
Improved Metastatic-Free Survival after Systematic Re-Excision Following Complete Macroscopic Unplanned Excision of Limb or Trunk Soft Tissue Sarcoma

 ,
,  , ,
, ,  on behalf of the NETSARC/RREPS and French Sarcoma Group-Groupe d’Etude des Tumeurs Osseuses (GSF-GETO) Networksadd
Show full author list
on behalf of the NETSARC/RREPS and French Sarcoma Group-Groupe d’Etude des Tumeurs Osseuses (GSF-GETO) Networksadd
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. NETSARC Network and Database
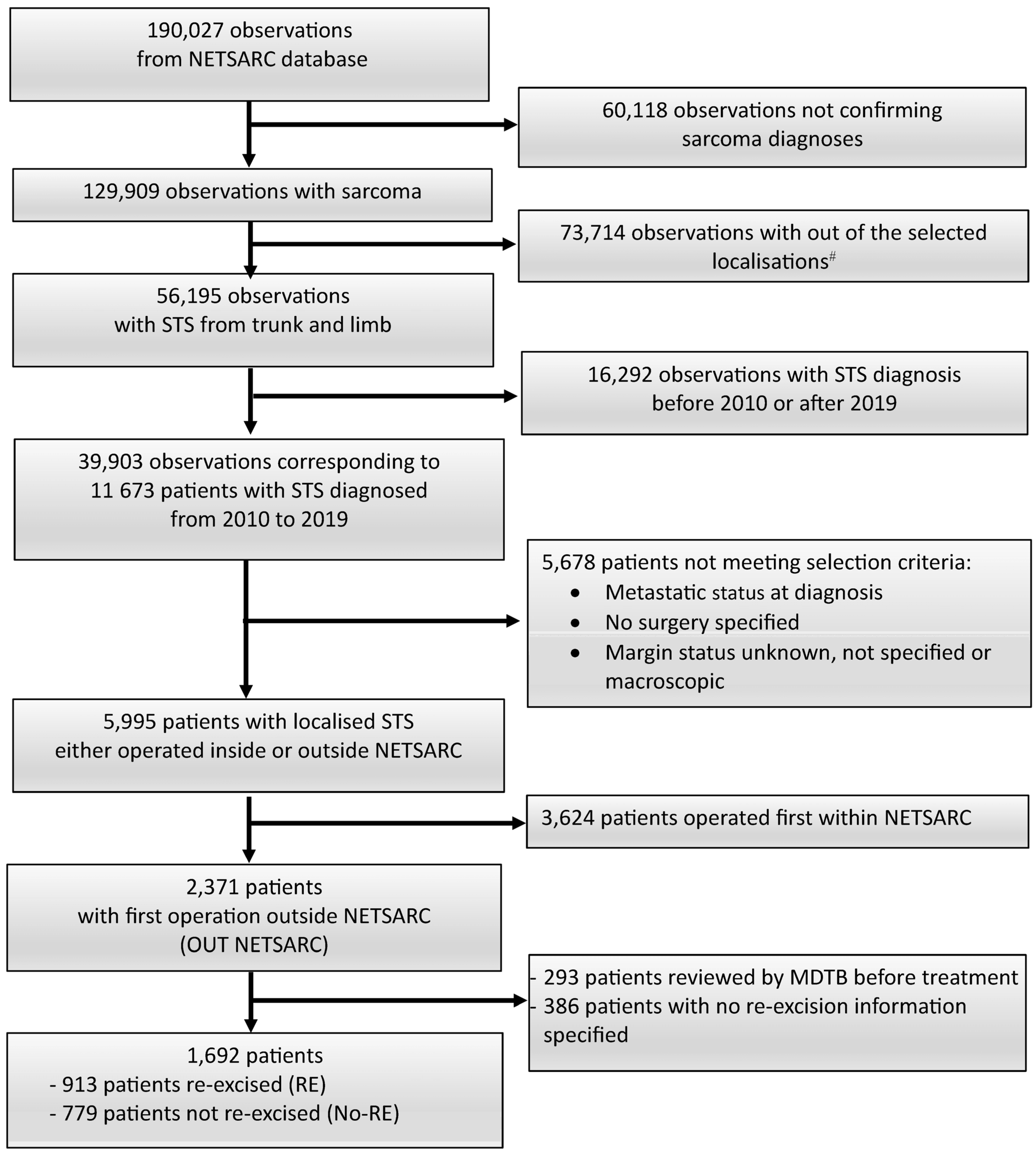
2.2. Patient Selection
2.3. Objectives
2.4. Statistical Methods
3. Results
3.1. Patient and Tumor Characteristics
3.2. Impact of RE on MFS
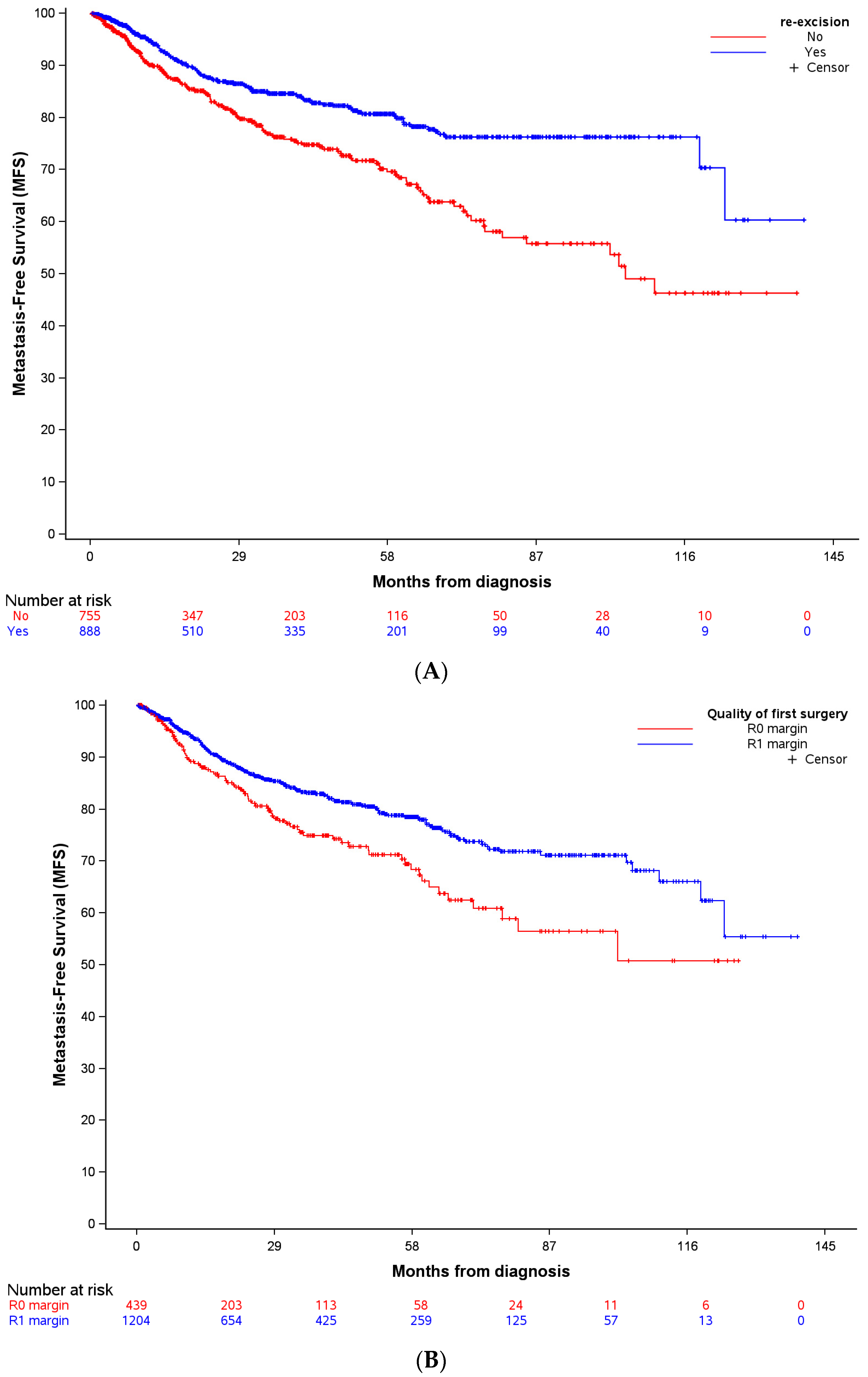
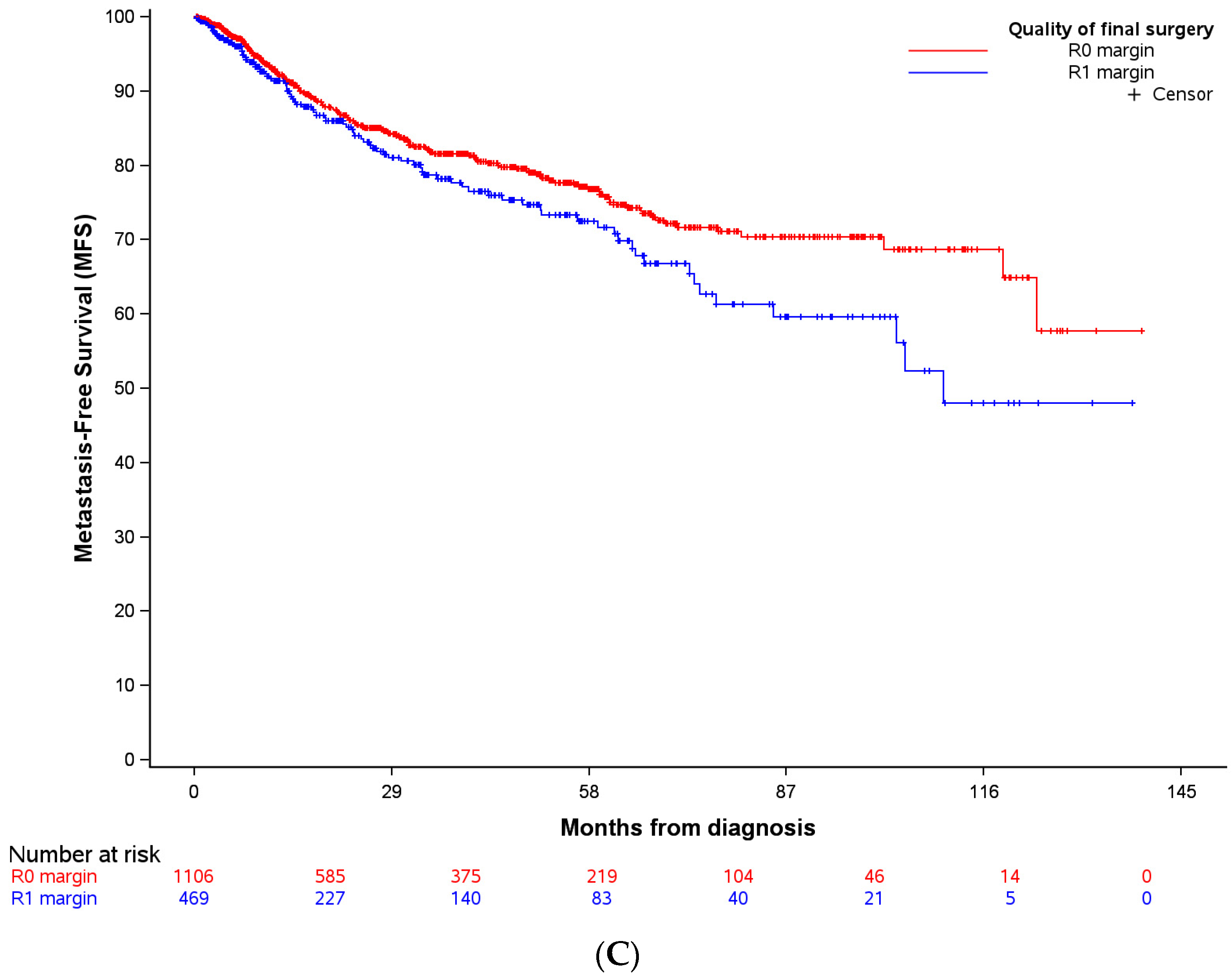
3.2.1. Kaplan–Meier Curves
3.2.2. Univariate Analysis
3.2.3. Multivariate Analysis
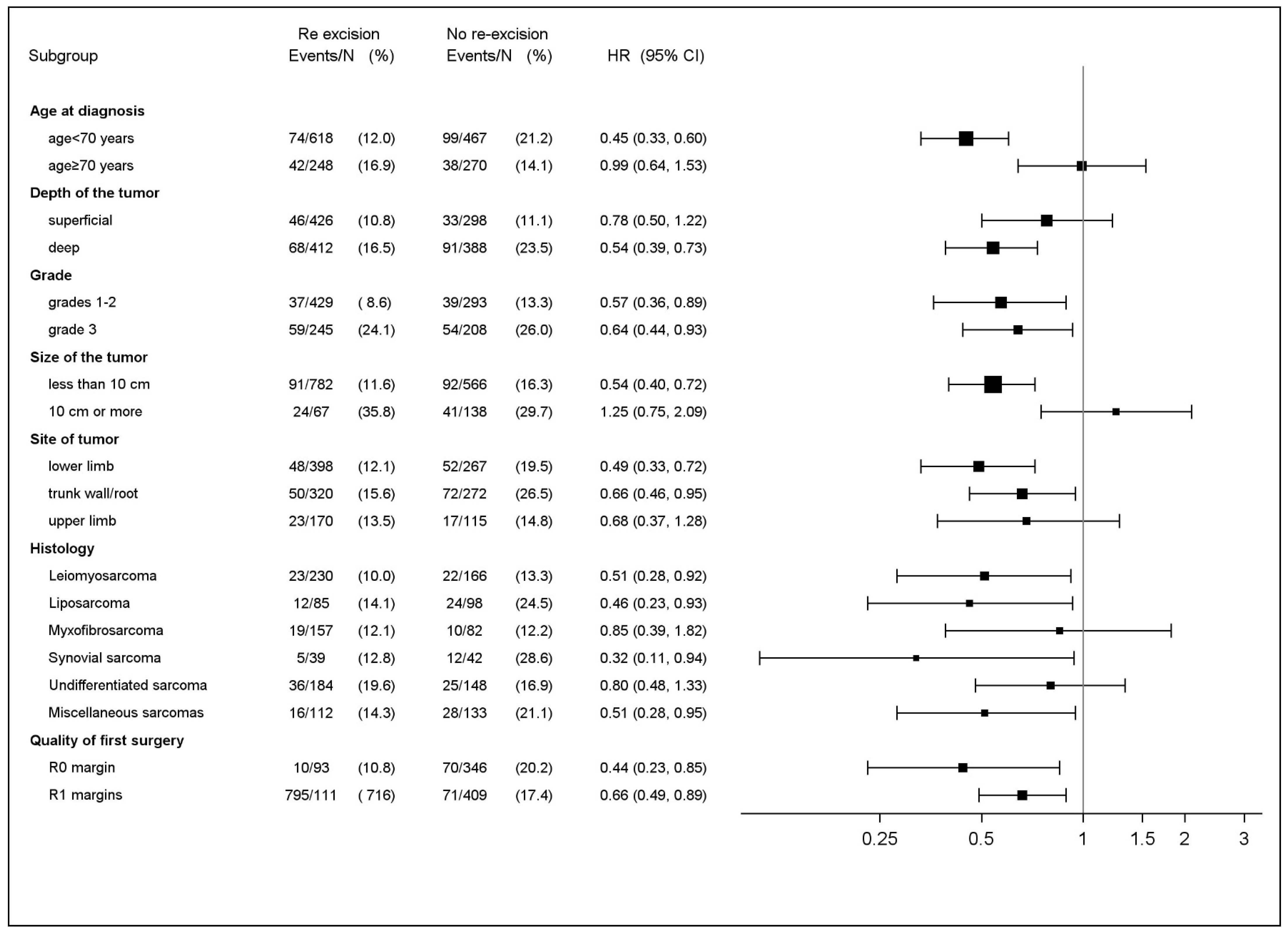
3.3. Sub-Group Analysis of Impact of RE on Patients MFS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fletcher, C.D.M.; Baldini, E.H.; Blay, J.Y.; Gronchi, A.; Lazar, A.J.; Messiou, C.; Pollock, R.E.; Singer, S.E.; WHO classification of soft tissue tumours. Introduction. In Soft Tissue and Bone Tumours Who Classification of Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France; WHO Classification of Tumours Editorial Boards: Geneva, Switzerland, 2020. [Google Scholar]
- De Pinieux, G.; Karanian, M.; Le Loarer, F.; Le Guellec, S.; Chabaud, S.; Terrier, P.; Bouvier, C.; Batistella, M.; Neuville, A.; Robin, Y.-M.; et al. Nationwide incidence of sarcomas and connective tissue tumors of intermediate malignancy over four years using an expert pathology review network. PLoS ONE 2021, 16, e0246958. [Google Scholar] [CrossRef] [PubMed]
- Gronchi, A.; Miah, A.B.; Dei Tos, A.P.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Blay, J.Y.; Bolle, S.; et al. Soft tissue and visceral sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up☆. Ann. Oncol. 2021, 32, 1348–1365. [Google Scholar] [CrossRef] [PubMed]
- Blay, J.Y.; Honoré, C.; Stoeckle, E.; Meeus, P.; Jafari, M.; Gouin, F.; Anract, P.; Ferron, G.; Rochwerger, A.; Ropars, M.; et al. Surgery in reference centers improves survival of sarcoma patients: A nationwide study. Ann. Oncol. 2019, 30, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekar, C.R.; Wafa, H.; Grimer, R.J.; Carter, S.R.; Tillman, R.M.; Abudu, A. The effect of an unplanned excision of a soft-tissue sarcoma on prognosis. J. Bone Jt. Surg. Br. 2008, 90, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Charoenlap, C.; Imanishi, J.; Tanaka, T.; Slavin, J.; Ngan, S.Y.; Chander, S.; Dowsey, M.M.; Goyal, C.; Choong, P.F. Outcomes of unplanned sarcoma excision: Impact of residual disease. Cancer Med. 2016, 5, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Kawai, A.; Sudo, A. The incidence of unplanned excision in patients with soft tissue sarcoma: Reports from the Bone and Soft Tissue Tumor registry in Japan. J. Orthop. Sci. 2022, 27, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Smolle, M.A.; Tunn, P.U.; Goldenitsch, E.; Posch, F.; Szkandera, J.; Bergovec, M.; Liegl-Atzwanger, B.; Leithner, A. The Prognostic Impact of Unplanned Excisions in a Cohort of 728 Soft Tissue Sarcoma Patients: A Multicentre Study. Ann. Surg. Oncol. 2017, 24, 1596–1605. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, E.J.; Ahmed, S.K.; Houdek, M.T. Extremity Soft Tissue Sarcoma: Role of Local Control. Curr. Treat. Opt. Oncol. 2020, 21, 13. [Google Scholar] [CrossRef] [PubMed]
- Von Mehren, M.; Randall, R.L.; Benjamin, R.S.; Boles, S.; Bui, M.M.; Ganjoo, K.N.; George, S.; Gonzalez, R.J.; Heslin, M.J.; Kane, J.M.; et al. Soft Tissue Sarcoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 536–563. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.M.; Kandel, R.A.; Wunder, J.S.; Unger, R.; Meer, J.; O’Sullivan, B.; Catton, C.N.; Bell, R.S. The impact of residual disease on local recurrence in patients treated by initial unplanned resection for soft tissue sarcoma of the extremity. J. Surg. Oncol. 1997, 66, 81–87. [Google Scholar] [CrossRef]
- Decanter, G.; Stoeckle, E.; Honore, C.; Meeus, P.; Mattei, J.C.; Dubray-Longeras, P.; Ferron, G.; Carrere, S.; Causeret, S.; Guilloit, J.-M.; et al. Watch and Wait Approach for Re-excision After Unplanned Yet Macroscopically Complete Excision of Extremity and Superficial Truncal Soft Tissue Sarcoma is Safe and Does Not Affect Metastatic Risk or Amputation Rate. Ann. Surg. Oncol. 2019, 26, 3526–3534. [Google Scholar] [CrossRef] [PubMed]
- Fiore, M.; Casali, P.G.; Miceli, R.; Mariani, L.; Bertulli, R.; Lozza, L.; Collini, P.; Olmi, P.; Mussi, C.; Gronchi, A. Prognostic effect of re-excision in adult soft tissue sarcoma of the extremity. Ann. Surg. Oncol. 2006, 13, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Eilber, F.R. The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J. Clin. Oncol. 1985, 3, 1344–1348. [Google Scholar] [CrossRef] [PubMed]
- Gouin, F.; Stoeckle, E.; Honoré, C.; Ropars, M.; Jafari, M.; Mattei, J.C.; Rochwerger, A.; Carrere, S.; Waast, D.; Ferron, G.; et al. Overall survival in patients with re-excision of positive microscopic margins of limb and trunk wall soft tissue sarcoma operated outside of a reference center: A nationwide cohort analysis. BMC Cancer 2022, 22, 1034. [Google Scholar] [CrossRef] [PubMed]
- Grimer, R.; Parry, M.; James, S. Inadvertent excision of malignant soft tissue tumours. EFORT Open Rev. 2019, 4, 321–329. [Google Scholar] [CrossRef]
- Nakamura, T.; Kawai, A.; Hagi, T.; Asanuma, K.; Sudo, A. A comparison of clinical outcomes between additional excision after unplanned and planned excisions in patients with soft-tissue sarcoma of the limb: A propensity matching cohort study. Bone Jt. J. 2021, 103-B, 1809–1814. [Google Scholar]
- Noria, S.; Davis, A.; Kandel, R.; Levesque, J.; O’Sullivan, B.; Wunder, J.; Bell, R. Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J. Bone Jt. Surg. Am. 1996, 78, 650–655. [Google Scholar] [CrossRef]
- Venkatesan, M.; Richards, C.J.; McCulloch, T.A.; Perks, A.G.B.; Raurell, A.; Ashford, R.U.; Service, E.M.S. Inadvertent surgical resection of soft tissue sarcomas. Eur. J. Surg. Oncol. 2012, 38, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Zagars, G.K.; Ballo, M.T.; Pisters, P.W.T.; Pollock, R.E.; Patel, S.R.; Benjamin, R.S. Surgical margins and reresection in the management of patients with soft tissue sarcoma using conservative surgery and radiation therapy. Cancer 2003, 97, 2544–2553. [Google Scholar] [CrossRef] [PubMed]
- Bonvalot, S.; Levy, A.; Terrier, P.; Tzanis, D.; Bellefqih, S.; Le Cesne, A.; Le Pechoux, C. Primary Extremity Soft Tissue Sarcomas: Does Local Control Impact Survival? Ann. Surg. Oncol. 2017, 24, 194–201. [Google Scholar] [CrossRef]
- Danieli, M.; Barretta, F.; Fiore, M.; Radaelli, S.; Sangalli, C.; Barisella, M.; Stacchiotti, S.; Palassini, E.; Miceli, R.; Callegaro, D.; et al. Unplanned Excision of Extremity and Trunk Wall Soft Tissue Sarcoma: To Re-resect or Not to Re-resect? Ann. Surg. Oncol. 2021, 28, 4706–4717. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, G.; Sambri, A.; Cammelli, S.; Galuppi, A.; Cortesi, A.; Righi, A.; Caldari, E.; Ferrari, S.; Donati, D. Impact of residual disease after “unplanned excision” of primary localized adult soft tissue sarcoma of the extremities: Evaluation of 452 cases at a single Institution. Musculoskelet. Surg. 2017, 101, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Guo, T.H.; Xu, B.S.; Hong, D.C.; Qiu, H.B.; Zhou, Z.W.; Zhang, X. The Impact of Unplanned Excision on the Outcomes of Patients With Soft Tissue Sarcoma of the Trunk and Extremity: A Propensity Score Matching Analysis. Front. Oncol. 2020, 10, 617590. [Google Scholar] [CrossRef] [PubMed]
- Rehders, A.; Stoecklein, N.H.; Poremba, C.; Alexander, A.; Knoefel, W.T.; Peiper, M. Reexcision of soft tissue sarcoma: Sufficient local control but increased rate of metastasis. World J. Surg. 2009, 33, 2599–2605. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, F.; Alsina, A.C.; Morganti, R.; Innocenti, M.; Andreani, L.; Muratori, F.; Scoccianti, G.; Totti, F.; Campanacci, D.A.; Capanna, R. Re-excision after unplanned excision of soft tissue sarcoma: A systematic review and metanalysis. The rationale of systematic re-excision. J. Orthop. 2021, 25, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Traub, F.; Griffin, A.M.; Wunder, J.S.; Ferguson, P.C. Influence of unplanned excisions on the outcomes of patients with stage III extremity soft-tissue sarcoma. Cancer 2018, 124, 3868–3875. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.J.; Leung, D.; Espat, J.; Woodruff, J.M.; Brennan, M.F. Effect of reresection in extremity soft tissue sarcoma. Ann. Surg. 2000, 231, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Wittekind, C.; Compton, C.C.; Greene, F.L.; Sobin, L.H. TNM residual tumor classification revisited. Cancer 2002, 94, 2511–2516. [Google Scholar] [CrossRef] [PubMed]
- Traweek, R.S.; Martin, A.N.; Rajkot, N.F.; Guadagnolo, B.A.; Bishop, A.J.; Lazar, A.J.; Keung, E.Z.; Torres, K.E.; Hunt, K.K.; Feig, B.W.; et al. Re-excision After Unplanned Excision of Soft Tissue Sarcoma is Associated with High Morbidity and Limited Pathologic Identification of Residual Disease. Ann. Surg. Oncol. 2023, 30, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Willeumier, J.; Fiocco, M.; Nout, R.; Dijkstra, S.; Aston, W.; Pollock, R.; Hartgrink, H.; Bovee, J.; Van De Sande, M. High-grade soft tissue sarcomas of the extremities: Surgical margins influence only local recurrence not overall survival. Int. Orthop. 2015, 39, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Takemori, T.; Kawamoto, T.; Hara, H.; Fukase, N.; Fujiwara, S.; Kitayama, K.; Yahiro, S.; Miyamoto, T.; Mifune, Y.; Hoshino, Y.; et al. Clinical Outcomes and Prognostic Factors in Soft Tissue Sarcoma Patients After Unplanned Excision. Cancer Manag. Res. 2022, 14, 1815–1824. [Google Scholar] [CrossRef] [PubMed]
- Potter, B.K.; Hwang, P.F.; Forsberg, J.A.; Hampton, C.B.; Graybill, J.C.; Peoples, G.E.; Stojadinovic, A. Impact of margin status and local recurrence on soft-tissue sarcoma outcomes. J. Bone Jt. Surg. Am. 2013, 95, e151. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, P.W.; Griffin, A.M.; Eward, W.C.; Sternheim, A.; Catton, C.N.; Chung, P.W.; O’Sullivan, B.; Ferguson, P.C.; Wunder, J.S. The effect of the setting of a positive surgical margin in soft tissue sarcoma. Cancer 2014, 120, 2866–2875. [Google Scholar] [CrossRef] [PubMed]
- Gronchi, A.; Lo Vullo, S.; Colombo, C.; Collini, P.; Stacchiotti, S.; Mariani, L.; Fiore, M.; Casali, P.G. Extremity soft tissue sarcoma in a series of patients treated at a single institution: Local control directly impacts survival. Ann. Surg. 2010, 251, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Trovik, C.S.; Bauer, H.C.; Alvegård, T.A.; Anderson, H.; Blomqvist, C.; Berlin, O.; Gustafson, P.; Sæter, G.; Wallöe, A. Surgical margins, local recurrence and metastasis in soft tissue sarcomas: 559 surgically-treated patients from the Scandinavian Sarcoma Group Register. Eur. J. Cancer 2000, 36, 710–716. [Google Scholar] [CrossRef]
- Saeed, H.; King, D.M.; Johnstone, C.A.; Charlson, J.A.; Hackbarth, D.A.; Neilson, J.C.; Bedi, M. Preoperative Radiation Therapy Followed by Reexcision May Improve Local Control and Progression-Free Survival in Unplanned Excisions of Soft Tissue Sarcomas of the Extremity and Chest-Wall. Int. J. Surg. Oncol. 2016, 2016, 5963167. [Google Scholar] [CrossRef] [PubMed]
- Samà, L.; Binder, J.P.; Darrigues, L.; Couturaud, B.; Boura, B.; Helfre, S.; Chiche, L.; Nicolas, N.; Tzanis, D.; Bouhadiba, T.; et al. Safe-margin surgery by plastic reconstruction in extremities or parietal trunk soft tissue sarcoma: A tertiary single centre experience. Eur. J. Surg. Oncol. 2022, 48, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.R.; Laupacis, A.; Hux, J.E.; Austin, P.C. Propensity score methods gave similar results to traditional regression modeling in observational studies: A systematic review. J. Clin. Epidemiol. 2005, 58, 550–559. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Re Excision | Total | Test | |||||
|---|---|---|---|---|---|---|---|
| No | Yes | ||||||
| N = 779 | N = 913 | N = 1692 | |||||
| Gender | Chi-2 p = 0.092 | ||||||
| Female | 374 | (48.0%) | 401 | (43.9%) | 775 | (45.8%) | |
| Male | 405 | (52.0%) | 512 | (56.1%) | 917 | (54.2%) | |
| Age at diagnosis | Kruskal-Wallis p = 0.010 | ||||||
| Mean (std) | 59.85 (20.39) | 57.79 (18.61) | 58.74 (19.47) | ||||
| Site of tumor | Chi-2 p ≤ 0.001 | ||||||
| Trunk/root member | 384 | (49.3%) | 329 | (36.0%) | 713 | (42.1%) | |
| Lower limb | 278 | (35.7%) | 411 | (45.0%) | 689 | (40.7%) | |
| Upper limb | 117 | (15.0%) | 173 | (18.9%) | 290 | (17.1%) | |
| Size of the tumor (mm) | Kruskal-Wallis p ≤ 0.001 | ||||||
| Mean (std) | 63.00 (53.22) | 45.97 (38.72) | 53.70 (46.63) | ||||
| Depth of the tumor | Chi-2 p = 0.002 | ||||||
| Missing data | 77 | 56 | 133 | ||||
| Deep (sub-facia) | 400 | (57.0%) | 422 | (49.2%) | 822 | (52.7%) | |
| Superficial (sus-facia) | 302 | (43.0%) | 435 | (50.8%) | 737 | (47.3%) | |
| Histology | Chi-2 p ≤ 0.001 | ||||||
| Leiomyosarcoma | 170 | (21.8%) | 237 | (26.0%) | 407 | (24.1%) | |
| Liposarcoma | 106 | (13.6%) | 88 | (9.6%) | 194 | (11.5%) | |
| Myxofibrosarcoma | 83 | (10.7%) | 161 | (17.6%) | 244 | (14.4%) | |
| Synovial sarcoma | 43 | (5.5%) | 41 | (4.5%) | 84 | (5.0%) | |
| Undifferentiated sarcoma | 152 | (19.5%) | 190 | (20.8%) | 342 | (20.2%) | |
| Miscellaneous sarcomas | 138 | (17.7%) | 112 | (12.3%) | 250 | (14.8%) | |
| Others ¥ | 87 | (11.2%) | 84 | (9.2%) | 171 | (10.1%) | |
| Grade of the tumor | Chi-2 p ≤ 0.001 | ||||||
| Missing data | 64 | 53 | 117 | ||||
| Grade 1 | 114 | (15.9%) | 146 | (17.0%) | 260 | (16.5%) | |
| Grade 2 | 189 | (26.4%) | 295 | (34.3%) | 484 | (30.7%) | |
| Grade 3 | 212 | (29.7%) | 249 | (29.0%) | 461 | (29.3%) | |
| Non gradable | 200 | (28.0%) | 170 | (19.8%) | 370 | (23.5%) | |
| Quality of 1st resection | Chi-2 p ≤ 0.001 | ||||||
| R0 | 355 | (45.6%) | 95 | (10.4%) | 450 | (26.6%) | |
| R1 | 424 | (54.4%) | 818 | (89.6%) | 1242 | (73.4%) | |
| 2nd surgery | |||||||
| Inside NETSARC | - | 647 | (70.9%) | 647 | (38.2%) | ||
| Outside NETSARC | - | 236 | (25.8%) | 236 | (13.9%) | ||
| Unknown | - | 30 | (3.3%) | 30 | (1.8%) | ||
| Quality after re-excision (RE) * | Chi-2 p ≤ 0.001 | ||||||
| R0 | 355 | (45.6%) | 778 | (85.2%) | 1133 | (67.0%) | |
| R1 | 424 | (54.4%) | 61 | (6.7%) | 485 | (28.7%) | |
| R2 | 0 | (0.0%) | 1 | (0.1%) | 1 | (0.1%) | |
| Margins not evaluable/not specified | 0 | (0.0%) | 73 | (8.0%) | 73 | (4.3%) | |
| Unadjusted HR | Adjusted HR Full Model 1 | Adjusted HR Full Model 2 | Adjusted HR Final Model | |
|---|---|---|---|---|
| Age at diagnosis | 1.013 (1.007–1.020); <0.0001 | 1.018 (1.009–1.026); <0.0001 | 1.017 (1.008–1.026); 0.0001 | 1.018 (1.009–1.026); <0.0001 |
| Gender female (ref: male) | 0.825 (0.646–1.053); 0.1227 | 0.765 (0.579–1.012); 0.0603 | 0.786 (0.593–1.040); 0.0920 | 0.773 (0.585–1.021); 0.0698 |
| Size of the tumor (ref: mm) | 1.006 (1.004–1.007); <0.0001 | 1.005 (1.003–1.007); <0.0001 | 1.005 (1.003–1.007); <0.0001 | 1.005 (1.003–1.007); <0.0001 |
| Site of tumor (ref: lower limb) | ||||
| Trunk/root member | 1.264 (0.970–1.646); 0.0829 | 1.085 (0.806–1.462); 0.5896 | 1.081 (0.800–1.461); 0.6107 | 1.088 (0.808–1.465); 0.5799 |
| Upper | 0.833 (0.577–1.202); 0.3277 | 0.861 (0.572–1.296); 0.4738 | 0.856 (0.568–1.291); 0.4588 | 0.856 (0.569–1.287); 0.4546 |
| Depth of tumor (ref: superficial) | 1.542 (1.177–2.020); 0.0017 | 1.304 (0.962–1.767); 0.0875 | 1.290 (0.950–1.751); 0.1027 | 1.291 (0.953–1.750); 0.0993 |
| Grade (ref: grades 1–2) | ||||
| Grade 3 | 2.481 (1.854–3.319); <0.0001 | 2.194 (1.571–3.066); <0.0001 | 2.197 (1.566–3.082); <0.0001 | 2.209 (1.581–3.086); <0.0001 |
| Not gradable | 1.402 (0.992–1.980); 0.0552 | 1.429 (0.713–2.862); 0.3141 | 1.370 (0.676–2.775); 0.3826 | 1.437 (0.716–2.881); 0.3076 |
| Histology (ref: others ¥) | ||||
| Leiomyosarcoma | 0.726 (0.457–1.153); 0.1747 | 1.003 (0.536–1.879); 0.9918 | 1.015 (0.540–1.909); 0.9625 | 0.989 (0.528–1.851); 0.9714 |
| Liposarcoma | 0.791 (0.487–1.286); 0.3446 | 0.541 (0.280–1.044); 0.0670 | 0.554 (0.284–1.082); 0.0838 | 0.527 (0.273–1.017); 0.0563 |
| Myxofibrosarcoma | 0.575 (0.345–0.957); 0.0334 | 0.625 (0.319–1.223); 0.1697 | 0.599 (0.303–1.182); 0.1395 | 0.615 (0.314–1.203); 0.1557 |
| Synovial sarcoma | 0.867 (0.478–1.573); 0.6390 | 1.571 (0.741–3.332); 0.2390 | 1.626 (0.765–3.456); 0.2063 | 1.559 (0.735–3.307); 0.2473 |
| Undifferentiated sarcoma | 0.966 (0.624–1.496); 0.8777 | 0.801 (0.440–1.457); 0.4667 | 0.777 (0.424–1.422); 0.4129 | 0.778 (0.428–1.412); 0.4086 |
| Miscelaneous sarcomas | 0.829 (0.521–1.319); 0.4283 | 0.824 (0.459–1.481); 0.5182 | 0.887 (0.489–1.607); 0.6919 | 0.826 (0.460–1.484); 0.5230 |
| Re-excision (RE) (ref: no re-excision (No-RE) | 0.571 (0.448–0.729); <0.0001 | 0.750 (0.552–1.019); 0.0656 | 0.734 (0.526–1.023); 0.0676 | 0.702 (0.531–0.929); 0.0132 |
| Quality of first surgery R0 (ref: R1 margin) | 1.525 (1.172–1.984); 0.0017 | 1.202 (0.862–1.676); 0.2785 | –– | – |
| Quality of final surgery R0 (ref: R1 margin) | 0.762 (0.589–0.987); 0.0394 | –– | 1.009 (0.712–1.430); 0.9614 | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gouin, F.; Michot, A.; Jafari, M.; Honoré, C.; Mattei, J.C.; Rochwerger, A.; Ropars, M.; Tzanis, D.; Anract, P.; Carrere, S.; et al. Improved Metastatic-Free Survival after Systematic Re-Excision Following Complete Macroscopic Unplanned Excision of Limb or Trunk Soft Tissue Sarcoma. Cancers 2024, 16, 1365. https://doi.org/10.3390/cancers16071365
Gouin F, Michot A, Jafari M, Honoré C, Mattei JC, Rochwerger A, Ropars M, Tzanis D, Anract P, Carrere S, et al. Improved Metastatic-Free Survival after Systematic Re-Excision Following Complete Macroscopic Unplanned Excision of Limb or Trunk Soft Tissue Sarcoma. Cancers. 2024; 16(7):1365. https://doi.org/10.3390/cancers16071365
Chicago/Turabian StyleGouin, Francois, Audrey Michot, Mehrdad Jafari, Charles Honoré, Jean Camille Mattei, Alexandre Rochwerger, Mickael Ropars, Dimitri Tzanis, Philippe Anract, Sébastien Carrere, and et al. 2024. "Improved Metastatic-Free Survival after Systematic Re-Excision Following Complete Macroscopic Unplanned Excision of Limb or Trunk Soft Tissue Sarcoma" Cancers 16, no. 7: 1365. https://doi.org/10.3390/cancers16071365
APA StyleGouin, F., Michot, A., Jafari, M., Honoré, C., Mattei, J. C., Rochwerger, A., Ropars, M., Tzanis, D., Anract, P., Carrere, S., Gangloff, D., Ducoulombier, A., Lebbe, C., Guiramand, J., Waast, D., Marchal, F., Sirveaux, F., Causeret, S., Gimbergues, P., ... Blay, J. -Y., on behalf of the NETSARC/RREPS and French Sarcoma Group-Groupe d’Etude des Tumeurs Osseuses (GSF-GETO) Networks. (2024). Improved Metastatic-Free Survival after Systematic Re-Excision Following Complete Macroscopic Unplanned Excision of Limb or Trunk Soft Tissue Sarcoma. Cancers, 16(7), 1365. https://doi.org/10.3390/cancers16071365