
The sGCa Vericiguat Exhibit Cardioprotective and Anti-Sarcopenic Effects through NLRP-3 Pathways: Potential Benefits for Anthracycline-Treated Cancer Patients

 ,
,  ,
,  ,
,  , , , and
, , , and 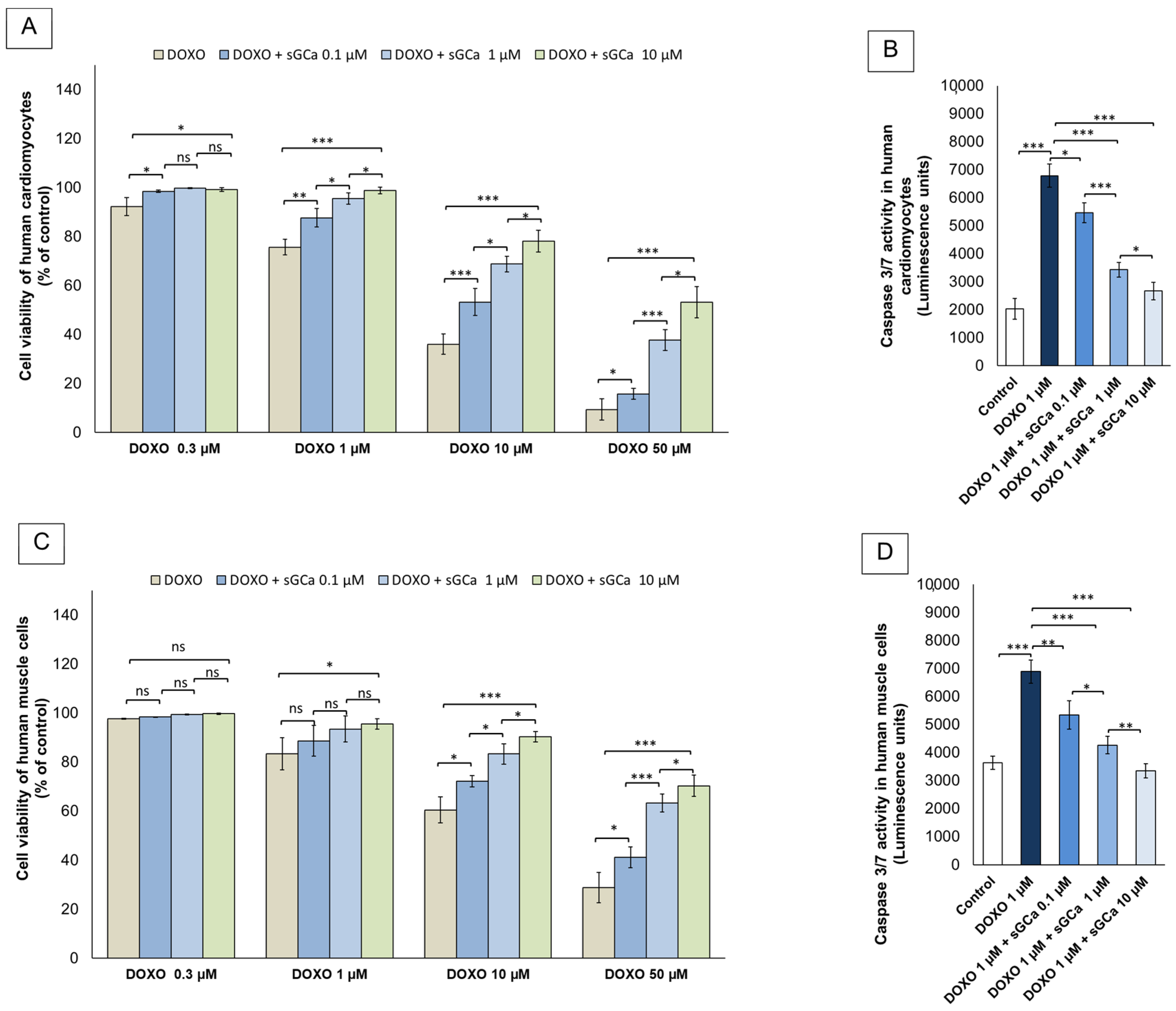{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Lines and Pharmacological Treatments
2.2. Cell Survival, LDH, and Cytochrome C Release during Exposure to Vericiguat Alone or Combined to Anthracyclines
2.3. Intracellular Ca++ Content
2.4. Measurement cGMP Intracellular Levels
2.5. Staining of Intracellular cGMP through CLSM
2.6. Apoptosis Study through TUNEL Assay
2.7. NLRP-3, MyD-88 Cellular Expression
2.8. Cytokines and Growth Factors Assay
2.9. Statistical Analysis
3. Results
3.1. Cytoprotective Properties of Vericiguat
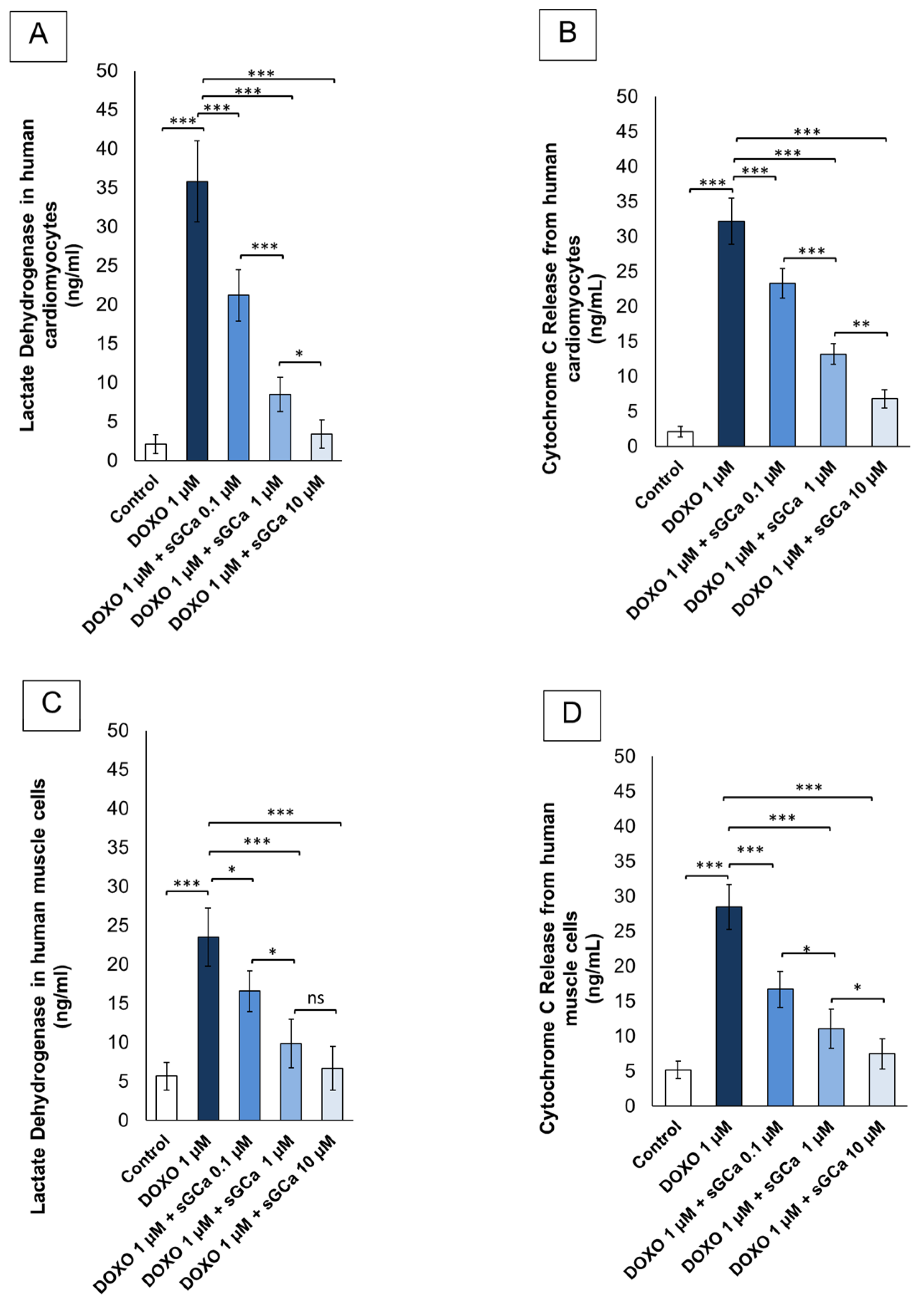
3.2. Vericiguat Reduces Lactate Dehydrogenases (LDH) and Cytochrome-c Release
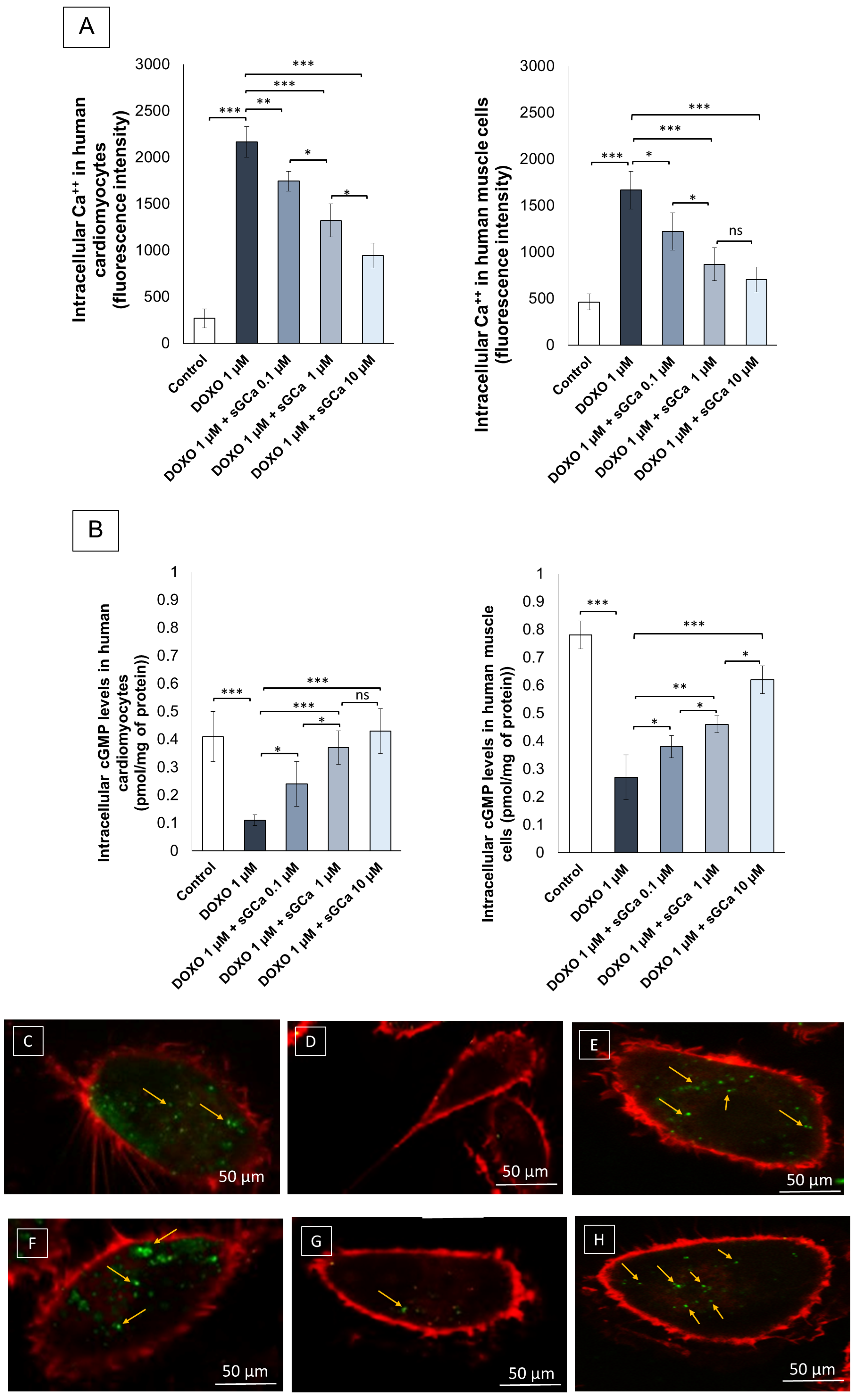
3.3. Vericiguat Reduced Intracellular Ca++ Levels during Exposure to Doxorubicin
3.4. Vericiguat Restores cGMP Intracellular Levels during Exposure to Doxorubicin
3.5. cGMP Levels Staining through Confocal Laser Scanning Microscope Method
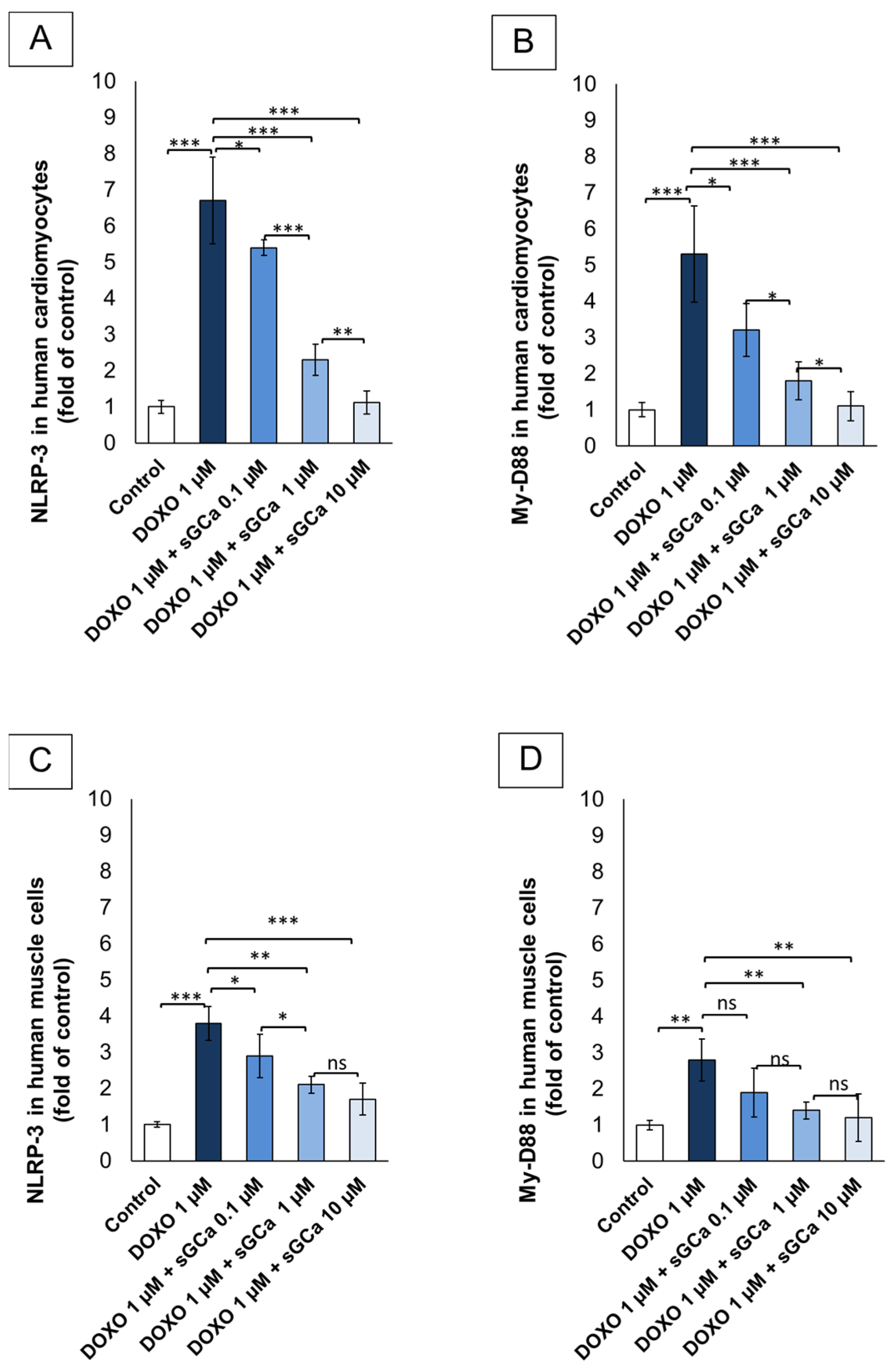
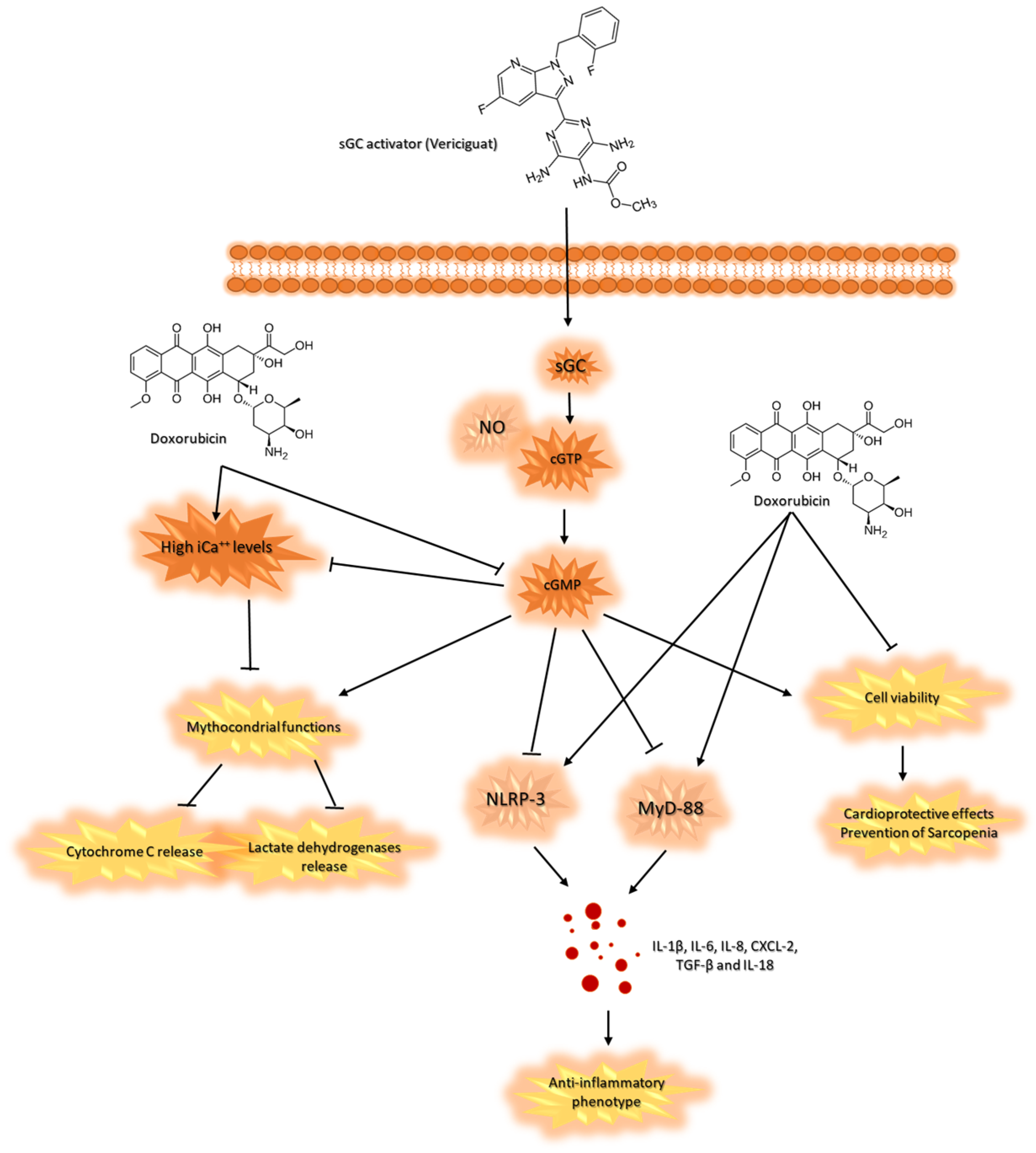
3.6. Vericiguat Reduces NLRP-3 and MyD88 Levels
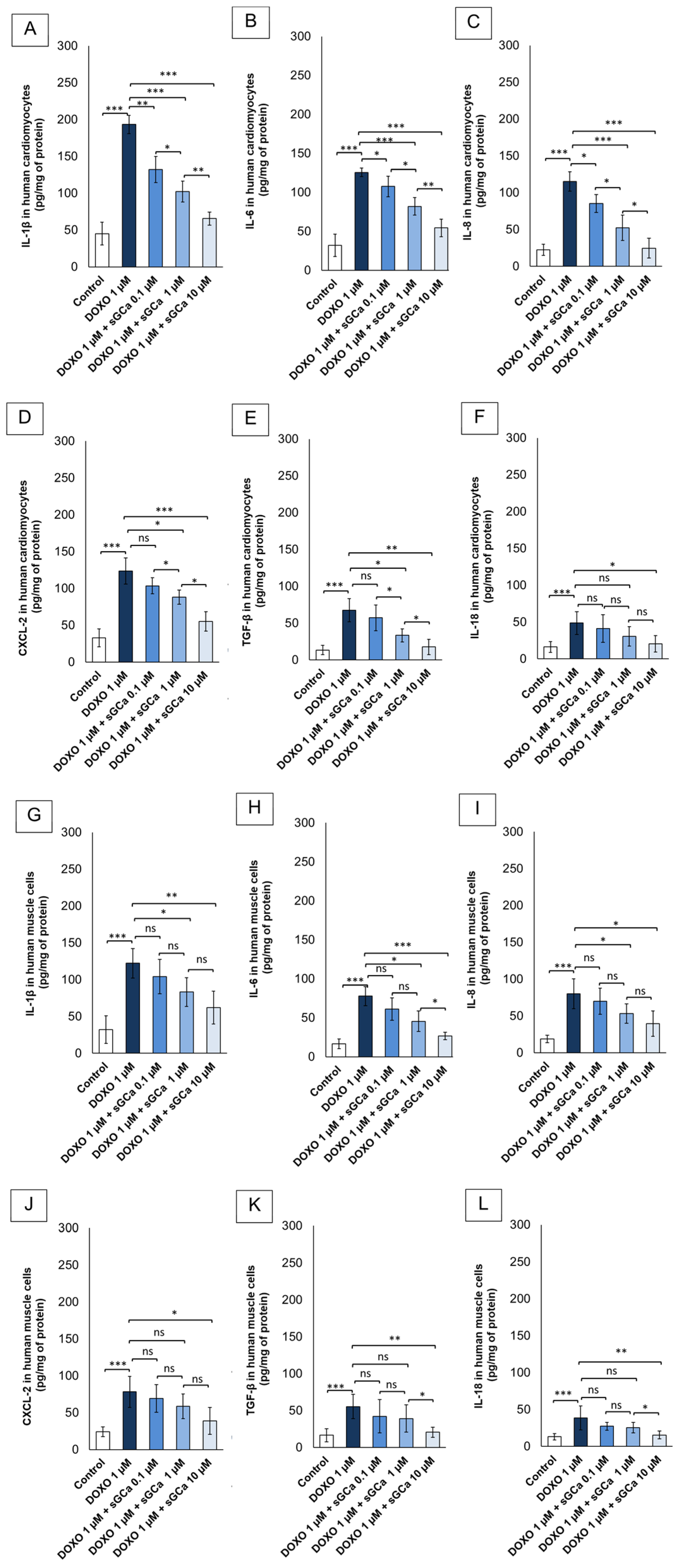
3.7. Vericiguat Reduces Intracellular Cytokines and Chemokines Involved in Sarcopenia and Cardiotoxicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, J.; Long, J.B.; Hurria, A.; Owusu, C.; Steingart, R.M.; Gross, C.P. Incidence of heart failure or cardiomyopathy after adjuvant trastuzumab therapy for breast cancer. J. Am. Coll. Cardiol. 2012, 60, 2504–2512. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Iacopo, F.; Cipolla, C.M. Cardiotoxicity of Anthracyclines. Front. Cardiovasc. Med. 2020, 7, 26. [Google Scholar] [CrossRef]
- Qiu, Y.; Jiang, P.; Huang, Y. Anthracycline-induced cardiotoxicity: Mechanisms, monitoring, and prevention. Front. Cardiovasc. Med. 2023, 10, 1242596. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.; Della Sala, A.; Tocchetti, C.G.; Porporato, P.E.; Ghigo, A. Metabolic Aspects of Anthracycline Cardiotoxicity. Curr. Treat. Options Oncol. 2021, 22, 18. [Google Scholar] [CrossRef]
- Carrasco, R.; Castillo, R.L.; Gormaz, J.G.; Carrillo, M.; Thavendiranathan, P. Role of Oxidative Stress in the Mechanisms of Anthracycline-Induced Cardiotoxicity: Effects of Preventive Strategies. Oxid. Med. Cell. Longev. 2021, 2021, 8863789. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Wu, R.; Chen, L.; Yang, Z.; Yan, D.; Li, M. Understanding Anthracycline Cardiotoxicity from Mitochondrial Aspect. Front. Pharmacol. 2022, 13, 811406. [Google Scholar] [CrossRef] [PubMed]
- Seara, F.A.C.; Kasai-Brunswick, T.H.; Nascimento, J.H.M.; Campos-de-Carvalho, A.C. Anthracycline-induced cardiotoxicity and cell senescence: New therapeutic option? Cell Mol. Life Sci. 2022, 79, 568. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Colombo, A.; Lamantia, G.; Colombo, N.; Civelli, M.; De Giacomi, G.; Rubino, M.; Veglia, F.; Fiorentini, C.; Cipolla, C.M. Anthracycline-induced cardiomyopathy: Clinical relevance and response to pharmacologic therapy. J. Am. Coll. Cardiol. 2010, 55, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Kelley, N.; Jeltema, D.; Duan, Y.; He, Y. The NLRP3 Inflammasome: An Overview of Mechanisms of Activation and Regulation. Int. J. Mol. Sci. 2019, 20, 3328. [Google Scholar] [CrossRef] [PubMed]
- Quagliariello, V.; Passariello, M.; Bisceglia, I.; Paccone, A.; Inno, A.; Maurea, C.; Rapuano Lembo, R.; Manna, L.; Iovine, M.; Canale, M.L.; et al. Combinatorial immune checkpoint blockade increases myocardial expression of NLRP-3 and secretion of H-FABP, NT-Pro-BNP, interleukin-1β and interleukin-6: Biochemical implications in cardio-immuno-oncology. Front. Cardiovasc. Med. 2024, 11, 1232269. [Google Scholar] [CrossRef]
- Leszek, P.; Klotzka, A.; Bartuś, S.; Burchardt, P.; Czarnecka, A.M.; Długosz-Danecka, M.; Gierlotka, M.; Koseła-Paterczyk, H.; Krawczyk-Ożóg, A.; Kubiatowski, T.; et al. A practical approach to the 2022 ESC cardio-oncology guidelines: Comments by a team of experts—Cardiologists and oncologists. Kardiol. Pol. 2023, 81, 1047–1063. [Google Scholar] [CrossRef] [PubMed]
- Bas, O.; Erdemir, A.G.; Onur, M.R.; Ozer, N.; Sener, Y.Z.; Aksu, S.; Barista, I.; Guner, G.; Guven, D.C.; Kertmen, N.; et al. Sarcopenia and anthracycline cardiotoxicity in patients with cancer. BMJ Support. Palliat. Care 2023, 13, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.L.; Azodi, M.; Heymans, S.; Heggermont, W. Anthracycline-Related Heart Failure: Certain Knowledge and Open Questions: Where Do we Stand with Chemotherapyinduced Cardiotoxicity? Curr. Heart Fail. Rep. 2020, 17, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Jang, M.K.; Park, C.; Tussing-Humphreys, L.; Fernhall, B.; Phillips, S.; Doorenbos, A.Z. The Effectiveness of Sarcopenia Interventions for Cancer Patients Receiving Chemotherapy: A Systematic Review and Meta-analysis. Cancer Nurs. 2023, 46, E81–E90. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.M.Y.; Wong, H.; Zhang, N.; Chow, S.K.H.; Chau, W.W.; Wang, J.; Chim, Y.N.; Leung, K.S.; Cheung, W.H. The relationship between sarcopenia and fragility fracture-a systematic review. Osteoporos. Int. 2019, 30, 541–553. [Google Scholar] [CrossRef] [PubMed]
- Wooten, S.V.; Roth, M.; Livingston, J.A.; Hildebrandt, M.A.T.; Chandra, J.; Amini, B.; Kleinerman, E.S.; Gilchrist, S.C. Short-Term Changes in Skeletal Muscle Mass After Anthracycline Administration in Adolescent and Young Adult Sarcoma Patients. J. Adolesc. Young Adult Oncol. 2022, 11, 320–322. [Google Scholar] [CrossRef]
- Prado, C.M.; Baracos, V.E.; McCargar, L.J.; Reiman, T.; Mourtzakis, M.; Tonkin, K.; Mackey, J.R.; Koski, S.; Pituskin, E.; Sawyer, M.B. Sarcopenia as a determinant of chemotherapy toxicity and time to tumor progression in metastatic breast cancer patients receiving capecitabine treatment. Clin. Cancer Res. 2009, 15, 2920–2926. [Google Scholar] [CrossRef] [PubMed]
- Kourek, C.; Touloupaki, M.; Rempakos, A.; Loritis, K.; Tsougkos, E.; Paraskevaidis, I.; Briasoulis, A. Cardioprotective Strategies from Cardiotoxicity in Cancer Patients: A Comprehensive Review. J. Cardiovasc. Dev. Dis. 2022, 9, 259. [Google Scholar] [CrossRef]
- Quagliariello, V.; De Laurentiis, M.; Rea, D.; Barbieri, A.; Monti, M.G.; Carbone, A.; Paccone, A.; Altucci, L.; Conte, M.; Canale, M.L.; et al. The SGLT-2 inhibitor empagliflozin improves myocardial strain, reduces cardiac fibrosis and pro-inflammatory cytokines in non-diabetic mice treated with doxorubicin. Cardiovasc. Diabetol. 2021, 20, 150. [Google Scholar] [CrossRef]
- Omland, T.; Heck, S.L.; Gulati, G. The Role of Cardioprotection in Cancer Therapy Cardiotoxicity: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2022, 4, 19–37. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.K.; Greene, S.J.; Fudim, M.; Mentz, R.J.; Butler, J.; Khan, M.S. Vericiguat for the treatment of heart failure with reduced ejection fraction. Expert Rev. Cardiovasc. Ther. 2023, 21, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, P.W.; Pieske, B.; Anstrom, K.J.; Ezekowitz, J.; Hernandez, A.F.; Butler, J.; Lam, C.S.P.; Ponikowski, P.; Voors, A.A.; Jia, G.; et al. VICTORIA Study Group. Vericiguat in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2020, 382, 1883–1893. [Google Scholar] [CrossRef] [PubMed]
- Hulot, J.S.; Trochu, J.N.; Donal, E.; Galinier, M.; Logeart, D.; De Groote, P.; Juillière, Y. Vericiguat for the treatment of heart failure: Mechanism of action and pharmacological properties compared with other emerging therapeutic options. Expert. Opin. Pharmacother. 2021, 22, 1847–1855. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, M.E.; Ayalasomayajula, S.; Blaustein, R.O.; Gheyas, F. Vericiguat, a novel sGC stimulator: Mechanism of action, clinical, and translational science. Clin. Transl. Sci. 2023, 16, 2458–2466. [Google Scholar] [CrossRef] [PubMed]
- Di Fusco, S.A.; Alonzo, A.; Aimo, A.; Matteucci, A.; Intravaia, R.C.; Aquilani, S.; Cipriani, M.; De Luca, L.; Navazio, A.; Valente, S.; et al. ANMCO position paper on vericiguat use in heart failure: From evidence to place in therapy. Eur. Heart J. Suppl. 2023, 25 (Suppl. D), D278–D286. [Google Scholar] [CrossRef] [PubMed]
- Sahana, U.; Wehland, M.; Simonsen, U.; Schulz, H.; Grimm, D. A Systematic Review of the Effect of Vericiguat on Patients with Heart Failure. Int. J. Mol. Sci. 2023, 24, 11826. [Google Scholar] [CrossRef] [PubMed]
- Belenkov, Y.N.; Arutyunov, G.P.; Mareev, V.Y.; Koziolova, N.A.; Sitnikova, M.Y.; Ageev, F.T.; Gilyarevsky, S.R.; Chesnikova, A.I.; Yakushin, S.S.; Perepech, N.B.; et al. Prospects for use of Vericiguat in HFrEF: Implications of VICTORIA Trial Results. Advisory Board Summary. Kardiologiia 2023, 63, 3–10. (In Russian) [Google Scholar] [CrossRef] [PubMed]
- Butler, J.; Stebbins, A.; Melenovský, V.; Sweitzer, N.K.; Cowie, M.R.; Stehlik, J.; Khan, M.S.; Blaustein, R.O.; Ezekowitz, J.A.; Hernandez, A.F.; et al. VICTORIA Study Group. Vericiguat and Health-Related Quality of Life in Patients with Heart Failure With Reduced Ejection Fraction: Insights From the VICTORIA Trial. Circ. Heart Fail. 2022, 15, e009337. [Google Scholar] [CrossRef]
- Hu, B.A.; Li, Y.L.; Han, H.T.; Lu, B.; Jia, X.; Han, L.; Ma, W.X.; Zhu, P.; Wang, Z.H.; Zhang, W.; et al. Stimulation of soluble guanylate cyclase by vericiguat reduces skeletal muscle atrophy of mice following chemotherapy. Front. Pharmacol. 2023, 14, 1112123. [Google Scholar] [CrossRef] [PubMed]
- Shakuta, S.; Noda, T.; Kamiya, K.; Hamazaki, N.; Nozaki, K.; Yamashita, M.; Uchida, S.; Ueno, K.; Maekawa, E.; Yamaoka-Tojo, M.; et al. Clinical Impact of Improvement in Sarcopenia through Cardiac Rehabilitation in Patients with Heart Failure. J. Am. Med. Dir. Assoc. 2024, 25, 514–520.e2. [Google Scholar] [CrossRef]
- Hardee, J.P.; Lynch, G.S. Current pharmacotherapies for sarcopenia. Expert. Opin. Pharmacother. 2019, 20, 1645–1657. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.X.; Cho, H.; Lee, S.; Woo, J.S.; Song, M.Y.; Cheng, X.W.; Lee, K.H.; Kim, W. BAY60-2770 attenuates doxorubicin-induced cardiotoxicity by decreased oxidative stress and enhanced autophagy. Chem. Biol. Interact. 2020, 328, 109190. [Google Scholar] [CrossRef] [PubMed]
- Bosman, M.; Krüger, D.N.; Favere, K.; Wesley, C.D.; Neutel, C.H.G.; Van Asbroeck, B.; Diebels, O.R.; Faes, B.; Schenk, T.J.; Martinet, W.; et al. Doxorubicin Impairs Smooth Muscle Cell Contraction: Novel Insights in Vascular Toxicity. Int. J. Mol. Sci. 2021, 22, 12812. [Google Scholar] [CrossRef] [PubMed]
- Murata, T.; Yamawaki, H.; Yoshimoto, R.; Hori, M.; Sato, K.; Ozaki, H.; Karaki, H. Chronic effect of doxorubicin on vascular endothelium assessed by organ culture study. Life Sci. 2001, 69, 2685–2695. [Google Scholar] [CrossRef] [PubMed]
- Quagliariello, V.; Berretta, M.; Buccolo, S.; Iovine, M.; Paccone, A.; Cavalcanti, E.; Taibi, R.; Montopoli, M.; Botti, G.; Maurea, N. Polydatin Reduces Cardiotoxicity and Enhances the Anticancer Effects of Sunitinib by Decreasing Pro-Oxidative Stress, Pro-Inflammatory Cytokines, and NLRP3 Inflammasome Expression. Front. Oncol. 2021, 11, 680758. [Google Scholar] [CrossRef]
- Almalik, A.; Alradwan, I.; Majrashi, M.A.; Alsaffar, B.A.; Algarni, A.T.; Alsuabeyl, M.S.; Alrabiah, H.; Tirelli, N.; Alhasan, A.H. Cellular responses of hyaluronic acid-coated chitosan nanoparticles. Toxicol. Res. 2018, 7, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Chraniuk, M.; Panasiuk, M.; Hovhannisyan, L.; Żołędowska, S.; Nidzworski, D.; Ciołek, L.; Woźniak, A.; Jaegermann, Z.; Biernat, M.; Gromadzka, B. The Preliminary Assessment of New Biomaterials Necessitates a Comparison of Direct and Indirect Cytotoxicity Methodological Approaches. Polymers 2022, 14, 4522. [Google Scholar] [CrossRef] [PubMed]
- Tesei, A.; Rosetti, M.; Ulivi, P.; Fabbri, F.; Medri, L.; Vannini, I.; Bolla, M.; Amadori, D.; Zoli, W. Study of molecular mechanisms of pro-apoptotic activity of NCX 4040, a novel nitric oxide-releasing aspirin, in colon cancer cell lines. J. Transl. Med. 2007, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Linders, A.N.; Dias, I.B.; López Fernández, T.; Tocchetti, C.G.; Bomer, N.; Van der Meer, P. A review of the pathophysiological mechanisms of doxorubicin-induced cardiotoxicity and aging. NPJ Aging 2024, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Occelli, L.M.; Sun, K.; Winkler, P.A.; Morgan, B.J.; Petersen-Jones, S.M. Elevated retinal cGMP is not associated with elevated circulating cGMP levels in a canine model of retinitis pigmentosa. PLoS ONE 2022, 17, e0279437. [Google Scholar] [CrossRef] [PubMed]
- Quagliariello, V.; Iaffaioli, R.V.; Armenia, E.; Clemente, O.; Barbarisi, M.; Nasti, G.; Berretta, M.; Ottaiano, A.; Barbarisi, A. Hyaluronic Acid Nanohydrogel Loaded with Quercetin Alone or in Combination to a Macrolide Derivative of Rapamycin RAD001 (Everolimus) as a New Treatment for Hormone-Responsive Human Breast Cancer. J. Cell. Physiol. 2017, 232, 2063–2074. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.M.; Zorman, J.; Horton, M.; Dubey, S.; ter Meulen, J.; Vora, K.A. Caspase activation as a versatile assay platform for detection of cytotoxic bacterial toxins. J. Clin. Microbiol. 2013, 51, 2970–2976. [Google Scholar] [CrossRef] [PubMed]
- Quagliariello, V.; Passariello, M.; Rea, D.; Barbieri, A.; Iovine, M.; Bonelli, A.; Caronna, A.; Botti, G.; De Lorenzo, C.; Maurea, N. Evidences of CTLA-4 and PD-1 Blocking Agents-Induced Cardiotoxicity in Cellular and Preclinical Models. J. Pers. Med. 2020, 10, 179. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gogia, A.; Deo, S.; Sharma, D.N.; Mathur, S.; Sagiraju, H.K.R. Neoadjuvant chemotherapy with or without anthracyclines in combination with single HER2-targeted therapy in HER2-positive breast cancer. Cancer Treat. Res. Commun. 2023, 36, 100741. [Google Scholar] [CrossRef] [PubMed]
- Mallard, J.; Hucteau, E.; Charles, A.L.; Bender, L.; Baeza, C.; Pélissie, M.; Trensz, P.; Pflumio, C.; Kalish-Weindling, M.; Gény, B.; et al. Chemotherapy impairs skeletal muscle mitochondrial homeostasis in early breast cancer patients. J. Cachexia Sarcopenia Muscle 2022, 13, 1896–1907. [Google Scholar] [CrossRef] [PubMed]
- Mallard, J.; Hucteau, E.; Bender, L.; Moinard-Butot, F.; Rochelle, E.; Boutonnet, L.; Grandperrin, A.; Schott, R.; Pflumio, C.; Trensz, P.; et al. A single chemotherapy administration induces muscle atrophy, mitochondrial alterations and apoptosis in breast cancer patients. J. Cachexia Sarcopenia Muscle 2024, 15, 292–305. [Google Scholar] [CrossRef] [PubMed]
- Eyob, T.; Ng, T.; Chan, R.; Chan, A. Impact of chemotherapy on cancer-related fatigue and cytokines in 1312 patients: A systematic review of quantitative studies. Curr. Opin. Support. Palliat. Care 2016, 10, 165–179. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Mendiguchía, J.; González-Costello, J.; Roca, J.; Ariza-Solé, A.; Manito, N.; Cequier, A. Anthracycline-mediated cardiomyopathy: Basic molecular knowledge for the cardiologist. Arch. Cardiol. Mex. 2014, 84, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Wienke, A. Prevalence of sarcopenia in patients with solid tumors: A meta-analysis based on 81,814 patients. JPEN J. Parenter. Enter. Nutr. 2022, 46, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- van Dronkelaar, C.; Tieland, M.; Aarden, J.J.; Reichardt, L.A.; van Seben, R.; van der Schaaf, M.; van der Esch, M.; Engelbert, R.H.H.; Twisk, J.W.R.; Bosch, J.A.; et al. Hospital-ADL Study Group. Decreased Appetite is Associated with Sarcopenia-Related Outcomes in Acute Hospitalized Older Adults. Nutrients 2019, 11, 932. [Google Scholar] [CrossRef]
- Prokopidis, K.; Cervo, M.M.; Gandham, A.; Scott, D. Impact of Protein Intake in Older Adults with Sarcopenia and Obesity: A Gut Microbiota Perspective. Nutrients 2020, 12, 2285. [Google Scholar] [CrossRef]
- Kreidieh, D.; Itani, L.; El Masri, D.; Tannir, H.; El Ghoch, M. Association Between Reduced Daily Steps and Sarcopenic Obesity in Treatment-Seeking Adults with Obesity. Front. Endocrinol. 2020, 11, 22. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Junior, H.J.; Calvani, R.; Azzolino, D.; Picca, A.; Tosato, M.; Landi, F.; Cesari, M.; Marzetti, E. Protein Intake and Sarcopenia in Older Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8718. [Google Scholar] [CrossRef] [PubMed]
- Bozzetti, F. Chemotherapy-Induced Sarcopenia. Curr. Treat. Options Oncol. 2020, 21, 7. [Google Scholar] [CrossRef] [PubMed]
- Mir, A.; Badi, Y.; Bugazia, S.; Nourelden, A.Z.; Fathallah, A.H.; Ragab, K.M.; Alsillak, M.; Elsayed, S.M.; Hagrass, A.I.; Bawek, S.; et al. Efficacy and safety of cardioprotective drugs in chemotherapy-induced cardiotoxicity: An updated systematic review & network meta-analysis. Cardiooncology 2023, 9, 10. [Google Scholar]
- Avula, V.; Sharma, G.; Kosiborod, M.N.; Vaduganathan, M.; Neilan, T.G.; Lopez, T.; Dent, S.; Baldassarre, L.; Scherrer-Crosbie, M.; Barac, A.; et al. SGLT2 Inhibitor Use and Risk of Clinical Events in Patients with Cancer Therapy-Related Cardiac Dysfunction. JACC Heart Fail. 2024, 12, 67–78. [Google Scholar] [CrossRef]
- Quagliariello, V.; Bisceglia, I.; Berretta, M.; Iovine, M.; Canale, M.L.; Maurea, C.; Giordano, V.; Paccone, A.; Inno, A.; Maurea, N. PCSK9 Inhibitors in Cancer Patients Treated with Immune-Checkpoint Inhibitors to Reduce Cardiovascular Events: New Frontiers in Cardioncology. Cancers 2023, 15, 1397. [Google Scholar] [CrossRef]
- Ke, Q.; Shi, C.; Lv, Y.; Wang, L.; Luo, J.; Jiang, L.; Yang, J.; Zhou, Y. SGLT2 inhibitor counteracts NLRP3 inflammasome via tubular metabolite itaconate in fibrosis kidney. FASEB J. 2022, 36, e22078. [Google Scholar] [CrossRef]
- Kukreja, R.C.; Salloum, F.N.; Das, A. Cyclic guanosine monophosphate signaling and phosphodiesterase-5 inhibitors in cardioprotection. J. Am. Coll. Cardiol. 2012, 59, 1921–1927. [Google Scholar] [CrossRef]
- Francis, S.H. The role of cGMP-dependent protein kinase in controlling cardiomyocyte cGMP. Circ. Res. 2010, 107, 1164–1166. [Google Scholar] [CrossRef]
- Castro, L.R.; Verde, I.; Cooper, D.M.; Fischmeister, R. Cyclic guanosine monophosphate compartmentation in rat cardiac myocytes. Circulation 2006, 113, 2221–2228. [Google Scholar] [CrossRef] [PubMed]
- Kraehling, J.; Sessa, W.C. Contemporary Approaches to Modulating the Nitric Oxide-cGMP Pathway in Cardiovascular Disease. Circ. Res. 2017, 120, 1174–1182. [Google Scholar] [CrossRef] [PubMed]
- Leite-Moreira, A.M.; Almeida-Coelho, J.; Neves, J.S.; Castro-Ferreira, R.; Ladeiras-Lopes, R.; Leite-Moreira, A.F.; Lourenço, A.P. Myocardial stretch-induced compliance is abrogated under ischemic conditions and restored by cGMP/PKG-related pathways. Front. Physiol. 2023, 14, 1271698. [Google Scholar] [CrossRef]
- Klinger, J.R.; Chakinala, M.M.; Langleben, D.; Rosenkranz, S.; Sitbon, O. Riociguat: Clinical research and evolving role in therapy. Br. J. Clin. Pharmacol. 2021, 87, 2645–2662. [Google Scholar] [CrossRef] [PubMed]
- Numata, G.; Takimoto, E. Cyclic GMP and PKG Signaling in Heart Failure. Front. Pharmacol. 2022, 13, 792798. [Google Scholar] [CrossRef]
- Caminiti, G.; Sposato, B.; Volterrani, M. Chronic heart failure: The role of di vericiguat. Eur. Heart J. Suppl. 2023, 25 (Suppl. C), C316–C318. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.H.; Axell, A.; Turek, I.; Wright, B.; Meehan-Andrews, T.; Irving, H.R. Modulation of Inflammatory Cytokine Production in Human Monocytes by cGMP and IRAK3. Int. J. Mol. Sci. 2022, 23, 2552. [Google Scholar] [CrossRef] [PubMed]
- Liberale, L.; Ministrini, S.; Carbone, F.; Camici, G.G.; Montecucco, F. Cytokines as therapeutic targets for cardio- and cerebrovascular diseases. Basic Res. Cardiol. 2021, 116, 23. [Google Scholar] [CrossRef] [PubMed]
- Moone, L.; Jackson, C.E.; Adamson, C.; McConnachie, A.; Welsh, P.; Myles, R.C.; McMurray, J.J.V.; Jhund, P.S.; Petrie, M.C.; Lang, N.N. Adverse Outcomes Associated with Interleukin-6 in Patients Recently Hospitalized for Heart Failure with Preserved Ejection Fraction. Circ. Heart Fail. 2023, 16, e010051. [Google Scholar] [CrossRef]
- Qaisar, R.; Karim, A.; Muhammad, T.; Shah, I.; Khan, J. Prediction of sarcopenia using a battery of circulating biomarkers. Sci. Rep. 2021, 11, 8632. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Sáez De Asteasu, M.L.; Martínez-Velilla, N.; Zambon-Ferraresi, F.; García-Hermoso, A.; Recarey, A.E.; Fernández-Irigoyen, J.; Santamaría, E.; Palomino-Echeverría, S.; Izquierdo, M. Circulating Cytokines and Lower Body Muscle Performance in Older Adults at Hospital Admission. J. Nutr. Health Aging 2020, 24, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Ismaeel, A.; Kim, J.S.; Kirk, J.S.; Smith, R.S.; Bohannon, W.T.; Koutakis, P. Role of Transforming Growth Factor-β in Skeletal Muscle Fibrosis: A Review. Int. J. Mol. Sci. 2019, 20, 2446. [Google Scholar] [CrossRef] [PubMed]
- Rauchhaus, M.; Doehner, W.; Francis, D.P.; Davos, C.; Kemp, M.; Liebenthal, C.; Niebauer, J.; Hooper, J.; Volk, H.D.; Coats, A.J.; et al. Plasma cytokine parameters and mortality in patients with chronic heart failure. Circulation 2000, 102, 3060–3067. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Jiang, Y.; Qu, Y.; Lv, J.; Zeng, H. sGC agonist BAY1021189 promotes thoracic aortic dissection formation by accelerating vascular smooth muscle cell phenotype switch. Eur. J. Pharmacol. 2023, 952, 175789. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quagliariello, V.; Berretta, M.; Bisceglia, I.; Giacobbe, I.; Iovine, M.; Giordano, V.; Arianna, R.; Barbato, M.; Izzo, F.; Maurea, C.; et al. The sGCa Vericiguat Exhibit Cardioprotective and Anti-Sarcopenic Effects through NLRP-3 Pathways: Potential Benefits for Anthracycline-Treated Cancer Patients. Cancers 2024, 16, 1487. https://doi.org/10.3390/cancers16081487
Quagliariello V, Berretta M, Bisceglia I, Giacobbe I, Iovine M, Giordano V, Arianna R, Barbato M, Izzo F, Maurea C, et al. The sGCa Vericiguat Exhibit Cardioprotective and Anti-Sarcopenic Effects through NLRP-3 Pathways: Potential Benefits for Anthracycline-Treated Cancer Patients. Cancers. 2024; 16(8):1487. https://doi.org/10.3390/cancers16081487
Chicago/Turabian StyleQuagliariello, Vincenzo, Massimiliano Berretta, Irma Bisceglia, Ilaria Giacobbe, Martina Iovine, Vienna Giordano, Raffaele Arianna, Matteo Barbato, Francesca Izzo, Carlo Maurea, and et al. 2024. "The sGCa Vericiguat Exhibit Cardioprotective and Anti-Sarcopenic Effects through NLRP-3 Pathways: Potential Benefits for Anthracycline-Treated Cancer Patients" Cancers 16, no. 8: 1487. https://doi.org/10.3390/cancers16081487
APA StyleQuagliariello, V., Berretta, M., Bisceglia, I., Giacobbe, I., Iovine, M., Giordano, V., Arianna, R., Barbato, M., Izzo, F., Maurea, C., Canale, M. L., Paccone, A., Inno, A., Scherillo, M., Gabrielli, D., & Maurea, N. (2024). The sGCa Vericiguat Exhibit Cardioprotective and Anti-Sarcopenic Effects through NLRP-3 Pathways: Potential Benefits for Anthracycline-Treated Cancer Patients. Cancers, 16(8), 1487. https://doi.org/10.3390/cancers16081487