
Metastatic Breast Cancer: Prolonging Life in Routine Oncology Care

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient and Tumor Characteristics
3.2. Treatment
3.2.1. Hormone-Receptor-Positive Tumors
3.2.2. HER2-Positive Tumors
3.2.3. Triple-Negative Tumors
3.2.4. Triple-Positive Tumors
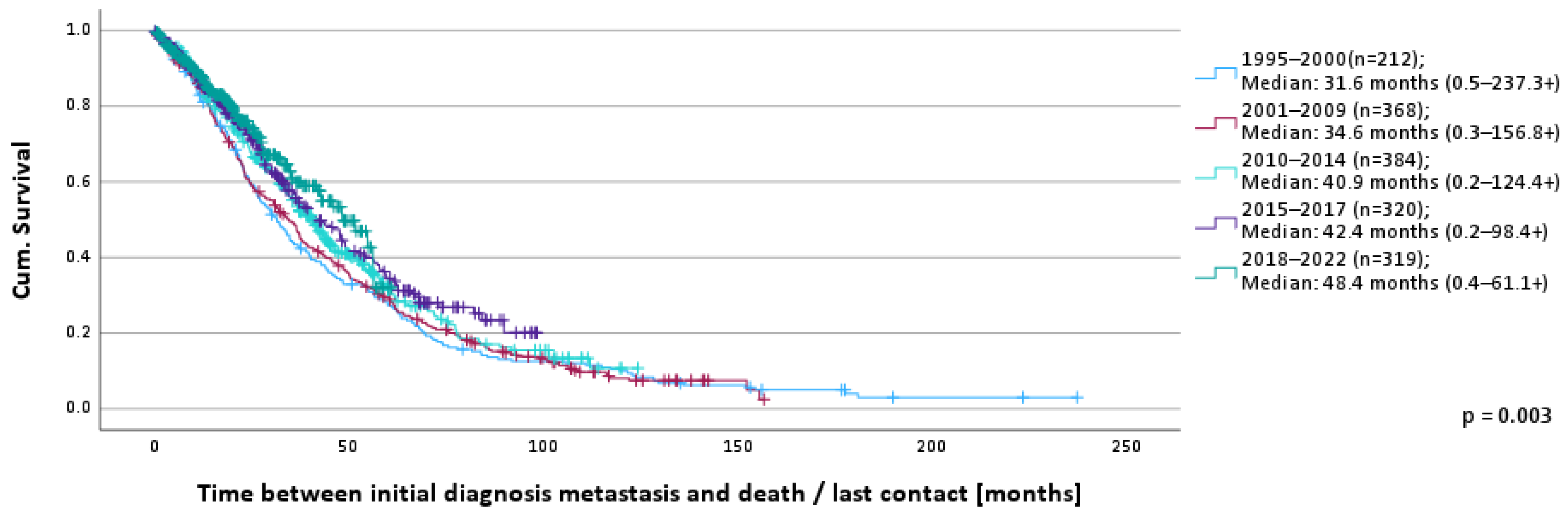
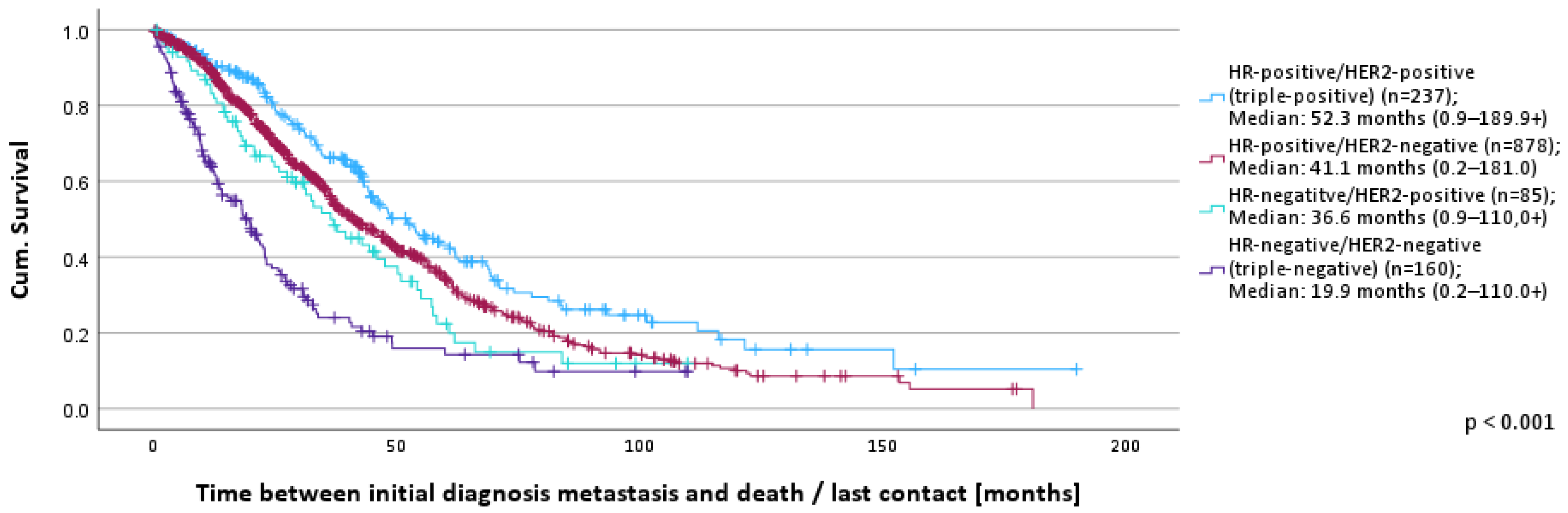
3.3. Overall Survival
4. Discussion
4.1. Hormone-Receptor-Positive Tumors
4.2. HER2-Positive Tumors
4.3. Triple-Negative Tumors
4.4. Triple-Positive Tumors
4.5. Patients with Brain Metastases
4.6. Strengths and Limitations of Our Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Riemsma, R.; Forbes, C.A.; Kessels, A.; Lykopoulos, K.; Amonkar, M.M.; Rea, D.W.; Kleijnen, J. Systematic review of aromatase inhibitors in the first-line treatment for hormone sensitive advanced or metastatic breast cancer. Breast Cancer Res. Treat. 2010, 123, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.I.; Goodwin, A.; Wilcken, N. Fulvestrant for hormone-sensitive metastatic breast cancer. Cochrane Database Syst. Rev. 2017, 1, Cd011093. [Google Scholar] [CrossRef] [PubMed]
- De Groot, A.F.; Kuijpers, C.J.; Kroep, J.R. CDK4/6 inhibition in early and metastatic breast cancer: A review. Cancer Treat. Rev. 2017, 60, 130–138. [Google Scholar] [CrossRef]
- Baselga, J.; Campone, M.; Piccart, M.; Burris, H.A., 3rd; Rugo, H.S.; Sahmoud, T.; Noguchi, S.; Gnant, M.; Pritchard, K.I.; Lebrun, F.; et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N. Engl. J. Med. 2012, 366, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger-Raab, A.; Eckel, R.; Engel, J.; Sauer, H.; Löhrs, U.; Molls, M.; Hölzel, D. Metastasiertes Mammakarzinom: Keine Lebensverlängerung seit 20 Jahren. Dtsch. Arztebl. 2005, 102, 2706–2714. [Google Scholar]
- Caswell-Jin, J.L.; Plevritis, S.K.; Tian, L.; Cadham, C.J.; Xu, C.; Stout, N.K.; Sledge, G.W.; Mandelblatt, J.S.; Kurian, A.W. Change in Survival in Metastatic Breast Cancer with Treatment Advances: Meta-Analysis and Systematic Review. JNCI Cancer Spectr. 2018, 2, pky062. [Google Scholar] [CrossRef]
- Sundquist, M.; Brudin, L.; Tejler, G. Improved survival in metastatic breast cancer 1985–2016. Breast 2017, 31, 46–50. [Google Scholar] [CrossRef]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef]
- Valachis, A.; Carlqvist, P.; Ma, Y.; Szilcz, M.; Freilich, J.; Vertuani, S.; Holm, B.; Lindman, H. Overall survival of patients with metastatic breast cancer in Sweden: A nationwide study. Br. J. Cancer 2022, 127, 720–725. [Google Scholar] [CrossRef]
- American Cancer Society. Survival Rates for Breast Cancer. Available online: https://www.cancer.org/cancer/types/breast-cancer/understanding-a-breast-cancer-diagnosis/breast-cancer-survival-rates.html (accessed on 12 July 2023).
- Thill, M.; Lüftner, D.; Kolberg-Liedtke, C.; Albert, U.S.; Banys-Paluchowski, M.; Bauerfeind, I.; Blohmer, J.U.; Budach, W.; Dall, P.; Fallenberg, E.M.; et al. AGO Recommendations for the Diagnosis and Treatment of Patients with Locally Advanced and Metastatic Breast Cancer: Update 2022. Breast Care 2022, 17, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Rugo, H.S.; Cescon, D.W.; Im, S.A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Perez-Garcia, J.; Iwata, H.; et al. Pembrolizumab plus Chemotherapy in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2022, 387, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Hurvitz, S.A.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Sardesai, S.D.; Kalinsky, K.; Zelnak, A.B.; et al. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N. Engl. J. Med. 2021, 384, 1529–1541. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; Nathan, H. Strengths and Limitations of Registries in Surgical Oncology Research. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2021, 25, 2989–2996. [Google Scholar] [CrossRef] [PubMed]
- Burstein, H.J.; Somerfield, M.R.; Barton, D.L.; Dorris, A.; Fallowfield, L.J.; Jain, D.; Johnston, S.R.D.; Korde, L.A.; Litton, J.K.; Macrae, E.R.; et al. Endocrine Treatment and Targeted Therapy for Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 3959–3977. [Google Scholar] [CrossRef] [PubMed]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.S.; Sonke, G.S.; Hart, L.; Campone, M.; Petrakova, K.; Winer, E.P.; Janni, W.; et al. Overall Survival with Ribociclib plus Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2022, 386, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.-S.; Mahidin, E.; Azim, H.; Eralp, Y.; Yap, Y.-S.; Im, S.-A.; Rihani, J.; Bowles, J.; Alfaro, T.; Wu, J.; et al. Abstract GS1-10: Primary results from the randomized Phase II RIGHT Choice trial of premenopausal patients with aggressive HR+/HER2− advanced breast cancer treated with ribociclib + endocrine therapy vs physician’s choice combination chemotherapy. Cancer Res. 2023, 83, GS1-10. [Google Scholar] [CrossRef]
- Lipsyc-Sharf, M.; Tolaney, S.M. Elacestrant: Who are optimal candidates for the first oral SERD? Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2023, 34, 449–451. [Google Scholar] [CrossRef]
- Bidard, F.C.; Kaklamani, V.G.; Neven, P.; Streich, G.; Montero, A.J.; Forget, F.; Mouret-Reynier, M.A.; Sohn, J.H.; Taylor, D.; Harnden, K.K.; et al. Elacestrant (oral selective estrogen receptor degrader) Versus Standard Endocrine Therapy for Estrogen Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer: Results from the Randomized Phase III EMERALD Trial. J. Clin. Oncol. 2022, 40, 3246–3256. [Google Scholar] [CrossRef]
- Rugo, H.S.; Bardia, A.; Marmé, F.; Cortes, J.; Schmid, P.; Loirat, D.; Trédan, O.; Ciruelos, E.; Dalenc, F.; Pardo, P.G.; et al. Sacituzumab Govitecan in Hormone Receptor-Positive/Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer. J. Clin. Oncol. 2022, 40, 3365–3376. [Google Scholar] [CrossRef]
- Swain, S.M.; Baselga, J.; Kim, S.B.; Ro, J.; Semiglazov, V.; Campone, M.; Ciruelos, E.; Ferrero, J.M.; Schneeweiss, A.; Heeson, S.; et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N. Engl. J. Med. 2015, 372, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [PubMed]
- Cortés, J.; Kim, S.B.; Chung, W.P.; Im, S.A.; Park, Y.H.; Hegg, R.; Kim, M.H.; Tseng, L.M.; Petry, V.; Chung, C.F.; et al. Trastuzumab Deruxtecan versus Trastuzumab Emtansine for Breast Cancer. N. Engl. J. Med. 2022, 386, 1143–1154. [Google Scholar] [CrossRef] [PubMed]
- Murthy, R.K.; Loi, S.; Okines, A.; Paplomata, E.; Hamilton, E.; Hurvitz, S.A.; Lin, N.U.; Borges, V.; Abramson, V.; Anders, C.; et al. Tucatinib, Trastuzumab, and Capecitabine for HER2-Positive Metastatic Breast Cancer. N. Engl. J. Med. 2020, 382, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Sáez, O.; Prat, A. Current and Future Management of HER2-Positive Metastatic Breast Cancer. JCO Oncol. Pract. 2021, 17, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Triple-negative Breast Cancer. Available online: https://www.cancer.org/cancer/types/breast-cancer/about/types-of-breast-cancer/triple-negative.html (accessed on 12 July 2023).
- Weide, R.; Feiten, S.; Friesenhahn, V.; Heymanns, J.; Kleboth, K.; Thomalla, J.; van Roye, C.; Koppler, H. Metastatic breast cancer: Prolongation of survival in routine care is restricted to hormone-receptor- and Her2-positive tumors. SpringerPlus 2014, 3, 535. [Google Scholar] [CrossRef]
- Thanopoulou, E.; Khader, L.; Caira, M.; Wardley, A.; Ettl, J.; Miglietta, F.; Neven, P.; Guarneri, V. Therapeutic Strategies for the Management of Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Positive (HR+/HER2+) Breast Cancer: A Review of the Current Literature. Cancers 2020, 12, 3317. [Google Scholar] [CrossRef]
- Rimawi, M.; Ferrero, J.M.; de la Haba-Rodriguez, J.; Poole, C.; De Placido, S.; Osborne, C.K.; Hegg, R.; Easton, V.; Wohlfarth, C.; Arpino, G.; et al. First-Line Trastuzumab Plus an Aromatase Inhibitor, With or Without Pertuzumab, in Human Epidermal Growth Factor Receptor 2-Positive and Hormone Receptor-Positive Metastatic or Locally Advanced Breast Cancer (PERTAIN): A Randomized, Open-Label Phase II Trial. J. Clin. Oncol. 2018, 36, 2826–2835. [Google Scholar] [CrossRef]
- Johnston, S.R.D.; Hegg, R.; Im, S.A.; Park, I.H.; Burdaeva, O.; Kurteva, G.; Press, M.F.; Tjulandin, S.; Iwata, H.; Simon, S.D.; et al. Phase III, Randomized Study of Dual Human Epidermal Growth Factor Receptor 2 (HER2) Blockade With Lapatinib Plus Trastuzumab in Combination With an Aromatase Inhibitor in Postmenopausal Women With HER2-Positive, Hormone Receptor-Positive Metastatic Breast Cancer: Updated Results of ALTERNATIVE. J. Clin. Oncol. 2021, 39, 79–89. [Google Scholar] [CrossRef]
- Yuan, Z.; Huang, J.-J.; Hua, X.; Zhao, J.-L.; Lin, Y.; Zhang, Y.-Q.; Wu, Z.; Zhang, L.; Bi, X.; Xia, W.; et al. Trastuzumab plus endocrine therapy or chemotherapy as first-line treatment for metastatic breast cancer with hormone receptor-positive and HER2-positive: The sysucc-002 randomized clinical trial. J. Clin. Oncol. 2021, 39, 1003. [Google Scholar] [CrossRef]
- Arbeitsgemeinchaft Gynäkologische Onkologie, Leitlinien und Empfehlungen/Guidelines. Available online: https://www.ago-online.de/leitlinien-empfehlungen/leitlinien-empfehlungen/kommission-mamma (accessed on 11 March 2024).
- Riecke, K.; Müller, V.; Neunhöffer, T.; Park-Simon, T.W.; Weide, R.; Polasik, A.; Schmidt, M.; Puppe, J.; Mundhenke, C.; Lübbe, K.; et al. Long-term survival of breast cancer patients with brain metastases: Subanalysis of the BMBC registry. ESMO Open 2023, 8, 101213. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Year of Initial Diagnosis Metastasis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1995–2000 | 2001–2009 | 2010–2014 | 2015–2017 | 2018–2022 | |||||||||
| Age at initial diagnosis metastasis | 50 years or younger | 315 | 19.6% | 66 | 31.0% | 65 | 17.6% | 63 | 16.3% | 59 | 18.3% | 62 | 19.4% |
| 51–60 years | 394 | 24.5% | 55 | 25.8% | 105 | 28.4% | 93 | 24.1% | 76 | 23.6% | 65 | 20.4% | |
| 61–70 years | 423 | 26.3% | 52 | 24.4% | 112 | 30.3% | 95 | 24.6% | 78 | 24.2% | 86 | 27.0% | |
| 71 years or older | 478 | 29.7% | 40 | 18.8% | 88 | 23.8% | 135 | 35.0% | 109 | 33.9% | 106 | 33.2% | |
| ECOG performance status at first presentation | ECOG 0–1 | 1005 | 86.1% | 90 | 97.8% | 185 | 89.8% | 259 | 86.0% | 207 | 82.8% | 264 | 83.0% |
| ECOG 2–4 | 162 | 13.9% | 2 | 2.2% | 21 | 10.2% | 42 | 14.0% | 43 | 17.2% | 54 | 17.0% | |
| Age-adjusted Charlson Comorbidity Index (aaCCI) at first presentation | aaCCI = 6 | 253 | 15.8% | 57 | 26.8% | 59 | 16.0% | 39 | 10.2% | 46 | 14.4% | 52 | 16.4% |
| aaCCI = 7 | 346 | 21.6% | 53 | 24.9% | 86 | 23.3% | 77 | 20.1% | 70 | 21.9% | 60 | 18.9% | |
| aaCCI = 8 | 336 | 21.0% | 42 | 19.7% | 94 | 25.5% | 73 | 19.1% | 56 | 17.5% | 71 | 22.3% | |
| aaCCI > 8 | 668 | 41.7% | 61 | 28.6% | 130 | 35.2% | 194 | 50.7% | 148 | 46.3% | 135 | 42.5% | |
| Grading at first presentation | G1 | 50 | 3.1% | 7 | 3.3% | 11 | 3.0% | 9 | 2.3% | 10 | 3.1% | 13 | 4.1% |
| G2 | 768 | 47.7% | 99 | 46.5% | 144 | 38.9% | 197 | 51.0% | 158 | 49.1% | 170 | 53.3% | |
| G3 | 586 | 36.4% | 77 | 36.2% | 166 | 44.9% | 117 | 30.3% | 111 | 34.5% | 115 | 36.1% | |
| GX | 45 | 2.8% | 19 | 8.9% | 13 | 3.5% | 9 | 2.3% | 4 | 1.2% | 0 | 0.0% | |
| not evaluable | 161 | 10.0% | 11 | 5.2% | 36 | 9.7% | 54 | 14.0% | 39 | 12.1% | 21 | 6.6% | |
| Hormone-receptor status (HR) | HR-positive | 1286 | 82.9% | 164 | 86.3% | 286 | 80.8% | 311 | 84.3% | 264 | 82.8% | 261 | 81.8% |
| HR-negative | 265 | 17.1% | 26 | 13.7% | 68 | 19.2% | 58 | 15.7% | 55 | 17.2% | 58 | 18.2% | |
| HER2 status | HER2-positive | 327 | 23.8% | 36 | 45.0% | 77 | 26.0% | 85 | 23.4% | 77 | 24.5% | 52 | 16.3% |
| HER2-negative | 1046 | 76.2% | 44 | 55.0% | 219 | 74.0% | 279 | 76.6% | 237 | 75.5% | 267 | 83.7% | |
| Receptor status | triple-positive | 238 | 17.4% | 27 | 34.2% | 50 | 17.0% | 66 | 18.3% | 55 | 17.5% | 40 | 12.5% |
| HR-positive/ HER2-negative | 880 | 64.4% | 36 | 45.6% | 180 | 61.2% | 238 | 66.1% | 205 | 65.3% | 221 | 69.3% | |
| HR-negative/ HER2-positive | 85 | 6.2% | 9 | 11.4% | 26 | 8.8% | 16 | 4.4% | 22 | 7.0% | 12 | 3.8% | |
| triple-negative | 163 | 11.9% | 7 | 8.9% | 38 | 12.9% | 40 | 11.1% | 32 | 10.2% | 46 | 14.4% | |
| Stage at diagnosis of breast cancer | M0 | 1111 | 72.9% | 174 | 81.7% | 290 | 78.4% | 231 | 69.4% | 193 | 66.6% | 223 | 69.9% |
| M1 | 414 | 27.1% | 39 | 18.3% | 80 | 21.6% | 102 | 30.6% | 97 | 33.4% | 96 | 30.1% | |
| Metastatic localizations at initial diagnosis metastasis | Lymph nodes | 102 | 6.3% | 19 | 8.9% | 35 | 9.5% | 23 | 6.0% | 14 | 4.3% | 11 | 3.4% |
| bone | 544 | 33.8% | 85 | 39.9% | 122 | 33.0% | 116 | 30.1% | 104 | 32.3% | 117 | 36.7% | |
| visceral | 796 | 49.4% | 96 | 45.1% | 181 | 48.9% | 201 | 52.1% | 157 | 48.8% | 161 | 50.5% | |
| CNS | 100 | 6.2% | 4 | 1.9% | 17 | 4.6% | 28 | 7.3% | 27 | 8.4% | 24 | 7.5% | |
| others | 68 | 4.2% | 9 | 4.2% | 15 | 4.1% | 18 | 4.7% | 20 | 6.2% | 6 | 1.9% | |
| Number of metastatic localisations at initial diagnosis metastasis | 1 localization | 984 | 61.1% | 159 | 74.6% | 240 | 64.9% | 229 | 59.3% | 198 | 61.5% | 158 | 49.5% |
| 2 localizations | 381 | 23.7% | 41 | 19.2% | 91 | 24.6% | 95 | 24.6% | 65 | 20.2% | 89 | 27.9% | |
| 3 and more localizations | 245 | 15.2% | 13 | 6.1% | 39 | 10.5% | 62 | 16.1% | 59 | 18.3% | 72 | 22.6% | |
| Total | 1st Line | 2nd Line | 3rd Line | 4th Line | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | ||
| HR-positive/HER2-positive (triple-positive (Total n = 614; 1st line n = 230; 2nd line n = 171; 3rd line n = 125; 4th line n = 88) | docetaxel/trastuzumab/pertuzumab | 43 | 7.0% | 34 | 14.8% | 7 | 4.1% | 2 | 1.6% | 0 | 0.0% |
| letrozole | 38 | 6.2% | 22 | 9.6% | 9 | 5.3% | 2 | 1.6% | 5 | 5.7% | |
| anastrozole | 33 | 5.4% | 22 | 9.6% | 6 | 3.5% | 5 | 4.0% | 0 | 0.0% | |
| trastuzumab | 33 | 5.4% | 1 | 0.4% | 12 | 7.0% | 12 | 9.6% | 8 | 9.1% | |
| trastuzumab emtansine | 28 | 4.6% | 2 | 0.9% | 12 | 7.0% | 9 | 7.2% | 5 | 5.7% | |
| exemestane | 25 | 4.1% | 4 | 1.7% | 6 | 3.5% | 11 | 8.8% | 4 | 4.5% | |
| letrozole/trastuzumab | 24 | 3.9% | 13 | 5.7% | 8 | 4.7% | 2 | 1.6% | 1 | 1.1% | |
| (nab-)paclitaxel/trastuzumab | 24 | 3.9% | 9 | 3.9% | 5 | 2.9% | 8 | 6.4% | 2 | 2.3% | |
| (nab-)paclitaxel/trastuzumab/pertuzumab | 20 | 3.3% | 14 | 6.1% | 4 | 2.3% | 1 | 0.8% | 1 | 1.1% | |
| fulvestrant | 20 | 3.3% | 5 | 2.2% | 4 | 2.3% | 7 | 5.6% | 4 | 4.5% | |
| capecitabine | 20 | 3.3% | 3 | 1.3% | 6 | 3.5% | 4 | 3.2% | 7 | 8.0% | |
| trastuzumab/pertuzumab | 20 | 3.3% | 2 | 0.9% | 13 | 7.6% | 5 | 4.0% | 0 | 0.0% | |
| letrozole/trastuzumab/pertuzumab | 18 | 2.9% | 4 | 1.7% | 12 | 7.0% | 2 | 1.6% | 0 | 0.0% | |
| mitoxantrone | 17 | 2.8% | 2 | 0.9% | 4 | 2.3% | 5 | 4.0% | 6 | 6.8% | |
| epirubicin/docetaxel | 16 | 2.6% | 3 | 1.3% | 6 | 3.5% | 6 | 4.8% | 1 | 1.1% | |
| vinorelbine/trastuzumab | 14 | 2.3% | 3 | 1.3% | 1 | 0.6% | 7 | 5.6% | 3 | 3.4% | |
| exemestane/trastuzumab | 11 | 1.8% | 6 | 2.6% | 4 | 2.3% | 0 | 0.0% | 1 | 1.1% | |
| tamoxifen | 11 | 1.8% | 4 | 1.7% | 5 | 2.9% | 1 | 0.8% | 1 | 1.1% | |
| epirubicin/cyclophosphamide | 10 | 1.6% | 9 | 3.9% | 1 | 0.6% | 0 | 0.0% | 0 | 0.0% | |
| docetaxel/trastuzumab | 10 | 1.6% | 3 | 1.3% | 3 | 1.8% | 2 | 1.6% | 2 | 2.3% | |
| capecitabine/trastuzumab | 9 | 1.5% | 2 | 0.9% | 4 | 2.3% | 1 | 0.8% | 2 | 2.3% | |
| others | 170 | 27.7% | 63 | 27.4% | 39 | 22.8% | 33 | 26.4% | 35 | 39.8% | |
| HR-positive/HER2-negative (Total n = 2113; 1st line n = 864; 2nd line n = 559; 3rd line n = 404; 4th line n = 286) | letrozole | 232 | 11.0% | 156 | 18.1% | 52 | 9.3% | 17 | 4.2% | 7 | 2.4% |
| fulvestrant | 230 | 10.9% | 61 | 7.1% | 94 | 16.8% | 42 | 10.4% | 33 | 11.5% | |
| exemestane | 177 | 8.4% | 62 | 7.2% | 60 | 10.7% | 34 | 8.4% | 21 | 7.3% | |
| capecitabine | 163 | 7.7% | 25 | 2.9% | 42 | 7.5% | 51 | 12.6% | 45 | 15.7% | |
| anastrozole | 150 | 7.1% | 114 | 13.2% | 24 | 4.3% | 9 | 2.2% | 3 | 1.0% | |
| palbociclib/letrozole | 145 | 6.9% | 118 | 13.7% | 18 | 3.2% | 5 | 1.2% | 4 | 1.4% | |
| tamoxifen | 81 | 3.8% | 46 | 5.3% | 13 | 2.3% | 19 | 4.7% | 3 | 1.0% | |
| exemestane/everolimus | 81 | 3.8% | 13 | 1.5% | 36 | 6.4% | 26 | 6.4% | 6 | 2.1% | |
| capecitabine/bevacizumab | 80 | 3.8% | 15 | 1.7% | 27 | 4.8% | 24 | 5.9% | 14 | 4.9% | |
| (nab-)paclitaxel | 71 | 3.4% | 38 | 4.4% | 13 | 2.3% | 14 | 3.5% | 6 | 2.1% | |
| epirubicin/docetaxel | 69 | 3.3% | 16 | 1.9% | 18 | 3.2% | 19 | 4.7% | 16 | 5.6% | |
| mitoxantrone | 68 | 3.2% | 11 | 1.3% | 24 | 4.3% | 20 | 5.0% | 13 | 4.5% | |
| palbociclib/fulvestrant | 57 | 2.7% | 27 | 3.1% | 18 | 3.2% | 7 | 1.7% | 5 | 1.7% | |
| ribociclib/letrozole | 33 | 1.6% | 32 | 3.7% | 1 | 0.2% | 0 | 0.0% | 0 | 0.0% | |
| vinorelbine | 32 | 1.5% | 2 | 0.2% | 7 | 1.3% | 7 | 1.7% | 16 | 5.6% | |
| others | 444 | 21.0% | 128 | 14.8% | 112 | 20.0% | 110 | 27.2% | 94 | 32.9% | |
| HR-negative/HER2-positive (Total n = 224; 1st line n = 80; 2nd line n = 65; 3rd line n = 45; 4th line n = 34) | trastuzumab | 32 | 14.3% | 7 | 8.8% | 17 | 26.2% | 8 | 17.8% | 0 | 0.0% |
| trastuzumab emtansine | 19 | 8.5% | 1 | 1.3% | 8 | 12.3% | 7 | 15.6% | 3 | 8.8% | |
| (nab-)paclitaxel/trastuzumab | 14 | 6.3% | 9 | 11.3% | 4 | 6.2% | 0 | 0.0% | 1 | 2.9% | |
| docetaxel/trastuzumab/pertuzumab | 13 | 5.8% | 12 | 15.0% | 0 | 0.0% | 0 | 0.0% | 1 | 2.9% | |
| vinorelbine/trastuzumab | 12 | 5.4% | 6 | 7.5% | 2 | 3.1% | 3 | 6.7% | 1 | 2.9% | |
| trastuzumab/pertuzumab | 12 | 5.4% | 1 | 1.3% | 9 | 13.8% | 2 | 4.4% | 0 | 0.0% | |
| capecitabine/lapatinib | 9 | 4.0% | 3 | 3.8% | 2 | 3.1% | 4 | 8.9% | 0 | 0.0% | |
| (nab-)paclitaxel/trastuzumab/pertuzumab | 8 | 3.6% | 6 | 7.5% | 2 | 3.1% | 0 | 0.0% | 0 | 0.0% | |
| capecitabine | 8 | 3.6% | 3 | 3.8% | 1 | 1.5% | 2 | 4.4% | 2 | 5.9% | |
| capecitabine/trastuzumab | 8 | 3.6% | 3 | 3.8% | 2 | 3.1% | 2 | 4.4% | 1 | 2.9% | |
| docetaxel/trastuzumab | 6 | 2.7% | 0 | 0.0% | 2 | 3.1% | 2 | 4.4% | 2 | 5.9% | |
| (nab-)paclitaxel/carboplatin/trastuzumab/ pertuzumab | 4 | 1.8% | 4 | 5.0% | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | |
| others | 79 | 35.3% | 25 | 31.3% | 16 | 24.6% | 15 | 33.3% | 23 | 67.6% | |
| HR-negative/HER2-negative (triple-negative) (Total n = 349; 1st line n = 142; 2nd line n = 105; 3rd line n = 37; 4th line n = 65) | capecitabine | 49 | 14.0% | 26 | 18.3% | 13 | 12.4% | 8 | 21.6% | 2 | 3.1% |
| capecitabine/bevacizumab | 20 | 5.7% | 20 | 14.1% | 0 | 0.0% | 0 | 0.0% | 0 | 0.0% | |
| eribulin | 20 | 5.7% | 3 | 2.1% | 10 | 9.5% | 6 | 16.2% | 1 | 1.5% | |
| epirubicin/docetaxel | 17 | 4.9% | 5 | 3.5% | 7 | 6.7% | 3 | 8.1% | 2 | 3.1% | |
| gemcitabine/vinorelbine | 17 | 4.9% | 0 | 0.0% | 8 | 7.6% | 3 | 8.1% | 6 | 9.2% | |
| vinorelbine | 16 | 4.6% | 3 | 2.1% | 5 | 4.8% | 4 | 10.8% | 4 | 6.2% | |
| (nab-)paclitaxel | 15 | 4.3% | 9 | 6.3% | 4 | 3.8% | 2 | 5.4% | 0 | 0.0% | |
| atezolizumab/(nab-)paclitaxel | 13 | 3.7% | 11 | 7.7% | 1 | 1.0% | 0 | 0.0% | 1 | 1.5% | |
| carboplatin/(nab-)paclitaxel | 12 | 3.4% | 5 | 3.5% | 4 | 3.8% | 0 | 0.0% | 3 | 4.6% | |
| mitoxantrone | 10 | 2.9% | 4 | 2.8% | 4 | 3.8% | 1 | 2.7% | 1 | 1.5% | |
| carboplatin/(nab-)paclitaxel/bevacizumab | 9 | 2.6% | 7 | 4.9% | 2 | 1.9% | 0 | 0.0% | 0 | 0.0% | |
| docetaxel | 9 | 2.6% | 5 | 3.5% | 1 | 1.0% | 2 | 5.4% | 1 | 1.5% | |
| (nab-)paclitaxel/bevacizumab | 9 | 2.6% | 4 | 2.8% | 3 | 2.9% | 2 | 5.4% | 0 | 0.0% | |
| clinical trial | 8 | 2.3% | 4 | 2.8% | 4 | 3.8% | 0 | 0.0% | 0 | 0.0% | |
| carboplatin/gemcitabine | 8 | 2.3% | 2 | 1.4% | 3 | 2.9% | 2 | 5.4% | 1 | 1.5% | |
| doxorubicin | 8 | 2.3% | 0 | 0.0% | 2 | 1.9% | 5 | 13.5% | 1 | 1.5% | |
| gemcitabine | 7 | 2.0% | 0 | 0.0% | 1 | 1.0% | 4 | 10.8% | 2 | 3.1% | |
| cyclophosphamide/methotrexate | 6 | 1.7% | 1 | 0.7% | 1 | 1.0% | 2 | 5.4% | 2 | 3.1% | |
| epirubicin/(nab-)paclitaxel | 6 | 1.7% | 1 | 0.7% | 3 | 2.9% | 1 | 2.7% | 1 | 1.5% | |
| others | 90 | 25.8% | 32 | 22.5% | 29 | 27.6% | 20 | 54.1% | 9 | 13.8% | |
| Year of Initial Diagnosis Metastasis | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1995–2000 | 2001–2009 | 2010–2014 | 2015–2017 | 2018–2022 | ||||||||||||
| n | Median | Range | n | Median | Range | n | Median | Range | n | Median | Range | n | Median | Range | ||
| Receptor status | triple-positive | 27 | 44.9 | 0.9–189.9+ | 50 | 42.5 | 1.1–156.8+ | 65 | 54.0 | 3.0–112.0 | 55 | 84.2 | 3.0–97.2+ | 40 | 48.3 | 1.6–61.1+ |
| HR-positive/ HER2-negative | 36 | 60.1 | 3.3–181.0 | 179 | 38.0 | 0.3–156.7 | 238 | 38.9 | 0.2–124.4+ | 204 | 38.9 | 0.4–98.4+ | 221 | 51.6 | 0.8–60.4+ | |
| HR-negative/ HER2 positive | 9 | 19.1 | 7.7–84.2 | 26 | 27.7 | 2.8–99.3+ | 16 | 46.2 | 8.0–110.0+ | 22 | 47.8 | 0.9–95.3+ | 12 | - | 1.2–53.5+ | |
| triple-negative | 7 | 6.8 | 1.0–21.2 | 37 | 18.4 | 0.5–109-5+ | 39 | 20.2 | 1.7–110.0+ | 31 | 24.5 | 0.2–78.2+ | 46 | 20.3 | 0.4–43.0+ | |
| Sig. | Hazard Ratio | 95% CI for Hazard Ratio | ||
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| Time between initial diagnosis breast cancer to initial diagnosis metastasis [months] | p < 0.001 | 0.996 | 0.994 | 0.997 |
| Receptor status | p < 0.001 | |||
| Receptor status: triple-positive vs. HR-positive/HER2-negative | p = 0.044 | 1.278 | 1.006 | 1.622 |
| Receptor status: triple-positive vs. HR-negative/HER2-positive | p = 0.197 | 1.307 | 0.870 | 1.962 |
| Receptor status: triple-positive vs. triple-negative | p < 0.001 | 2.459 | 1.801 | 3.357 |
| Stage at initial diagnosis of breast cancer | p < 0.001 | 0.580 | 0.460 | 0.730 |
| ECOG performance status at presentation | p < 0.001 | 1.872 | 1.468 | 2.387 |
| Number of metastatic localizations at diagnosis metastasis | p < 0.001 | |||
| Number of metastatic localizations: 1 localization vs. 2 localizations | p = 0.021 | 1.269 | 1.037 | 1.552 |
| Number of metastatic localizations: 1 localization vs. 3 or more localizations | p < 0.001 | 1.883 | 1.497 | 2.368 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weide, R.; Feiten, S.; Waßmann, C.; Rendenbach, B.; Braun, U.; Burkhard, O.; Ehscheidt, P.; Schmidt, M. Metastatic Breast Cancer: Prolonging Life in Routine Oncology Care. Cancers 2024, 16, 1255. https://doi.org/10.3390/cancers16071255
Weide R, Feiten S, Waßmann C, Rendenbach B, Braun U, Burkhard O, Ehscheidt P, Schmidt M. Metastatic Breast Cancer: Prolonging Life in Routine Oncology Care. Cancers. 2024; 16(7):1255. https://doi.org/10.3390/cancers16071255
Chicago/Turabian StyleWeide, Rudolf, Stefan Feiten, Christina Waßmann, Bernhard Rendenbach, Ute Braun, Oswald Burkhard, Peter Ehscheidt, and Marcus Schmidt. 2024. "Metastatic Breast Cancer: Prolonging Life in Routine Oncology Care" Cancers 16, no. 7: 1255. https://doi.org/10.3390/cancers16071255
APA StyleWeide, R., Feiten, S., Waßmann, C., Rendenbach, B., Braun, U., Burkhard, O., Ehscheidt, P., & Schmidt, M. (2024). Metastatic Breast Cancer: Prolonging Life in Routine Oncology Care. Cancers, 16(7), 1255. https://doi.org/10.3390/cancers16071255