


Overall Survival after Radiotherapy for Brain Metastases According to ECOG Status—A Prospective Study of 294 NSCLC Patients
 ,
,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
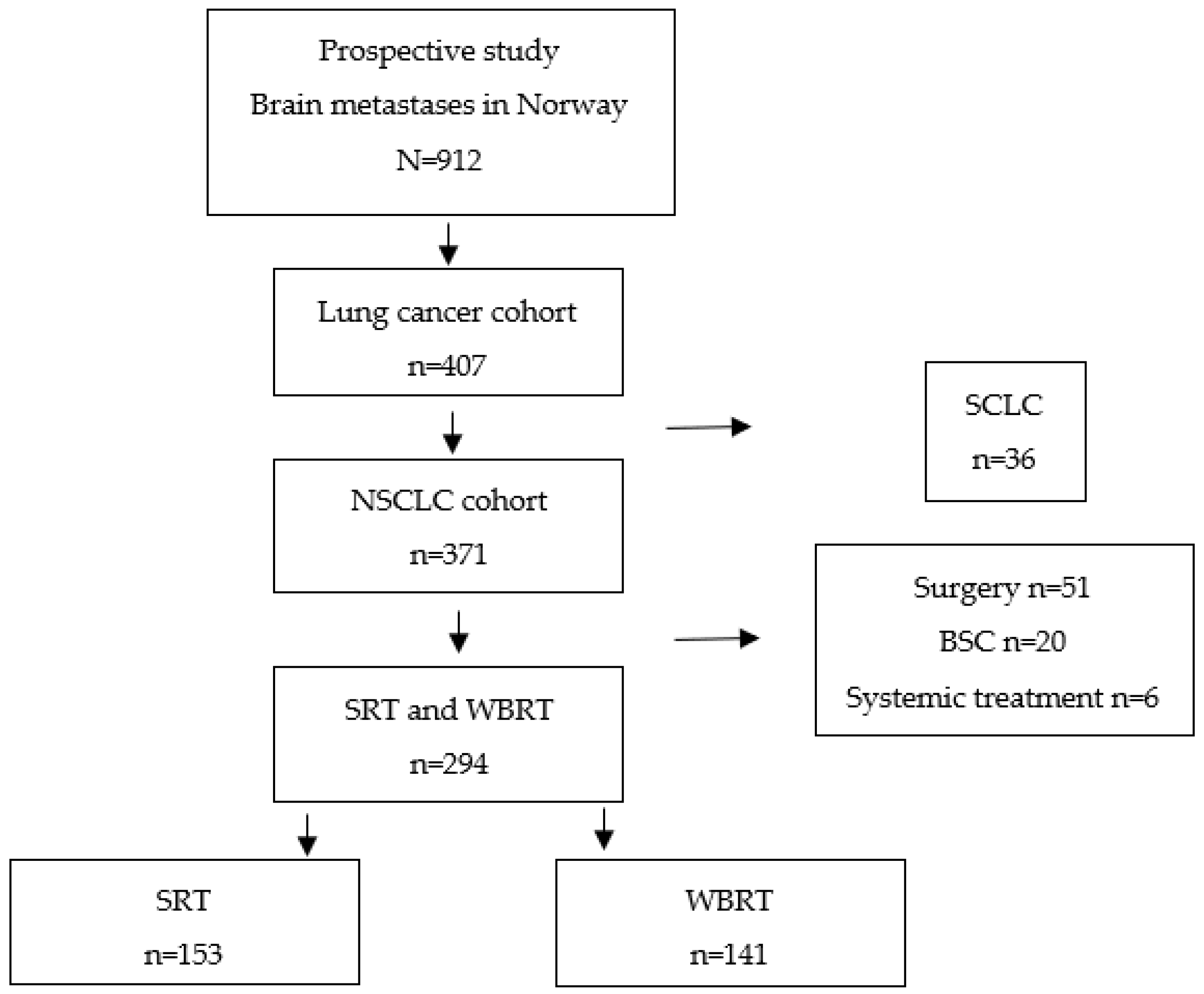
2.1. Study Design
2.2. Identification
2.3. Patient Characteristics
2.4. Treatment
2.5. Lung GPA and Updated RPA
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Characteristics
3.2. Treatment
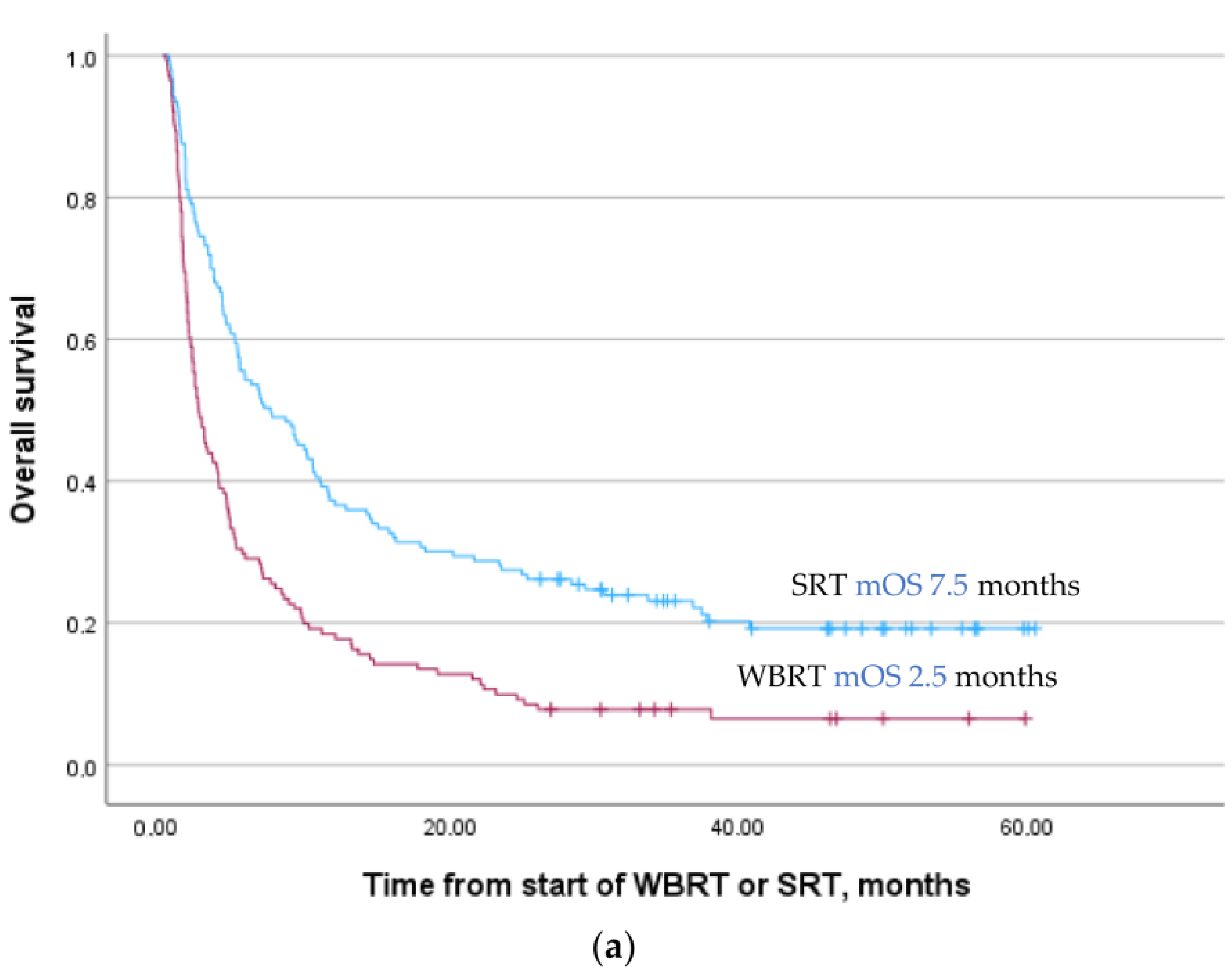
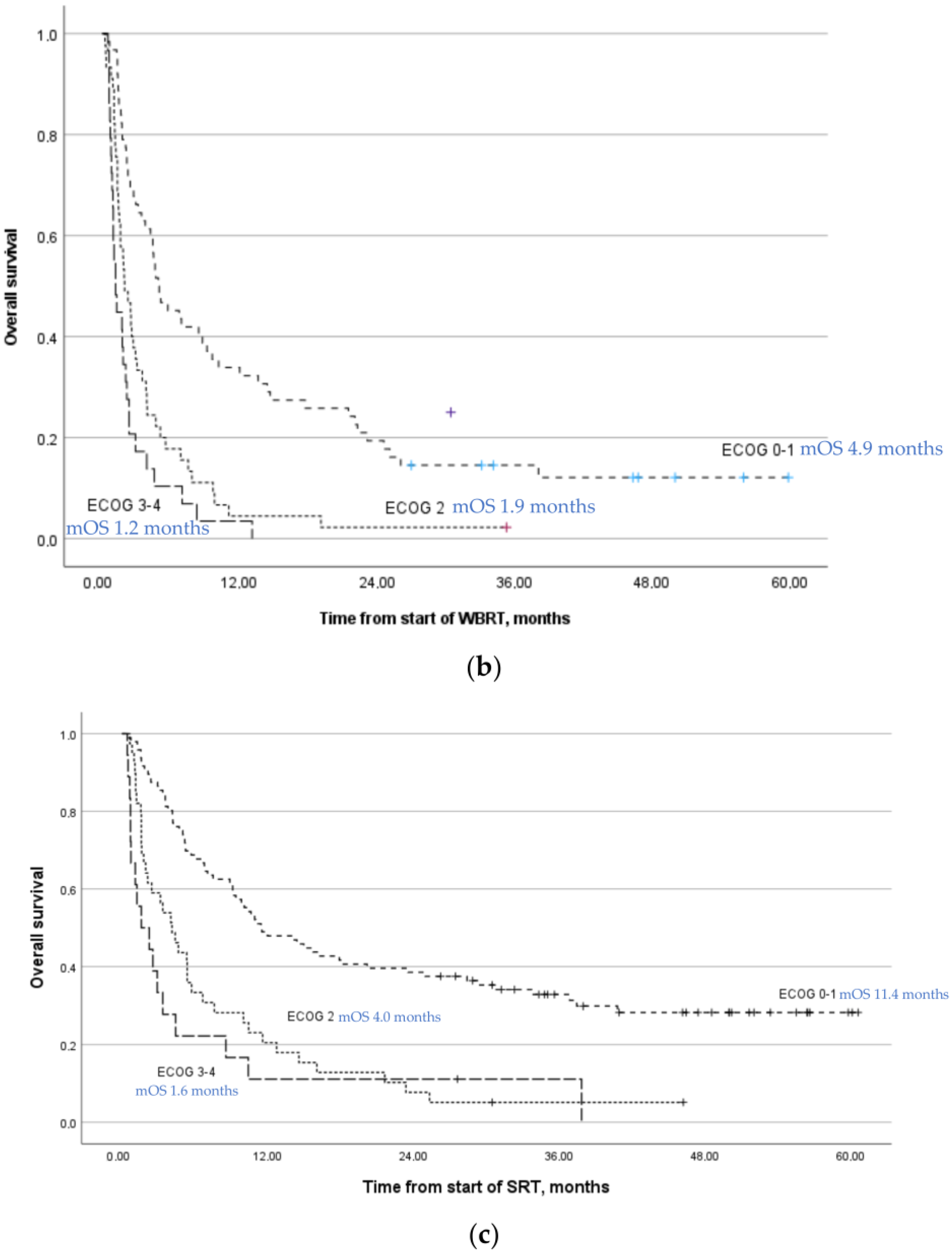
3.3. Overall Survival
3.4. Lung GPA and U-RPA
3.4.1. Lung GPA
3.4.2. U-RPA
3.5. Univariable and Multivariable Analysis
4. Discussion
4.1. Major Findings
4.2. Multivariable Analysis
4.3. Patients with ECOG 2–4
4.4. Lung GPA and U-RPA
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Registry of Norway. Cancer Incidence, Mortality, Survival and Prevalence in Norway; Cancer Registry of Norway: Oslo, Norway, 2022. [Google Scholar]
- Thandra, K.C.; Barsouk, A.; Saginala, K.; Aluru, J.S.; Barsouk, A. Epidemiology of lung cancer. Contemp. Oncol. 2021, 25, 45–52. [Google Scholar] [CrossRef]
- Sacks, P.; Rahman, M. Epidemiology of Brain Metastases. Neurosurg. Clin. N. Am. 2020, 31, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of brain metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Cagney, D.N.; Martin, A.M.; Catalano, P.J.; Redig, A.J.; Lin, N.U.; Lee, E.Q.; Wen, P.Y.; Dunn, I.F.; Bi, W.L.; Weiss, S.E.; et al. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: A population-based study. Neuro Oncol. 2017, 19, 1511–1521. [Google Scholar] [CrossRef] [PubMed]
- Brockelsby, C.; Maconachie, R.; Navani, N.; Prendecki, R.; Randles, V.; King, J.; Dildar, B.; Lee, X.; Nagarajan, T.; Rice, M.; et al. Brain imaging in lung cancer staging: A real-world, multi-centre study of prevalence of brain metastases, impact on treatment and re-modelling of the NICE health economic analysis. Lung Cancer 2023, 178, 145–150. [Google Scholar] [CrossRef]
- Martin, M.; Hernanz, R.; Vallejo, C.; Guerrero, L.; Mielgo, X.; Lopez, A.; Trujillo-Reyes, J.C.; Couñago, F. Brain metastases from non-small cell lung carcinoma: An overview of classical and novel treatment strategies. Rep. Pract. Oncol. Radiother. J. Greatpoland Cancer Cent. Pozn. Pol. Soc. Radiat. Oncol. 2022, 27, 527–544. [Google Scholar] [CrossRef] [PubMed]
- Tsui, D.C.C.; Camidge, D.R.; Rusthoven, C.G. Managing Central Nervous System Spread of Lung Cancer: The State of the Art. J. Clin. Oncol. 2022, 40, 642–660. [Google Scholar] [CrossRef]
- Tsakonas, G.; Ekman, S.; Koulouris, A.; Adderley, H.; Ackermann, C.J.; Califano, R. Safety and efficacy of immune checkpoint blockade in patients with advanced nonsmall cell lung cancer and brain metastasis. Int. J. Cancer 2023, 153, 1556–1567. [Google Scholar] [CrossRef]
- Vogelbaum, M.A.; Brown, P.D.; Messersmith, H.; Brastianos, P.K.; Burri, S.; Cahill, D.; Dunn, I.F.; Gaspar, L.E.; Gatson, N.T.N.; Gondi, V.; et al. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J. Clin. Oncol. 2022, 40, 492–516. [Google Scholar] [CrossRef]
- Brown, P.D.; Ballman, K.V.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Whitton, A.C.; Greenspoon, J.; Parney, I.F.; Laack, N.N.I.; Ashman, J.B.; et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC.3): A multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1049–1060. [Google Scholar] [CrossRef]
- El Gantery, M.M.; Abd El Baky, H.M.; El Hossieny, H.A.; Mahmoud, M.; Youssef, O. Management of brain metastases with stereotactic radiosurgery alone versus whole brain irradiation alone versus both. Radiat. Oncol. 2014, 9, 116. [Google Scholar] [CrossRef]
- Mulvenna, P.; Nankivell, M.; Barton, R.; Faivre-Finn, C.; Wilson, P.; McColl, E.; Moore, B.; Brisbane, I.; Ardron, D.; Holt, T.; et al. Dexamethasone and supportive care with or without whole brain radiotherapy in treating patients with non-small cell lung cancer with brain metastases unsuitable for resection or stereotactic radiotherapy (QUARTZ): Results from a phase 3, non-inferiority, randomised trial. Lancet 2016, 388, 2004–2014. [Google Scholar] [CrossRef]
- Glatzer, M.; Faivre-Finn, C.; De Ruysscher, D.; Widder, J.; Van Houtte, P.; Troost, E.G.C.; Slotman, B.J.; Ramella, S.; Pöttgen, C.; Peeters, S.T.H.; et al. Role of radiotherapy in the management of brain metastases of NSCLC—Decision criteria in clinical routine. Radiother. Oncol. 2021, 154, 269–273. [Google Scholar] [CrossRef]
- Frisk, G.; Helde Frankling, M.; Warnqvist, A.; Björkhem-Bergman, L.; Hedman, M. Evaluation of Whole Brain Radiotherapy among Lung Cancer Patients with Brain Metastases in Relation to Health Care Level and Survival. Life 2022, 12, 525. [Google Scholar] [CrossRef]
- Bernat, J.L. Medical futility: Definition, determination, and disputes in critical care. Neurocrit. Care 2005, 2, 198–205. [Google Scholar] [CrossRef]
- Gaspar, L.; Scott, C.; Rotman, M.; Asbell, S.; Phillips, T.; Wasserman, T.; McKenna, W.G.; Byhardt, R. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 745–751. [Google Scholar] [CrossRef]
- Sperduto, P.W.; De, B.; Li, J.; Carpenter, D.; Kirkpatrick, J.; Milligan, M.; Shih, H.A.; Kutuk, T.; Kotecha, R.; Higaki, H.; et al. Graded Prognostic Assessment (GPA) for Patients With Lung Cancer and Brain Metastases: Initial Report of the Small Cell Lung Cancer GPA and Update of the Non-Small Cell Lung Cancer GPA Including the Effect of Programmed Death Ligand 1 and Other Prognostic Factors. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 60–74. [Google Scholar] [CrossRef]
- Fadul, C.E.; Sarai, G.; Bovi, J.A.; Thomas, A.A.; Novicoff, W.; Anderson, R.; Amidon, R.F.; Schuetz, S.; Singh, R.; Chang, A.; et al. Relevance of the Updated Recursive Partitioning Analysis (U-RPA) Classification in the Contemporary Care of Patients with Brain Metastases. Cancers 2023, 15, 3255. [Google Scholar] [CrossRef]
- ESMO. Performance Scales: Karnofsky & ECOG Scores Practice Tools. Available online: https://oncologypro.esmo.org/oncology-in-practice/practice-tools/performance-scales (accessed on 8 March 2024).
- Altmann, D.G.; Bryant, T.N.; Gardner, M.J. Statistics with Confidence, 2nd ed.; BMK Books: London, UK, 2000. [Google Scholar]
- STROBE Strengthening the Reporting of Observational Studies in Epidemiology. Available online: https://www.strobe-statement.org (accessed on 8 March 2024).
- Karlsson, A.T.; Hjermstad, M.J.; Omdahl, T.; Aass, N.; Skovlund, E.; Hellebust, T.P.; Johansen, S.; Kaasa, S.; Yri, O.E. Overall survival after initial radiotherapy for brain metastases; a population based study of 2140 patients with non-small cell lung cancer. Acta Oncol. 2021, 60, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- van Schie, P.; Rijksen, B.L.T.; Bot, M.; Wiersma, T.; Merckel, L.G.; Brandsma, D.; Compter, A.; de Witt Hamer, P.C.; Post, R.; Borst, G.R. Optimizing treatment of brain metastases in an era of novel systemic treatments: A single center consecutive series. J. Neurooncol. 2023, 163, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Jiang, K.; Parker, M.; Materi, J.; Azad, T.D.; Kamson, D.O.; Kleinberg, L.; Ye, X.; Rincon-Torroella, J.; Bettegowda, C. Epidemiology and survival outcomes of synchronous and metachronous brain metastases: A retrospective population-based study. Neurosurg. Focus 2023, 55, E3. [Google Scholar] [CrossRef]
- Natesan, D.; Carpenter, D.J.; Giles, W.; Oyekunle, T.; Niedzwiecki, D.; Reitman, Z.J.; Kirkpatrick, J.P.; Floyd, S.R. Clinical Factors Associated With 30-Day Mortality Among Patients Undergoing Radiation Therapy for Brain Metastases. Adv. Radiat. Oncol. 2023, 8, 101211. [Google Scholar] [CrossRef]
- Jeene, P.M.; de Vries, K.C.; van Nes, J.G.H.; Kwakman, J.J.M.; Wester, G.; Rozema, T.; Braam, P.M.; Zindler, J.D.; Koper, P.; Nuyttens, J.J.; et al. Survival after whole brain radiotherapy for brain metastases from lung cancer and breast cancer is poor in 6325 Dutch patients treated between 2000 and 2014. Acta Oncol. 2018, 57, 637–643. [Google Scholar] [CrossRef]
- Le Rhun, E.; Guckenberger, M.; Smits, M.; Dummer, R.; Bachelot, T.; Sahm, F.; Galldiks, N.; de Azambuja, E.; Berghoff, A.S.; Metellus, P.; et al. EANO-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours. Ann. Oncol. 2021, 32, 1332–1347. [Google Scholar] [CrossRef]
- Gondi, V.; Bauman, G.; Bradfield, L.; Burri, S.H.; Cabrera, A.R.; Cunningham, D.A.; Eaton, B.R.; Hattangadi-Gluth, J.A.; Kim, M.M.; Kotecha, R.; et al. Radiation Therapy for Brain Metastases: An ASTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 2022, 12, 265–282. [Google Scholar] [CrossRef]
- Hollen, P.J.; Gralla, R.J.; Stewart, J.A.; Chin, C.; Bizette, G.A.; Leighl, N.B.; Kuruvilla, P.G.; Meharchand, J.M.; Solow, H. A Prospective Comparison of Karnofsky (KPS) with ECOG Performance Status in Patients with Non-Small Cell Lung Cancer (NSCLC): A COMET Group Study Investigating Sensitivity and Specificity Issues Important in Clinical Decision Making. J. Clin. Oncol. 2005, 23, 8134. Available online: https://ascopubs.org/doi/10.1200/jco.2005.23.16_suppl.8134 (accessed on 10 October 2023). [CrossRef]
- Temel, J.S.; Greer, J.A.; Muzikansky, A.; Gallagher, E.R.; Admane, S.; Jackson, V.A.; Dahlin, C.M.; Blinderman, C.D.; Jacobsen, J.; Pirl, W.F.; et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 733–742. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients n 294 (%) | WBRT n 141 (%) | SRT n 153 (%) | p-Value WBRT vs. SRT | |
|---|---|---|---|---|
| Age | 0.430 | |||
| <70 | 152 (52) | 76 (54) | 76 (50) | |
| ≥70 | 142 (48) | 65 (46) | 77 (50) | |
| ECOG | 0.009 | |||
| ECOG 0–1 | 158 (54) | 62 (44) | 96 (63) | |
| ECOG 2 | 85 (29) | 46 (32) | 39 (25) | |
| ECOG 3–4 | 47 (16) | 29 (21) | 18 (12) | |
| Unknown | 4 (1) | 4 (3) | ||
| Histology | 0.092 | |||
| Adenocarcinoma | 216 (73) | 111 (79) | 105 (69) | |
| Squamous cell carcinoma | 44 (15) | 14 (10) | 30 (20) | |
| Others * | 34 (12) | 16 (11) | 18 (11) | |
| Number of BMs | <0.001 | |||
| 1 | 89 (30) | 9 (6) | 80 (52) | |
| 2–4 | 100 (34) | 30 (21) | 70 (46) | |
| ≥5 | 102 (35) | 99 (71) | 3 (2) | |
| Unknown | 3 (1) | 3 (2) | ||
| EGFR mutation | 0.846 | |||
| Yes | 18 (6) | 9 (6) | 9 (6) | |
| No/unknown | 276 (94) | 132 (94) | 144 (94) | |
| ALK translocation | 0.929 | |||
| Yes | 4 (1) | 2 (1) | 2 (1) | |
| No/unknown | 299 (99) | 139 (99) | 153 (99) | |
| PD-L1 positive | 0.009 | |||
| Yes | 153 (52) | 62 (44) | 91 (59) | |
| No/unknown | 141 (48) | 79 (56) | 62 (41) | |
| Clinical status primary tumor | 0.305 | |||
| Primary tumor controlled/removed | 86 (30) | 37 (26) | 49 (32) | |
| Progressive/not evaluated | 55 (18) | 31 (22) | 24 (16) | |
| Synchronous diagnosis of BMs and lung tumor | 153 (52) | 73 (52) | 80 (52) | |
| Extracranial metastases | <0.001 | |||
| Controlled | 124 (42) | 45 (32) | 79 (52) | |
| Uncontrolled | 170 (58) | 96 (68) | 74 (48) |
| (a) | |||||||
| Total Cohort Adenocarcinoma | WBRT | SRT | Lung GPA | ||||
| Score Lung GPA | Actual mOS m (IQR) | n = 216 (%) | Actual mOS m (IQR) | n = 110 (%) | Actual mOS m (IQR) | n = 104 (%) | Predicted mOS m (IQR) * |
| 0.0–1.0 | 3.5 (2, 9) | 80 (37) | 3.2 (2, 7) | 62 (56) | 6.8 (2, 12) | 18 (17) | 6 (2, 13) |
| 1.5–2.0 | 6.9 (3, 23) | 96 (44) | 4.3 (3, 15) | 43 (39) | 10.2 (3, 38) | 53 (51) | 15 (5, 38) |
| 2.5–3.0 | 25.1 (7, NR) | 38 (18) | 38.2 (6, NR) | 5 (5) | 25.1 (8, NR) | 33 (32) | 30 (12, NR) |
| 3.5–4.0 | 2 (1) | 52 (25, 69) | |||||
| (b) | |||||||
| Total Cohort Non-adenocarcinoma | WBRT | SRT | Lung GPA | ||||
| Score Lung GPA | Actual mOS m (IQR) | n = 78 (%) | Actual mOS m (IQR) | n = 30 (%) | Actual mOS m (IQR) | n = 48 (%) | Predicted mOS m (IQR) |
| 0.0–1.0 | 2.2 (2, 4) | 17 (22) | 2.4 (2, 4) | 13 (43) | 1.4 (1, 2) | 4 (8) | 2 (1, 49) |
| 1.5–2.0 | 3.7 (2, 7) | 28 (36) | 2.9 (2, 4) | 10 (33) | 5.5 (2, 7) | 18 (38) | 5 (3, 12) |
| 2.5–3.0 | 5.2 (3, 12) | 27 (35) | 2.7 (2, 5) | 6 (20 | 5.7 (2, 16) | 28 (44) | 10 (4, 21) |
| 3.5–4.0 | 4.6 (3, 24) | 6 (7) | 1 (3) | 17.1 (5, 24) | 5 (10) | 19 (8, 33) | |
| U-RPA | Total Cohort * | WBRT | SRT | U-RPA | |||
|---|---|---|---|---|---|---|---|
| Actual mOS Months (95% CI) | n = 290 (%) | Actual mOS Months (95% CI) | n = 137 (%) | Actual mOS Months (95% CI) | n = 153 (%) | Predicted mOS Months | |
| Class 1 | 17.1 (0–42.3) | 16 (6) | 22.3 (0.0–46.7) | 8 (6) | 9.5 (0.0–26.5) | 8 (5) | 28.1 |
| Class 2 | |||||||
| A | 14.9 (4.1–25.8) | 40 (14) | 4.3 (0.0–13.7) | 12 (9) | 19.7 (0.0–49.9) | 28 (18) | 14.7 |
| B | 5.6 (4.2–7.0) | 187(64) | 3.4 (2.7–4.2) | 88 (64) | 7.5 (4.5–10.4) | 99 (65) | 7.6 |
| Class 3 | 2.2 (1.6–2.8) | 47 (16) | 2.0 (1.3–2.6) | 29 (21) | 2.5 (1.4–3.6) | 18 (12) | 3.3 |
| All Patients n 294 | |||||
|---|---|---|---|---|---|
| n | Unadjusted HR (95% CI) | p-Value | Adjusted HR (95% CI) | p-Value | |
| Age | |||||
| <70 | 152 | 1 | 1 | ||
| ≥70 | 142 | 1.3 (1.0–1.6) | 0.053 | 1.3 (1.0–1.6) | 0.082 |
| ECOG | |||||
| ECOG 0–1 | 158 | 1 | 1 | ||
| ECOG 2 | 85 | 2.5 (1.9–3.4) | <0.001 | 2.3 (1.7–3.1) | <0.001 |
| ECOG 3–4 | 47 | 4.0 (2.8–5.7) | <0.001 | 3.8 (2.6–5.5) | <0.001 |
| Unknown | 4 | 1.3 (0.4–4.0) | 0.685 | 0.8 (0.2–2.5) | 0.674 |
| Histology | |||||
| Adenocarcinoma | 216 | 1 | 1 | ||
| Squamous cell carcinoma | 44 | 1.4 (1.0–2.0) | 0.055 | 1.4 (0.9–1.9) | 0.105 |
| Others * | 34 | 1.7 (1.2–2.5) | 0.006 | 1.7 (1.1–2.6) | 0.009 |
| Number of BMs | |||||
| 1 | 89 | 1 | 1 | ||
| 2–4 | 100 | 1.1 (0.8–1.5) | 0.658 | 1.4 (1.0–1.9) | 0.052 |
| ≥5 | 102 | 1.6 (1.1–2.1) | 0.005 | 1.5 (1.1–2.2) | 0.012 |
| Unknown | 3 | 4.5 (1.4–14.5) | 0.011 | 5.3 (1.5–17.9) | 0.008 |
| Mutation/PD-L1 positive ** | |||||
| Yes | 172 | 1 | 1 | ||
| No | 122 | 1.3 (1.0–1.6) | 0.051 | 1.1 (0.8–1.4) | 0.505 |
| Clinical status primary tumor | |||||
| Primary tumor controlled/removed | 86 | 1 | 1 | ||
| Progressive/not evaluated | 55 | 1.4 (1.0–2.1) | 0.044 | 1.3 (0.9–1.9) | 0.214 |
| Synchronous diagnosis of BMs and lung tumor | 153 | 0.9 (0.7–1.2) | 0.399 | 0.7 (0.5–1.0) | 0.045 |
| Extracranial metastases | |||||
| Controlled | 124 | 1 | 1 | ||
| Uncontrolled | 170 | 1.7 (1.3–2.1) | <0.001 | 1.7 (1.3–2.3) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karlsson, A.T.; Hjermstad, M.J.; Aass, N.; Skovlund, E.; Kaasa, S.; Yri, O.E. Overall Survival after Radiotherapy for Brain Metastases According to ECOG Status—A Prospective Study of 294 NSCLC Patients. Cancers 2024, 16, 1486. https://doi.org/10.3390/cancers16081486
Karlsson AT, Hjermstad MJ, Aass N, Skovlund E, Kaasa S, Yri OE. Overall Survival after Radiotherapy for Brain Metastases According to ECOG Status—A Prospective Study of 294 NSCLC Patients. Cancers. 2024; 16(8):1486. https://doi.org/10.3390/cancers16081486
Chicago/Turabian StyleKarlsson, Astrid Telhaug, Marianne Jensen Hjermstad, Nina Aass, Eva Skovlund, Stein Kaasa, and Olav Erich Yri. 2024. "Overall Survival after Radiotherapy for Brain Metastases According to ECOG Status—A Prospective Study of 294 NSCLC Patients" Cancers 16, no. 8: 1486. https://doi.org/10.3390/cancers16081486
APA StyleKarlsson, A. T., Hjermstad, M. J., Aass, N., Skovlund, E., Kaasa, S., & Yri, O. E. (2024). Overall Survival after Radiotherapy for Brain Metastases According to ECOG Status—A Prospective Study of 294 NSCLC Patients. Cancers, 16(8), 1486. https://doi.org/10.3390/cancers16081486