

Spinal Meningiomas: A Comprehensive Review and Update on Advancements in Molecular Characterization, Diagnostics, Surgical Approach and Technology, and Alternative Therapies
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
3. Epidemiology and Clinical Presentation
4. Neuroimaging
5. Origin, Histopathology, and Grading
6. Molecular Genetics
7. Surgical Resection
7.1. Surgical Principles
7.2. Challenging Cases
7.3. Complications and Clinical Outcomes
8. Illustrative Clinical Case Studies
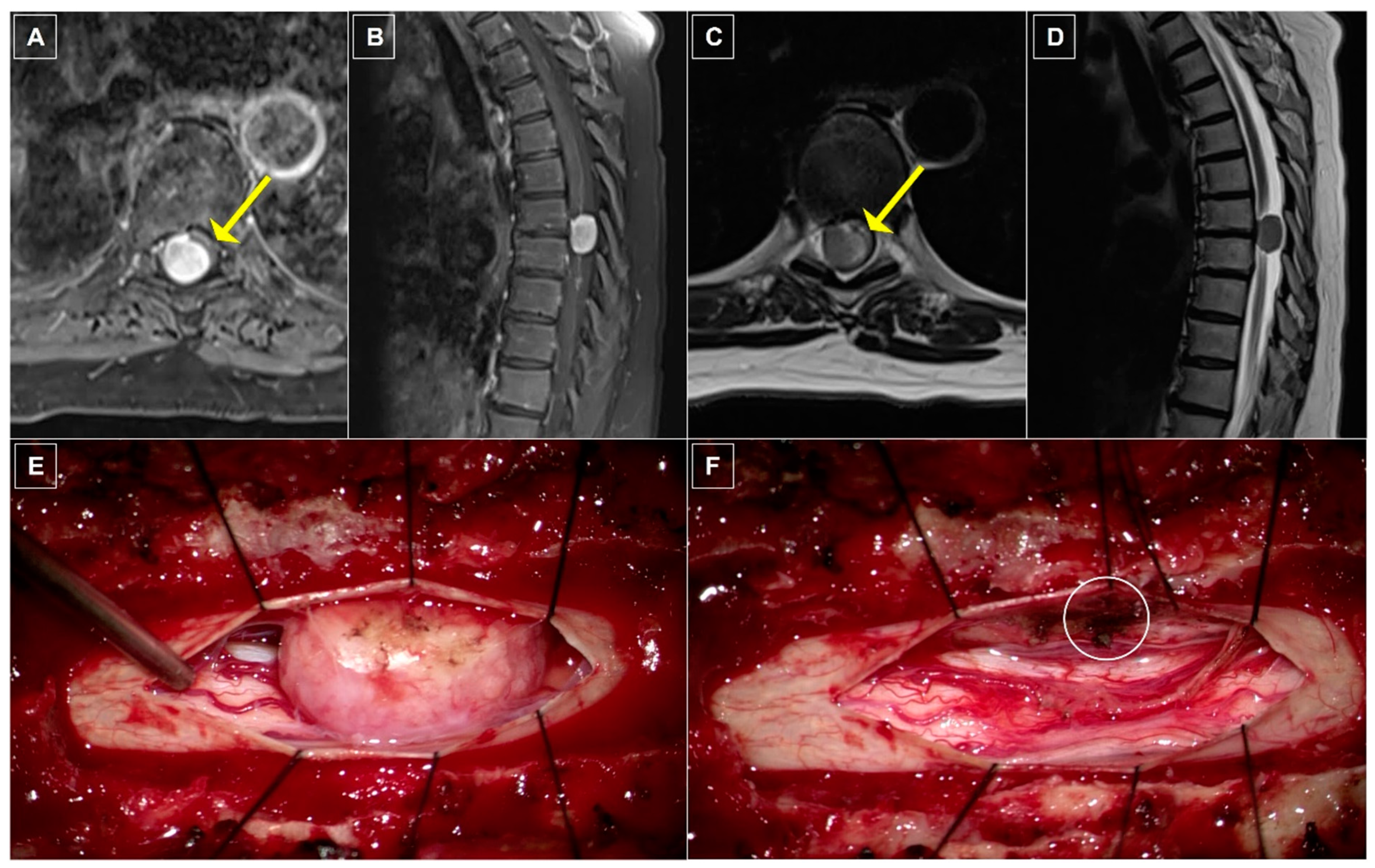
8.1. Case One: Dorsolateral Thoracic Meningioma
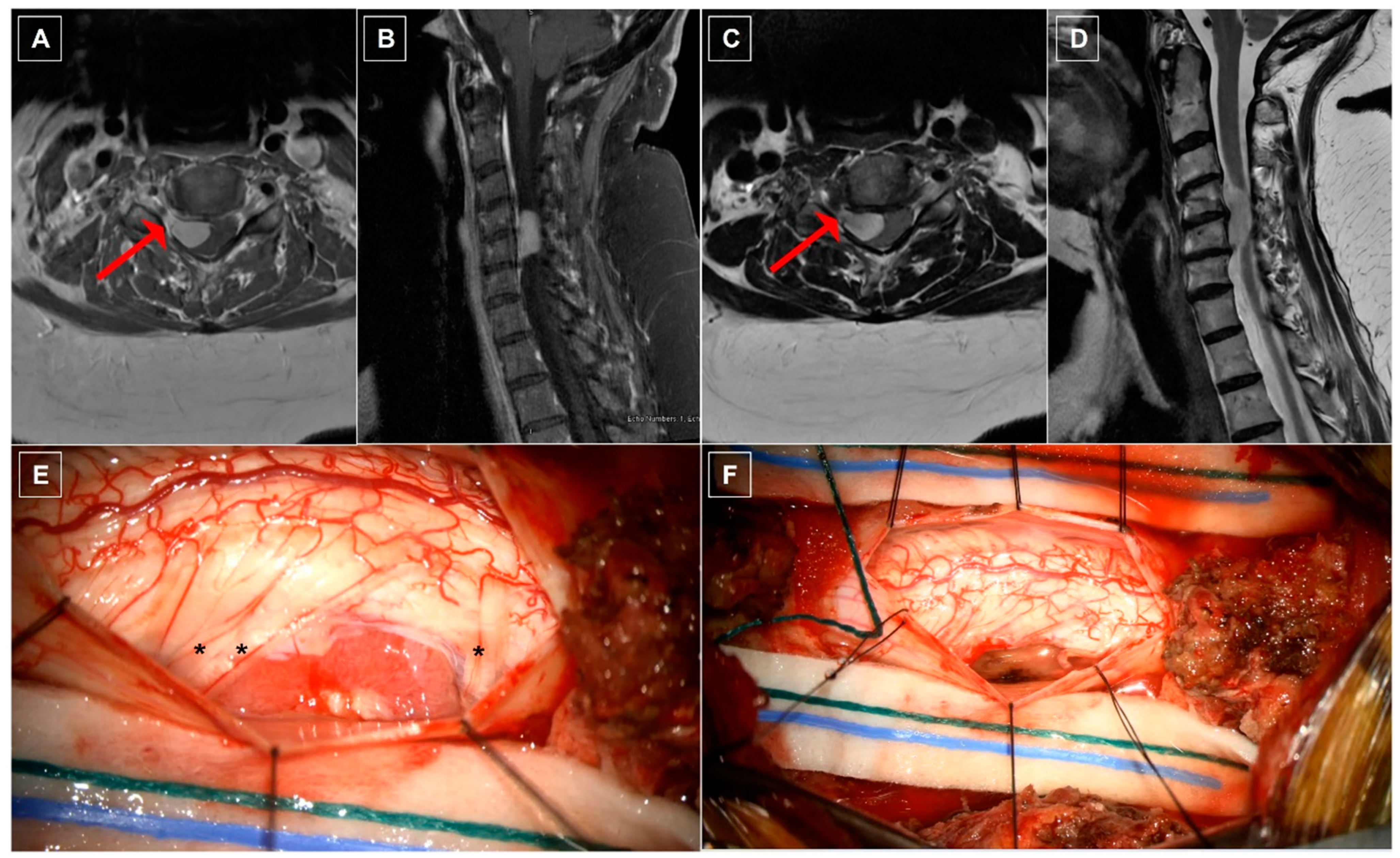
8.2. Case Two: Ventrolateral Cervical Meningioma
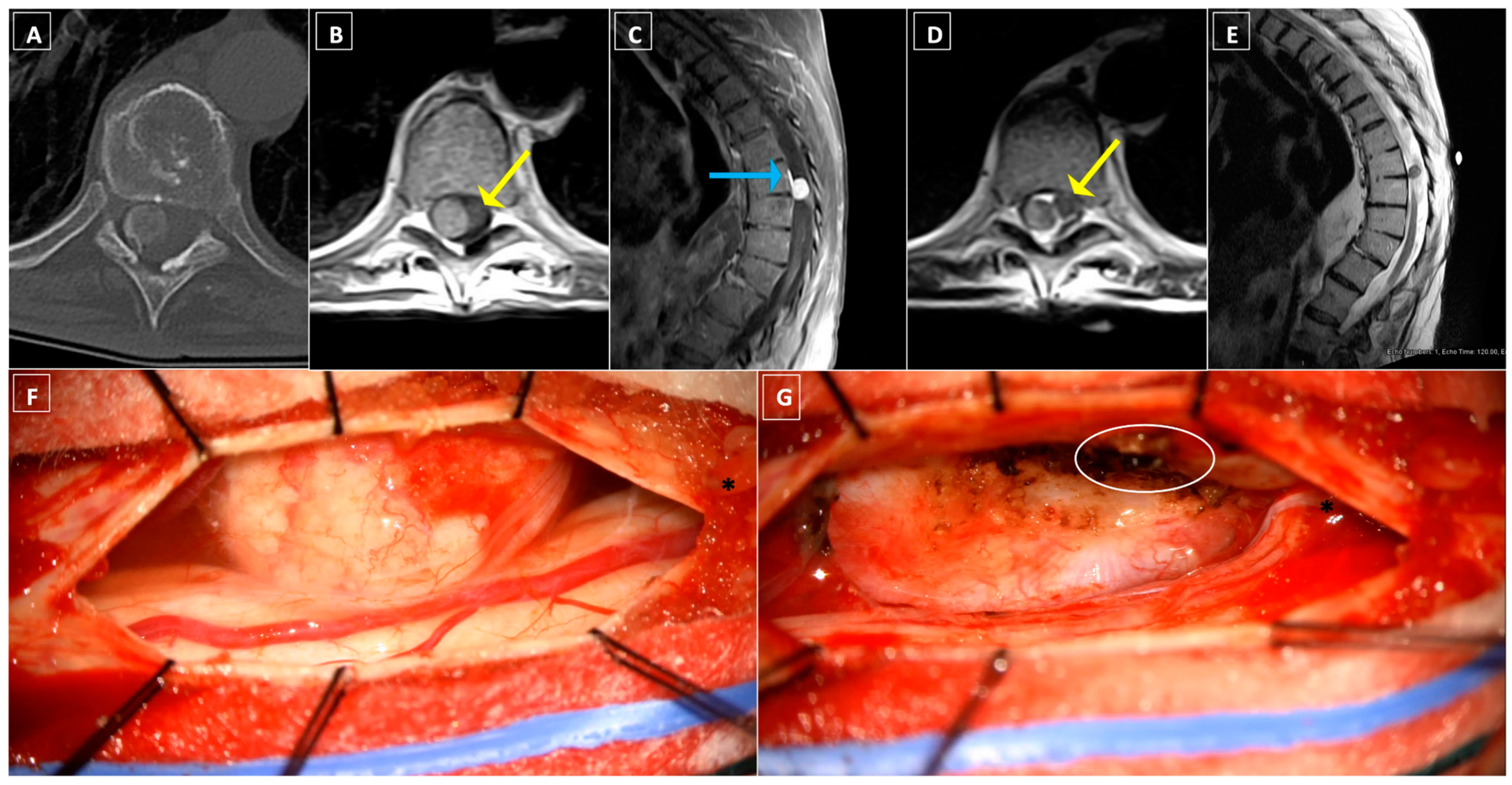
8.3. Case Three: Lateral Thoracic Meningioma
9. Adjuvant Therapies
9.1. Radiotherapy
9.2. Alternative Systemic Therapies
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duong, L.M.; McCarthy, B.J.; McLendon, R.E.; Dolecek, T.A.; Kruchko, C.; Douglas, L.L.; Ajani, U.A. Descriptive Epidemiology of Malignant and Nonmalignant Primary Spinal Cord, Spinal Meninges, and Cauda Equina Tumors, United States, 2004–2007. Cancer 2012, 118, 4220–4227. [Google Scholar] [CrossRef]
- Sandalcioglu, I.E.; Hunold, A.; Müller, O.; Bassiouni, H.; Stolke, D.; Asgari, S. Spinal Meningiomas: Critical Review of 131 Surgically Treated Patients. Eur. Spine J. 2008, 17, 1035–1041. [Google Scholar] [CrossRef]
- Solero, C.L.; Fornari, M.; Giombini, S.; Lasio, G.; Oliveri, G.; Cimino, C.; Pluchino, F. Spinal Meningiomas: Review of 174 Operated Cases. Neurosurgery 1989, 25, 153–160. [Google Scholar] [CrossRef]
- Sayagués, J.M.; Tabernero, M.D.; Maíllo, A.; Trelles, O.; Espinosa, A.B.; Sarasquete, M.E.; Merino, M.; Rasillo, A.; Vera, J.F.; Santos-Briz, A.; et al. Microarray-Based Analysis of Spinal versus Intracranial Meningiomas: Different Clinical, Biological, and Genetic Characteristics Associated with Distinct Patterns of Gene Expression. J. Neuropathol. Exp. Neurol. 2006, 65, 445–454. [Google Scholar] [CrossRef]
- Foda, A.A.M.; Rafi, S.; Ikram, N.; Alam, M.S.; Ayesha, S. Spinal Versus Intracranial Meningioma: Aberrant Expression of CD10 and Inhibin with Relation to Clinicopathological Features and Prognosis. Pathol. Oncol. Res. POR 2020, 26, 1313–1318. [Google Scholar] [CrossRef]
- Foda, A.A.M.; Alam, M.S.; Ikram, N.; Rafi, S.; Elnaghi, K. Spinal versus Intracranial Meningioma: Expression of E-Cadherin and Fascin with Relation to Clinicopathological Features. Cancer Biomark. Sect. Dis. Markers 2019, 25, 333–339. [Google Scholar] [CrossRef]
- Schaller, B. Spinal Meningioma: Relationship between Histological Subtypes and Surgical Outcome? J. Neurooncol. 2005, 75, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Setzer, M.; Vatter, H.; Marquardt, G.; Seifert, V.; Vrionis, F.D. Management of Spinal Meningiomas: Surgical Results and a Review of the Literature. Neurosurg. Focus 2007, 23, E14. [Google Scholar] [CrossRef]
- Barber, S.M.; Konakondla, S.; Nakhla, J.; Fridley, J.S.; Xia, J.; Oyelese, A.A.; Telfeian, A.E.; Gokaslan, Z.L. Oncologic Benefits of Dural Resection in Spinal Meningiomas: A Meta-Analysis of Simpson Grades and Recurrence Rates. J. Neurosurg. Spine 2019, 32, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Price, M.; Neff, C.; Cioffi, G.; Waite, K.A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2015–2019. Neuro-Oncology 2022, 24 (Suppl. S5), v1–v95. [Google Scholar] [CrossRef] [PubMed]
- Sadrameli, S.S.; Chan, T.M.; Lee, J.J.; Desai, V.R.; Holman, P.J. Resection of Spinal Meningioma Using Ultrasonic BoneScalpel Microshaver: Cases, Technique, and Review of the Literature. Oper. Neurosurg. Hagerstown Md 2020, 19, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Tan, W.L.B.; Wei, W.; Vellayappan, B.A. An Overview of the Tumors Affecting the Spine-inside to Out. Neuro-Oncol. Pract. 2020, 7 (Suppl. S1), i10–i17. [Google Scholar] [CrossRef]
- Westwick, H.J.; Shamji, M.F. Effects of Sex on the Incidence and Prognosis of Spinal Meningiomas: A Surveillance, Epidemiology, and End Results Study. J. Neurosurg. Spine 2015, 23, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Weil, S.M.; Gewirtz, R.J.; Tew, J.M. Concurrent Intradural and Extradural Meningiomas of the Cervical Spine. Neurosurgery 1990, 27, 629–631. [Google Scholar] [CrossRef]
- El-Hajj, V.G.; Pettersson-Segerlind, J.; Fletcher-Sandersjöö, A.; Edström, E.; Elmi-Terander, A. Current Knowledge on Spinal Meningiomas Epidemiology, Tumor Characteristics and Non-Surgical Treatment Options: A Systematic Review and Pooled Analysis (Part 1). Cancers 2022, 14, 6251. [Google Scholar] [CrossRef] [PubMed]
- Kshettry, V.R.; Hsieh, J.K.; Ostrom, Q.T.; Kruchko, C.; Benzel, E.C.; Barnholtz-Sloan, J.S. Descriptive Epidemiology of Spinal Meningiomas in the United States. Spine 2015, 40, E886–E889. [Google Scholar] [CrossRef] [PubMed]
- Ogasawara, C.; Philbrick, B.D.; Adamson, D.C. Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future Directions. Biomedicines 2021, 9, 319. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Gadol, A.A.; Zikel, O.M.; Koch, C.A.; Scheithauer, B.W.; Krauss, W.E. Spinal Meningiomas in Patients Younger than 50 Years of Age: A 21-Year Experience. J. Neurosurg. 2003, 98 (Suppl. S3), 258–263. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.R. Neurofibromatosis Type 2 (NF2): A Clinical and Molecular Review. Orphanet J. Rare Dis. 2009, 4, 16. [Google Scholar] [CrossRef]
- Agopiantz, M.; Carnot, M.; Denis, C.; Martin, E.; Gauchotte, G. Hormone Receptor Expression in Meningiomas: A Systematic Review. Cancers 2023, 15, 980. [Google Scholar] [CrossRef]
- Yang, X.; Liu, F.; Zheng, J.; Cheng, W.; Zhao, C.; Di, J. Relationship Between Oral Contraceptives and the Risk of Gliomas and Meningiomas: A Dose-Response Meta-Analysis and Systematic Review. World Neurosurg. 2021, 147, e148–e162. [Google Scholar] [CrossRef] [PubMed]
- Roehrkasse, A.M.; Peterson, J.E.G.; Fung, K.-M.; Pelargos, P.E.; Dunn, I.F. The Discrepancy Between Standard Histologic WHO Grading of Meningioma and Molecular Profile: A Single Institution Series. Front. Oncol. 2022, 12, 846232. [Google Scholar] [CrossRef] [PubMed]
- Cioffi, F.; Buric, J.; Carnesecchi, S.; Romoli, S.; Conti, P. Spinal Meningiomas in Pregnancy: Report of Two Cases and Review of the Literature. Eur. J. Gynaecol. Oncol. 1996, 17, 384–388. [Google Scholar]
- Maiuri, F.; De Caro, M.L.D.B.; de Divitiis, O.; Vergara, P.; Mariniello, G. Spinal Meningiomas: Age-Related Features. Clin. Neurol. Neurosurg. 2011, 113, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Menezes, A.H.; Shimizu, K.; Woodroffe, R.W.; Helland, L.C.; Hitchon, P.W.; Howard, M.A. Differences and Characteristics of Symptoms by Tumor Location, Size, and Degree of Spinal Cord Compression: A Retrospective Study on 53 Surgically Treated, Symptomatic Spinal Meningiomas. J. Neurosurg. Spine 2020, 32, 931–940. [Google Scholar] [CrossRef] [PubMed]
- Jamilson Araújo Pereira, B.; Nogueira de Almeida, A.; Silva Paiva, W.; Henrique Pires de Aguiar, P.; Jacobsen Teixeira, M.; Kazue Nagahashi Marie, S. Neuro-Oncological Features of Spinal Meningiomas: Systematic Review. Neurochirurgie 2020, 66, 41–44. [Google Scholar] [CrossRef]
- Klekamp, J.; Samii, M. Surgical Results for Spinal Meningiomas. Surg. Neurol. 1999, 52, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Gezen, F.; Kahraman, S.; Canakci, Z.; Bedük, A. Review of 36 Cases of Spinal Cord Meningioma. Spine 2000, 25, 727–731. [Google Scholar] [CrossRef]
- King, A.T.; Sharr, M.M.; Gullan, R.W.; Bartlett, J.R. Spinal Meningiomas: A 20-Year Review. Br. J. Neurosurg. 1998, 12, 521–526. [Google Scholar] [CrossRef]
- Levy, W.J.; Bay, J.; Dohn, D. Spinal Cord Meningioma. J. Neurosurg. 1982, 57, 804–812. [Google Scholar] [CrossRef]
- Morandi, X.; Haegelen, C.; Riffaud, L.; Amlashi, S.; Adn, M.; Brassier, G. Results in the Operative Treatment of Elderly Patients with Spinal Meningiomas. Spine 2004, 29, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Postalci, L.; Tugcu, B.; Gungor, A.; Guclu, G. Spinal Meningiomas: Recurrence in Ventrally Located Individuals on Long-Term Follow-up; a Review of 46 Operated Cases. Turk. Neurosurg. 2011, 21, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Onken, J.; Obermüller, K.; Staub-Bartelt, F.; Meyer, B.; Vajkoczy, P.; Wostrack, M. Surgical Management of Spinal Meningiomas: Focus on Unilateral Posterior Approach and Anterior Localization. J. Neurosurg. Spine 2018, 30, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Schwake, M.; Adeli, A.; Sporns, P.; Ewelt, C.; Schmitz, T.; Sicking, J.; Hess, K.; Cäcilia Spille, D.; Paulus, W.; Stummer, W.; et al. Spinal Meningiomas—Risks and Potential of an Increasing Age at the Time of Surgery. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2018, 57, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Roux, F.X.; Nataf, F.; Pinaudeau, M.; Borne, G.; Devaux, B.; Meder, J.F. Intraspinal Meningiomas: Review of 54 Cases with Discussion of Poor Prognosis Factors and Modern Therapeutic Management. Surg. Neurol. 1996, 46, 458–463, discussion 463–464. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.C.; Choi, G.; Lee, S.-H.; Han, H.; Lee, J.Y.; Jeon, Y.H.; Park, H.S.; Park, J.Y.; Paeng, S.S. Radiological Findings of Spinal Schwannomas and Meningiomas: Focus on Discrimination of Two Disease Entities. Eur. Radiol. 2009, 19, 2707–2715. [Google Scholar] [CrossRef]
- McCormick, J.D.; Werner, B.C.; Shimer, A.L. Patient-Reported Outcome Measures in Spine Surgery. J. Am. Acad. Orthop. Surg. 2013, 21, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Frankel, H.L.; Hancock, D.O.; Hyslop, G.; Melzak, J.; Michaelis, L.S.; Ungar, G.H.; Vernon, J.D.; Walsh, J.J. The Value of Postural Reduction in the Initial Management of Closed Injuries of the Spine with Paraplegia and Tetraplegia. I. Paraplegia 1969, 7, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, D.; Kalasauskas, D.; Othman, A.; Brockmann, M.A.; Sommer, C.J.; Ringel, F.; Keric, N. Predictors of Neurological Worsening after Resection of Spinal Meningiomas. Cancers 2023, 15, 5408. [Google Scholar] [CrossRef]
- Yeo, Y.; Park, C.; Lee, J.W.; Kang, Y.; Ahn, J.M.; Kang, H.S.; Lee, E. Magnetic Resonance Imaging Spectrum of Spinal Meningioma. Clin. Imaging 2019, 55, 100–106. [Google Scholar] [CrossRef]
- Aoyama, T.; Ogiwara, T.; Ito, K.; Miyaoka, Y.; Fujii, Y.; Hanaoka, Y.; Hasegawa, T.; Watanabe, G.; Seguchi, T.; Hongo, K. Correlations Among Consistency, Computed Tomography Values, and Histopathological Subtypes of Spinal Meningioma. Acta Med. Okayama 2021, 75, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Ando, K.; Matsumoto, T.; Sato, K.; Kato, F.; Kanemura, T.; Yoshihara, H.; Sakai, Y.; Hirasawa, A.; Nakashima, H.; et al. Clinical Features and Prognostic Factors in Spinal Meningioma Surgery from a Multicenter Study. Sci. Rep. 2021, 11, 11630. [Google Scholar] [CrossRef] [PubMed]
- Watts, J.; Box, G.; Galvin, A.; Brotchie, P.; Trost, N.; Sutherland, T. Magnetic Resonance Imaging of Meningiomas: A Pictorial Review. Insights Imaging 2014, 5, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Ono, H.; Kumagai, G.; Wada, K.; Ono, A.; Asari, T.; Aoki, M.; Ishibashi, Y. Assessing the Utility of 18F-Fluorodeoxyglucose Positron Emission Tomography in the Differential Diagnosis Between Spinal Schwannomas and Meningiomas. Cureus 2021, 13, e18890. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, H.S.; Yoon, Y.C.; Cha, M.J.; Lee, S.-H.; Kim, E.-S. Differentiating between Spinal Schwannomas and Meningiomas Using MRI: A Focus on Cystic Change. PLoS ONE 2020, 15, e0233623. [Google Scholar] [CrossRef] [PubMed]
- De Verdelhan, O.; Haegelen, C.; Carsin-Nicol, B.; Riffaud, L.; Amlashi, S.F.A.; Brassier, G.; Carsin, M.; Morandi, X. MR Imaging Features of Spinal Schwannomas and Meningiomas. J. Neuroradiol. J. Neuroradiol. 2005, 32, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Baro, V.; Moiraghi, A.; Carlucci, V.; Paun, L.; Anglani, M.; Ermani, M.; Saladino, A.; Chioffi, F.; d’Avella, D.; Landi, A.; et al. Spinal Meningiomas: Influence of Cord Compression and Radiological Features on Preoperative Functional Status and Outcome. Cancers 2021, 13, 4183. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lee, I.S.; Choi, K.-U.; Lee, Y.H.; Yi, J.H.; Song, J.W.; Suh, K.J.; Kim, H.J. CT and MRI Findings of Calcified Spinal Meningiomas: Correlation with Pathological Findings. Skelet. Radiol. 2010, 39, 345–352. [Google Scholar] [CrossRef]
- Umana, G.E.; Scalia, G.; Vats, A.; Pompili, G.; Barone, F.; Passanisi, M.; Graziano, F.; Maugeri, R.; Tranchina, M.G.; Cosentino, S.; et al. Primary Extracranial Meningiomas of the Head and Neck. Life 2021, 11, 942. [Google Scholar] [CrossRef]
- Kim, H.; Jung, T.-Y.; Kim, I.-Y.; Lee, J.-K. Two Cases of Primary Osteolytic Intraosseous Meningioma of the Skull Metastasizing to Whole Skull and the Spine. J. Korean Neurosurg. Soc. 2012, 51, 151–154. [Google Scholar] [CrossRef]
- Kwon, S.M.; Ko, Y.; Bang, S.S. Primary Intraosseous Osteolytic Meningioma: A Case Report and Review of the Literature. BMC Neurol. 2019, 19, 176. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Ferini, G.; Haque, M.; Umana, G.E.; Scalia, G.; Chaurasia, B.; Vats, A.; Rahman, A. Primary Intraosseous Osteolytic Meningioma with Aggressive Clinical Behaviour: Clinico-Pathologic Correlation and Proposed New Clinical Classification. Life 2022, 12, 548. [Google Scholar] [CrossRef] [PubMed]
- Apostolov, G.; Kehayov, I.; Kitov, B. Clinical Aspects of Spinal Meningiomas: A Review. Folia Medica 2021, 63, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-Q.; Zeng, X.-W.; Zhang, B.-Y.; Dou, Y.-F.; Wu, J.-S.; Jiang, C.-C.; Zhong, P.; Chen, H. Spinal Meningioma in Childhood: Clinical Features and Treatment. Childs Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2012, 28, 129–136. [Google Scholar] [CrossRef]
- Fanous, A.A.; Lipinski, L.J.; Krishna, C.; Roger, E.P.; Siddiqui, A.H.; Levy, E.I.; Leonardo, J.; Pollina, J. The Impact of Preoperative Angiographic Identification of the Artery of Adamkiewicz on Surgical Decision Making in Patients Undergoing Thoracolumbar Corpectomy. Spine 2015, 40, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- A Galgano, M. Spinal Meningiomas: A Review. J. Spine 2013, 3. [Google Scholar] [CrossRef]
- Batista, S.; Andreão, F.F.; Palavani, L.B.; Borges, P.; Verly, G.; Bertani, R.; Filho, J.A.A.; Paiva, W.S.; de Abreu, L.V.; Pessoa, B.L. Enhancing Meningioma Resection: A Comprehensive Study on the Safety and Effectiveness of OnyxTM Presurgical Embolization. Neurosurg. Rev. 2023, 46, 299. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours Editorial Board. Central Nervous System Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021; Volume 6. [Google Scholar]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Cao, Y.; Jiang, Y.; Liu, C.; Jin, R.; Jin, Z.; Hong, X.; Zhao, L.; Zhao, G.; Wang, Y. Epidemiology and Survival of Patients with Spinal Meningiomas: A SEER Analysis. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2021, 47, 2340–2345. [Google Scholar] [CrossRef]
- Perry, A.; Stafford, S.L.; Scheithauer, B.W.; Suman, V.J.; Lohse, C.M. Meningioma Grading: An Analysis of Histologic Parameters. Am. J. Surg. Pathol. 1997, 21, 1455–1465. [Google Scholar] [CrossRef]
- Delgado-López, P.D.; Cubo-Delgado, E.; González-Bernal, J.J.; Martín-Alonso, J. A Practical Overview on the Molecular Biology of Meningioma. Curr. Neurol. Neurosci. Rep. 2020, 20, 62. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Zhang, L.; Jia, W.; Yang, J. Clinical Features and Surgical Outcomes of High-Grade Spinal Meningiomas: Report of 19 Cases and Literature Review. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2020, 72, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Yang, T.; Deng, X.; Yang, C.; Zhao, L.; Yao, N.; Fang, J.; Wang, G.; Yang, J.; Xu, Y. Spinal Extradural En Plaque Meningiomas: Clinical Features and Long-Term Outcomes of 12 Cases. J. Neurosurg. Spine 2014, 21, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Hua, L.; Zhu, H.; Deng, J.; Tian, M.; Jiang, X.; Tang, H.; Luan, S.; Wakimoto, H.; Xie, Q.; Gong, Y. Clinical and Prognostic Features of Spinal Meningioma: A Thorough Analysis from a Single Neurosurgical Center. J. Neurooncol. 2018, 140, 639–647. [Google Scholar] [CrossRef]
- Adelhoefer, S.J.; Feghali, J.; Rajan, S.; Eberhart, C.G.; Staedtke, V.; Cohen, A.R. An Unusual Finding of an Anaplastic Meningioma in NF2-Related Schwannomatosis. Childs Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2024. [Google Scholar] [CrossRef] [PubMed]
- Morita, S.; Horiba, A.; Masui, K.; Yamaguchi, K.; Asamoto, S.; Hayashi, M.; Komori, T.; Kawamata, T. A Difficult-to-Diagnose Anaplastic Meningioma with Spinal Cord Dissemination and Cytokeratin Positivity. Pathol. Int. 2023, 73, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Al-Habib, A.; Lach, B.; Al Khani, A. Intracerebral Rhabdoid and Papillary Meningioma with Leptomeningeal Spread and Rapid Clinical Progression. Clin. Neuropathol. 2005, 24, 1. [Google Scholar]
- Driver, J.; Hoffman, S.E.; Tavakol, S.; Woodward, E.; Maury, E.A.; Bhave, V.; Greenwald, N.F.; Nassiri, F.; Aldape, K.; Zadeh, G.; et al. A Molecularly Integrated Grade for Meningioma. Neuro-Oncology 2022, 24, 796–808. [Google Scholar] [CrossRef] [PubMed]
- Sahm, M.; Perry, A.; von Deimling, A.; Claus, E.B.; Mawrin, C.; Brastianos, P.K.; Santagata, S. Chapter 7: Meningioma. In WHO Classification of Tumours Editorial Board. Central Nervous System Tumours; International Agency for Research on Cancer: Lyon, France, 2021; Volume 6. [Google Scholar]
- Sanson, M.; Marineau, C.; Desmaze, C.; Lutchman, M.; Ruttledge, M.; Baron, C.; Narod, S.; Delattre, O.; Lenoir, G.; Thomas, G. Germline Deletion in a Neurofibromatosis Type 2 Kindred Inactivates the NF2 Gene and a Candidate Meningioma Locus. Hum. Mol. Genet. 1993, 2, 1215–1220. [Google Scholar] [CrossRef]
- Ruttledge, M.H.; Sarrazin, J.; Rangaratnam, S.; Phelan, C.M.; Twist, E.; Merel, P.; Delattre, O.; Thomas, G.; Nordenskjöld, M.; Collins, V.P. Evidence for the Complete Inactivation of the NF2 Gene in the Majority of Sporadic Meningiomas. Nat. Genet. 1994, 6, 180–184. [Google Scholar] [CrossRef]
- Clark, V.E.; Harmancı, A.S.; Bai, H.; Youngblood, M.W.; Lee, T.I.; Baranoski, J.F.; Ercan-Sencicek, A.G.; Abraham, B.J.; Weintraub, A.S.; Hnisz, D.; et al. Recurrent Somatic Mutations in POLR2A Define a Distinct Subset of Meningiomas. Nat. Genet. 2016, 48, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Pereira, B.J.A.; Oba-Shinjo, S.M.; de Almeida, A.N.; Marie, S.K.N. Molecular Alterations in Meningiomas: Literature Review. Clin. Neurol. Neurosurg. 2019, 176, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Brastianos, P.K.; Horowitz, P.M.; Santagata, S.; Jones, R.T.; McKenna, A.; Getz, G.; Ligon, K.L.; Palescandolo, E.; Van Hummelen, P.; Ducar, M.D.; et al. Genomic Sequencing of Meningiomas Identifies Oncogenic SMO and AKT1 Mutations. Nat. Genet. 2013, 45, 285–289. [Google Scholar] [CrossRef]
- Linsler, S.; Kraemer, D.; Driess, C.; Oertel, J.; Kammers, K.; Rahnenführer, J.; Ketter, R.; Urbschat, S. Molecular Biological Determinations of Meningioma Progression and Recurrence. PLoS ONE 2014, 9, e94987. [Google Scholar] [CrossRef]
- Yoon, S.H.; Chung, C.K.; Jahng, T.A. Surgical Outcome of Spinal Canal Meningiomas. J. Korean Neurosurg. Soc. 2007, 42, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Hohenberger, C.; Gugg, C.; Schmidt, N.O.; Zeman, F.; Schebesch, K.-M. Functional Outcome after Surgical Treatment of Spinal Meningioma. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2020, 77, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Ampie, L.; Snyder, M.H.; Dominguez, J.F.; Buchholz, A.; Yen, C.-P.; Shaffrey, M.E.; Syed, H.R.; Shaffrey, C.I.; Smith, J.S. Clinical Characteristics and Long-Term Outcomes for Patients Who Undergo Cytoreductive Surgery for Thoracic Meningiomas: A Retrospective Analysis. Neurosurg. Focus 2021, 50, E18. [Google Scholar] [CrossRef]
- Choudhury, A.; Magill, S.T.; Eaton, C.D.; Prager, B.C.; Chen, W.C.; Cady, M.A.; Seo, K.; Lucas, C.-H.G.; Casey-Clyde, T.J.; Vasudevan, H.N.; et al. Meningioma DNA Methylation Groups Identify Biological Drivers and Therapeutic Vulnerabilities. Nat. Genet. 2022, 54, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Nassiri, F.; Liu, J.; Patil, V.; Mamatjan, Y.; Wang, J.Z.; Hugh-White, R.; Macklin, A.M.; Khan, S.; Singh, O.; Karimi, S.; et al. A Clinically Applicable Integrative Molecular Classification of Meningiomas. Nature 2021, 597, 119–125. [Google Scholar] [CrossRef]
- Darshan, H.R.; Patel, B.K.; Singh, A.; Nair, P.; Poyuran, R.; Easwer, H.V. Simultaneous Trigonal and Spinal Meningioma with Varied Histology: A Rare Case Report. Surg. Neurol. Int. 2021, 12, 611. [Google Scholar] [CrossRef]
- St Pierre, R.; Collings, C.K.; Samé Guerra, D.D.; Widmer, C.J.; Bolonduro, O.; Mashtalir, N.; Sankar, A.; Liang, Y.; Bi, W.L.; Gerkes, E.H.; et al. SMARCE1 Deficiency Generates a Targetable mSWI/SNF Dependency in Clear Cell Meningioma. Nat. Genet. 2022, 54, 861–873. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.J.; O’Sullivan, J.; Bhaskar, S.S.; Hadfield, K.D.; Poke, G.; Caird, J.; Sharif, S.; Eccles, D.; Fitzpatrick, D.; Rawluk, D.; et al. Loss-of-Function Mutations in SMARCE1 Cause an Inherited Disorder of Multiple Spinal Meningiomas. Nat. Genet. 2013, 45, 295–298. [Google Scholar] [CrossRef]
- Arslantas, A.; Artan, S.; Oner, U.; Durmaz, R.; Müslümanoglu, H.; Atasoy, M.A.; Başaran, N.; Tel, E. Detection of Chromosomal Imbalances in Spinal Meningiomas by Comparative Genomic Hybridization. Neurol. Med. Chir. 2003, 43, 12–18, discussion 19. [Google Scholar] [CrossRef] [PubMed]
- Barresi, V.; Vitarelli, E.; Tuccari, G.; Barresi, G. MMP-9 Expression in Meningiomas: A Prognostic Marker for Recurrence Risk? J. Neurooncol. 2011, 102, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Azad, T.D.; Jiang, B.; Bettegowda, C. Molecular Foundations of Primary Spinal Tumors-Implications for Surgical Management. Ann. Transl. Med. 2019, 7, 222. [Google Scholar] [CrossRef] [PubMed]
- Ketter, R.; Rahnenführer, J.; Henn, W.; Kim, Y.-J.; Feiden, W.; Steudel, W.-I.; Zang, K.D.; Urbschat, S. Correspondence of Tumor Localization with Tumor Recurrence and Cytogenetic Progression in Meningiomas. Neurosurgery 2008, 62, 61–69, discussion 69–70. [Google Scholar] [CrossRef] [PubMed]
- El-Hajj, V.G.; Pettersson-Segerlind, J.; Fletcher-Sandersjöö, A.; Edström, E.; Elmi-Terander, A. Current Knowledge on Spinal Meningiomas-Surgical Treatment, Complications, and Outcomes: A Systematic Review and Meta-Analysis (Part 2). Cancers 2022, 14, 6221. [Google Scholar] [CrossRef]
- Roth, P.; Happold, C.; Weller, M. Corticosteroid Use in Neuro-Oncology: An Update. Neuro-Oncol. Pract. 2015, 2, 6–12. [Google Scholar] [CrossRef]
- Basques, B.A.; Golinvaux, N.S.; Bohl, D.D.; Yacob, A.; Toy, J.O.; Varthi, A.G.; Grauer, J.N. Use of an Operating Microscope during Spine Surgery Is Associated with Minor Increases in Operating Room Times and No Increased Risk of Infection. Spine 2014, 39, 1910–1916. [Google Scholar] [CrossRef]
- de Divitiis, O.; D’avella, E.; Sacco, M.; Somma, T.; Turgut, M.; Baro, V.; Denaro, L. The Role of Vitom-3D in the Management of Spinal Meningiomas: Review of the Literature and Illustrative Case. Mini-Invasive Surg. 2020, 4, 75. [Google Scholar] [CrossRef]
- Montemurro, N.; Scerrati, A.; Ricciardi, L.; Trevisi, G. The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery. J. Clin. Med. 2021, 11, 223. [Google Scholar] [CrossRef] [PubMed]
- Prada, F.; Vetrano, I.G.; Filippini, A.; Del Bene, M.; Perin, A.; Casali, C.; Legnani, F.; Saini, M.; DiMeco, F. Intraoperative Ultrasound in Spinal Tumor Surgery. J. Ultrasound 2014, 17, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Henzi, S.; Krayenbühl, N.; Bozinov, O.; Regli, L.; Stienen, M.N. Ultrasonic Aspiration in Neurosurgery: Comparative Analysis of Complications and Outcome for Three Commonly Used Models. Acta Neurochir. 2019, 161, 2073–2082. [Google Scholar] [CrossRef] [PubMed]
- Tuncer, C.; Polat, Ö.; Duru, S. The Use of Tissue-Selective Ultrasonic Aspirators in the Surgical Treatment of Brain and Spinal Cord Tumors. Duzce Med. J. 2019, 21, 94–97. [Google Scholar] [CrossRef]
- Fraioli, M.F.; Marciani, M.G.; Umana, G.E.; Fraioli, B. Anterior Microsurgical Approach to Ventral Lower Cervical Spine Meningiomas: Indications, Surgical Technique and Long Term Outcome. Technol. Cancer Res. Treat. 2015, 14, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Scibilia, A.; Terranova, C.; Rizzo, V.; Raffa, G.; Morelli, A.; Esposito, F.; Mallamace, R.; Buda, G.; Conti, A.; Quartarone, A.; et al. Intraoperative Neurophysiological Mapping and Monitoring in Spinal Tumor Surgery: Sirens or Indispensable Tools? Neurosurg. Focus 2016, 41, E18. [Google Scholar] [CrossRef] [PubMed]
- Harel, R.; Schleifer, D.; Appel, S.; Attia, M.; Cohen, Z.R.; Knoller, N. Spinal Intradural Extramedullary Tumors: The Value of Intraoperative Neurophysiologic Monitoring on Surgical Outcome. Neurosurg. Rev. 2017, 40, 613–619. [Google Scholar] [CrossRef]
- Gottfried, O.N.; Gluf, W.; Quinones-Hinojosa, A.; Kan, P.; Schmidt, M.H. Spinal Meningiomas: Surgical Management and Outcome. Neurosurg. Focus 2003, 14, e2. [Google Scholar] [CrossRef] [PubMed]
- Black, P.M.; Villavicencio, A.T.; Rhouddou, C.; Loeffler, J.S. Aggressive Surgery and Focal Radiation in the Management of Meningiomas of the Skull Base: Preservation of Function with Maintenance of Local Control. Acta Neurochir. 2001, 143, 555–562. [Google Scholar] [CrossRef]
- Wiedemayer, H.; Sandalcioglu, I.E.; Aalders, M.; Wiedemayer, H.; Floerke, M.; Stolke, D. Reconstruction of the Laminar Roof with Miniplates for a Posterior Approach in Intraspinal Surgery: Technical Considerations and Critical Evaluation of Follow-up Results. Spine 2004, 29, E333–E342. [Google Scholar] [CrossRef]
- Tatter, C.; Fletcher-Sandersjöö, A.; Persson, O.; Burström, G.; Grane, P.; Edström, E.; Elmi-Terander, A. Incidence and Predictors of Kyphotic Deformity Following Resection of Cervical Intradural Tumors in Adults: A Population-Based Cohort Study. Acta Neurochir. 2020, 162, 2905–2913. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Garcés-Ambrossi, G.L.; Parker, S.L.; Sciubba, D.M.; Bydon, A.; Wolinksy, J.-P.; Gokaslan, Z.L.; Jallo, G.; Witham, T.F. Short-Term Progressive Spinal Deformity Following Laminoplasty versus Laminectomy for Resection of Intradural Spinal Tumors: Analysis of 238 Patients. Neurosurgery 2010, 66, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Boström, A.; Bürgel, U.; Reinacher, P.; Krings, T.; Rohde, V.; Gilsbach, J.M.; Hans, F.J. A Less Invasive Surgical Concept for the Resection of Spinal Meningiomas. Acta Neurochir. 2008, 150, 551–556, discussion 556. [Google Scholar] [CrossRef]
- Thakur, J.; Ulrich, C.T.; Schär, R.T.; Seidel, K.; Raabe, A.; Jesse, C.M. The Surgical Challenge of Ossified Ventrolateral Spinal Meningiomas: Tricks and Pearls for Managing Large Ossified Meningiomas of the Thoracic Spine. J. Neurosurg. Spine 2021, 35, 516–526. [Google Scholar] [CrossRef] [PubMed]
- Nzokou, A.; Weil, A.G.; Shedid, D. Minimally Invasive Removal of Thoracic and Lumbar Spinal Tumors Using a Nonexpandable Tubular Retractor. J. Neurosurg. Spine 2013, 19, 708–715. [Google Scholar] [CrossRef]
- Xu, J.; Yu, B.F.; Zheng, W.; Xiao, Y.H.; Lin, Y.; Tian, J.P. Microscopic keyhole technique for surgical resection of thoracic spinal meningioma via an oblique placing tube. Zhonghua Yi Xue Za Zhi 2019, 99, 983–987. [Google Scholar] [CrossRef] [PubMed]
- Iacoangeli, M.; Gladi, M.; Di Rienzo, A.; Dobran, M.; Alvaro, L.; Nocchi, N.; Maria, L.G.; Somma, D.; Colasanti, R.; Scerrati, M. Minimally Invasive Surgery for Benign Intradural Extramedullary Spinal Meningiomas: Experience of a Single Institution in a Cohort of Elderly Patients and Review of the Literature. Clin. Interv. Aging 2012, 7, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Saiwai, H.; Okada, S.; Hayashida, M.; Harimaya, K.; Matsumoto, Y.; Kawaguchi, K.-I.; Iida, K.-I.; Kobayakawa, K.; Yokota, K.; Maeda, T.; et al. Long-Term Outcomes of Spinal Meningioma Resection with Outer Layer of Dura Preservation Technique. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2021, 83, 68–70. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Arizono, T.; Maeda, T.; Terada, K.; Iwamoto, Y. A Novel Technique for Surgical Resection of Spinal Meningioma. Spine 2001, 26, 1805–1808. [Google Scholar] [CrossRef]
- Thavara, B.D.; Kidangan, G.S.; Rajagopalawarrier, B. Analysis of the Surgical Technique and Outcome of the Thoracic and Lumbar Intradural Spinal Tumor Excision Using Minimally Invasive Tubular Retractor System. Asian J. Neurosurg. 2019, 14, 453–460. [Google Scholar] [CrossRef]
- Dauleac, C.; Leroy, H.-A.; Karnoub, M.-A.; Obled, L.; Mertens, P.; Assaker, R. Minimally Invasive Surgery for Intradural Spinal Meningioma: A New Standard? A Comparative Study between Minimally Invasive and Open Approaches. Neurochirurgie 2022, 68, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Raygor, K.P.; Than, K.D.; Chou, D.; Mummaneni, P.V. Comparison of Minimally Invasive Transspinous and Open Approaches for Thoracolumbar Intradural-Extramedullary Spinal Tumors. Neurosurg. Focus 2015, 39, E12. [Google Scholar] [CrossRef] [PubMed]
- Helal, A.; Yolcu, Y.U.; Kamath, A.; Wahood, W.; Bydon, M. Minimally Invasive versus Open Surgery for Patients Undergoing Intradural Extramedullary Spinal Cord Tumor Resection: A Systematic Review and Meta-Analysis. Clin. Neurol. Neurosurg. 2022, 214, 107176. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, J.; Wang, L.; Lin, Y.; Yang, M.; Chen, X.; Teng, L.; Guo, H.; Chen, X. Surgical Resection of Dorsal Spinal Meningiomas with the Inner Dura Layer-An Improved Preservation Technique of Spinal Dura in 40 Cases. World Neurosurg. 2022, 160, e250–e255. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D. The Recurrence of Intracranial Meningiomas after Surgical Treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [PubMed]
- Naito, K.; Yamagata, T.; Arima, H.; Takami, T. Low Recurrence after Simpson Grade II Resection of Spinal Benign Meningiomas in a Single-Institute 10-Year Retrospective Study. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2020, 77, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Chung, C.K.; Lee, S.-H.; Jahng, T.-A.; Hyun, S.-J.; Kim, K.-J.; Yoon, S.H.; Kim, E.-S.; Eoh, W.; Kim, H.-J.; et al. Long-Term Recurrence Rates after the Removal of Spinal Meningiomas in Relation to Simpson Grades. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2016, 25, 4025–4032. [Google Scholar] [CrossRef] [PubMed]
- Ruggeri, A.G.; Fazzolari, B.; Colistra, D.; Cappelletti, M.; Marotta, N.; Delfini, R. Calcified Spinal Meningiomas. World Neurosurg. 2017, 102, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Engel, D.C.; Gawellek, L.; Peraio, S.; Stanojevic, M.; Tatagiba, M.; Ebner, F.H. Spinal Meningioma Surgery in the Elderly: Who Can Benefit from It? J. Neurosurg. Sci. 2021, 65, 408–413. [Google Scholar] [CrossRef]
- Viereck, M.J.; Ghobrial, G.M.; Beygi, S.; Harrop, J.S. Improved Patient Quality of Life Following Intradural Extramedullary Spinal Tumor Resection. J. Neurosurg. Spine 2016, 25, 640–645. [Google Scholar] [CrossRef]
- Noh, S.H.; Kim, K.H.; Shin, D.A.; Park, J.Y.; Yi, S.; Kuh, S.U.; Kim, K.N.; Chin, D.K.; Kim, K.S.; Yoon, D.H.; et al. Treatment Outcomes of 17 Patients with Atypical Spinal Meningioma, Including 4 with Metastases: A Retrospective Observational Study. Spine J. Off. J. N. Am. Spine Soc. 2019, 19, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Jia, Q.; Wu, Z.; Chu, R.; Zhao, C.; Wang, T.; Zhou, Z.; Cai, X.; Yang, X.; Xiao, J. Surgical Management of de Novo Metastatic Meningioma of the Spine: An Underestimated Issue for WHO Grade II/III Meningiomas. Clin. Neurol. Neurosurg. 2021, 210, 106995. [Google Scholar] [CrossRef]
- Westwick, H.J.; Yuh, S.-J.; Shamji, M.F. Complication Avoidance in the Resection of Spinal Meningiomas. World Neurosurg. 2015, 83, 627–634. [Google Scholar] [CrossRef]
- El-Hajj, V.G.; Pettersson Segerlind, J.; Burström, G.; Edström, E.; Elmi-Terander, A. Current Knowledge on Spinal Meningiomas: A Systematic Review Protocol. BMJ Open 2022, 12, e061614. [Google Scholar] [CrossRef] [PubMed]
- Yolcu, Y.U.; Goyal, A.; Alvi, M.A.; Moinuddin, F.M.; Bydon, M. Trends in the Utilization of Radiotherapy for Spinal Meningiomas: Insights from the 2004-2015 National Cancer Database. Neurosurg. Focus 2019, 46, E6. [Google Scholar] [CrossRef]
- Krauss, W.E.; Yolcu, Y.U.; Alvi, M.A.; Moinuddin, F.M.; Goyal, A.; Clarke, M.J.; Marsh, W.R.; Bydon, M. Clinical Characteristics and Management Differences for Grade II and III Spinal Meningiomas. J. Neurooncol. 2021, 153, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Hwang, L.; Okoye, C.C.; Patel, R.B.; Sahgal, A.; Foote, M.; Redmond, K.J.; Hofstetter, C.; Saigal, R.; Mossa-Basha, M.; Yuh, W.; et al. Stereotactic Body Radiotherapy for Benign Spinal Tumors: Meningiomas, Schwannomas, and Neurofibromas. J. Radiosurgery SBRT 2019, 6, 167–177. [Google Scholar]
- Epstein, N.E. Nursing Review of Spinal Meningiomas. Surg. Neurol. Int. 2018, 9, 41. [Google Scholar] [CrossRef]
- Lee, M.E.; Hwang, Y.J.; Sohn, M.J.; Lee, B.H.; Kim, S.Y. Assessment of the Treatment Response of Spinal Meningiomas after Radiosurgery Focusing on Serial MRI Findings. Jpn. J. Radiol. 2015, 33, 547–558. [Google Scholar] [CrossRef]
- Kufeld, M.; Wowra, B.; Muacevic, A.; Zausinger, S.; Tonn, J.-C. Radiosurgery of Spinal Meningiomas and Schwannomas. Technol. Cancer Res. Treat. 2012, 11, 27–34. [Google Scholar] [CrossRef]
- Chin, A.L.; Fujimoto, D.; Kumar, K.A.; Tupper, L.; Mansour, S.; Chang, S.D.; Adler, J.R.; Gibbs, I.C.; Hancock, S.L.; Dodd, R.; et al. Long-Term Update of Stereotactic Radiosurgery for Benign Spinal Tumors. Neurosurgery 2019, 85, 708–716. [Google Scholar] [CrossRef] [PubMed]
- Gerszten, P.C.; Burton, S.A.; Ozhasoglu, C.; McCue, K.J.; Quinn, A.E. Radiosurgery for Benign Intradural Spinal Tumors. Neurosurgery 2008, 62, 887–895, discussion 895–896. [Google Scholar] [CrossRef]
- Golanov, A.V.; Konovalov, N.A.; Antipina, N.A.; Vetlova, E.R.; Zolotova, S.V.; Galkin, M.V.; Arutyunov, N.V.; Chamorsov, A.Y.; Krasnyanskiy, S.A.; Nazarenko, A.G.; et al. Stereotactic Radiotherapy for Spinal Meningiomas and Neurinomas. Zh. Vopr. Neirokhir. Im. N. N. Burdenko 2015, 79, 4–13. [Google Scholar] [CrossRef] [PubMed]
- DiGiorgio, A.M.; Virk, M.S.; Mummaneni, P.V. Spinal Meningiomas. Handb. Clin. Neurol. 2020, 170, 251–256. [Google Scholar] [CrossRef]
- Sachdev, S.; Dodd, R.L.; Chang, S.D.; Soltys, S.G.; Adler, J.R.; Luxton, G.; Choi, C.Y.H.; Tupper, L.; Gibbs, I.C. Stereotactic Radiosurgery Yields Long-Term Control for Benign Intradural, Extramedullary Spinal Tumors. Neurosurgery 2011, 69, 533–539, discussion 539. [Google Scholar] [CrossRef]
- Gerszten, P.C.; Burton, S.A. Clinical Assessment of Stereotactic IGRT: Spinal Radiosurgery. Med. Dosim. Off. J. Am. Assoc. Med. Dosim. 2008, 33, 107–116. [Google Scholar] [CrossRef]
- Gerszten, P.C.; Quader, M.; Novotny, J.; Flickinger, J.C. Radiosurgery for Benign Tumors of the Spine: Clinical Experience and Current Trends. Technol. Cancer Res. Treat. 2012, 11, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, M.; De Martin, E.; Milanesi, I.; Fariselli, L. Intradural Extramedullary Benign Spinal Lesions Radiosurgery. Medium- to Long-Term Results from a Single Institution Experience. Acta Neurochir. 2013, 155, 1215–1222. [Google Scholar] [CrossRef]
- Gerszten, P.C.; Ozhasoglu, C.; Burton, S.A.; Kalnicki, S.; Welch, W.C. Feasibility of Frameless Single-Fraction Stereotactic Radiosurgery for Spinal Lesions. Neurosurg. Focus 2002, 13, e2. [Google Scholar] [CrossRef]
- Gerszten, P.C.; Ozhasoglu, C.; Burton, S.A.; Vogel, W.J.; Atkins, B.A.; Kalnicki, S.; Welch, W.C. CyberKnife Frameless Stereotactic Radiosurgery for Spinal Lesions: Clinical Experience in 125 Cases. Neurosurgery 2004, 55, 89–98, discussion 98–99. [Google Scholar] [CrossRef]
- Bhatnagar, A.K.; Gerszten, P.C.; Ozhasaglu, C.; Vogel, W.J.; Kalnicki, S.; Welch, W.C.; Burton, S.A. CyberKnife Frameless Radiosurgery for the Treatment of Extracranial Benign Tumors. Technol. Cancer Res. Treat. 2005, 4, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Zenonos, G.; Kondziolka, D.; Flickinger, J.C.; Gardner, P.; Lunsford, L.D. Gamma Knife Surgery in the Treatment Paradigm for Foramen Magnum Meningiomas. J. Neurosurg. 2012, 117, 864–873. [Google Scholar] [CrossRef]
- Weber, D.C.; Bizzocchi, N.; Bolsi, A.; Jenkinson, M.D. Proton Therapy for Intracranial Meningioma for the Treatment of Primary/Recurrent Disease Including Re-Irradiation. Front. Oncol. 2020, 10, 558845. [Google Scholar] [CrossRef] [PubMed]
- Cramer, P.; Thomale, U.-W.; Okuducu, A.F.; Lemke, A.J.; Stockhammer, F.; Woiciechowsky, C. An Atypical Spinal Meningioma with CSF Metastasis: Fatal Progression despite Aggressive Treatment. Case Report. J. Neurosurg. Spine 2005, 3, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Read, W.L.; Williams, F. Recurrent Meningioma of the Cervical Spine, Successfully Treated with Liposomal Doxorubicin. Case Rep. Oncol. 2017, 10, 656–659. [Google Scholar] [CrossRef] [PubMed]
- Kaley, T.J.; Wen, P.; Schiff, D.; Ligon, K.; Haidar, S.; Karimi, S.; Lassman, A.B.; Nolan, C.P.; DeAngelis, L.M.; Gavrilovic, I.; et al. Phase II Trial of Sunitinib for Recurrent and Progressive Atypical and Anaplastic Meningioma. Neuro-Oncology 2015, 17, 116–121. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dang, D.D.; Mugge, L.A.; Awan, O.K.; Gong, A.D.; Fanous, A.A. Spinal Meningiomas: A Comprehensive Review and Update on Advancements in Molecular Characterization, Diagnostics, Surgical Approach and Technology, and Alternative Therapies. Cancers 2024, 16, 1426. https://doi.org/10.3390/cancers16071426
Dang DD, Mugge LA, Awan OK, Gong AD, Fanous AA. Spinal Meningiomas: A Comprehensive Review and Update on Advancements in Molecular Characterization, Diagnostics, Surgical Approach and Technology, and Alternative Therapies. Cancers. 2024; 16(7):1426. https://doi.org/10.3390/cancers16071426
Chicago/Turabian StyleDang, Danielle D., Luke A. Mugge, Omar K. Awan, Andrew D. Gong, and Andrew A. Fanous. 2024. "Spinal Meningiomas: A Comprehensive Review and Update on Advancements in Molecular Characterization, Diagnostics, Surgical Approach and Technology, and Alternative Therapies" Cancers 16, no. 7: 1426. https://doi.org/10.3390/cancers16071426
APA StyleDang, D. D., Mugge, L. A., Awan, O. K., Gong, A. D., & Fanous, A. A. (2024). Spinal Meningiomas: A Comprehensive Review and Update on Advancements in Molecular Characterization, Diagnostics, Surgical Approach and Technology, and Alternative Therapies. Cancers, 16(7), 1426. https://doi.org/10.3390/cancers16071426