
MRI–Ultrasound Fused Approach for Prostate Biopsy—How It Is Performed


Abstract
:Simple Summary
Abstract
1. Introduction
2. mpMRI and Identification of Lesions
3. Current Indications
4. Overview of mpMRI-Guided Biopsy Techniques
4.1. Cognitive Fusion
4.2. mpMRI–TRUS Fusion
4.3. Direct In-Bore/In-Gantry
5. Comparative Effectiveness
5.1. mpMRI-Guided versus Systematic TRUS Biopsy
5.2. Comparison across mpMRI-Guided Biopsy Techniques
5.3. TP vs. TR Approach
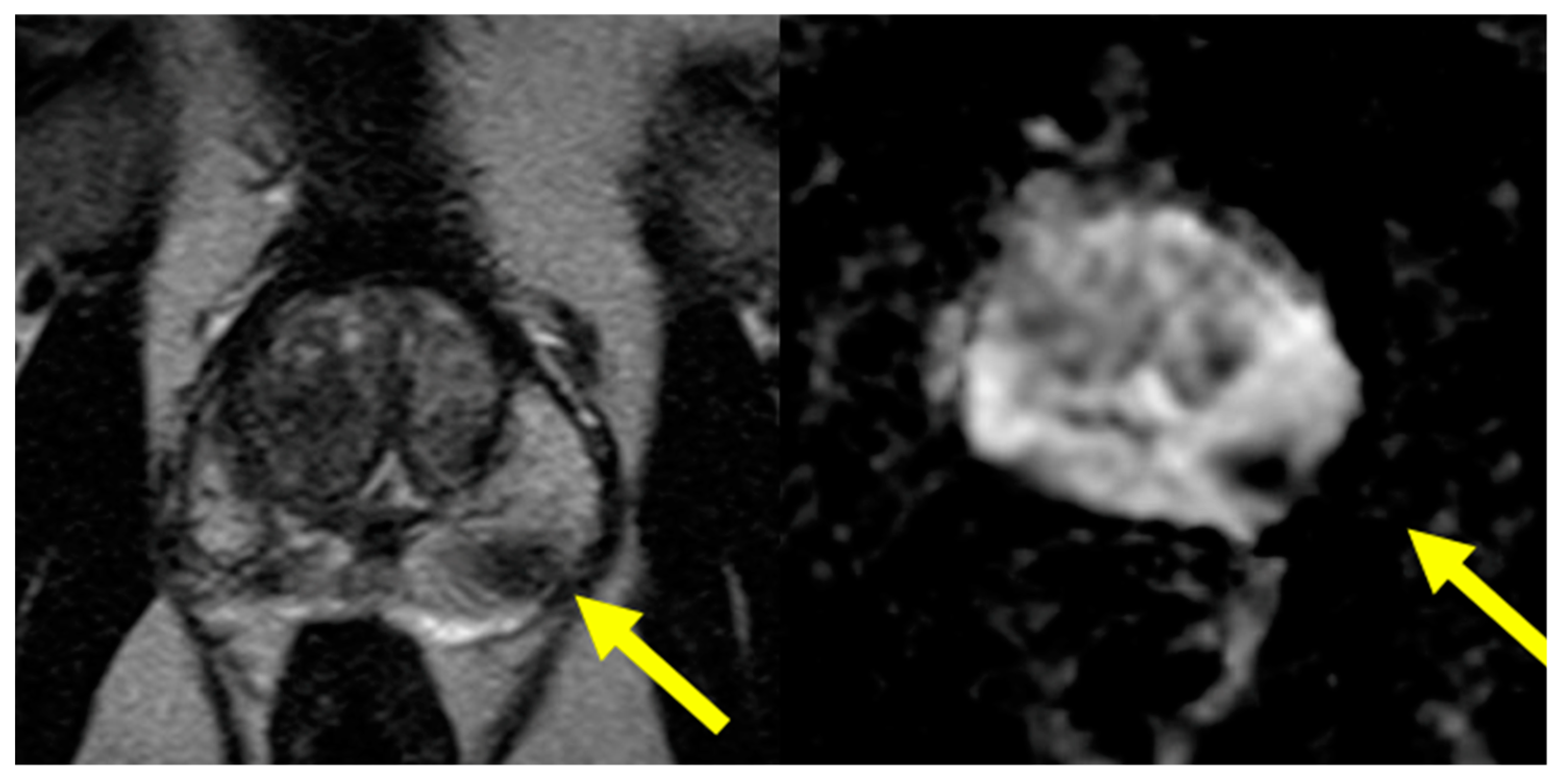
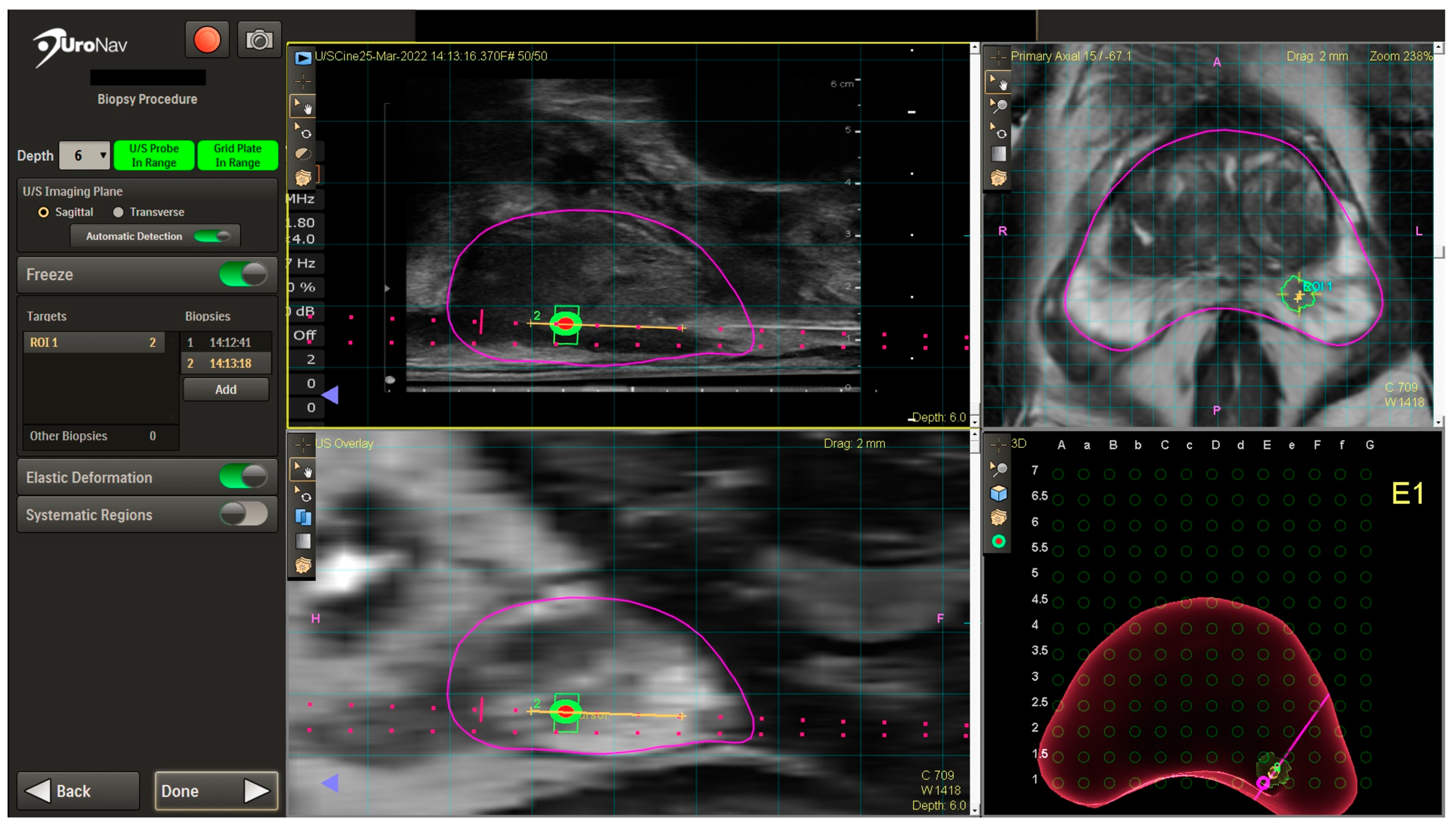
5.4. Case Presentation
5.5. Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Connor, M.J.; Gorin, M.A.; Eldred-Evans, D.; Bass, E.J.; Desai, A.; Dudderidge, T.; Winkler, M.; Ahmed, H.U. Landmarks in the evolution of prostate biopsy. Nat. Rev. Urol. 2023, 20, 241–258. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.M.; Rais-Bahrami, S.; Truong, H.; Stamatakis, L.; Vourganti, S.; Nix, J.; Hoang, A.N.; Walton-Diaz, A.; Shuch, B.; Weintraub, M.; et al. Magnetic resonance imaging/ultrasound-fusion biopsy significantly upgrades prostate cancer versus systematic 12-core transrectal ultrasound biopsy. Eur. Urol. 2013, 64, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Serefoglu, E.C.; Altinova, S.; Ugras, N.S.; Akincioglu, E.; Asil, E.; Balbay, M.D. How reliable is 12-core prostate biopsy procedure in the detection of prostate cancer? Can. Urol. Assoc. J. 2013, 7, E293–E298. [Google Scholar] [CrossRef] [PubMed]
- Drost, F.-J.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst. Rev. 2019, 4, CD012663. [Google Scholar] [CrossRef] [PubMed]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. PRECISION Study Group Collaborators MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. PROMIS study group Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Schoots, I.G.; Roobol, M.J.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Hunink, M.G.M. Magnetic resonance imaging-targeted biopsy may enhance the diagnostic accuracy of significant prostate cancer detection compared to standard transrectal ultrasound-guided biopsy: A systematic review and meta-analysis. Eur. Urol. 2015, 68, 438–450. [Google Scholar] [CrossRef]
- van der Leest, M.; Cornel, E.; Israël, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-head Comparison of Transrectal Ultrasound-guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-guided Biopsy in Biopsy-naïve Men with Elevated Prostate-specific Antigen: A Large Prospective Multicenter Clinical Study. Eur. Urol. 2019, 75, 570–578. [Google Scholar] [CrossRef]
- Kvåle, R.; Møller, B.; Wahlqvist, R.; Fosså, S.D.; Berner, A.; Busch, C.; Kyrdalen, A.E.; Svindland, A.; Viset, T.; Halvorsen, O.J. Concordance between Gleason scores of needle biopsies and radical prostatectomy specimens: A population-based study. BJU Int. 2009, 103, 1647–1654. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.R.; Ansbro, B.; Shah, P.V.; Aguiar, J.A.; Li, E.V.; Rich, J.M.; Mahenthiran, A.K.; Moataz, S.A.S.; Keeter, M.-K.; Mai, Q.; et al. Real-world use of MRI for risk stratification prior to prostate biopsy. Prostate Cancer Prostatic Dis. 2023, 26, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.; Abdulkareem, R.; Nasrollah, D.; Ljung, A.; Hintze, P.; Wallby, S.; Ståhlbrandt, H.; Frennvall, T.; Styrke, J.; Stattin, P.; et al. Frequency of biopsy and tumor grade before vs after introduction of prostate magnetic resonance imaging. JAMA Netw. Open 2023, 6, e2330233. [Google Scholar] [CrossRef]
- Stabile, A.; Giganti, F.; Rosenkrantz, A.B.; Taneja, S.S.; Villeirs, G.; Gill, I.S.; Allen, C.; Emberton, M.; Moore, C.M.; Kasivisvanathan, V. Multiparametric MRI for prostate cancer diagnosis: Current status and future directions. Nat. Rev. Urol. 2020, 17, 41–61. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Diagnostic Performance of Prostate Imaging Reporting and Data System Version 2 for Detection of Prostate Cancer: A Systematic Review and Diagnostic Meta-analysis. Eur. Urol. 2017, 72, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.; Misser, S.K.; Cioni, D.; Neri, E. PI-RADS v2.1: What has changed and how to report. SA J. Radiol. 2021, 25, 2062. [Google Scholar] [CrossRef] [PubMed]
- PI-RADS|American College of Radiology. Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/PI-RADS (accessed on 12 February 2024).
- Park, K.J.; Choi, S.H.; Kim, M.-H.; Kim, J.K.; Jeong, I.G. Performance of Prostate Imaging Reporting and Data System Version 2.1 for Diagnosis of Prostate Cancer: A Systematic Review and Meta-Analysis. J. Magn. Reson. Imaging 2021, 54, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Park, K.J.; Choi, S.H.; Lee, J.S.; Kim, J.K.; Kim, M.-H.; Jeong, I.G. Risk Stratification of Prostate Cancer According to PI-RADS® Version 2 Categories: Meta-Analysis for Prospective Studies. J. Urol. 2020, 204, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Camacho, A.; Salah, F.; Bay, C.P.; Waring, J.; Umeton, R.; Hirsch, M.S.; Cole, A.P.; Kibel, A.S.; Loda, M.; Tempany, C.M.; et al. PI-RADS 3 score: A retrospective experience of clinically significant prostate cancer detection. BJUI Compass 2023, 4, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Fang, A.M.; Shumaker, L.A.; Martin, K.D.; Jackson, J.C.; Fan, R.E.; Khajir, G.; Patel, H.D.; Soodana-Prakash, N.; Vourganti, S.; Filson, C.P.; et al. Multi-institutional analysis of clinical and imaging risk factors for detecting clinically significant prostate cancer in men with PI-RADS 3 lesions. Cancer 2022, 128, 3287–3296. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Early Detection of Prostate Cancer: AUA/SUO Guideline (2023)—American Urological Association. Available online: https://www.auanet.org/guidelines-and-quality/guidelines/early-detection-of-prostate-cancer-guidelines (accessed on 13 February 2024).
- Wei, J.T.; Barocas, D.; Carlsson, S.; Coakley, F.; Eggener, S.; Etzioni, R.; Fine, S.W.; Han, M.; Kim, S.K.; Kirkby, E.; et al. Early detection of prostate cancer: AUA/SUO guideline part I: Prostate cancer screening. J. Urol. 2023, 210, 46–53. [Google Scholar] [CrossRef]
- Fedorov, A.; Khallaghi, S.; Sánchez, C.A.; Lasso, A.; Fels, S.; Tuncali, K.; Sugar, E.N.; Kapur, T.; Zhang, C.; Wells, W.; et al. Open-source image registration for MRI-TRUS fusion-guided prostate interventions. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 925–934. [Google Scholar] [CrossRef]
- Sparks, R.; Bloch, B.N.; Feleppa, E.; Barratt, D.; Madabhushi, A. Fully automated prostate magnetic resonance imaging and transrectal ultrasound fusion via a probabilistic registration metric. Proc. SPIE 2013, 8671, 72–85. [Google Scholar] [CrossRef]
- Chang, S.D.; Ghai, S.; Kim, C.K.; Oto, A.; Giganti, F.; Moore, C.M. MRI targeted prostate biopsy techniques: AJR expert panel narrative review. AJR Am. J. Roentgenol. 2021, 217, 1263–1281. [Google Scholar] [CrossRef]
- Venderink, W.; de Rooij, M.; Sedelaar, J.P.M.; Huisman, H.J.; Fütterer, J.J. Elastic Versus Rigid Image Registration in Magnetic Resonance Imaging-transrectal Ultrasound Fusion Prostate Biopsy: A Systematic Review and Meta-analysis. Eur. Urol. Focus 2018, 4, 219–227. [Google Scholar] [CrossRef]
- Lenfant, L.; Beitone, C.; Troccaz, J.; Rouprêt, M.; Seisen, T.; Voros, S.; Mozer, P.C. Learning curve for fusion magnetic resonance imaging targeted prostate biopsy and three-dimensional transrectal ultrasonography segmentation. BJU Int. 2024; early view. [Google Scholar] [CrossRef]
- Taha, F.; Larre, S.; Branchu, B.; ReSurg. Surgeon seniority and experience have no effect on CaP detection rates using MRI/TRUS fusion-guided targeted biopsies. Urol. Oncol. 2024, 42, 67.e1–67.e7. [Google Scholar] [CrossRef]
- Overduin, C.G.; Fütterer, J.J.; Barentsz, J.O. MRI-guided biopsy for prostate cancer detection: A systematic review of current clinical results. Curr. Urol. Rep. 2013, 14, 209–213. [Google Scholar] [CrossRef]
- Beyersdorff, D.; Winkel, A.; Hamm, B.; Lenk, S.; Loening, S.A.; Taupitz, M. MR imaging-guided prostate biopsy with a closed MR unit at 1.5 T: Initial results. Radiology 2005, 234, 576–581. [Google Scholar] [CrossRef]
- Venderink, W.; Govers, T.M.; de Rooij, M.; Fütterer, J.J.; Sedelaar, J.P.M. Cost-Effectiveness Comparison of Imaging-Guided Prostate Biopsy Techniques: Systematic Transrectal Ultrasound, Direct In-Bore MRI, and Image Fusion. AJR Am. J. Roentgenol. 2017, 208, 1058–1063. [Google Scholar] [CrossRef]
- Goldberg, H.; Ahmad, A.E.; Chandrasekar, T.; Klotz, L.; Emberton, M.; Haider, M.A.; Taneja, S.S.; Arora, K.; Fleshner, N.; Finelli, A.; et al. Comparison of Magnetic Resonance Imaging and Transrectal Ultrasound Informed Prostate Biopsy for Prostate Cancer Diagnosis in Biopsy Naïve Men: A Systematic Review and Meta-Analysis. J. Urol. 2020, 203, 1085–1093. [Google Scholar] [CrossRef]
- Rouse, P.; Shaw, G.; Ahmed, H.U.; Freeman, A.; Allen, C.; Emberton, M. Multi-parametric magnetic resonance imaging to rule-in and rule-out clinically important prostate cancer in men at risk: A cohort study. Urol. Int. 2011, 87, 49–53. [Google Scholar] [CrossRef]
- Puech, P.; Rouvière, O.; Renard-Penna, R.; Villers, A.; Devos, P.; Colombel, M.; Bitker, M.-O.; Leroy, X.; Mège-Lechevallier, F.; Comperat, E.; et al. Prostate cancer diagnosis: Multiparametric MR-targeted biopsy with cognitive and transrectal US-MR fusion guidance versus systematic biopsy--prospective multicenter study. Radiology 2013, 268, 461–469. [Google Scholar] [CrossRef]
- Zheng, T.; Bi, K.; Tang, Y.; Zeng, Y.; Wang, J.; Yan, L. Cognitive fusion-targeted biopsy versus transrectal ultrasonography-guided systematic biopsy: Comparison and analysis of the risk of Gleason score upgrading. Int. Urol. Nephrol. 2024, 56, 981–988. [Google Scholar] [CrossRef]
- Bass, E.J.; Pantovic, A.; Connor, M.J.; Loeb, S.; Rastinehad, A.R.; Winkler, M.; Gabe, R.; Ahmed, H.U. Diagnostic accuracy of magnetic resonance imaging targeted biopsy techniques compared to transrectal ultrasound guided biopsy of the prostate: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2022, 25, 174–179. [Google Scholar] [CrossRef]
- Kasivisvanathan, V.; Dufour, R.; Moore, C.M.; Ahmed, H.U.; Abd-Alazeez, M.; Charman, S.C.; Freeman, A.; Allen, C.; Kirkham, A.; van der Meulen, J.; et al. Transperineal magnetic resonance image targeted prostate biopsy versus transperineal template prostate biopsy in the detection of clinically significant prostate cancer. J. Urol. 2013, 189, 860–866. [Google Scholar] [CrossRef]
- Wegelin, O.; van Melick, H.H.E.; Hooft, L.; Bosch, J.L.H.R.; Reitsma, H.B.; Barentsz, J.O.; Somford, D.M. Comparing Three Different Techniques for Magnetic Resonance Imaging-targeted Prostate Biopsies: A Systematic Review of In-bore versus Magnetic Resonance Imaging-transrectal Ultrasound fusion versus Cognitive Registration. Is There a Preferred Technique? Eur. Urol. 2017, 71, 517–531. [Google Scholar] [CrossRef]
- Connor, M.J.; Eldred-Evans, D.; van Son, M.; Hosking-Jervis, F.; Bertoncelli Tanaka, M.; Reddy, D.; Bass, E.J.; Powell, L.; Ahmad, S.; Pegers, E.; et al. A Multicenter Study of the Clinical Utility of Nontargeted Systematic Transperineal Prostate Biopsies in Patients Undergoing Pre-Biopsy Multiparametric Magnetic Resonance Imaging. J. Urol. 2020, 204, 1195–1201. [Google Scholar] [CrossRef]
- Miah, S.; Hosking-Jervis, F.; Connor, M.J.; Eldred-Evans, D.; Shah, T.T.; Arya, M.; Barber, N.; Bhardwa, J.; Bott, S.; Burke, D.; et al. A Multicentre Analysis of the Detection of Clinically Significant Prostate Cancer Following Transperineal Image-fusion Targeted and Nontargeted Systematic Prostate Biopsy in Men at Risk. Eur. Urol. Oncol 2020, 3, 262–269. [Google Scholar] [CrossRef]
- Elkhoury, F.F.; Felker, E.R.; Kwan, L.; Sisk, A.E.; Delfin, M.; Natarajan, S.; Marks, L.S. Comparison of targeted vs systematic prostate biopsy in men who are biopsy naive: The prospective assessment of image registration in the diagnosis of prostate cancer (PAIREDCAP) study. JAMA Surg. 2019, 154, 811–818. [Google Scholar] [CrossRef]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. MRI-FIRST Investigators Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef]
- Ahdoot, M.; Wilbur, A.R.; Reese, S.E.; Lebastchi, A.H.; Mehralivand, S.; Gomella, P.T.; Bloom, J.; Gurram, S.; Siddiqui, M.; Pinsky, P.; et al. MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. N. Engl. J. Med. 2020, 382, 917–928. [Google Scholar] [CrossRef]
- Wei, C.; Szewczyk-Bieda, M.; Bates, A.S.; Donnan, P.T.; Rauchhaus, P.; Gandy, S.; Ragupathy, S.K.A.; Singh, P.; Coll, K.; Serhan, J.; et al. Multicenter Randomized Trial Assessing MRI and Image-guided Biopsy for Suspected Prostate Cancer: The MULTIPROS Study. Radiology 2023, 308, e221428. [Google Scholar] [CrossRef]
- Thompson, A.; Eguru, V.; Moosa, S.; Ng, Y. Do concomitant systematic biopsies add to fusion targeted biopsies in the diagnosis and management of clinically significant prostate cancer? Urol. Res. Pract. 2023, 49, 169–177. [Google Scholar] [CrossRef]
- Novara, G.; Zattoni, F.; Zecchini, G.; Aceti, A.; Pellizzari, A.; Ferraioli, G.; Cobacchini, C.; Taverna, A.; Sattin, F.; Carletti, F.; et al. Role of targeted biopsy, perilesional biopsy, random biopsy, and their combination in the detection of clinically significant prostate cancer by mpMRI/transrectal ultrasonography fusion biopsy in confirmatory biopsy during active surveillance program. Prostate Cancer Prostatic Dis. 2024, 27, 129–135. [Google Scholar] [CrossRef]
- Brisbane, W.G.; Priester, A.M.; Ballon, J.; Kwan, L.; Delfin, M.K.; Felker, E.R.; Sisk, A.E.; Hu, J.C.; Marks, L.S. Targeted prostate biopsy: Umbra, penumbra, and value of perilesional sampling. Eur. Urol. 2022, 82, 303–310. [Google Scholar] [CrossRef]
- Williams, C.; Ahdoot, M.; Daneshvar, M.A.; Hague, C.; Wilbur, A.R.; Gomella, P.T.; Shih, J.; Khondakar, N.; Yerram, N.; Mehralivand, S.; et al. Why Does Magnetic Resonance Imaging-Targeted Biopsy Miss Clinically Significant Cancer? J. Urol. 2022, 207, 95–107. [Google Scholar] [CrossRef]
- Wegelin, O.; Exterkate, L.; van der Leest, M.; Kummer, J.A.; Vreuls, W.; de Bruin, P.C.; Bosch, J.L.H.R.; Barentsz, J.O.; Somford, D.M.; van Melick, H.H.E. The FUTURE Trial: A Multicenter Randomised Controlled Trial on Target Biopsy Techniques Based on Magnetic Resonance Imaging in the Diagnosis of Prostate Cancer in Patients with Prior Negative Biopsies. Eur. Urol. 2019, 75, 582–590. [Google Scholar] [CrossRef]
- Osses, D.F.; van Asten, J.J.; Tijsterman, J.D. Cognitive-Targeted versus Magnetic Resonance Imaging-Guided Prostate Biopsy in Prostate Cancer Detection. Curr. Urol. 2018, 11, 182–188. [Google Scholar] [CrossRef]
- Cool, D.W.; Zhang, X.; Romagnoli, C.; Izawa, J.I.; Romano, W.M.; Fenster, A. Evaluation of MRI-TRUS fusion versus cognitive registration accuracy for MRI-targeted, TRUS-guided prostate biopsy. AJR Am. J. Roentgenol. 2015, 204, 83–91. [Google Scholar] [CrossRef]
- Delongchamps, N.B.; Peyromaure, M.; Schull, A.; Beuvon, F.; Bouazza, N.; Flam, T.; Zerbib, M.; Muradyan, N.; Legman, P.; Cornud, F. Prebiopsy magnetic resonance imaging and prostate cancer detection: Comparison of random and targeted biopsies. J. Urol. 2013, 189, 493–499. [Google Scholar] [CrossRef]
- Watts, K.L.; Frechette, L.; Muller, B.; Ilinksy, D.; Kovac, E.; Sankin, A.; Aboumohamed, A. Systematic review and meta-analysis comparing cognitive vs. image-guided fusion prostate biopsy for the detection of prostate cancer. Urol. Oncol. 2020, 38, 734.e19. [Google Scholar] [CrossRef]
- Wysock, J.S.; Rosenkrantz, A.B.; Huang, W.C.; Stifelman, M.D.; Lepor, H.; Deng, F.-M.; Melamed, J.; Taneja, S.S. A prospective, blinded comparison of magnetic resonance (MR) imaging-ultrasound fusion and visual estimation in the performance of MR-targeted prostate biopsy: The PROFUS trial. Eur. Urol. 2014, 66, 343–351. [Google Scholar] [CrossRef]
- Lee, D.J.; Recabal, P.; Sjoberg, D.D.; Thong, A.; Lee, J.K.; Eastham, J.A.; Scardino, P.T.; Vargas, H.A.; Coleman, J.; Ehdaie, B. Comparative effectiveness of targeted prostate biopsy using magnetic resonance imaging ultrasound fusion software and visual targeting: A prospective study. J. Urol. 2016, 196, 697–702. [Google Scholar] [CrossRef]
- Ho, K.; Zhu, D.; Gupta, K.; Loloi, J.; Abramson, M.; Watts, K.; Agalliu, I.; Sankin, A. Performance of cognitive vs. image-guided fusion biopsy for detection of overall and clinically significant prostate cancer in a multiethnic population. Urol. Oncol. 2024, 42, e1–e29. [Google Scholar] [CrossRef]
- Pirola, G.M.; Castellani, D.; Orecchia, L.; Giulioni, C.; Gubbiotti, M.; Rubilotta, E.; Maggi, M.; Teoh, J.Y.-C.; Gauhar, V.; Naselli, A. Transperineal US-MRI Fusion-Guided Biopsy for the Detection of Clinical Significant Prostate Cancer: A Systematic Review and Meta-Analysis Comparing Cognitive and Software-Assisted Technique. Cancers 2023, 15, 3443. [Google Scholar] [CrossRef]
- Claros, O.R.; Tourinho-Barbosa, R.R.; Fregeville, A.; Gallardo, A.C.; Muttin, F.; Carneiro, A.; Stabile, A.; Moschini, M.; Macek, P.; Cathala, N.; et al. Comparison of Initial Experience with Transrectal Magnetic Resonance Imaging Cognitive Guided Micro-Ultrasound Biopsies versus Established Transperineal Robotic Ultrasound Magnetic Resonance Imaging Fusion Biopsies for Prostate Cancer. J. Urol. 2020, 203, 918–925. [Google Scholar] [CrossRef]
- Klotz, L.; Lughezzani, G.; Maffei, D.; Sánchez, A.; Pereira, J.G.; Staerman, F.; Cash, H.; Luger, F.; Lopez, L.; Sanchez-Salas, R.; et al. Comparison of micro-ultrasound and multiparametric magnetic resonance imaging for prostate cancer: A multicenter, prospective analysis. Can. Urol. Assoc. J. 2021, 15, E11–E16. [Google Scholar] [CrossRef]
- Calace, F.P.; Napolitano, L.; Arcaniolo, D.; Stizzo, M.; Barone, B.; Crocetto, F.; Olivetta, M.; Amicuzi, U.; Cirillo, L.; Rubinacci, A.; et al. Micro-Ultrasound in the Diagnosis and Staging of Prostate and Bladder Cancer: A Comprehensive Review. Medicina 2022, 58, 1624. [Google Scholar] [CrossRef]
- Prince, M.; Foster, B.R.; Kaempf, A.; Liu, J.-J.; Amling, C.L.; Isharwal, S.; Chen, Y.; Coakley, F.V. In-Bore Versus Fusion MRI-Targeted Biopsy of PI-RADS Category 4 and 5 Lesions: A Retrospective Comparative Analysis Using Propensity Score Weighting. AJR Am. J. Roentgenol. 2021, 217, 1123–1130. [Google Scholar] [CrossRef]
- Venderink, W.; van der Leest, M.; van Luijtelaar, A.; van de Ven, W.J.M.; Fütterer, J.J.; Sedelaar, J.P.M.; Huisman, H.J. Retrospective comparison of direct in-bore magnetic resonance imaging (MRI)-guided biopsy and fusion-guided biopsy in patients with MRI lesions which are likely or highly likely to be clinically significant prostate cancer. World J. Urol. 2017, 35, 1849–1855. [Google Scholar] [CrossRef]
- Kaufmann, S.; Russo, G.I.; Bamberg, F.; Löwe, L.; Morgia, G.; Nikolaou, K.; Stenzl, A.; Kruck, S.; Bedke, J. Prostate cancer detection in patients with prior negative biopsy undergoing cognitive-, robotic- or in-bore MRI target biopsy. World J. Urol. 2018, 36, 761–768. [Google Scholar] [CrossRef]
- Arsov, C.; Rabenalt, R.; Blondin, D.; Quentin, M.; Hiester, A.; Godehardt, E.; Gabbert, H.E.; Becker, N.; Antoch, G.; Albers, P.; et al. Prospective randomized trial comparing magnetic resonance imaging (MRI)-guided in-bore biopsy to MRI-ultrasound fusion and transrectal ultrasound-guided prostate biopsy in patients with prior negative biopsies. Eur. Urol. 2015, 68, 713–720. [Google Scholar] [CrossRef]
- Chung, Y.; Hong, S.K. Shifting to transperineal prostate biopsy: A narrative review. Prostate Int. 2023, 12, 10–14. [Google Scholar] [CrossRef]
- Tzeng, M.; Basourakos, S.P.; Patel, H.D.; Allaway, M.J.; Hu, J.C.; Gorin, M.A. Pooled outcomes of performing freehand transperineal prostate biopsy with the PrecisionPoint Transperineal Access System. BJUI Compass 2022, 3, 434–442. [Google Scholar] [CrossRef]
- Gereta, S.; Hung, M.; Alexanderani, M.K.; Robinson, B.D.; Hu, J.C. Evaluating the Learning Curve for In-office Freehand Cognitive Fusion Transperineal Prostate Biopsy. Urology 2023, 181, 31–37. [Google Scholar] [CrossRef]
- Uleri, A.; Baboudjian, M.; Tedde, A.; Gallioli, A.; Long-Depaquit, T.; Palou, J.; Basile, G.; Gaya, J.M.; Sanguedolce, F.; Lughezzani, G.; et al. Is There an Impact of Transperineal Versus Transrectal Magnetic Resonance Imaging-targeted Biopsy in Clinically Significant Prostate Cancer Detection Rate? A Systematic Review and Meta-analysis. Eur. Urol. Oncol 2023, 6, 621–628. [Google Scholar] [CrossRef]
- Hu, J.C.; Assel, M.; Allaf, M.E.; Ehdaie, B.; Vickers, A.J.; Cohen, A.J.; Ristau, B.T.; Green, D.A.; Han, M.; Rezaee, M.E.; et al. Transperineal Versus Transrectal Magnetic Resonance Imaging-targeted and Systematic Prostate Biopsy to Prevent Infectious Complications: The PREVENT Randomized Trial. Eur. Urol. 2024, in press. [Google Scholar] [CrossRef]
- Bryant, R.J.; Yamamoto, H.; Eddy, B.; Kommu, S.; Narahari, K.; Omer, A.; Leslie, T.; Catto, J.W.F.; Rosario, D.J.; Good, D.W.; et al. Protocol for the TRANSLATE prospective, multicentre, randomised clinical trial of prostate biopsy technique. BJU Int. 2023, 131, 694–704. [Google Scholar] [CrossRef]
- Kosarek, C.D.; Mahmoud, A.M.; Eyzaguirre, E.J.; Shan, Y.; Walser, E.M.; Horn, G.L.; Williams, S.B. Initial series of magnetic resonance imaging (MRI)-fusion targeted prostate biopsy using the first transperineal targeted platform available in the USA. BJU Int. 2018, 122, 909–912. [Google Scholar] [CrossRef]
- Yang, C.; Li, B.; Luan, Y.; Wang, S.; Bian, Y.; Zhang, J.; Wang, Z.; Liu, B.; Chen, X.; Hacker, M. Deep learning model for the detection of prostate cancer and classification of clinically significant disease using multiparametric MRI in comparison to PI-RADs score. Urol. Oncol. 2024, in press. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zheng, H.; Liang, Z.; Miao, Q.; Brisbane, W.G.; Marks, L.S.; Raman, S.S.; Reiter, R.E.; Yang, G.; Sung, K. Textured-Based Deep Learning in Prostate Cancer Classification with 3T Multiparametric MRI: Comparison with PI-RADS-Based Classification. Diagnostics 2021, 11, 1785. [Google Scholar] [CrossRef] [PubMed]
- Sushentsev, N.; Moreira Da Silva, N.; Yeung, M.; Barrett, T.; Sala, E.; Roberts, M.; Rundo, L. Comparative performance of fully-automated and semi-automated artificial intelligence methods for the detection of clinically significant prostate cancer on MRI: A systematic review. Insights Imaging 2022, 13, 59. [Google Scholar] [CrossRef] [PubMed]
- Basso Dias, A.; Ghai, S. Micro-Ultrasound: Current Role in Prostate Cancer Diagnosis and Future Possibilities. Cancers 2023, 15, 1280. [Google Scholar] [CrossRef]
- Klotz, L.; Andriole, G.; Cash, H.; Cooperberg, M.; Crawford, E.D.; Emberton, M.; Gomez-Sancha, F.; Klein, E.; Lughezzani, G.; Marks, L.; et al. Optimization of prostate biopsy—Micro-Ultrasound versus MRI (OPTIMUM): A 3-arm randomized controlled trial evaluating the role of 29 MHz micro-ultrasound in guiding prostate biopsy in men with clinical suspicion of prostate cancer. Contemp. Clin. Trials 2022, 112, 106618. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Society—Guideline | Statement(s) | Recommendation (Grade) |
|---|---|---|
| AUA/SUO— Early Detection of Prostate Cancer | Clinicians may use MRI prior to initial biopsy to increase the detection of GG2+ | Conditional Recommendation; Evidence Level (Grade B) |
| For biopsy-naïve patients who have a suspicious lesion on MRI, clinicians should perform targeted biopsies of the suspicious lesion and may also perform a systematic template biopsy. | Moderate Recommendation [targeted biopsies]/Conditional Recommendation [systematic template biopsy]; Evidence Level (Grade C) | |
| In patients undergoing repeat biopsy with no prior prostate MRI, clinicians should obtain a prostate MRI prior to biopsy. | Strong Recommendation; Evidence Level: Grade C) | |
| In patients undergoing repeat biopsy and who have a suspicious lesion on MRI, clinicians should perform targeted biopsies of the suspicious lesion and may also perform a systematic template biopsy. | Moderate Recommendation [targeted biopsies]/Conditional Recommendation [systematic template biopsy] Evidence Level: Grade C | |
| Clinicians may use software registration of MRI and ultrasound images during fusion biopsy, when available. | Expert Opinion | |
| Clinicians should obtain at least 2 needle biopsy cores per target in patients with suspicious prostate lesion(s) on MRI. | Moderate Recommendation; Evidence Level: Grade C | |
| European Association of Urology/European Association of Nuclear Medicine/European Society for Radiotherapy and Oncology/European Society of Urogenital Radiology/International Society of Urological Pathology/International Society of Geriatric Oncology (EAU/EANM/ESTRO/ESUR/ISUP/SIOG)— Guidelines on Prostate Cancer | Guidelines for MRI in biopsy decision Recommendations in biopsy-naïve patients | |
| Perform MRI before prostate biopsy. | Strong | |
| When MRI is positive (i.e., PI-RADS ≥ 3), combine targeted and systematic biopsy | Strong | |
| Recommendations in patients with prior negative biopsy | ||
| Perform MRI before prostate biopsy | Strong | |
| When MRI is positive (i.e., PI-RADS ≥ 3), perform targeted biopsy only. | Weak | |
| Guidelines for first-line treatment of various disease stages Active Surveillance | ||
| Perform MRI before a confirmatory biopsy if no MRI has been performed before the initial biopsy | Strong | |
| Take both targeted biopsy (of any PI-RADS ≥ 3 lesion) and systematic biopsy if a confirmatory biopsy is performed. | Weak | |
| If a patient has had upfront MRI followed by systematic and targeted biopsies there is no need for confirmatory biopsies | Weak | |
| NCCN—Prostate Cancer Early Detection | Further evaluation and indications for biopsy | |
| mpMRI if available High suspicion for clinically significant cancer: Image-guided biopsy via TR or TP approach with MRI targeting (preferred) or without MRI targeting | It is strongly recommended that image-guided biopsy techniques be employed routinely | |
| Management of biopsy results | ||
| Atypical intraductal proliferation (AIP) without invasive carcinoma Repeat biopsy using MRI targeting and systematic biopsy to look for invasive carcinoma | AIP is potentially considered a marker of unsampled cancer, and it is associated with an increased risk (50%) of invasive carcinoma and/or intraductal carcinoma on repeat biopsy | |
| Vendor/Device | Ultrasound | Tracking Mechanism | Biopsy Route | FDA 510(k) |
|---|---|---|---|---|
| Invivo(Philips) UroNav | Manual sweep | Electromagnetic | Transrectal, ṗ transperineal | 2005 |
| Eigen Artemis | Manual rotation | Articulated arm | Transrectal | 2008 |
| Koelis Urostation | Automatic rotation | Image-based | Transrectal | 2010 |
| Pi Medical BiopSee | Biplane probe on stepper | Stepper with encoders | Transperineal | N/A |
| Esaote Virtual Navigator | Manual sweep/rotation | Electromagnetic | Transrectal | 2014 |
| BK Ultrasound BioJet Fusion | Biplane probe on stepper | Stepper with encoders | Transrectal or transperineal | 2012 |
| Hitachi/Real-Time Virtual Sonography | Real-time biplanar | Electromagnetic | Transrectal or transperineal | 2010 |
| MIM Software Symphony Bx | Biplane probe on stepper | Stepper with encoders | Transperineal | 2014 |
| Focal Healthcare Fusion Bx | Manual rotation | Articulated arm | Transrectal | 2016 |
| UC-Care Navigo | Manual sweep | Electromagnetic | Transrectal | 2016 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lang, J.; McClure, T.D.; Margolis, D.J.A. MRI–Ultrasound Fused Approach for Prostate Biopsy—How It Is Performed. Cancers 2024, 16, 1424. https://doi.org/10.3390/cancers16071424
Lang J, McClure TD, Margolis DJA. MRI–Ultrasound Fused Approach for Prostate Biopsy—How It Is Performed. Cancers. 2024; 16(7):1424. https://doi.org/10.3390/cancers16071424
Chicago/Turabian StyleLang, Jacob, Timothy Dale McClure, and Daniel J. A. Margolis. 2024. "MRI–Ultrasound Fused Approach for Prostate Biopsy—How It Is Performed" Cancers 16, no. 7: 1424. https://doi.org/10.3390/cancers16071424
APA StyleLang, J., McClure, T. D., & Margolis, D. J. A. (2024). MRI–Ultrasound Fused Approach for Prostate Biopsy—How It Is Performed. Cancers, 16(7), 1424. https://doi.org/10.3390/cancers16071424