

Exploring The Prognostic Significance of SET-Domain Containing 2 (SETD2) Expression in Advanced and Castrate-Resistant Prostate Cancer

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methodology
2.1. Tissue Microarray Construction
2.2. Immunohistochemistry
2.3. Pathological Assessment
2.4. Bioinformatics and Public Database Analysis
2.5. SETD2 Gene Expression Analysis in TCGA PRAD Database
2.6. Statistical Analysis
3. Results
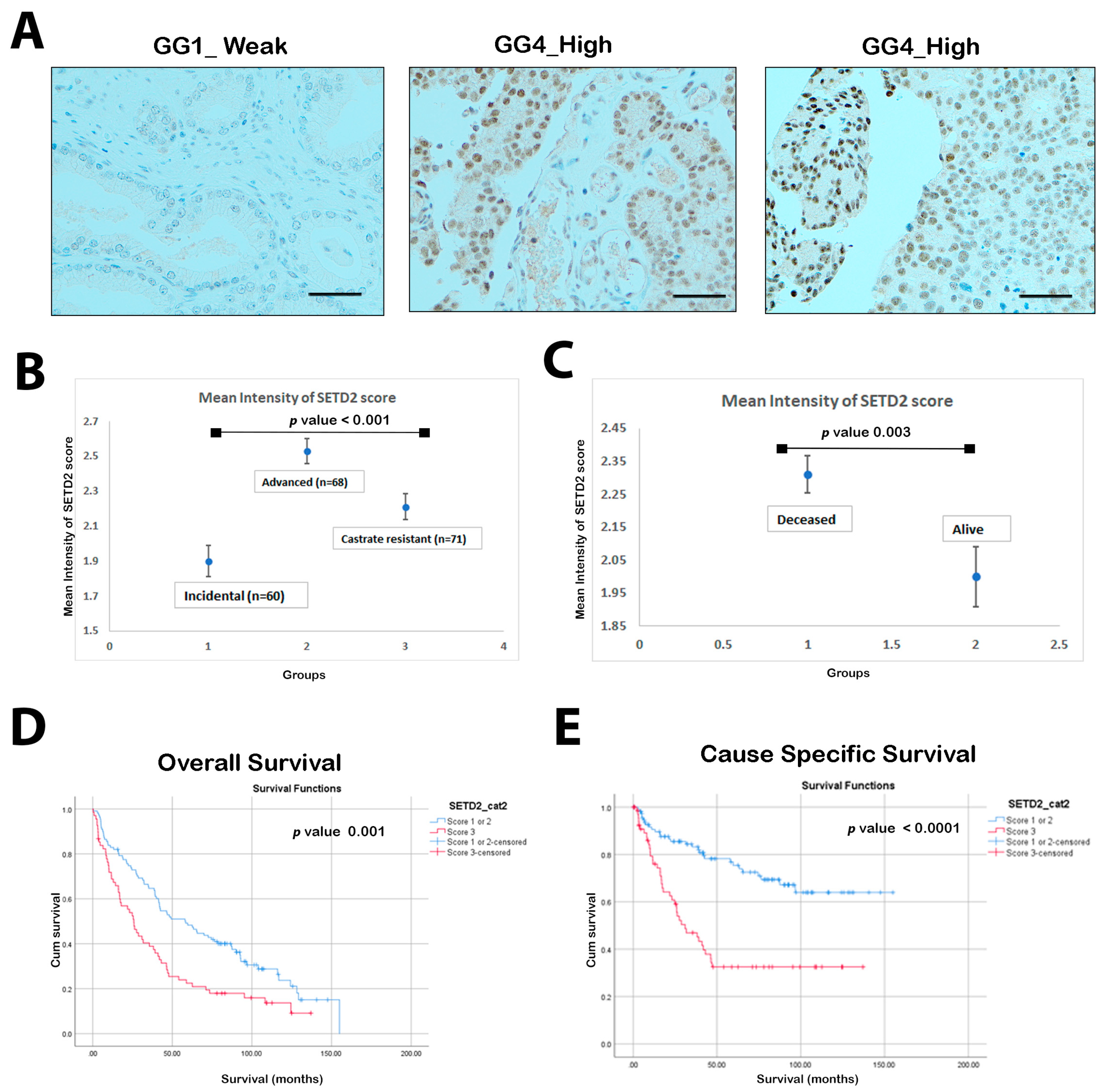
3.1. SETD2 Expression in the Prostate Cancer Cohort
3.2. SETD2 Expression in Relation to Gleason Grade Grouping
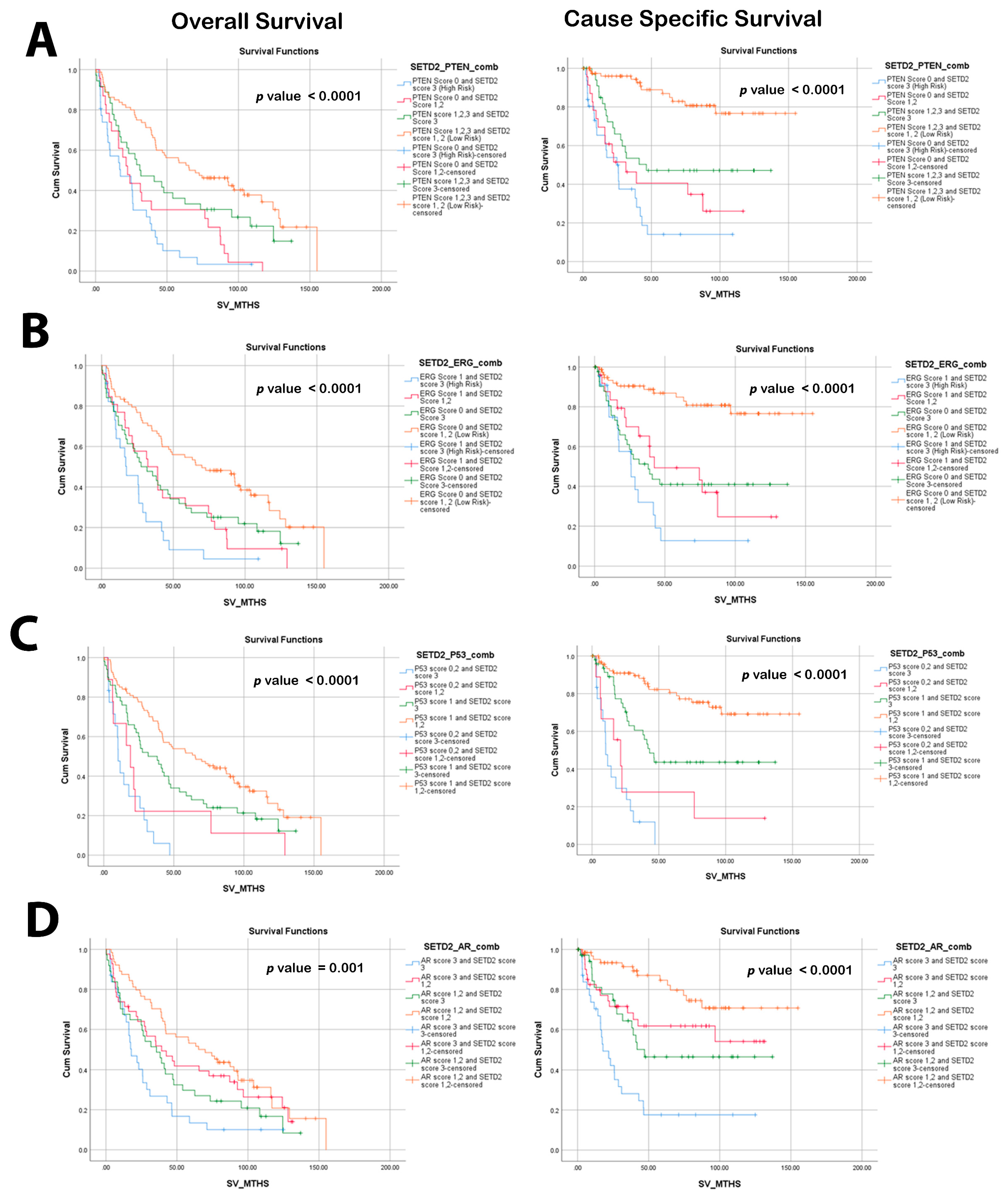
3.3. SETD2 Expression in Relation to PTEN, ERG, and p53
3.4. High SETD2 Expression Is Associated with Poor Overall Survival (OS) and Cause-Specific Survival (CSS) Related to Prostate Cancer Lethality
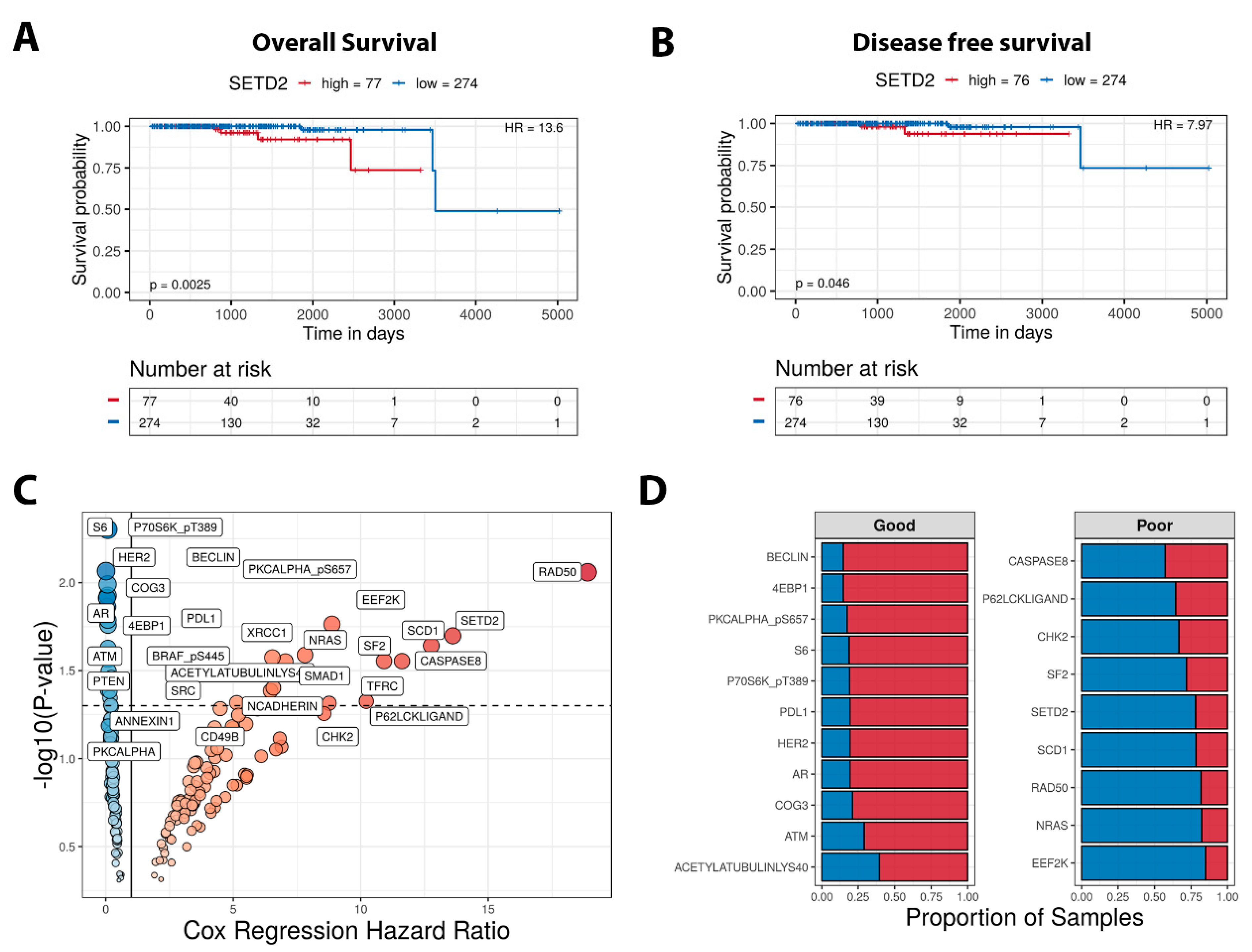
3.5. High Expression of SETD2 Is a Risk Factor and an Indicator of Poor Prognosis in Prostate Cancer (PCa)
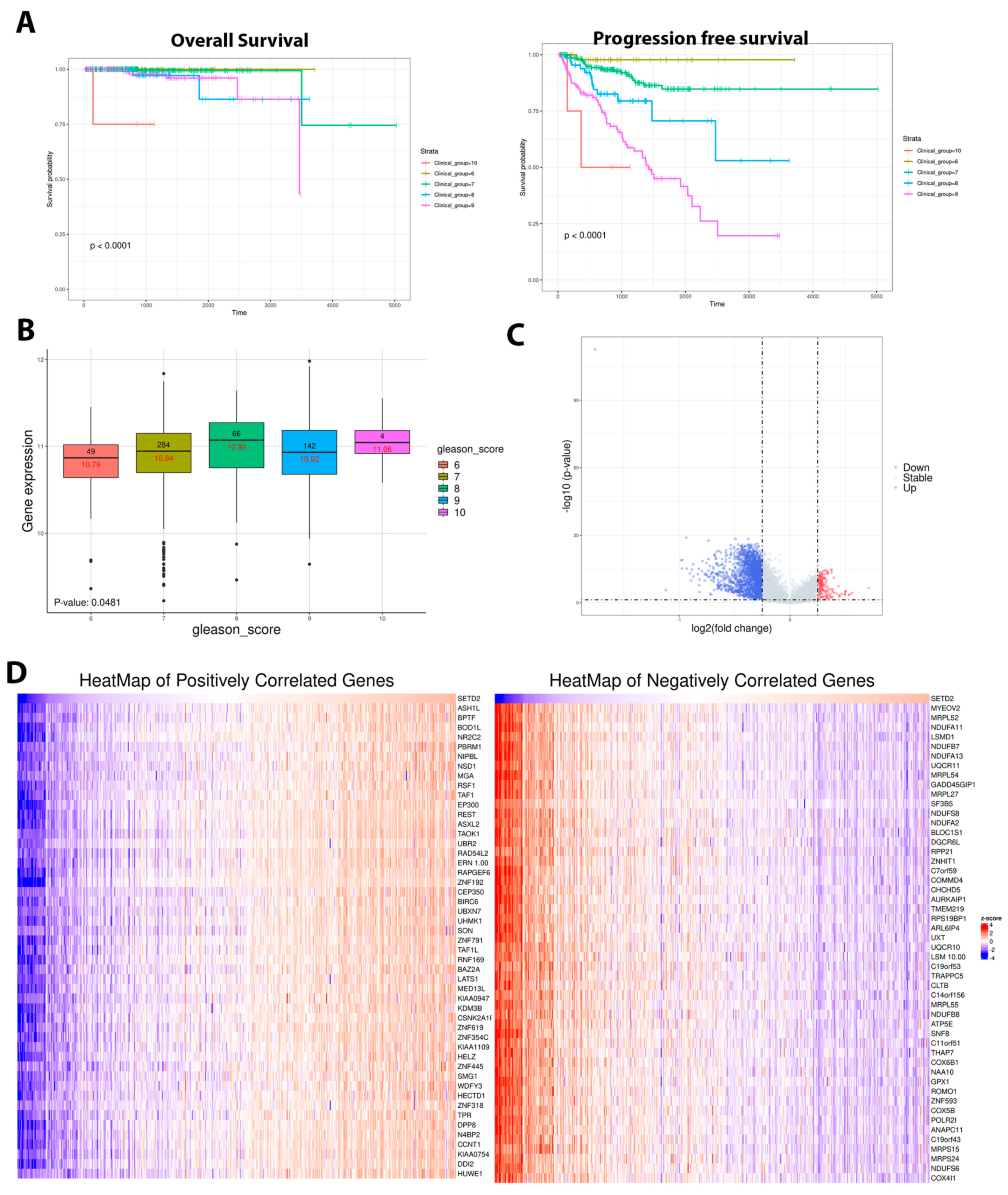
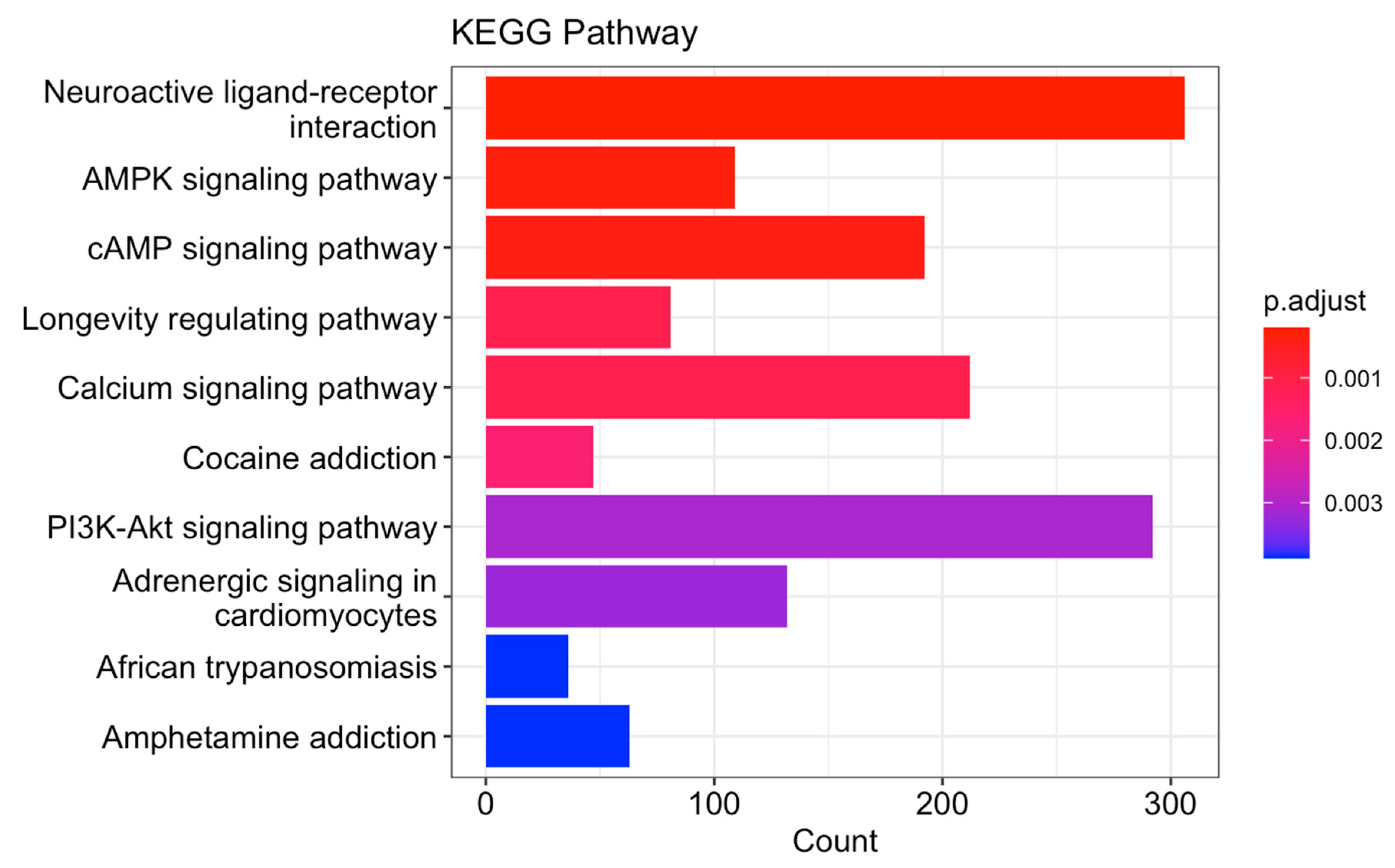
3.6. Gene Set Enrichment Analysis of the Revealed Potential Role of SETD2 in PCa Oncogenesis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SETD2 | SET Domain containing 2 |
| IHC | Immunohistochemistry |
| TMA | Tissue microarray |
| PRAD | Prostate adenocarcinoma |
| CRPCa | Castration-resistant prostate cancer |
| PTEN | Phosphatase and tensin homolog |
| ERG ETS | Transcription factor ERG |
| CSS | Cause-specific survival |
| OS | Overall survival |
| GSEA | Gene set enrichment analysis |
| TCGA | The cancer genome atlas |
| TCPA | The cancer proteome atlas |
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Porzycki, P.; Ciszkowicz, E. Modern biomarkers in prostate cancer diagnosis. Cent. Eur. J. Urol. 2020, 73, 300–306. [Google Scholar] [CrossRef]
- Bismar, T.A.; Hegazy, S.; Feng, Z.; Yu, D.; Donnelly, B.; Palanisamy, N.; Trock, B.J. Clinical utility of assessing PTEN and ERG protein expression in prostate cancer patients: A proposed method for risk stratification. J. Cancer Res. Clin. Oncol. 2018, 144, 2117–2125. [Google Scholar] [CrossRef]
- Kok, K.; Naylor, S.L.; Buys, C.H. Deletions of the short arm of chromosome 3 in solid tumors and the search for suppressor genes. Adv. Cancer Res. 1997, 71, 27–92. [Google Scholar]
- Sun, X.J.; Wei, J.; Wu, X.Y.; Hu, M.; Wang, L.; Wang, H.H.; Chen, C.-J.; Huang, Q.-H.; Chen, Z. Identification and characterization of a novel human histone H3 lysine 36-specific methyltransferase. J. Biol. Chem. 2005, 280, 35261–35271. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, S.; Raposo, A.C.; Martins, F.B.; Grosso, A.R.; Sridhara, S.C.; Rino, J.; Carmo-Fonseca, M.; de Almeida, S.F. Histone methyltransferase SETD2 coordinates FACT recruitment with nucleosome dynamics during transcription. Nucleic Acids Res. 2013, 41, 2881–2893. [Google Scholar] [CrossRef]
- Li, J.; Duns, G.; Westers, H.; Sijmons, R.; van den Berg, A.; Kok, K. SETD2: An epigenetic modifier with tumor suppressor functionality. Oncotarget 2016, 7, 50719. [Google Scholar] [CrossRef] [PubMed]
- Kumari, S.; Singh, M.; Kumar, S.; Muthuswamy, S. SETD2 controls m6A modification of transcriptome and regulates the molecular oncogenesis of glioma. Med. Oncol. 2023, 40, 249. [Google Scholar] [CrossRef]
- Battaglin, F.; Krause, H.; Elliot, A.; Abraham, J.; Soni, S.; Algaze, S.; Jayachandran, P.; Arai, H.; Zhang, W.; Lo, J.H. SETD2 gene expression and the molecular landscape of colorectal cancer (CRC). J. Clin. Oncol. 2023, 41, 4. [Google Scholar] [CrossRef]
- Chen, Z.; Raghoonundun, C.; Chen, W.; Zhang, Y.; Tang, W.; Fan, X.; Shi, X. SETD2 indicates favourable prognosis in gastric cancer and suppresses cancer cell proliferation, migration, and invasion. Biochem. Biophys. Res. Commun. 2018, 498, 579–585. [Google Scholar] [CrossRef]
- Al Sarakbi, W.; Sasi, W.; Jiang, W.G.; Roberts, T.; Newbold, R.F.; Mokbel, K. The mRNA expression of SETD2 in human breast cancer: Correlation with clinico-pathological parameters. BMC Cancer 2009, 9, 290. [Google Scholar] [CrossRef] [PubMed]
- Thienger, P.; Rubin, M.A. SETting Up for Epigenetic Regulation of Advanced Prostate Cancer. Cancer Cell 2020, 38, 309–311. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Xu, T.; Zhao, F.; Guo, J.; Hu, Q. SETD2-H3K36ME3: An important bridge between the environment and tumors. Front. Genet. 2023, 14, 1204463. [Google Scholar] [CrossRef] [PubMed]
- Dalgliesh, G.L.; Furge, K.; Greenman, C.; Chen, L.; Bignell, G.; Butler, A.; Davies, H.; Edkins, S.; Hardy, C.; Latimer, C. Systematic sequencing of renal carcinoma reveals inactivation of histone modifying genes. Nature 2010, 463, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Viaene, A.N.; Santi, M.; Rosenbaum, J.; Li, M.M.; Surrey, L.F.; Nasrallah, M.P. SETD2 mutations in primary central nervous system tumors. Acta Neuropathol. Commun. 2018, 6, 123. [Google Scholar] [CrossRef]
- Forbes, S.A.; Beare, D.; Gunasekaran, P.; Leung, K.; Bindal, N.; Boutselakis, H.; Ding, M.; Bamford, S.; Cole, C.; Ward, S.; et al. COSMIC: Exploring the world’s knowledge of somatic mutations in human cancer. Nucleic Acids Res. 2015, 43, D805–D811. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Ortega, J.; Gu, L.; Li, G.M. Regulation of mismatch repair by histone code and posttranslational modifications in eukaryotic cells. DNA Repair. 2016, 38, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Beltran, H.; Prandi, D.; Mosquera, J.M.; Benelli, M.; Puca, L.; Cyrta, J.; Marotz, C.; Giannopoulou, E.; Balabhadrapatruni, V.S.K.; Elemento, O. Divergent clonal evolution of castration resistant neuroendocrine prostate cancer. Nat. Med. 2016, 22, 298–305. [Google Scholar] [CrossRef]
- Yemelyanova, A.; Vang, R.; Kshirsagar, M.; Lu, D.; Marks, M.A.; Shih, I.M.; Kurman, R.J. Immunohistochemical staining patterns of p53 can serve as a surrogate marker for TP53 mutations in ovarian carcinoma: An immunohistochemical and nucleotide sequencing analysis. Mod. Pathol. 2011, 24, 1248–1253. [Google Scholar] [CrossRef]
- Guedes, L.B.; Almutairi, F.; Haffner, M.C.; Rajoria, G.; Liu, Z.; Klimek, S.; Zoino, R.; Yousefi, K.; Sharma, R.; De Marzo, A.M.; et al. Analytic, Preanalytic, and Clinical Validation of p53 IHC for Detection of TP53 Missense Mutation in Prostate Cancer. Clin. Cancer Res. 2017, 23, 4693–4703. [Google Scholar] [CrossRef]
- Li, J.; Lu, Y.; Akbani, R.; Ju, Z.; Roebuck, P.L.; Liu, W.; Yang, J.-Y.; Broom, B.M.; Verhaak, R.G.; Kane, D.W. TCPA: A resource for cancer functional proteomics data. Nat. Methods 2013, 10, 1046–1047. [Google Scholar] [CrossRef] [PubMed]
- Borcherding, N.; Bormann, N.L.; Voigt, A.P.; Zhang, W. TRGAted: A web tool for survival analysis using protein data in the Cancer Genome Atlas. F1000Research 2018, 7, 1235. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Lichtenberg, T.; Hoadley, K.A.; Poisson, L.M.; Lazar, A.J.; Cherniack, A.D.; Kovatich, A.J.; Benz, C.C.; Levine, D.A.; Lee, A.V.; et al. An Integrated TCGA Pan-Cancer Clinical Data Resource to Drive High-Quality Survival Outcome Analytics. Cell 2018, 173, 400–416.e411. [Google Scholar] [CrossRef] [PubMed]
- Biolake. Available online: https://biolake.ucalgary.ca/ (accessed on 26 December 2023).
- Zhou, J.; Lai, Y.; Peng, S.; Tang, C.; Chen, Y.; Li, L.; Huang, H.; Guo, Z. Comprehensive analysis of TP53 and SPOP mutations and their impact on survival in metastatic prostate cancer. Front. Oncol. 2022, 12, 957404. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Han, Y.; Wang, X.; Li, N.; Liu, Q.; Yin, Y.; Wang, H.; Pan, L.; Li, L.; Song, K. SETD2 restricts prostate cancer metastasis by integrating EZH2 and AMPK signaling pathways. Cancer Cell 2020, 38, 350–365.e357. [Google Scholar] [CrossRef] [PubMed]
- Pungsrinont, T.; Kallenbach, J.; Baniahmad, A. Role of PI3K-AKT-mTOR pathway as a pro-survival signaling and resistance-mediating mechanism to therapy of prostate cancer. Int. J. Mol. Sci. 2021, 22, 11088. [Google Scholar] [CrossRef] [PubMed]
- Khosh Kish, E.; Choudhry, M.; Gamallat, Y.; Buharideen, S.M.; Bismar, T.A. The expression of proto-oncogene ETS-related gene (ERG) plays a central role in the oncogenic mechanism involved in the development and progression of prostate cancer. Int. J. Mol. Sci. 2022, 23, 4772. [Google Scholar] [CrossRef]
- Tosoian, J.J.; Almutairi, F.; Morais, C.L.; Glavaris, S.; Hicks, J.; Sundi, D.; Humphreys, E.; Han, M.; De Marzo, A.M.; Ross, A.E. Prevalence and prognostic significance of PTEN loss in African-American and European-American men undergoing radical prostatectomy. Eur. Urol. 2017, 71, 697–700. [Google Scholar] [CrossRef]
- Shorning, B.Y.; Dass, M.S.; Smalley, M.J.; Pearson, H.B. The PI3K-AKT-mTOR pathway and prostate cancer: At the crossroads of AR, MAPK, and WNT signaling. Int. J. Mol. Sci. 2020, 21, 4507. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ISUP Grade Group Cohort (Gleason Score) | Number and Percentage % |
|---|---|
| Grade group 1 | 63 (61.1%) |
| Grade group 2 (3 + 4) | 14 (13.8%) |
| Grade group 3 (4 + 3) | 20 (19.5%) |
| Grade group 4 (8) | 11 (14.6%) |
| Grade group 5 (9,10) | 78 (91%) |
| Missing | 16 (7.9%) |
| Deceased | |
| Yes | 139 (67.8%) |
| No | 57 (28.2%) |
| Missing | 8 (3.9%) |
| Cancer subgroup | |
| Incidental | 61 (30.2%) |
| Advanced | 69 (34.2%) |
| Castrate-resistant | 72 (35.6%) |
| SEDT2 score (by cancer subgroup) | |
| Score 1 | |
| Incidental | 17 (60.7%) |
| Advanced | 3 (10.7%) |
| Castrate-resistant | 8 (28.6%) |
| Score 2 | |
| Incidental | 32 (32.7%) |
| Advanced | 26 (26.5%) |
| Castrate-resistant | 40 (40.8%) |
| Score 3 | |
| Incidental | 11 (15.1%) |
| Advanced | 39 (53.4%) |
| Castrate-resistant | 23 (31.5%) |
| TP53 and SEDT2 combined | |
| TP53 scores 0, 2, 3, and SEDT2 1/2 | 0 (0%) |
| TP53 scores 0, 2, 3, and SEDT2 3 | 31 (18.1%) |
| TP53 score 1 and SEDT2 1/2 | 25 (100%) |
| TP53 score 1 and SEDT2 3 | 134 (78.6%) |
| PTEN and SEDT2 combined | |
| PTEN loss and SEDT2 score 1/2 | 3 (12%) |
| PTEN loss and SEDT2 score 3 | 52 (30.4%) |
| PTEN intact and SEDT2 1/2 | 22 (88%) |
| PTEN intact and SEDT2 3 | 107 (62.5%) |
| ERG and SEDT2 combined | |
| ERG-positive and SEDT2 score 1/2 | 27 (23.3%) |
| ERG-positive and SEDT2 score 3 | 23 (33.3%) |
| ERG-negative and SEDT2 score 1/2 | 89 (76.7%) |
| ERG-negative and SEDT2 score 3 | 46 (66.7%) |
| Variable | SETD2 Score 3 (High Risk) | SETD2 Score 1 or 2 (Low Risk) | p-Value |
|---|---|---|---|
| Gleason acore | |||
| <=6 | 12 (17.1) | 51 (44.0) | <0.0001 |
| 3 + 4 | 3 (4.3) | 11 (9.5) | |
| 4 + 3 | 4 (5.7) | 16 (13.8) | |
| 8 | 9 (12.9) | 2 (1.7) | |
| 9–10 | 42 (60.0) | 36 (31.0) | |
| PTEN intensity | |||
| Score 0 | 31 (44.9) | 24 (20.9) | 0.001 |
| Score > 0 | 38 (55.1) | 91 (79.1) | |
| ERG dual intensity | |||
| Negative | 46 (66.7) | 89 (76.7) | 0.136 |
| Positive | 23 (33.3) | 27 (23.3) | |
| AR | 0.237 | ||
| Score 1,2 | 39 (54.2) | 76 (62.8) | |
| Score 3 | 33 (45.8) | 45 (37.2) | |
| P53 | 0.003 | ||
| Score 1 | 53 (73.6) | 106 (89.8) | |
| Score 0, 2 | 19 (26.4) | 12 (10.2) |
| Overall Survival HR (95% CI) | p-Value | Cause-Specific Survival HR (95% CI) | p-Value | |
|---|---|---|---|---|
| PTEN gain score 1, 2, and 3) | ||||
| Loss—score 0 | 2.71 (1.89–3.89) | <0.0001 | 4.50 (2.76–7.34) | <0.0001 |
| ERG (Negative) | ||||
| Positive | 1.93 (1.34–2.77) | <0.0001 | 2.53 (1.55–4.11) | <0.0001 |
| GS (<=6) | ||||
| GS 3 + 4 | 2.03 (0.98–4.20) | 0.056 | 24.18 (2.70–216.62) | <0.0001 |
| GS 4 + 3 | 1.41 (0.72–2.77) | 0.322 | 9.68 (1.01–93.15) | 0.049 |
| GS 8 | 5.09 (2.47–10.49) | <0.0001 | 71.43 (8.68–588.10) | <0.0001 |
| GS 9, 10 | 6.02 (3.80–9.51) | <0.0001 | 107.23 (14.73–780.83) | <0.0001 |
| SETD2 low risk—score 1 or 2 | ||||
| SETD2 high risk—score 3 | 1.80 (1.28–2.53) | 0.001 | 3.14 (1.94–5.08) | <0.0001 |
| Combination PTEN and SETD2 (PTEN score 1, 2, and 3 and SETD2 score 1 and 2) | ||||
| PTEN score 0 and SETD2 score 3 | 3.78 (2.36–6.08) | <0.0001 | 10.10 (4.93–20.67) | <0.0001 |
| PTEN score 0 and SETD2 score 1 and 2 | 2.68 (1.62–4.41) | <0.0001 | 6.59 (3.07–14.12) | <0.0001 |
| PTEN score 1, 2, and 3 and SETD2 score 3 | 1.60 (1.01–2.54) | 0.047 | 3.98 (1.90–8.35) | <0.0001 |
| Combination PTEN and SETD2 (PTEN score 1, 2, and 3 and SETD2 score 1 and 2) * | ||||
| PTEN score 0 and SETD2 score 3 | 2.12 (1.22–3.69) | 0.008 | 3.74 (1.67–8.34) | 0.001 |
| PTEN score 0 and SETD2 score 1 and 2 | 1.28 (0.73–2.26) | 0.395 | 1.85 (0.81–4.22) | 0.144 |
| PTEN score 1, 2, and 3 and SETD2 score 3 | 0.96 (0.58–1.59) | 0.866 | 1.55 (0.70–3.43) | 0.278 |
| Combination ERG and SETD2 (ERG negative and SETD2 score 1 and 2) | ||||
| ERG positive and SETD2 score 3 | 3.30 (1.96–5.58) | <0.0001 | 7.64 (3.59–16.25) | <0.0001 |
| ERG positive and SETD2 score 1 and 2 | 1.99 (1.22–3.25) | 0.006 | 4.20 (1.97–8.96) | <0.0001 |
| ERG negative and SETD2 score 3 | 1.80 (1.17–2.76) | 0.008 | 4.41 (2.24–8.67) | <0.0001 |
| Combination ERG and SETD2 (ERG negative and SETD2 score 1 and 2) * | ||||
| ERG positive and SETD2 score 3 | 1.99 (0.87–4.59) | 0.015 | 2.14 (0.98–4.68) | 0.058 |
| ERG positive and SETD2 score 1 and 2 | 1.45 (0.73–2.89) | 0.292 | 1.12 (0.50–2.51) | 0.782 |
| ERG negative and SETD2 score 3 | 1.02 (0.63–1.63) | 0.943 | 1.54 (0.77–3.11) | 0.225 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gamallat, Y.; Felipe Lima, J.; Seyedi, S.; Li, Q.; Rokne, J.G.; Alhajj, R.; Ghosh, S.; Bismar, T.A. Exploring The Prognostic Significance of SET-Domain Containing 2 (SETD2) Expression in Advanced and Castrate-Resistant Prostate Cancer. Cancers 2024, 16, 1436. https://doi.org/10.3390/cancers16071436
Gamallat Y, Felipe Lima J, Seyedi S, Li Q, Rokne JG, Alhajj R, Ghosh S, Bismar TA. Exploring The Prognostic Significance of SET-Domain Containing 2 (SETD2) Expression in Advanced and Castrate-Resistant Prostate Cancer. Cancers. 2024; 16(7):1436. https://doi.org/10.3390/cancers16071436
Chicago/Turabian StyleGamallat, Yaser, Joema Felipe Lima, Sima Seyedi, Qiaowang Li, Jon George Rokne, Reda Alhajj, Sunita Ghosh, and Tarek A. Bismar. 2024. "Exploring The Prognostic Significance of SET-Domain Containing 2 (SETD2) Expression in Advanced and Castrate-Resistant Prostate Cancer" Cancers 16, no. 7: 1436. https://doi.org/10.3390/cancers16071436
APA StyleGamallat, Y., Felipe Lima, J., Seyedi, S., Li, Q., Rokne, J. G., Alhajj, R., Ghosh, S., & Bismar, T. A. (2024). Exploring The Prognostic Significance of SET-Domain Containing 2 (SETD2) Expression in Advanced and Castrate-Resistant Prostate Cancer. Cancers, 16(7), 1436. https://doi.org/10.3390/cancers16071436