
The Emotional Impact of a Cancer Diagnosis: A Qualitative Study of Adolescent and Young Adult Experience


 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Data Collection
2.4. Data Analysis
- The transcripts were reviewed for accuracy, and the researchers familiarized themselves with the content.
- A framework was developed deductively based on the interview schedule. This was a means of breaking down the transcripts into multiple working themes and subthemes. For example, the theme “Emotional Impact” included the subthemes: acceptance, anger/frustration, anxiety, autonomy, avoidance, guilt, humor, identity, low mood, overwhelmed, and resilience.
- The third stage involved indexing each transcript, i.e., reviewing the transcripts and adding the themes and subthemes to them. The framework was not fixed so new themes and subthemes were added as they were identified in transcripts. When new themes or subthemes were added, previous transcripts we re-reviewed to ensure these had not been missed previously.
- Charting involved developing a matrix within Microsoft Excel (Version 2402), and for each participant, summarizing the text from the transcript, or entering verbatim quotes into the theme (each line in the Excel worksheet was a participant and each column a subtheme).
- Finally, the chart was examined by the research team to map the themes and subthemes to a higher level of interpretation (as this was a means of deconstructing the transcripts) to gain more insightful meaning into young people’s experiences.
3. Results
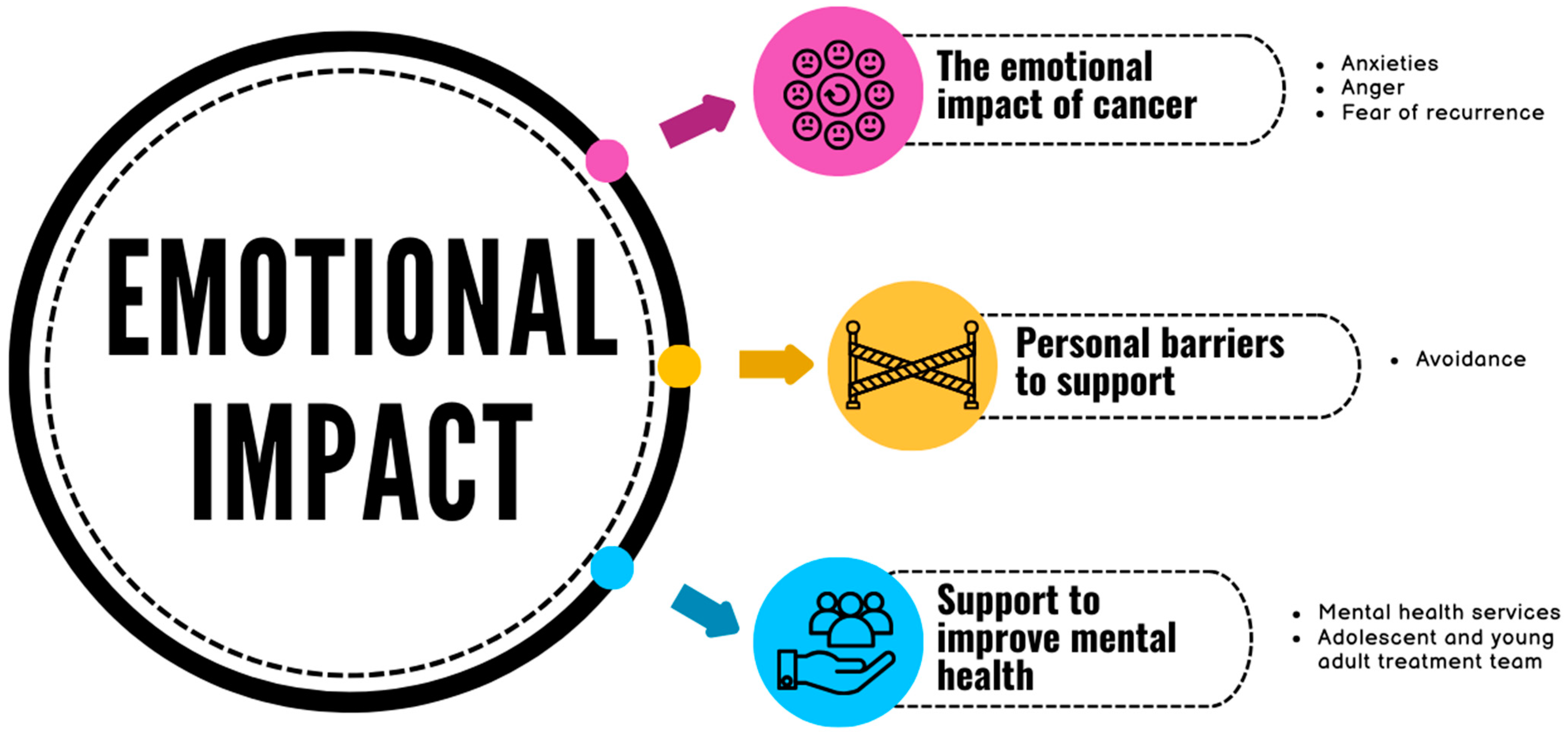
3.1. The Emotional Impact of Cancer
3.1.1. Anxiety
“I think I’ve learned that I’ve got way less mental strength than I thought I had. I thought I was quite a stable person but coming through diagnosis I crumble a lot and I don’t, I really struggle through days, just from basic stuff and I can spiral from really little things,”(Participant 1.162, Cohort 1, male, 25+)
“You’re not sleeping on a night, physically shaking with the anxiety just crying at absolutely everything from—and I’m quite a strong person, quite a resilient person anyway—mentally I’m always like ‘I can face that challenge. Let’s break it down’. But when you hit that brick wall, and it’s not—it’s very much out of the norm for you.”(Participant 1.130, Cohort 1, female, 25+)
“I was staring at the ceiling erm oh, honestly it’s, I don’t know, it might have been overwhelming—So, so much was going on erm so much I wasn’t sure of … because I wasn’t sure of what was going on as well, it did really—it-it took a deep effect and it was just like … you’re really empty.”(Participant 2.021, Cohort 2, female, 25+)
“Yeah, so like directly after treatment was not a great time. I had like I got panic attacks like quite bad panic attacks like I remember one time specifically I woke up in bed this was like a month after treatment, or maybe it was like right towards the end when we’d had a clear set of scans and was like it was nearing the end of treatment and I woke up in my bed at like 3:00 am shaking just complete body shaking and I did not know why and I could not stop myself…my brain was going like 100 miles an hour and they had to like bring me to hospital…I think I was kind of just scared like deeply petrified.”(Participant 2.619, Cohort 2, female, <25)
3.1.2. Anger
“I went to the doctors and…they basically said it was nothing. It really [expletive] me off if I’m perfectly honest … he sort of just said ‘oh it’s nothing’ but he—I was—I mean—my thing to him was ‘What have you got X-ray eyes? How can you say that it’s nothing?’ Anyway he said ‘well I can refer you but it’s gonna take loads of time because COVID and blah blah blah’. So anyway, he got my back up, so I just said ‘Right. Refer me. I’m not I’m not happy with what you’ve said’. So he referred me and it took like seven months before I had any scans. Because of COVID, every appointment just kept being cancelled.”(Participant 1.159, Cohort 1, male, 25+)
“I got quite angry, most of the time I was very annoyed.”(Participant 2.315, Cohort 2, male, <25)
“When I was sick, I would have just loved, just smash up some plates and just … a bunch of anger and then just again, you know in a safe space, obviously. But I think it would just be an interesting sort of thing.”(Participant 2.203, Cohort 2, female, 25+)
3.1.3. Fear of Recurrence
“Since having cancer, I have really bad health anxiety, really bad … Everything kind of settles, then it kind of kicks in a little bit, the mental health side of things. And then it’s like no one’s there anymore … because I think while you’re having your treatment, you’re so busy, you’ve been seen by a medical professional all the time. So, you don’t kind of worry because it’s all in hand. You know, you’ve been seen. But then when everything stops and your treatment stops and then you go home and you’re like’ oh that’s just happened’, and it kind of sinks in then like I wasn’t anxious or overly worried throughout my whole treatment once they said that like you know it hasn’t spread then like I wasn’t worried throughout my treatment then I were happy to just take whatever as it comes it were fine, you know, I’d be fine at end of it. So, whatever, just throw it at me. It’s fine, but it’s the after realization when you’re not as busy and got all these appointments to go to and stuff.”(Participant 2.355, Cohort 2, female, 25+)
“After a while it just felt like I’m well for now but am I going to get another cancer diagnosis which will hurt me or will this one come back and hurt me. Or will there be something else and I will die suddenly? So, I say these thoughts are probably a bit intrusive, like, I don’t want them, they just happen. I’ve spoken to one person, like a friend. But I don’t really feel like that’s something people want to hear, maybe that makes me less, happy less able to enjoy my life, or it’s just one of those things. It is what it is.”(Participant 1.113, Cohort 1, female, 25+)
3.2. Personal Barriers to Support
“I’ll be perfectly honest, I’m not someone who requires a lot of support so, you know, I’m quite a private person and whatnot. So if, if someone sort of started trying to, I don’t know, if I were in there, and they were trying to probe me with loads of questions, you know, I’d probably just sort of shut them down anyway because I don’t really want or need much in terms of, you know I’ve got my family. I’ve got my friends. I don’t really need that much in terms of like—like emotional support or anything like that.”(Participant 1.159, Cohort 1, male, 25+)
“Suddenly you sort of realize that you that you actually might sort of try to keep it all in, but then by talking about it, you realize that actually is helpful … but if you don’t have to make the first step of call someone or whatever it might be. If it’s just sort of like a chat then maybe that would help some people realize that they can get help if they need it you don’t know, they don’t have to just do it all by themselves.”(Participant 1.084, Cohort 1, male, <25)
“That was one thing that actually did come up, which I now maybe do regret. But at that time I just wasn’t sort of ready for, was just people telling me like you should go talk to someone about this. Like talk to a counsellor or something and throughout treatment and even a bit after treatment finished, I was just absolutely certain that I did not want to talk to any form of like counsellor or therapist or you know psychological support person. I was like oh I’m super fine. I don’t want to talk about it … which was probably very silly and stubborn of me at the time … I don’t know, I’m not sure. I think maybe it was like my own like you know, closed into my shell. Like if I’m, if I don’t talk about it then it means I’m fine and I wanted to believe that I was fine.”(Participant 2.619, Cohort 2, female, <25)
“I’d got myself into a such nasty place—it was just, I was—I felt I was on my own. I wasn’t at all. I wasn’t. Never in this world was I on my own. I had everybody at HOSPITAL, I had all my friends and family. I had my colleagues, I had my bosses. I had absolutely anybody I wanted. I just wouldn’t go to them, just wouldn’t, I was just like No, you don’t—I don’t want anybody to see me like this.”(Participant 2.021, Cohort 2, female, 25+)
3.3. Support to Improve Mental Health
3.3.1. Mental Health Services
“Meeting with my psychologist, which was really helpful and I really, you know, needed this one in the earlier stage of my treatment? No one offered to me and didn’t support me. They just general called from the nurses, you know and the doctors, but I mentioned that several times that I need to have a psychologist.”(Participant 1.129, Cohort 1, 25+)
“I was in like such a bad place anyway, and I think the main thing that I had was I was very, very angry and I couldn’t really understand what the anger was about because a lot of the time it related things that happened three years before. Uh, so I had already started seeing a therapist, which I think I’m like lucky enough to be able to afford so I’ve done it privately … I’ve managed to keep that up throughout this entire process, and I do think that made a difference. I don’t know how I would be if I hadn’t had that because I see her once a week and she’s been really really good.”(Participant 1.160, Cohort 1, female, 25+)
“I think there’s so much support in the medical and physical side of things where I don’t think there is in the mental and emotional support—it isn’t on par with that in regard to its availability … You need to go for physical check-ups and medical check-ups, but you don’t need to go to emotional and mental check-ups kind of thing. So, I think just having a bit more sort of enforced in that respect, because I think it does, it will make people better. And just and just again making it seem like that’s completely fine like…after treatment it’s OK to, you know, have a bit of reaction from any treatment or anything. It’s sometimes seen as not OK … it’s a much bigger deal. If you’ve got depression after treatment kind of thing and they have to treat it as a completely separate thing. Whereas I don’t think it should be. I think it should be again normalized and feel more accessible.”(Participant 2.203, Cohort 2, female, 25+)
“Therapy. Definitely. Having consistent therapy for a while and not just a couple of sessions. I was in therapy for four years and still am because, you need time to get into it and a lot of the time you need a year to, like get over the fact that you don’t wanna do therapy so yeah, like having some kind of contact available for that for that kind of support because it does go on and there are things that come up five years after you treatment related to your experience that you would not even think about two years after. I think having a good support system who have that tangible list of things that need to get done, or things that they need specific things is really helpful because it takes the weight off completely.”(Participant 2.040, Cohort 2, female, 25+)
3.3.2. Adolescent and Young Adult Treatment Team
“I did find like just sometimes ranting to the YSC [youth support coordinator], you know was enough in itself. Like and not labelling it like psychological support, more just like having someone you know Because I actually genuinely feel like they care about me, you know? Like, it’s not just a job to them. It’s like they come in and they actually, you know…that that kind of special touch…Like you don’t necessarily need to talk to someone, you just need someone to say like I care about you.”(Participant 1.128, Cohort 1, female, <25)
“We had a support worker [youth worker] there whose main job was just to kind of have fun with us and like, chat with us. He wasn’t there to be a particular signpost and that was like one of the best things ever, because you get very used to people who are there to like, care for you, and then sometimes you just want a mate who like it wasn’t your parent… I remember there was a time where like my mum had been sleeping there for ages and I was like, I just wanted a night alone. I don’t want her to sleep here tonight, and my mum was very like, no, I’m not going to leave you alone. And so, it was the support worker who I could talk to and he was like, yeah, maybe she might just want one night of, like, independence. That’s all. It’s nothing to do with you. Like, which was good.”(Participant 2.040, Cohort 2, female, 25+)
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stoneham, S.J. AYA Survivorship: The Next Challenge. Cancer 2020, 126, 2116–2119. [Google Scholar] [CrossRef] [PubMed]
- Osborn, M.; Johnson, R.; Thompson, K.; Anazodo, A.; Albritton, K.; Ferrari, A.; Stark, D. Models of Care for Adolescent and Young Adult Cancer Programs. Pediatr. Blood Cancer 2019, 66, e27991. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Peters, M.; Ellis, I.; Mcmonagle, L. The Impact of COVID-19 on Adolescent and Young Adult Cancer Services. Cancer Care Res. Online 2022, 2, e018. [Google Scholar] [CrossRef]
- Fardell, J.E.; Patterson, P.; Wakefield, C.E.; Signorelli, C.; Cohn, R.J.; Anazodo, A.; Zebrack, B.; Sansom-Daly, U.M. A Narrative Review of Models of Care for Adolescents and Young Adults with Cancer: Barriers and Recommendations. J. Adolesc. Young Adult Oncol. 2018, 7, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Lea, S.; Taylor, R.M.; Martins, A.; Fern, L.A.; Whelan, J.S.; Gibson, F. Conceptualising Age-Appropriate Care for Teenagers and Young Adults with Cancer: A Qualitative Mixed Methods Study. Adolesc. Health Med. Ther. 2018, 9, 149–166. [Google Scholar] [PubMed]
- Hubbard, G.; Forbat, L. Cancer as Biographical Disruption: Constructions of Living with Cancer. Support. Care Cancer 2012, 20, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Braun, I.; Friedrich, M.; Morgenstern, L.; Sender, A.; Geue, K.; Mehnert-Theuerkauf, A.; Leuteritz, K. Changes, Challenges and Support in Work, Education and Finances of Adolescent and Young Adult (AYA) Cancer Survivors: A Qualitative Study. Eur. J. Oncol. Nurs. 2023, 64, 102329. [Google Scholar] [CrossRef] [PubMed]
- Lidington, E.; Vlooswijk, C.; Stallard, K.; Travis, E.; Younger, E.; Edwards, P.; Nandhabalan, M.; Hunter, N.; Sarpal, N.; Flett, D.; et al. ‘This is Not Part of My Life Plan’: A Qualitative Study on the Psychosocial Experiences and Practical Challenges in Young Adults with Cancer Age 25 to 39 Years at Diagnosis. Eur. J. Cancer Care 2021, 30, e13458. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S. ‘When You have Children, You’re Obliged to Live’ 1: Motherhood, Chronic Illness and Biographical Disruption. Sociol. Health Illn. 2007, 29, 610–626. [Google Scholar] [CrossRef]
- NHS England. Specialist Cancer Services for Children and Young People: Teenage and Young Adults Principal Treatment Centre Services; NHS England: London, UK, 2023. [Google Scholar]
- Fernandez, C.; Fraser, G.A.M.; Freeman, C.; Grunfeld, E.; Gupta, A.; Mery, L.S.; De Pauw, S.; Schacter, B. Principles and Recommendations for the Provision of Healthcare in Canada to Adolescent and Young Adult–Aged Cancer Patients and Survivors. J. Adolesc. Young Adult Oncol. 2011, 1, 53–59. [Google Scholar] [CrossRef]
- Wood, D.; Crapnell, T.; Lau, L.; Bennett, A.; Lotstein, D.; Ferris, M.; Kuo, A. Emerging Adulthood as a Critical Stage in the Life Course. In Handbook of Life Course Health Development; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Lie, N.K.; Larsen, T.M.B.; Hauken, M.A. Coping with Changes and Uncertainty: A Qualitative Study of Young Adult Cancer Patients’ Challenges and Coping Strategies during Treatment. Eur. J. Cancer Care 2018, 27, e12743. [Google Scholar] [CrossRef]
- Barton, K.S.; Steineck, A.; Walsh, C.A.; Lau, N.; O’Donnell, M.B.; Rosenberg, A.R. “I Won’T Get to Live My Life the Way I Planned it”: A Qualitative Analysis of the Experiences of Adolescents and Young Adults with Advanced Cancer. Pediatr. Blood Cancer 2023, 70, e30554. [Google Scholar] [CrossRef] [PubMed]
- Grinyer, A. The Biographical Impact of Teenage and Adolescent Cancer. Chronic Illn. 2007, 3, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.J. Emerging Adulthood: The Winding Road from the Late Teens through the Twenties, 2nd ed.; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- Taylor, R.M.; Pearce, S.; Gibson, F.; Fern, L.; Whelan, J. Developing a Conceptual Model of Teenage and Young Adult Experiences of Cancer through Meta-Syntheisis. Int. J. Nurs. Stud. 2013, 50, 832–846. [Google Scholar] [CrossRef] [PubMed]
- Stark, D.; Bowen, D.; Dunwoodie, E.; Feltbower, R.; Johnson, R.; Moran, A.; Stiller, C.; O’Hara, C. Survival Patterns in Teenagers and Young Adults with Cancer in the United Kingdom: Comparisons with Younger and Older Age Groups. Eur. J. Cancer 2015, 51, 2643–2654. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.W.; Seibel, N.L.; Lewis, D.R.; Albritton, K.H.; Blair, D.F.; Blanke, C.D.; Bleyer, W.A.; Freyer, D.R.; Geiger, A.M.; Hayes-Lattin, B.; et al. Next Steps for Adolescent and Young Adult Oncology Workshop: An Update on Progress and Recommendations for the Future. Cancer 2016, 122, 988–999. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.R.; Zhou, C.; Bradford, M.C.; Salsman, J.M.; Sexton, K.; O’Daffer, A.; Yi-Frazier, J.P. Assessment of the Promoting Resilience in Stress Management Intervention for Adolescent and Young Adult Survivors of Cancer at 2 Years: Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2136039. [Google Scholar] [CrossRef]
- Nass, S.J.; Beaupin, L.K.; Demark-Wahnefried, W.; Fasciano, K.; Ganz, P.A.; Hayes-Lattin, B.; Hudson, M.M.; Nevidjon, B.; Oeffinger, K.C.; Rechis, R.; et al. Identifying and Addressing the Needs of Adolescents and Young Adults with Cancer: Summary of an Institute of Medicine Workshop. Oncologist 2015, 20, 186–195. [Google Scholar] [CrossRef]
- Hanghoj, S.; Pappot, N.; Hjerming, M.; Taarnhoj, G.A.; Boisen, K.A.; Pappot, H. Experiences of Social Isolation during the COVID-19 Lockdown among Adolescents and Young Adult Cancer Patients and Survivors. J. Adolesc. Young-Adult Oncol. 2021, 10, 142–147. [Google Scholar] [CrossRef]
- Tremolada, M.; Taverna, L.; Vietina, F.; Incardona, R.M.; Pierobon, M.; Bonichini, S.; Biffi, A.; Bisogno, G. Adolescents and Young Adults with Oncohematological Disease: Use of Social Networks, Impact of SARS-CoV-2, and Psychosocial Well-Being. Front. Psychiatry 2023, 14, 1239131. [Google Scholar] [CrossRef]
- Aldiss, S.; Fern, L.A.; Philips, R.S.; Callaghan, A.; Dyker, K.; Gravestock, H.; Groszman, M.; Hamrang, L.; Hough, R.; McGeachy, D.; et al. Research Priorities for Young People with Cancer: A UK Priority Setting Partnership with the James Lind Alliance. BMJ Open 2019, 9, e028119. [Google Scholar] [CrossRef] [PubMed]
- Baclig, N.V.; Comulada, W.S.; Ganz, P.A. Mental Health and Care Utilization in Survivors of Adolescent and Young Adult Cancer. JNCI Cancer Spectr. 2023, 7, pkad098. [Google Scholar] [CrossRef] [PubMed]
- Riba, M.B.; Donovan, K.A.; Ahmed, K.; Andersen, B.; Braun, I.; Breitbart, W.S.; Brewer, B.W.; Corbett, C.; Fann, J.; Fleishman, S.; et al. NCCN Guidelines®® Insights: Distress Management, Version 2.2023. J. Natl. Compr. Canc Netw. 2023, 21, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Pressman, S.D.; Cohen, S. Does Positive Affect Influence Health? Psychol. Bull. 2005, 131, 925–971. [Google Scholar] [CrossRef] [PubMed]
- Tremolada, M.; Bonichini, S.; Basso, G.; Pillon, M. Adolescent and Young Adult Cancer Survivors Narrate their Stories: Predictive Model of their Personal Growth and their Follow-Up Acceptance. Eur. J. Oncol. Nurs. 2018, 36, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Faller, H.; Schuler, M.; Richard, M.; Heckl, U.; Weis, J.; Kuffner, R. Effects of Psycho-Oncologic Interventions on Emotional Distress and Quality of Life in Adult Patients with Cancer: Systematic Review and Meta-Analysis. J. Clin. Oncol. 2013, 31, 782–793. [Google Scholar] [CrossRef]
- Barth, J.; Delfino, S.; Kunzler, A. Naturalistic Study on the Effectiveness of Psycho-Oncological Interventions in Cancer Patients and their Partners. Support. Care Cancer 2013, 21, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- Clover, K.A.; Mitchell, A.J.; Britton, B.; Carter, G. Why do Oncology Outpatients Who Report Emotional Distress Decline Help? Psychooncology 2015, 24, 812–818. [Google Scholar] [CrossRef]
- Cohen, A.; Ianovski, L.E.; Frenkiel, S.; Hier, M.; Zeitouni, A.; Kost, K.; Mlynarek, A.; Richardson, K.; Black, M.; MacDonald, C.; et al. Barriers to Psychosocial Oncology Service Utilization in Patients Newly Diagnosed with Head and Neck Cancer. Psychooncology 2018, 27, 2786–2793. [Google Scholar] [CrossRef]
- Pichler, T.; Dinkel, A.; Marten-Mittag, B.; Hermelink, K.; Telzerow, E.; Ackermann, U.; Belka, C.; Combs, S.E.; Gratzke, C.; Gschwend, J.; et al. Factors Associated with the Decline of Psychological Support in Hospitalized Patients with Cancer. Psychooncology 2019, 28, 2049–2059. [Google Scholar] [CrossRef]
- Tondorf, T.; Grossert, A.; Rothschild, S.I.; Koller, M.T.; Rochlitz, C.; Kiss, A.; Schaefert, R.; Meinlschmidt, G.; Hunziker, S.; Zwahlen, D. Focusing on Cancer Patients’ Intentions to use Psychooncological Support: A Longitudinal, Mixed-Methods Study. Psychooncology 2018, 27, 1656–1663. [Google Scholar] [CrossRef] [PubMed]
- Weis, J.; Honig, K.; Bergelt, C.; Faller, H.; Brechtel, A.; Hornemann, B.; Stein, B.; Teufel, M.; Goerling, U.; Erim, Y.; et al. Psychosocial Distress and Utilization of Professional Psychological Care in Cancer Patients: An Observational Study in National Comprehensive Cancer Centers (CCCs) in Germany. Psychooncology 2018, 27, 2847–2854. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Wang, K.; Zebrack, B.; Tan, C.Y.; Walling, E.; Chugh, R. Psychosocial, Behavioral, and Supportive Interventions for Pediatric, Adolescent, and Young Adult Cancer Survivors: A Systematic Review and Meta-Analysis. Crit. Rev. Oncol. 2021, 160, 103291. [Google Scholar] [CrossRef] [PubMed]
- Blasco, T.; Jovell, E.; Mirapeix, R.; Leon, C. Patients’ Desire for Psychological Support when Receiving a Cancer Diagnostic. Int. J. Environ. Res. Public Health 2022, 19, 14474. [Google Scholar] [CrossRef] [PubMed]
- Osmani, V.; Hörner, L.; Klug, S.J.; Tanaka, L.F. Prevalence and Risk of Psychological Distress, Anxiety and Depression in Adolescent and Young Adult (AYA) Cancer Survivors: A Systematic Review and Meta-Analysis. Cancer Med. 2023, 12, 18354–18367. [Google Scholar] [CrossRef] [PubMed]
- Quinn, G.P.; Goncalves, V.; Sehovic, I.; Bowman, M.L.; Reed, D.R. Quality of Life in Adolescent and Young Adult Cancer Patients: A Systematic Review of Literature. Patient Relat. Outcome Meas. 2015, 6, 19–51. [Google Scholar] [CrossRef]
- Zebrack, B.J.; Corbett, V.; Embry, L.; Aguilar, C.; Meeske, K.A.; Hayes-Lattin, B.; Block, R.; Zeman, D.T.; Cole, S. Psychological Distress and Unsatisfied Need for Psychosocial Support in Adolescent and Young Adult Cancer Patients during the First Year Following Diagnosis. Psychooncology 2014, 23, 1267–1275. [Google Scholar] [CrossRef] [PubMed]
- Stark, D.; Kiely, M.; Smith, A.; Velikova, G.; House, A.; Selby, P. Anxiety Disorders in Cancer Patients: Their Nature, Associations, and Relation to Quality of Life. J. Clin. Oncol. 2002, 20, 3137–3148. [Google Scholar] [CrossRef]
- Mehnert, A.; Brahler, E.; Faller, H.; Harter, M.; Keller, M.; Schulz, H.; Wegscheider, K.; Weis, J.; Boehncke, A.; Hund, B.; et al. Four-Week Prevalence of Mental Disorders in Patients with Cancer across Major Tumor Entities. J. Clin. Oncol. 2014, 32, 3540–3546. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression is a Risk Factor for Noncompliance with Medical Treatment: Meta-Analysis of the Effects of Anxiety and Depression on Patient Adherence. Arch. Intern. Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef]
- Brebach, R.; Sharpe, L.; Costa, D.S.J.; Rhodes, P.; Butow, P. Psychological Intervention Targeting Distress for Cancer Patients: A Meta-Analytic Study Investigating Uptake and Adherence. Psychooncology 2016, 25, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Salmon, P.; Clark, L.; McGrath, E.; Fisher, P. Screening for Psychological Distress in Cancer: Renewing the Research Agenda. Psychooncology 2015, 24, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Children’s Commissioner. Lightening Review: Access to Children and Adolescent Mental Health Services. 2016. Available online: https://www.childrenscommissioner.gov.uk/wp-content/uploads/2017/06/Childrens-Commissioners-Mental-Health-Lightning-Review.pdf (accessed on 23 March 2024).
- Seamark, D.; Gabriel, L. Barriers to Support: A Qualitative Exploration into the Help-Seeking and Avoidance Factors of Young Adults. Br. J. Guid. Couns. 2018, 46, 120–131. [Google Scholar] [CrossRef]
- Sansom-Daly, U.M.; Wakefield, C.E. Distress and Adjustment among Adolescents and Young Adults with Cancer: An Empirical and Conceptual Review. Transl. Pediatr. 2013, 2, 167–197. [Google Scholar] [PubMed]
- Okuyama, T.; Kizawa, Y.; Morita, T.; Kinoshita, H.; Uchida, M.; Shimada, A.; Naito, A.S.; Akechi, T. Current Status of Distress Screening in Designated Cancer Hospitals: A Cross-Sectional Nationwide Survey in Japan. J. Natl. Compr. Cancer Netw. 2016, 14, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, S.; Torres, A.; Morgadinho, R.; Pereira, A. Psychosocial Outcomes in Young Adults with Cancer: Emotional Distress, Quality of Life and Personal Growth. Arch. Psychiatr. Nurs. 2013, 27, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; Min, Y.H.; Lee, S.B. Longitudinal Trends in Illness Perception and Depression during Adjuvant Breast Cancer Endocrine Therapy: A Prospective Observational Study. Healthcare 2021, 9, 1223. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, J.; Spencer, L. Qualitative data analysis for applied policy research. In The Qualitative Researcher’s Companion; Bryman, A., Burgess, R.G., Eds.; Routledge: London, UK, 1994; pp. 173–194. [Google Scholar]
- Taylor, R.M.; Fern, L.A.; Barber, J.A.; Alvarez-Galvez, J.; Feltbower, R.; Morris, S.; Hooker, L.; McCabe, M.G.; Gibson, F.; Raine, R.; et al. Description of the BRIGHTLIGHT Cohort: The Evaluation of Teenagers and Young Adult Cancer Services in England. BMJ Open 2019, 9, e027797. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Taylor, R. How to Read a Paper: Papers that Go Beyond Numbers (Qualitative Research). BMJ 1997, 315, 740–743. [Google Scholar] [CrossRef]
- Krebber, A.M.H.; Buffart, L.M.; Kleijn, G.; Riepma, I.C.; de Bree, R.; Leemans, C.R.; Becker, A.; Brug, J.; van Straten, A.; Cuijpers, P.; et al. Prevalence of Depression in Cancer Patients: A Meta-Analysis of Diagnostic Interviews and Self-Report Instruments. Psycho-Oncology 2014, 23, 121–130. [Google Scholar] [CrossRef]
- Upreti, R.P.; Mmbaga, E.; Haugnes, H.S.; Kiserud, C.E.; Del Risco Kollerud, R. Most Common Health Problems in General Practice among Adolescents, and Young Adults’ Survivors of Lymphoma: A Register-Based Cohort Study in Norway. Acta Oncol. 2023, 62, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Tanner, S.; Engstrom, T.; Lee, W.R.; Forbes, C.; Walker, R.; Bradford, N.; Pole, J.D. Mental Health Patient-reported Outcomes among Adolescents and Young Adult Cancer Survivors: A Systematic Review. Cancer Med. 2023, 12, 18381–18393. [Google Scholar] [CrossRef] [PubMed]
- Forster, A.; Herbert, A.; Koo, M.M.; Taylor, R.M.; Gibson, F.; Whelan, J.; Lyratzopoulos, G.; Fern, L. Associations between Diagnostic Time Intervals and Quality of Life, Clinical Anxiety and Depression in Adolescents and Young Adults with Cancer: The BRIGHTLIGHT Cohort. Br. J. Cancer 2022, 126, 1725–1734. [Google Scholar] [CrossRef] [PubMed]
- May, E.A.; McGill, B.C.; Robertson, E.G.; Anazodo, A.; Wakefield, C.E.; Sansom-Daly, U.M. Adolescent and Young Adult Cancer Survivors’ Experiences of the Healthcare System: A Qualitative Study. J. Adolesc. Young-Adult Oncol. 2018, 7, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Thompson, K.; Palmer, S.; Dyson, G. Adolescents & Young Adults: Issues in Transition from Active Therapy into Follow-Up Care. Eur. J. Oncol. Nurs. 2009, 13, 207–212. [Google Scholar] [PubMed]
- Lea, S.; Martins, A.; Cable, M.; Fern, L.A.; Morgan, S.; Soanes, L.; Whelan, M.; Taylor, R.M. Exploring Young People’s Experience of Ending Active Cancer Treatment: When the “little Cancer Treatment Bubble” Pops. Cancer Nurs. 2021, 44, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Simard, S.; Thewes, B.; Humphris, G.; Dixon, M.; Hayden, C.; Mireskandari, S.; Ozakinci, G. Fear of Cancer Recurrence in Adult Cancer Survivors: A Systematic Review of Quantitative Studies. J. Cancer Surviv. 2013, 7, 300–322. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, W.; Wen, Y.; Wang, H.; Sun, H.; Liang, W.; Zhang, B.; Humphris, G. Fear of Cancer Recurrence in Adolescent and Young Adult Cancer Survivors: A Systematic Review of the Literature. Psychooncology 2019, 28, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Gormley, M.; Ghazal, L.; Fu, M.R.; Van Cleave, J.H.; Knobf, T.; Hammer, M. An Integrative Review on Factors Contributing to Fear of Cancer Recurrence among Young Adult Breast Cancer Survivors. Cancer Nurs. 2022, 45, E10–E26. [Google Scholar] [CrossRef]
- Richter, D.; Clever, K.; Mehnert-Theuerkauf, A.; Schönfelder, A. Fear of Recurrence in Young Adult Cancer Patients—A Network Analysis. Cancers 2022, 14, 2092. [Google Scholar] [CrossRef]
- Essig, S.; Steiner, C.; Kuehni, C.E.; Weber, H.; Kiss, A. Improving Communication in Adolescent Cancer Care: A Multiperspective Study. Pediatr. Blood Cancer 2016, 63, 1423–1430. [Google Scholar] [CrossRef]
- Pyke-Grimm, K.; Franck, L.; Halpern-Felsher, B.; Goldsby, R.; Rehm, R. 3 Dimensions of Treatment Decision Making in Adolescents and Young Adults with Cancer. Cancer Nurs. 2020, 43, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Chiou, S.; Lin, P.; Liao, Y.M.; Su, H. Decisional Conflicts, Anxiety, and Perceptions of Shared Decision-making in Cancer Treatment Trajectory among Adolescents with Cancer: A Longitudinal Study. J. Nurs. Scholarsh. 2022, 54, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Soanes, L.; Gibson, F. Protecting an Adult Identity: A Grounded Theory of Supportive Care for Young Adults Recently Diagnosed with Cancer. Int. J. Nurs. Stud. 2018, 81, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Leslie, M.; Beatty, L.; Hulbert-Williams, L.; Pendrous, R.; Cartwright, T.; Jackson, R.; Hulbert-Williams, N.J. Web-Based Psychological Interventions for People Living with and Beyond Cancer: Meta-Review of what Works and what does Not for Maximizing Recruitment, Engagement, and Efficacy. JMIR Cancer 2022, 8, e36255. [Google Scholar] [CrossRef] [PubMed]
- Stroske, I.; Geue, K.; Friedrich, M.; Sender, A.; Schmidt, R.; Richter, D.; Leuteritz, K. Health Behavior and Associated Factors in Young Adult Cancer Patients. Front. Psychol. 2021, 12, 697096. [Google Scholar] [CrossRef]
- Litz, B.T.; Gray, M.J.; Bryant, R.A.; Adler, A.B. Early Intervention for Trauma: Current Status and Future Directions. Clin. Psychol. Sci. Pract. 2002, 9, 112–134. [Google Scholar] [CrossRef]
- Lang-Rollin, I.; Berberich, G. Psycho-Oncology. Dialogues Clin. Neurosci. 2018, 20, 13–22. [Google Scholar] [CrossRef]
- National Collaborating Centre for Mental Health (Great Britain); National Institute for Health and Clinical Excellence (Great Britain). Common Mental Health Disorders: Identification and Pathways to Care; British Psychological Society: London, UK, 2011. [Google Scholar]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; Salazar de Pablo, G.; Il Shin, J.; Kirkbride, J.B.; Jones, P.; Kim, J.H.; et al. Age at Onset of Mental Disorders Worldwide: Large-Scale Meta-Analysis of 192 Epidemiological Studies. Mol. Psychiatry 2022, 27, 281–295. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Topic Checklist |
|---|
| Functional limitations—Attribution and impact on daily activities |
| Fatigue source/attribution and impact |
| Education—past and future plans |
| Reasons for discontinuing education (if discontinued) |
| Sources of dissatisfaction with education (if in education/training) |
| Understanding of cancer by others in school (if in education/training) |
| Support provided by school or others (if in education/training) |
| Work—past and future plans |
| Diagnosis disclosure and support from co-workers (if in employment) |
| Diagnosis disclosure and support from employer (if in employment) |
| Sources of satisfaction or dissatisfaction with work (if in employment) |
| Perceived barriers to employment |
| Perceived pressures to re-enter education or work |
| Sources of formal and informal support: wanted, available, accessed |
| * Impact of diagnosis on fertility (if fertility is brought up naturally or the consent to discussing this) |
| * Impact of fertility on image and life plans (if fertility is brought up naturally or the consent to discussing this) |
| * Impact of fertility worries on personal relationships (if fertility is brought up naturally or the consent to discussing this) |
| Taking everything into account, what do you feel like your experiences have taught you—about the world, about yourself, about others |
| Location | Age | Gender | Time Since Diagnosis | Time Since End of Treatment | Diagnosis | Disease Severity | |
|---|---|---|---|---|---|---|---|
| Cohort 1 1 (n = 21) | North = 14 South = 7 | 18–36 | M = 12 F = 9 | 1–8 months | N/A | Solid tumors = 12 Hematological = 6 | Least = 11 Intermediate or Severe = 10 |
| Cohort 2 2 (n = 22) | North = 11 South = 11 | 22–38 | M = 13 F = 9 | 3–6 years | 3–6 years | Solid tumors = 13 Hematological = 9 | Least = 12; Intermediate or Severe = 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hughes, L.; Taylor, R.M.; Beckett, A.E.; Lindner, O.C.; Martin, A.; McCulloch, J.; Morgan, S.; Soanes, L.; Uddin, R.; Stark, D.P. The Emotional Impact of a Cancer Diagnosis: A Qualitative Study of Adolescent and Young Adult Experience. Cancers 2024, 16, 1332. https://doi.org/10.3390/cancers16071332
Hughes L, Taylor RM, Beckett AE, Lindner OC, Martin A, McCulloch J, Morgan S, Soanes L, Uddin R, Stark DP. The Emotional Impact of a Cancer Diagnosis: A Qualitative Study of Adolescent and Young Adult Experience. Cancers. 2024; 16(7):1332. https://doi.org/10.3390/cancers16071332
Chicago/Turabian StyleHughes, Luke, Rachel M. Taylor, Angharad E. Beckett, Oana C. Lindner, Adam Martin, Joanne McCulloch, Sue Morgan, Louise Soanes, Rizwana Uddin, and Dan P. Stark. 2024. "The Emotional Impact of a Cancer Diagnosis: A Qualitative Study of Adolescent and Young Adult Experience" Cancers 16, no. 7: 1332. https://doi.org/10.3390/cancers16071332
APA StyleHughes, L., Taylor, R. M., Beckett, A. E., Lindner, O. C., Martin, A., McCulloch, J., Morgan, S., Soanes, L., Uddin, R., & Stark, D. P. (2024). The Emotional Impact of a Cancer Diagnosis: A Qualitative Study of Adolescent and Young Adult Experience. Cancers, 16(7), 1332. https://doi.org/10.3390/cancers16071332