results
3.1. Flow Chart of Patient Enrollment and Clinicopathological Characteristics Associated with ctDNA Expression
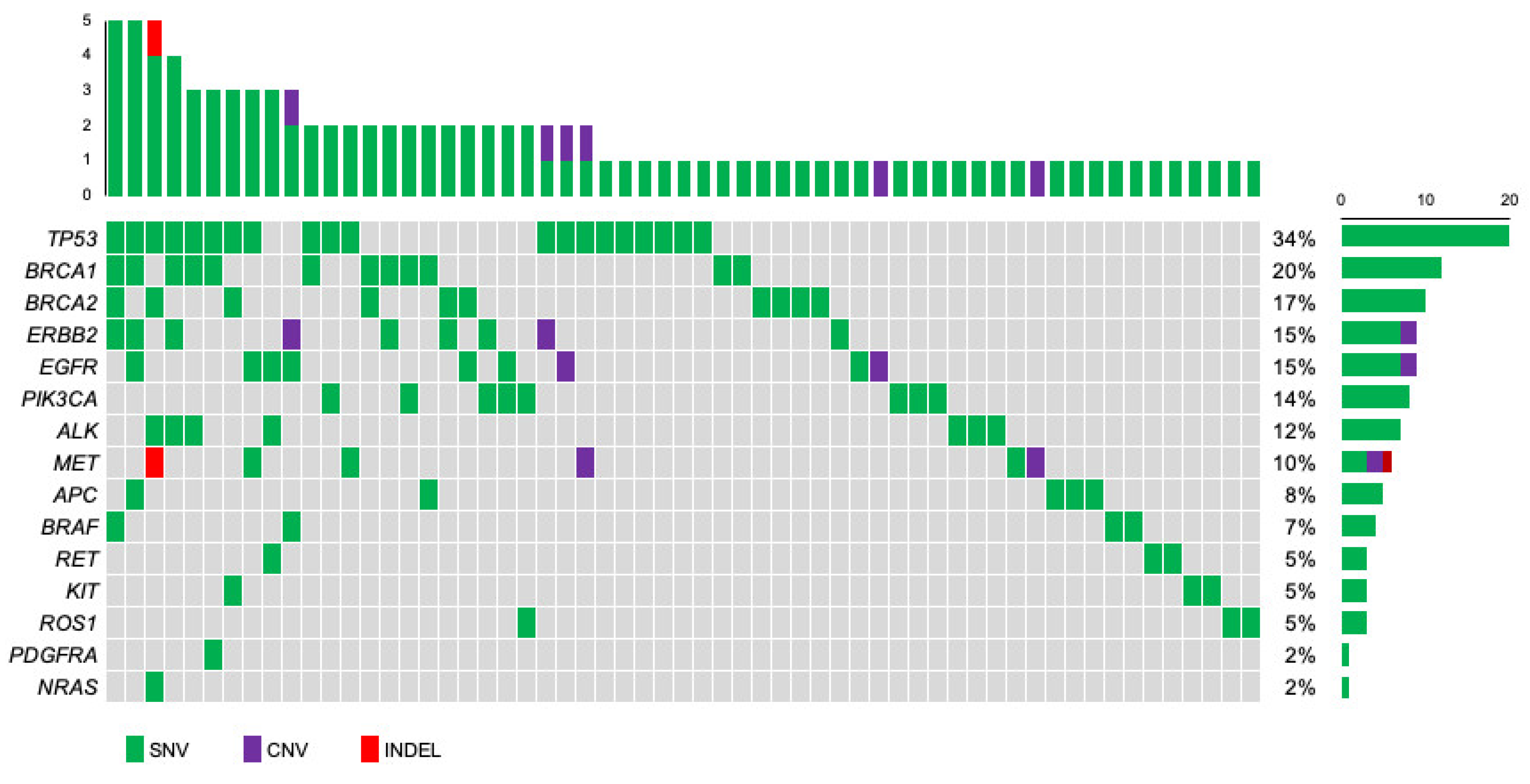
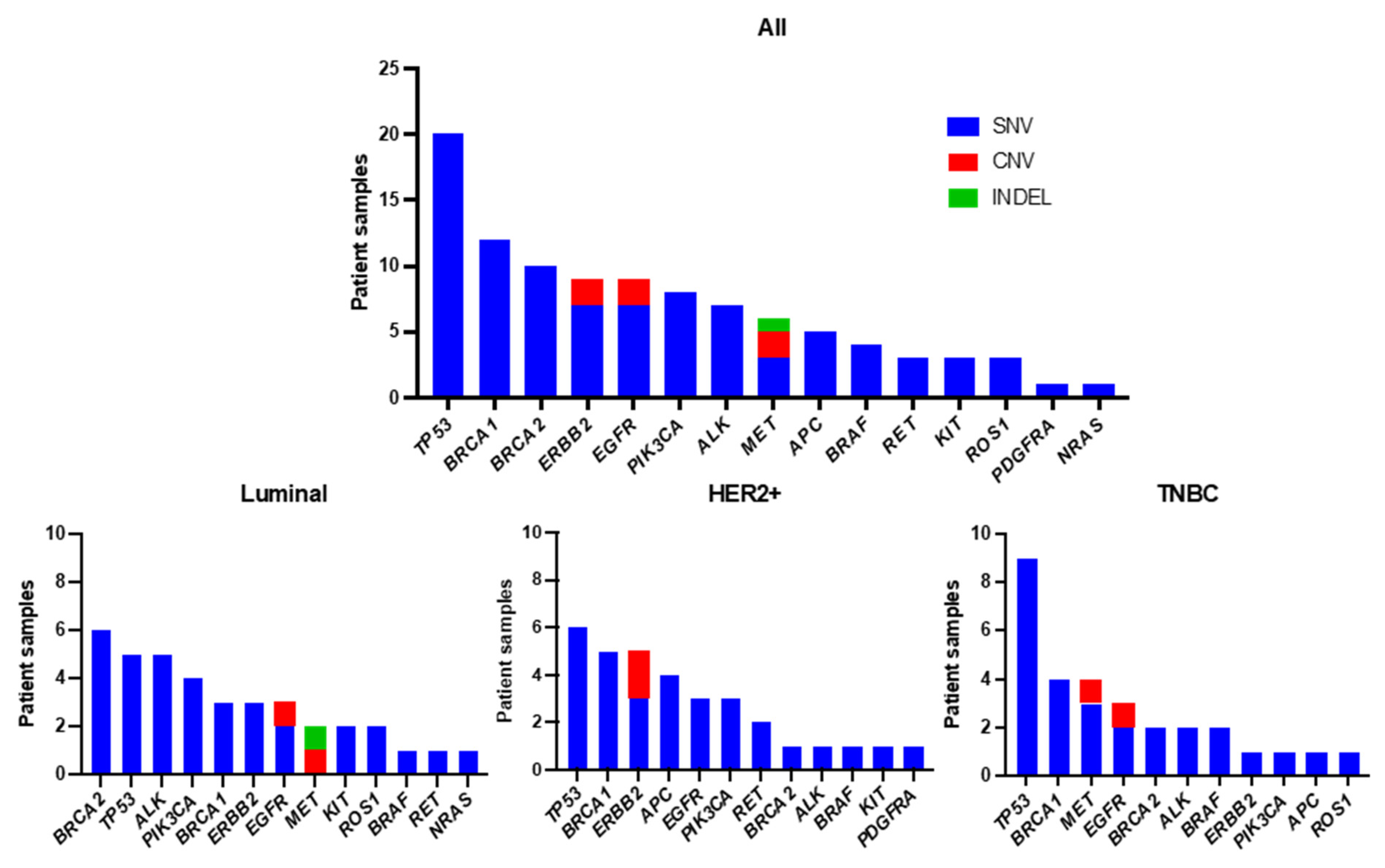
3.2. Profiling of Genetic Mutations in Breast Cancer Using CAPP-Seq
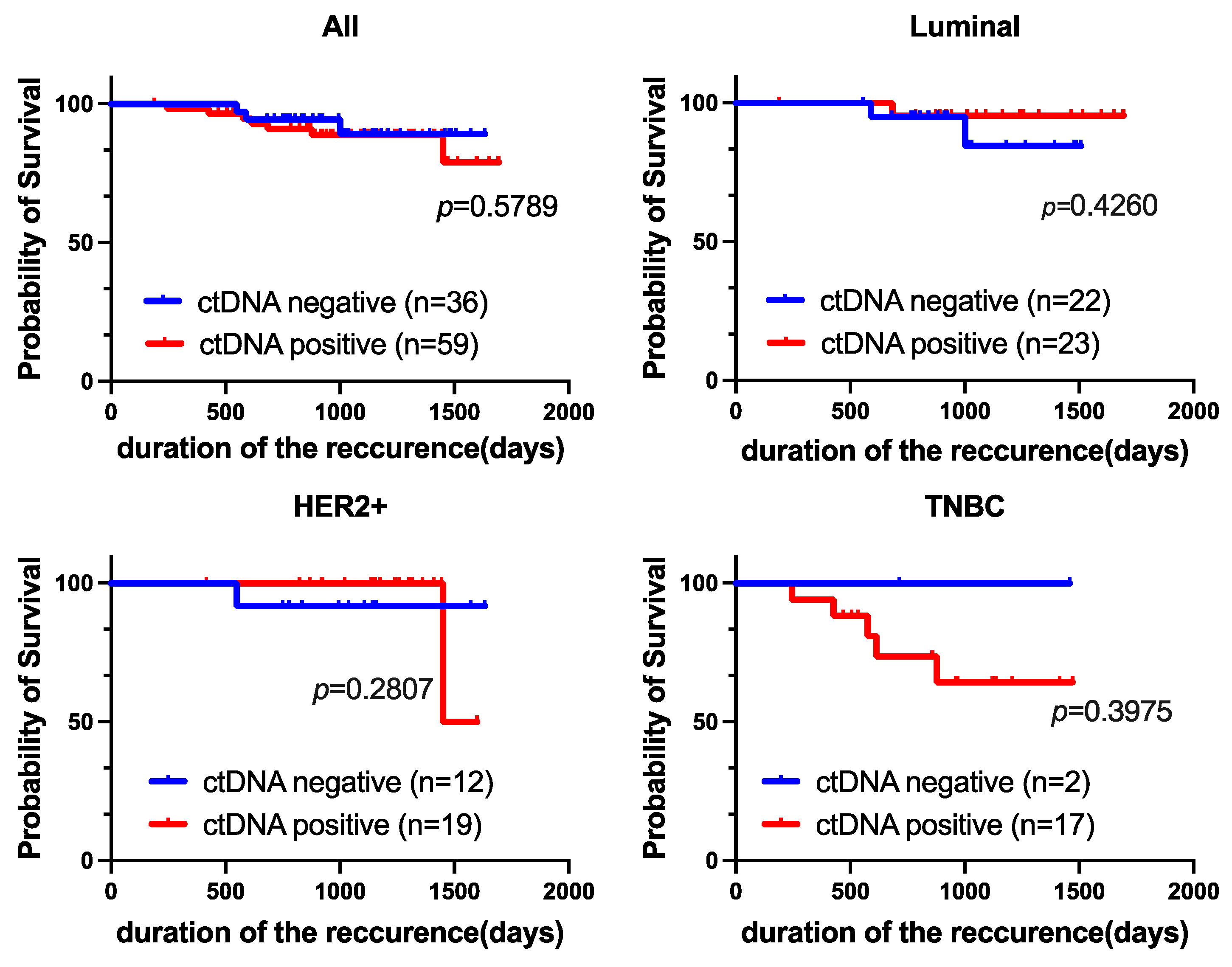
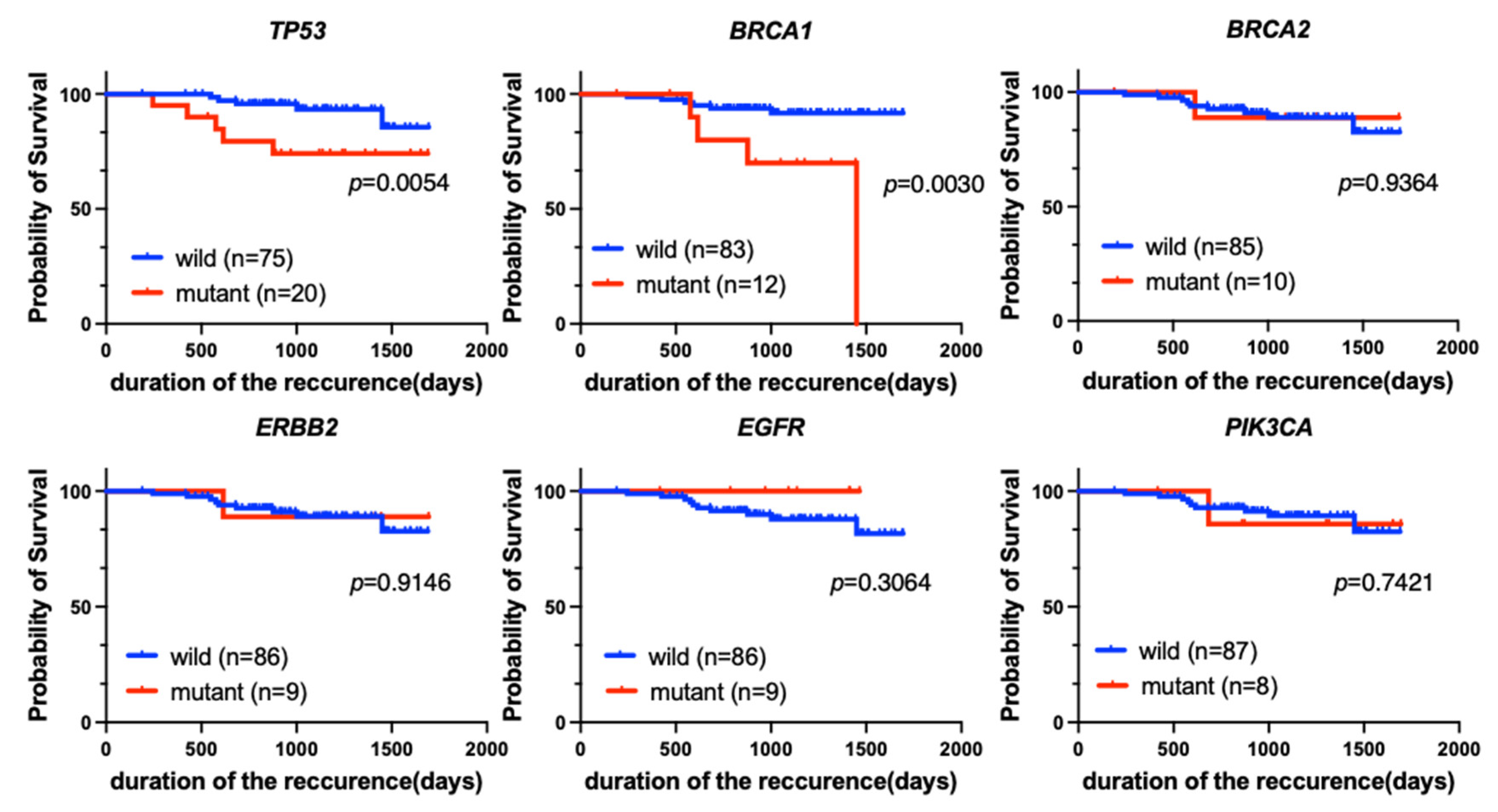
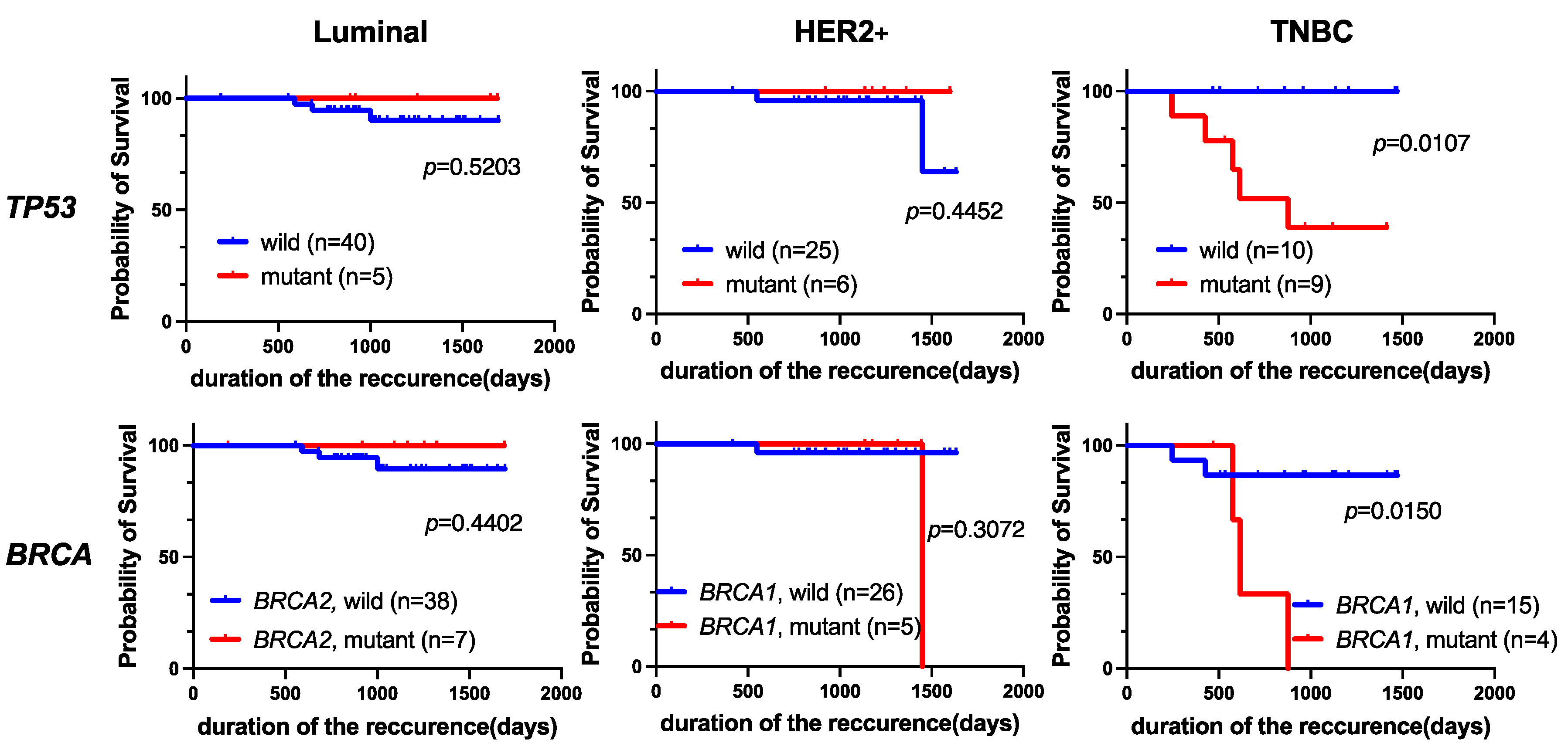
3.3. Patient Survival
3.4. Univariate and Multivariate Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Center for Cancer Control and Information Services of National Cancer Center, Japan. Available online: https://ganjoho.jp/reg_stat/index.html (accessed on 13 December 2023).
- Clinical Practice Guideline of Breast Cancer by the Japanese Breast Cancer Society, Version 3. 2022. Available online: https://jbcs.xsrv.jp/guideline/2022/ (accessed on 13 December 2023). (In Japanese).
- Clinical Practice Guidelines of Breast Cancer by American Society of Clinical Oncology. Available online: http://old-prod.asco.org/practice-patients/guidelines/breast-cancer (accessed on 13 December 2023).
- Clinical Practice Guidelines of Breast Cancer by European Society for Medical Oncology. Available online: http://www.esmo.org/guidelines (accessed on 13 December 2023).
- Clinical Practice Guidelines in Oncology of Breast Cancer by National Comprehensive Cancer Network, Version 5. 2023. Available online: http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 13 December 2023).
- Mahmoud, R.; Ordóñez-Morán, P.; Allegrucci, C. Challenges for Triple Negative Breast Cancer Treatment: Defeating Heterogeneity and Cancer Stemness. Cancers 2022, 14, 4280. [Google Scholar] [CrossRef]
- Bianchini, G.; Balko, J.M.; Mayer, I.A.; Sanders, M.E.; Gianni, L. Triple-negative breast cancer: Challenges and opportunities of a heterogeneous disease. Nat. Rev. Clin. Oncol. 2016, 13, 674–690. [Google Scholar] [CrossRef]
- Stratification of Prognosis of Triple-Negative Breast Cancer Patients Using Combinatorial Biomarkers. PLoS ONE 2016, 11, e0149661. [CrossRef]
- Liu, X.; Yue, S.; Huang, H.; Duan, M.; Zhao, B.; Liu, J.; Xiang, T. Risk Stratification Model for Predicting the Overall Survival of Elderly Triple-Negative Breast Cancer Patients: A Population-Based Study. Front. Med. 2021, 8, 705515. [Google Scholar] [CrossRef]
- Gibbs, S.N.; Peneva, D.; Cuyun Carter, G.; Palomares, M.R.; Thakkar, S.; Hall, D.W.; Dalglish, H.; Campos, C.; Yermilov, I. Comprehensive Review on the Clinical Impact of Next-Generation Sequencing Tests for the Management of Advanced Cancer. JCO Precis. Oncol. 2023, 7, e2200715. [Google Scholar] [CrossRef] [PubMed]
- Malone, E.R.; Oliva, M.; Sabatini, P.J.B.; Stockley, T.L.; Siu, L.L. Molecular profiling for precision cancer therapies. Genome Med. 2020, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Loong, H.H.; Shimizu, T.; Prawira, A.; Tan, A.C.; Tran, B.; Day, D.; Tan, D.S.P.; Ting, F.I.L.; Chiu, J.W.; Hui, M.; et al. Recommendations for the use of next-generation sequencing in patients with metastatic cancer in the Asia-Pacific region: A report from the APODDC working group. ESMO Open 2023, 8, 101586. [Google Scholar] [CrossRef] [PubMed]
- Guidance for Cancer Management Based on Genetic Panel Testing Using Next-Generation Sequencers and Other Methods, Version 2.1. 2020. Available online: https://www.jsmo.or.jp/about/doc/20200310.pdf (accessed on 13 December 2023). (In Japanese).
- Stewart, C.M.; Kothari, P.D.; Mouliere, F.; Mair, R.; Somnay, S.; Benayed, R.; Zehir, A.; Weigelt, B.; Dawson, S.J.; Arcila, M.E.; et al. The value of cell-free DNA for molecular pathology. J. Pathol. 2018, 244, 616–627. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Zhao, H. Next-generation sequencing in liquid biopsy: Cancer screening and early detection. Hum. Genom. 2019, 13, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.; Su, L.; Qian, C. Circulating tumor DNA: A promising biomarker in the liquid biopsy of cancer. Oncotarget 2016, 7, 48832–48841. [Google Scholar] [CrossRef]
- Sun, Y.; Haglund, T.A.; Rogers, A.J.; Ghanim, A.F.; Sethu, P. Review: Microfluidics technologies for blood-based cancer liquid biopsies. Anal. Chim. Acta 2018, 1012, 10–29. [Google Scholar] [CrossRef]
- Nakamura, Y.; Taniguchi, H.; Ikeda, M.; Bando, H.; Kato, K.; Morizane, C.; Esaki, T.; Komatsu, Y.; Kawamoto, Y.; Takahashi, N.; et al. Clinical utility of circulating tumor DNA sequencing in advanced gastrointestinal cancer: SCRUM-Japan GI-SCREEN and GOZILA studies. Nat. Med. 2020, 26, 1859–1864. [Google Scholar] [CrossRef]
- Turner, N.C.; Kingston, B.; Kilburn, L.S.; Kernaghan, S.; Wardley, A.M.; Macpherson, I.R.; Baird, R.D.; Roylance, R.; Stephens, P.; Oikonomidou, O.; et al. Circulating tumour DNA analysis to direct therapy in advanced breast cancer (plasmaMATCH): A multicentre, multicohort, phase 2a, platform trial. Lancet Oncol. 2020, 21, 1296–1308. [Google Scholar] [CrossRef]
- Fribbens, C.; O’Leary, B.; Kilburn, L.; Hrebien, S.; Garcia-Murillas, I.; Beaney, M.; Cristofanilli, M.; Andre, F.; Loi, S.; Loibl, S.; et al. Plasma ESR1 Mutations and the Treatment of Estrogen Receptor–Positive Advanced Breast Cancer. J. Clin. Oncol. 2016, 34, 2961–2968. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, B.; Hrebien, S.; Morden, J.P.; Beaney, M.; Fribbens, C.; Huang, X.; Liu, Y.; Bartlett, C.H.; Koehler, M.; Cristofanilli, M.; et al. Early circulating tumor DNA dynamics and clonal selection with palbociclib and fulvestrant for breast cancer. Nat. Commun. 2018, 9, 896. [Google Scholar] [CrossRef] [PubMed]
- André, F.; Ciruelos, E.; Rubovszky, G.; Campone, M.; Loibl, S.; Rugo, H.S.; Iwata, H.; Conte, P.; Mayer, I.A.; Kaufman, B.; et al. Alpelisib for PIK3CA-Mutated, Hormone Receptor-Positive Advanced Breast Cancer. N. Engl. J. Med. 2019, 380, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- Radovich, M.; Jiang, G.; Hancock, B.A.; Chitambar, C.; Nanda, R.; Falkson, C.; Lynce, F.C.; Gallagher, C.; Isaacs, C.; Blaya, M.; et al. Association of Circulating Tumor DNA and Circulating Tumor Cells After Neoadjuvant Chemotherapy with Disease Recurrence in Patients with Triple-Negative Breast Cancer: Preplanned Secondary Analysis of the BRE12-158 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1410–1415. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C.; Union for International Cancer Control (UICC). TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2017. [Google Scholar]
- Kurata, K.; Kubo, M.; Kai, M.; Mori, H.; Kawaji, H.; Kaneshiro, K.; Yamada, M.; Nishimura, R.; Osako, T.; Arima, N.; et al. Microsatellite instability in Japanese female patients with triple-negative breast cancer. Breast Cancer 2020, 27, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; Dowsett, M.; Fitzgibbons, P.L.; Hanna, W.M.; Langer, A.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J. Clin. Oncol. 2007, 25, 118–145. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef]
- Shimazaki, A.; Kubo, M.; Kurata, K.; Takao, Y.; Hayashi, S.; Harada, Y.; Kawaji, H.; Kaneshiro, K.; Yamada, M.; Kai, M.; et al. CCND1 Copy Number Variation in Circulating Tumor DNA from Luminal B Breast Cancer Patients. Anticancer Res. 2022, 42, 4071–4077. [Google Scholar] [CrossRef]
- Newman, A.M.; Bratman, S.V.; To, J.; Wynne, J.F.; Eclov, N.C.; Modlin, L.A.; Liu, C.L.; Neal, J.W.; Wakelee, H.A.; Merritt, R.E.; et al. An ultrasensitive method for quantitating circulating tumor DNA with broad patient coverage. Nat. Med. 2014, 20, 548–554. [Google Scholar] [CrossRef]
- Newman, A.M.; Lovejoy, A.F.; Klass, D.M.; Kurtz, D.M.; Chabon, J.J.; Scherer, F.; Stehr, H.; Liu, C.L.; Bratman, S.V.; Say, C.; et al. Integrated digital error suppression for improved detection of circulating tumor DNA. Nat. Biotechnol. 2016, 34, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Sunami, K.; Ichikawa, H.; Kubo, T.; Kato, M.; Fujiwara, Y.; Shimomura, A.; Koyama, T.; Kakishima, H.; Kitami, M.; Matsushita, H.; et al. Feasibility and utility of a panel testing for 114 cancer-associated genes in a clinical setting: A hospital-based study. Cancer Sci. 2019, 110, 1480–1490. [Google Scholar] [CrossRef]
- André, F.; Bachelot, T.; Commo, F.; Campone, M.; Arnedos, M.; Dieras, V.; Lacroix-Triki, M.; Lacroix, L.; Cohen, P.; Gentien, D.; et al. Comparative genomic hybridisation array and DNA sequencing to direct treatment of metastatic breast cancer: A multicentre, prospective trial (SAFIR01/UNICANCER). Lancet Oncol. 2014, 15, 267–274. [Google Scholar] [CrossRef]
- Lanman, R.B.; Mortimer, S.A.; Zill, O.A.; Sebisanovic, D.; Lopez, R.; Blau, S.; Collisson, E.A.; Divers, S.G.; Hoon, D.S.; Kopetz, E.S.; et al. Analytical and Clinical Validation of a Digital Sequencing Panel for Quantitative, Highly Accurate Evaluation of Cell-Free Circulating Tumor DNA. PLoS ONE 2015, 10, e0140712. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Gong, Y.; Lam, V.K.; Shi, Y.; Guan, Y.; Zhang, Y.; Ji, L.; Chen, Y.; Zhao, Y.; Qian, F.; et al. Deep sequencing of circulating tumor DNA detects molecular residual disease and predicts recurrence in gastric cancer. Cell Death Dis. 2020, 11, 346. [Google Scholar] [CrossRef] [PubMed]
- Symonds, E.L.; Pedersen, S.K.; Murray, D.; Byrne, S.E.; Roy, A.; Karapetis, C.; Hollington, P.; Rabbitt, P.; Jones, F.S.; LaPointe, L.; et al. Circulating epigenetic biomarkers for detection of recurrent colorectal cancer. Cancer 2020, 126, 1460–1469. [Google Scholar] [CrossRef]
- Osumi, H.; Shinozaki, E.; Takeda, Y.; Wakatsuki, T.; Ichimura, T.; Saiura, A.; Yamaguchi, K.; Takahashi, S.; Noda, T.; Zembutsu, H. Clinical relevance of circulating tumor DNA assessed through deep sequencing in patients with metastatic colorectal cancer. Cancer Med. 2019, 8, 408–417. [Google Scholar] [CrossRef]
- Garcia-Murillas, I.; Chopra, N.; Comino-Méndez, I.; Beaney, M.; Tovey, H.; Cutts, R.J.; Swift, C.; Kriplani, D.; Afentakis, M.; Hrebien, S.; et al. Assessment of Molecular Relapse Detection in Early-Stage Breast Cancer. JAMA Oncol. 2019, 5, 1473–1478. [Google Scholar] [CrossRef]
- Mendiratta, G.; Ke, E.; Aziz, M.; Liarakos, D.; Tong, M.; Stites, E.C. Cancer gene mutation frequencies for the U.S. population. Nat. Commun. 2021, 12, 5961. [Google Scholar] [CrossRef]
- Xiao, W.; Zhang, G.; Chen, B.; Chen, X.; Wen, L.; Lai, J.; Li, X.; Li, M.; Liu, H.; Liu, J.; et al. Characterization of Frequently Mutated Cancer Genes and Tumor Mutation Burden in Chinese Breast Cancer. Front. Oncol. 2021, 11, 618767. [Google Scholar] [CrossRef]
- Network, C.G.A. Comprehensive molecular portraits of human breast tumours. Nature 2012, 490, 61–70. [Google Scholar] [CrossRef]
- Cullinane, C.; Fleming, C.; O’Leary, D.P.; Hassan, F.; Kelly, L.; O’Sullivan, M.J.; Corrigan, M.A.; Redmond, H.P. Association of Circulating Tumor DNA With Disease-Free Survival in Breast Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2026921. [Google Scholar] [CrossRef]
- Zhu, W.; Ren, C.; Wang, Y.; Wen, L.; Zhang, G.; Liao, N. Prevalence of ESR1 Mutation in Chinese ER-Positive Breast Cancer. Onco Targets Ther. 2020, 13, 615–621. [Google Scholar] [CrossRef]
- Yi, Z.; Ma, F.; Rong, G.; Guan, Y.; Li, C.; Xu, B. Clinical spectrum and prognostic value of TP53 mutations in circulating tumor DNA from breast cancer patients in China. Cancer Commun. 2020, 40, 260–269. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, K.; Jung, H.H.; Lee, E.; Cho, E.Y.; Lee, K.H.; Bae, S.Y.; Lee, S.K.; Kim, S.W.; Lee, J.E.; et al. Association between Mutation and Expression of TP53 as a Potential Prognostic Marker of Triple-Negative Breast Cancer. Cancer Res. Treat. 2016, 48, 1338–1350. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.; Im, S.A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef]
- Indovina, P.; Giordano, A. Targeting the checkpoint kinase WEE1: Selective sensitization of cancer cells to DNA-damaging drugs. Cancer Biol. Ther. 2010, 9, 523–525. [Google Scholar] [CrossRef] [PubMed]
- Hirai, H.; Arai, T.; Okada, M.; Nishibata, T.; Kobayashi, M.; Sakai, N.; Imagaki, K.; Ohtani, J.; Sakai, T.; Yoshizumi, T.; et al. MK-1775, a small molecule Wee1 inhibitor, enhances anti-tumor efficacy of various DNA-damaging agents, including 5-fluorouracil. Cancer Biol. Ther. 2010, 9, 514–522. [Google Scholar] [CrossRef]
- Liu, J.F.; Xiong, N.; Campos, S.M.; Wright, A.A.; Krasner, C.; Schumer, S.; Horowitz, N.; Veneris, J.; Tayob, N.; Morrissey, S.; et al. Phase II Study of the WEE1 Inhibitor Adavosertib in Recurrent Uterine Serous Carcinoma. J. Clin. Oncol. 2021, 39, 1531–1539. [Google Scholar] [CrossRef] [PubMed]
- Ku, B.M.; Bae, Y.H.; Koh, J.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; Park, K.; Ahn, M.J. Mutational status of TP53 defines the efficacy of Wee1 inhibitor AZD1775 in KRAS-mutant non-small cell lung cancer. Oncotarget 2017, 8, 67526–67537. [Google Scholar] [CrossRef] [PubMed]
- Miyake, K.; Takano, N.; Kazama, H.; Kikuchi, H.; Hiramoto, M.; Tsukahara, K.; Miyazawa, K. Ricolinostat enhances adavosertib-induced mitotic catastrophe in TP53-mutated head and neck squamous cell carcinoma cells. Int. J. Oncol. 2022, 60, 54. [Google Scholar] [CrossRef] [PubMed]
- Dent, R.; Trudeau, M.; Pritchard, K.I.; Hanna, W.M.; Kahn, H.K.; Sawka, C.A.; Lickley, L.A.; Rawlinson, E.; Sun, P.; Narod, S.A. Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin. Cancer Res. 2007, 13 Pt 1, 4429–4434. [Google Scholar] [CrossRef]
- Carey, L.A.; Dees, E.C.; Sawyer, L.; Gatti, L.; Moore, D.T.; Collichio, F.; Ollila, D.W.; Sartor, C.I.; Graham, M.L.; Perou, C.M. The triple negative paradox: Primary tumor chemosensitivity of breast cancer subtypes. Clin. Cancer Res. 2007, 13, 2329–2334. [Google Scholar] [CrossRef]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; André, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M.; et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J. Clin. Oncol. 2008, 26, 1275–1281. [Google Scholar] [CrossRef]
- Saphner, T.; Tormey, D.C.; Gray, R. Annual hazard rates of recurrence for breast cancer after primary therapy. J. Clin. Oncol. 1996, 14, 2738–2746. [Google Scholar] [CrossRef]
- Kiba, T.; Inamoto, T.; Nishimura, T.; Ueno, M.; Yanagihara, K.; Teramukai, S.; Kato, H.; Toi, M.; Fukushima, M. The reversal of recurrence hazard rate between ER positive and negative breast cancer patients with axillary lymph node dissection (pathological stage I-III) 3 years after surgery. BMC Cancer 2008, 8, 323. [Google Scholar] [CrossRef]
- Patel, J.M.; Goss, A.; Garber, J.E.; Torous, V.; Richardson, E.T.; Haviland, M.J.; Hacker, M.R.; Freeman, G.J.; Nalven, T.; Alexander, B.; et al. Retinoblastoma protein expression and its predictors in triple-negative breast cancer. NPJ Breast Cancer 2020, 6, 19. [Google Scholar] [CrossRef]
- Baselga, J.; Im, S.A.; Iwata, H.; Cortés, J.; De Laurentiis, M.; Jiang, Z.; Arteaga, C.L.; Jonat, W.; Clemons, M.; Ito, Y.; et al. Buparlisib plus fulvestrant versus placebo plus fulvestrant in postmenopausal, hormone receptor-positive, HER2-negative, advanced breast cancer (BELLE-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2017, 18, 904–916. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ctDNA Positive | ctDNA Negative | p | |||
|---|---|---|---|---|---|
| n = 59 (62.1%) | n = 36 (37.9%) | ||||
| Age at diagnosis | |||||
| Median (range) | 62 | (33–91) | 54 | (33–84) | 0.0138 |
| Tumor size | |||||
| T1 (≤2 cm) | 21 | (35.6%) | 14 | (38.9%) | 0.4880 |
| T2 (>2 cm, ≤5 cm) | 30 | (50.8%) | 18 | (50.0%) | |
| T3 (>5 cm) | 5 | (8.5%) | 4 | (11.1%) | |
| T4 | 3 | (5.1%) | |||
| Nodal status | |||||
| Negative | 24 | (40.7%) | 20 | (55.6%) | 0.1583 |
| Positive | 35 | (59.3%) | 16 | (44.4%) | |
| Clinical stage | |||||
| I | 16 | (27.1%) | 12 | (33.3%) | 0.0345 |
| II | 28 | (47.5%) | 22 | (61.1%) | |
| III | 15 | (25.4%) | 2 | (5.6%) | |
| HR status | |||||
| Positive | 35 | (59.3%) | 31 | (86.1%) | 0.0059 |
| Negative | 24 | (40.7%) | 5 | (13.9%) | |
| HER2 overexpression | |||||
| Positive | 19 | (32.2%) | 12 | (33.3%) | 0.9093 |
| Negative | 40 | (67.8%) | 24 | (66.7%) | |
| Nuclear grade | |||||
| 1 | 15 | (25.4%) | 8 | (22.2%) | 0.7899 |
| 2 | 13 | (22.1%) | 9 | (25.0%) | |
| 3 | 30 | (50.8%) | 19 | (52.8%) | |
| Unknown | 1 | (1.7%) | |||
| Ki67 levels | 0.6962 | ||||
| ≤20% | 25 | (42.4%) | 17 | (47.2%) | |
| >20% | 33 | (55.9%) | 19 | (52.8%) | |
| Unknown | 1 | (1.7%) | |||
| Subtypes | |||||
| Luminal | 23 | (39.0%) | 22 | (61.1%) | 0.0254 |
| Luminal/HER2 | 12 | (20.3%) | 9 | (25.0%) | |
| HER2 | 7 | (11.9%) | 3 | (8.3%) | |
| TNBC | 17 | (28.8%) | 2 | (5.6%) | |
| Tumor marker | |||||
| Positive | 23 | (39.0%) | (16.7%) | 0.0190 | |
| Negative | 35 | (59.3%) | (83.3%) | ||
| Unknown | 1 | (1.7%) | |||
| Relapse | |||||
| Yes | 7 | (11.9%) | 3 | (8.3%) | 0.5864 |
| No | 52 | (88.1%) | 33 | (91.7%) | |
| A. Univariate Analysis | ||||
| Recurrence-Free Survival | ||||
| HR | 95% CI | p-Value | ||
| Age | (>50 vs. ≤50) | 0.5 | 0.1–1.7 | 0.295 |
| Tumor size | (>2 cm vs. ≤2 cm) | 5.6 | 0.7–43.9 | 0.104 |
| Nodal status | (Positive vs. Negative) | 1.4 | 0.4–5.0 | 0.599 |
| Nuclear grade | (3 vs. 1 and 2) | 1.4 | 0.4–5.0 | 0.587 |
| Ki67 | (>20% vs. ≤20%) | 1.3 | 0.6–1.5 | 0.726 |
| HR status | (Positive vs. Negative) | 0.3 | 0.09–1.1 | 0.072 |
| HER2 status | (Positive vs. Negative) | 0.5 | 0.1–2.2 | 0.353 |
| Subtype | (TNBC vs. non-TNBC) | 5.5 | 1.6–19.0 | 0.0075 |
| Tumor marker | (Positive vs. Negative) | 1.5 | 0.4–5.2 | 0.565 |
| ctDNA | (Positive vs. Negative) | 1.4 | 0.4–5.6 | 0.581 |
| TP53 | (mutant vs. wild-type) | 4.0 | 1.2–13.9 | 0.028 |
| BRCA1 | (mutant vs. wild-type) | 5.5 | 1.6–19.7 | 0.0083 |
| B. Multivariate Analysis | ||||
| Recurrence-Free Survival | ||||
| HR | 95% CI | p-Value | ||
| Tumor size | (>2 cm vs. ≤2 cm) | 4.7 | 0.5–42.3 | 0.165 |
| Nodal status | (Positive vs. Negative) | 1.4 | 0.4–5.3 | 0.621 |
| Subtype | (TNBC vs. non-TNBC) | 4.1 | 1.1–15.2 | 0.038 |
| TP53 | (mutant vs. wild-type) | 1.9 | 0.5–8.0 | 0.38 |
| BRCA1 | (mutant vs. wild-type) | 2.9 | 0.7–13.0 | 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arimura, A.; Sakai, K.; Kaneshiro, K.; Morisaki, T.; Hayashi, S.; Mizoguchi, K.; Yamada, M.; Kai, M.; Ono, M.; Nishio, K.; et al. TP53 and/or BRCA1 Mutations Based on CtDNA Analysis as Prognostic Biomarkers for Primary Triple-Negative Breast Cancer. Cancers 2024, 16, 1184. https://doi.org/10.3390/cancers16061184
Arimura A, Sakai K, Kaneshiro K, Morisaki T, Hayashi S, Mizoguchi K, Yamada M, Kai M, Ono M, Nishio K, et al. TP53 and/or BRCA1 Mutations Based on CtDNA Analysis as Prognostic Biomarkers for Primary Triple-Negative Breast Cancer. Cancers. 2024; 16(6):1184. https://doi.org/10.3390/cancers16061184
Chicago/Turabian StyleArimura, Akiko, Kazuko Sakai, Kazuhisa Kaneshiro, Takafumi Morisaki, Saori Hayashi, Kimihisa Mizoguchi, Mai Yamada, Masaya Kai, Mayumi Ono, Kazuto Nishio, and et al. 2024. "TP53 and/or BRCA1 Mutations Based on CtDNA Analysis as Prognostic Biomarkers for Primary Triple-Negative Breast Cancer" Cancers 16, no. 6: 1184. https://doi.org/10.3390/cancers16061184
APA StyleArimura, A., Sakai, K., Kaneshiro, K., Morisaki, T., Hayashi, S., Mizoguchi, K., Yamada, M., Kai, M., Ono, M., Nishio, K., Nakamura, M., & Kubo, M. (2024). TP53 and/or BRCA1 Mutations Based on CtDNA Analysis as Prognostic Biomarkers for Primary Triple-Negative Breast Cancer. Cancers, 16(6), 1184. https://doi.org/10.3390/cancers16061184