
Peritoneal Flap Following Lymph Node Dissection in Robotic Radical Prostatectomy: A Novel “Bunching” Technique



 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Endpoints
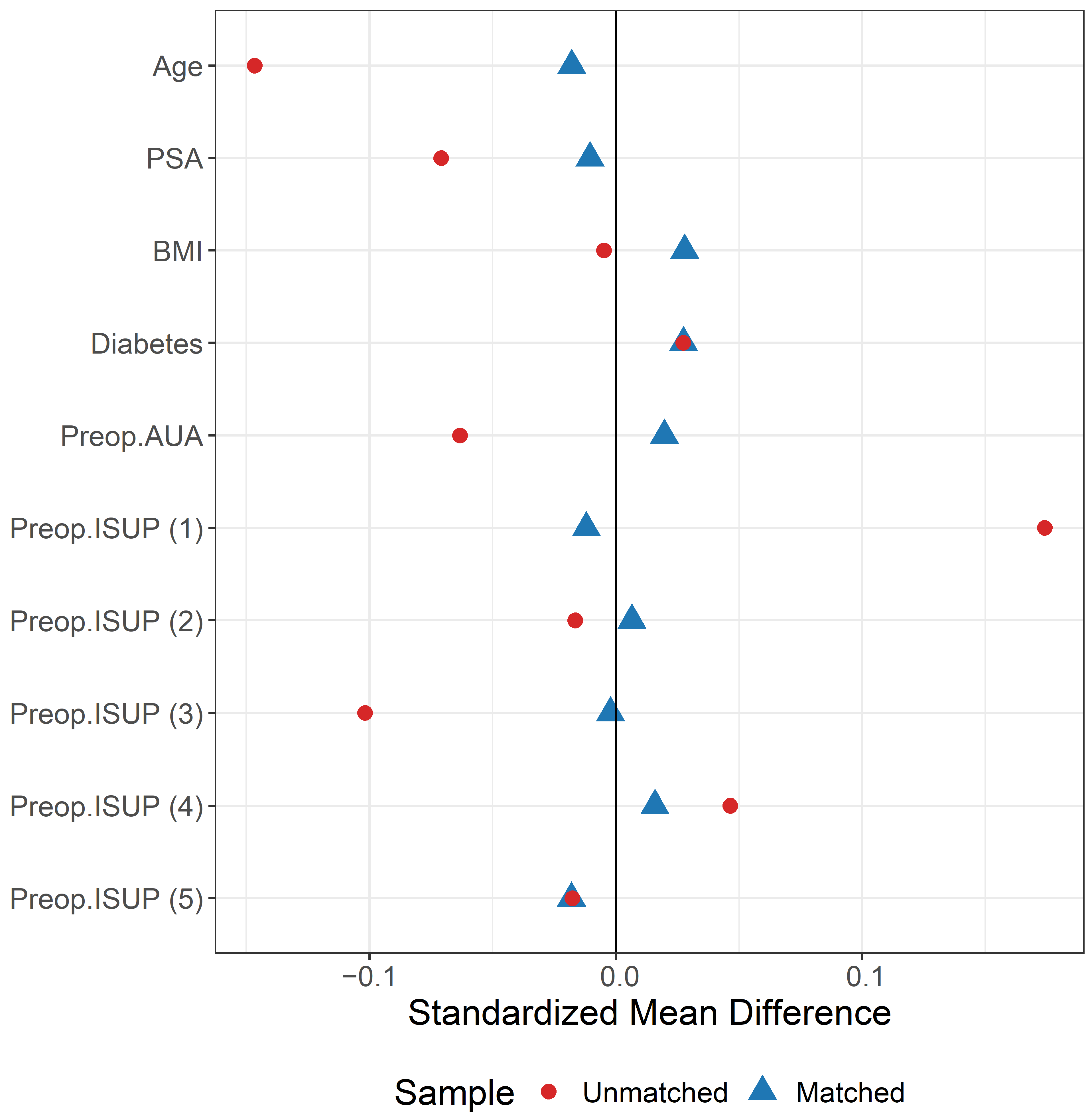
2.3. Propensity Score Matching
2.4. Statistical Analysis
2.4.1. Surgical Technique
2.4.2. Peritoneal Bladder Flap Bunching Technique (PBFB)
3. Results
3.1. Patient Demography
3.2. Intraoperative Parameters
3.3. Postoperative Parameters and Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanda, M.G.; Cadeddu, J.A.; Kirkby, E.; Chen, R.C.; Crispino, T.; Fontanarosa, J.; Freedland, S.J.; Greene, K.; Klotz, L.H.; Makarov, D.V.; et al. Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline. Part I: Risk Stratification, Shared Decision Making, and Care Options. J. Urol. 2018, 199, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Briganti, A.; Blute, M.L.; Eastham, J.H.; Graefen, M.; Heidenreich, A.; Karnes, J.R.; Montorsi, F.; Studer, U.E. Pelvic Lymph Node Dissection in Prostate Cancer. Eur. Urol. 2009, 55, 1251–1265. [Google Scholar] [CrossRef] [PubMed]
- Touijer, K.A.; Ahallal, Y.; Guillonneau, B.D. Indications for and anatomical extent of pelvic lymph node dissection for prostate cancer: Practice patterns of uro-oncologists in North America. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 1517–1521.e2. [Google Scholar] [CrossRef] [PubMed]
- Lestingi, J.F.; Guglielmetti, G.B.; Trinh, Q.D.; Coelho, R.F.; Pontes, J., Jr.; Bastos, D.A.; Cordeiro, M.D.; Sarkis, A.S.; Faraj, S.F.; Mitre, A.I.; et al. Extended Versus Limited Pelvic Lymph Node Dissection During Radical Prostatectomy for Intermediate- and High-risk Prostate Cancer: Early Oncological Outcomes from a Randomized Phase 3 Trial. Eur. Urol. 2021, 79, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Orvieto, M.A.; Coelho, R.F.; Chauhan, S.; Palmer, K.J.; Rocco, B.; Patel, V.R. Incidence of lymphoceles after robot-assisted pelvic lymph node dissection: Lymphocele Formation after Plnd. BJU Int. 2011, 108, 1185–1189. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Briganti, A.; De La Taille, A.; Haese, A.; Heidenreich, A.; Menon, M.; Sulser, T.; Tewari, A.K.; Eastham, J.A. Pelvic Lymph Node Dissection During Robot-assisted Radical Prostatectomy: Efficacy, Limitations, and Complications—A Systematic Review of the Literature. Eur. Urol. 2014, 65, 7–16. [Google Scholar] [CrossRef]
- Zorn, K.C.; Katz, M.H.; Bernstein, A.; Shikanov, S.A.; Brendler, C.B.; Zagaja, G.P.; Shalhav, A.L. Pelvic Lymphadenectomy During Robot-assisted Radical Prostatectomy: Assessing Nodal Yield, Perioperative Outcomes, and Complications. Urology 2009, 74, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Liss, M.A.; Palazzi, K.; Stroup, S.P.; Jabaji, R.; Raheem, O.A.; Kane, C.J. Outcomes and complications of pelvic lymph node dissection during robotic-assisted radical prostatectomy. World J. Urol. 2013, 31, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Stolzenburg, J.U.; Kyriazis, I.; Liatsikos, E. Postoperative Lymphocele Formation after Pelvic Lymph Node Dissection at the Time of Radical Prostatectomy Should Not Be Considered an Inevitable Consequence of the Approach. Eur. Urol. 2017, 71, 159–160. [Google Scholar] [CrossRef]
- Mattei, A.; Grande, P.; Di Pierro, G.B. Reply from Authors re: Jens Uwe Stolzenburg, Iason Kyriazis, Evangelos Liatsikos. Postoperative Lymphocele Formation after Pelvic Lymph Node Dissection at the Time of Radical Prostatectomy Should Not Be Considered an Inevitable Consequence of the Approach. Eur Urol 2017, 71, 159–160: Which Lymphatic Vessels Have To Be Secured During Pelvic Lymph Node Dissection for Prostate Cancer? Eur. Urol. 2017, 71, 161. [Google Scholar] [CrossRef]
- Buelens, S.; Van Praet, C.; Poelaert, F.; Van Huele, A.; Decaestecker, K.; Lumen, N. Prospective Randomized Controlled Trial Exploring the Effect of TachoSil on Lymphocele Formation After Extended Pelvic Lymph Node Dissection in Prostate Cancer. Urology 2018, 118, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Garayev, A.; Aytaç, Ö.; Tavukcu, H.H.; Atug, F. Effect of Autologous Fibrin Glue on Lymphatic Drainage and Lymphocele Formation in Extended Bilateral Pelvic Lymphadenectomy in Robot-Assisted Radical Prostatectomy. J. Endourol. 2019, 33, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Waldert, M.; Remzi, M.; Klatte, T.; Klingler, H.C. Floseal Reduces the Incidence of Lymphoceles After Lymphadenectomies in Laparoscopic and Robot-Assisted Extraperitoneal Radical Prostatectomy. J. Endourol. 2011, 25, 969–973. [Google Scholar] [CrossRef] [PubMed]
- Stolzenburg, J.U.; Arthanareeswaran, V.K.; Dietel, A.; Franz, T.; Liatsikos, E.; Kyriazis, I.; Ganzer, R.; Yaney, K.; Do, H.M. Four-point Peritoneal Flap Fixation in Preventing Lymphocele Formation Following Radical Prostatectomy. Eur. Urol. Oncol. 2018, 1, 443–448. [Google Scholar] [CrossRef]
- Lebeis, C.; Canes, D.; Sorcini, A.; Moinzadeh, A. Novel Technique Prevents Lymphoceles After Transperitoneal Robotic-assisted Pelvic Lymph Node Dissection: Peritoneal Flap Interposition. Urology 2015, 85, 1505–1509. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Lee, Z.; Eun, D.D. Utilization of a Peritoneal Interposition Flap to Prevent Symptomatic Lymphoceles After Robotic Radical Prostatectomy and Bilateral Pelvic Lymph Node Dissection. J. Endourol. 2020, 34, 821–827. [Google Scholar] [CrossRef]
- Stolzenburg, J.U.; Wasserscheid, J.; Rabenalt, R.; Do, M.; Schwalenberg, T.; McNeill, A.; Constantinides, C.; Kallidonis, P.; Ganzer, R.; Liatsikos, E. Reduction in incidence of lymphocele following extraperitoneal radical prostatectomy and pelvic lymph node dissection by bilateral peritoneal fenestration. World J. Urol. 2008, 26, 581–586. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A New Proposal With Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef]
- Greifer, N. Cobalt: Covariate Balance Tables and Plots. R Package Version 4.5.5. 2024. Available online: https://cran.r-project.org/web/packages/cobalt/index.html (accessed on 14 April 2024).
- Bhat, K.R.; Moschovas, M.C.; Onol, F.F.; Rogers, T.; Reddy, S.S.; Corder, C.; Roof, S.; Patel, V.R. Evidence-based evolution of our robot-assisted laparoscopic prostatectomy (RALP) technique through 13,000 cases. J. Robot. Surg. 2021, 15, 651–660. [Google Scholar] [CrossRef]
- Moschovas, M.C.; Patel, V. Nerve-sparing robotic-assisted radical prostatectomy: How I do it after 15.000 cases. Int. Braz. J. Urol. 2022, 48, 369–370. [Google Scholar] [CrossRef] [PubMed]
- Moschovas, M.C.; Bhat, S.; Onol, F.F.; Rogers, T.; Roof, S.; Mazzone, E.; Mottrie, A.; Patel, V. Modified Apical Dissection and Lateral Prostatic Fascia Preservation Improves Early Postoperative Functional Recovery in Robotic-assisted Laparoscopic Radical Prostatectomy: Results from a Propensity Score–matched Analysis. Eur. Urol. 2020, 78, 875–884. [Google Scholar] [CrossRef] [PubMed]
- American Joint Committee on Cancer. AJCC Cancer Staging Manual; Greene, F.L., Page, D.L., Fleming, I.D., April, G., Fritz, C.T.R., Balch, C.M., Haller, D.G., Morrow, M., Eds.; Springer: New York, NY, USA, 2002. [Google Scholar] [CrossRef]
- Seetharam Bhat, K.R.; Moschovas, M.C.; Sandri, M.; Reddy, S.; Onol, F.F.; Noel, J.; Rogers, T.; Schatloff, O.; Coelho, R.; Ko, Y.H.; et al. Stratification of Potency Outcomes Following Robot-Assisted Laparoscopic Radical Prostatectomy Based on Age, Preoperative Potency, and Nerve Sparing. J. Endourol. 2021, 35, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Gloger, S.; Ubrig, B.; Boy, A.; Leyh-Bannurah, S.R.; Siemer, S.; Arndt, M.; Stolzenburg, J.U.; Franz, T.; Oelke, M.; Witt, J.H. Bilateral Peritoneal Flaps Reduce Incidence and Complications of Lymphoceles after Robotic Radical Prostatectomy with Pelvic Lymph Node Dissection—Results of the Prospective Randomized Multicenter Trial ProLy. J. Urol. 2022, 208, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, S.; Hadaschik, B.; Lebentrau, S.; Ubrig, B.; Burger, M.; May, M. Clinical Importance of a Peritoneal Interposition Flap to Prevent Symptomatic Lymphoceles after Robot-Assisted Radical Prostatectomy and Pelvic Lymph Node Dissection: A Systematic Review and Meta-Analysis. Urol. Int. 2022, 106, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Bründl, J.; Lenart, S.; Stojanoski, G.; Gilfrich, C.; Rosenhammer, B.; Stolzlechner, M.; Ponholzer, A.; Dreissig, C.; Weikert, S.; Burger, M.; et al. Peritoneal Flap in Robot-Assisted Radical Prostatectomy. Dtsch. Ärztebl. Int. 2020, 117, 243. [Google Scholar] [CrossRef]
- Neuberger, M.; Kowalewski, K.F.; Simon, V.; von Hardenberg, J.; Siegel, F.; Wessels, F.; Worst, T.S.; Michel, M.S.; Westhoff, N.; Kriegmair, M.C.; et al. Peritoneal Flap for Lymphocele Prophylaxis Following Robotic-assisted Radical Prostatectomy with Lymph Node Dissection: The Randomised Controlled Phase 3 PELYCAN Trial. Eur. Urol. Oncol. 2024, 7, 53–62. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Flap (n = 567) | Control (n = 1700) | p | Standardized Mean Difference after 1:3 PS Matching |
|---|---|---|---|---|
| Age (years) | 65 (60–70) | 65 (60–70) | 1.0 | −0.18 |
| PSA (ng/mL) | 6.4 (4.8–9.6) | 6.5 (4.8–9.5) | 0.9 | −0.015 |
| BMI (Kg/m2) | 27.8 (25.4–30.9) | 28.1 (25.5–30.9) | 0.8 | 0.028 |
| Diabetes (n, %) | 0.6 | |||
| No | 479 (84.5) | 1419 (83.5) | −0.028 | |
| Yes | 88 (15.5) | 281(16.5) | 0.028 | |
| Charlson Comorbidity Index (n, %) | 0.16 | |||
| 0 | 14 (2.5) | 26 (1.4) | ||
| 1–2 | 335 (59) | 963 (56.7) | ||
| 3–4 | 200 (35.3) | 635 (37.4) | ||
| >4 | 18 (3.2) | 76 (4.5) | ||
| Preoperative AUA | 8 | 8 | 1 | 0.02 |
| (4–15) | (4–15) | |||
| Biopsy ISUP Grade (n, %) | 0.9 | |||
| Group 1 | 23 (4.1) | 65 (3.8) | –0.012 | |
| Group 2 | 214 (37.7) | 647 (38.1) | 0.007 | |
| Group 3 | 166 (29.3) | 496 (29.2) | 0.002 | |
| Group 4 | 96 (16.9) | 298 (17.5) | –0.016 | |
| Group 5 | 68 (12) | 194 (11.4) | –0.018 |
| Parameters | Flap (n = 567) | Control (n = 4070) | p |
|---|---|---|---|
| Age (years) | 65 (60–70) | 65 (59–69) | 0.01 |
| PSA (ng/mL) | 6.4 (4.8–9.6) | 6.3 (4.6–9.3) | 0.2 |
| BMI (Kg/m2) | 27.8 (25.4–30.9) | 27.9 (25.5–30.8) | 0.8 |
| Diabetes (n, %) | 0.5 | ||
| No | 479 (84.5) | 3400 (83.5) | |
| Yes | 88 (15.5) | 670(16.5) | |
| Charlson Comorbidity Index (n, %) | 0.9 | ||
| 0 | 14 (2.5) | 107 (2.6) | |
| 1–2 | 335 (59) | 2394 (58.8) | |
| 3–4 | 200 (35.3) | 1407 (34.6) | |
| >4 | 18 (3.2) | 162 (4) | |
| Preoperative AUA | 8 | 8 | 0.1 |
| (4–15) | (4–14) | ||
| Biopsy ISUP Grade (n, %) | 0.002 | ||
| Group 1 | 23 (4.1) | 335 (8.2) | |
| Group 2 | 214 (37.7) | 1502 (36.9) | |
| Group 3 | 166 (29.3) | 1022 (25.1) | |
| Group 4 | 96 (16.9) | 747 (18.4) | |
| Group 5 | 68 (12) | 464 (11.4) |
| Parameters | Flap (n = 567) | Control (n = 1700) | p |
|---|---|---|---|
| EBL (mL) | 100 (100–200) | 100 (100–150) | <0.001 <0.001 |
| EBL < 100 mL (n, %) | 323 (57) | 1232 (72.5) | |
| EBL ≥ 100 mL (n, %) | 244 (43) | 468 (27.5) | |
| Console Time (min) | 80 (80–90) | 80 (75–90) | <0.001 <0.001 |
| <80 (n, %) | 58 (10.3) | 495 (29.3) | |
| 80–89 | 275 (48.7) | 642 (38) | |
| ≥90 | 232 (41) | 552 (32.7) | |
| Hospitalization (n, %) | 0.5 | ||
| ≤1 day | 548 (96.7) | 1631 (95.9) | |
| >1 day | 19 (3.3) | 69 (4.1) | |
| Postoperative Complications | 0.1 | ||
| (Clavien–Dindo) (n, %) | |||
| 2 | 22 (3.9) | 27 (1.5) | |
| ≥3 | 20 (3.5) | 48 (2.8) | |
| Pathological Stage (n, %) | 0.7s71 | ||
| pT2 | 267 (47.2) | 815 (47.9) | |
| ≥pT3a | 299 (52.8) | 885 (52.1) | |
| Total Number of LN | 3 (2–5) | 3 (2–5) | 0.001 |
| Total Number of LN (n, %) | 0.001 | ||
| 0 | 0 | 19 (1.1) | |
| 1–3 | 328 (57.9) | 832 (50) | |
| >3 | 239 (42.1) | 849 (49.9) | |
| Post-op Lymphocele (n, %) | |||
| No | 431 (76) | 1344 (79.1) | 0.14 |
| Yes | 136 (24) | 356 (20.9) | |
| ≤5 cm | 124 (21.9) | 167 (9.8) | |
| >5 cm | 12 (2.1) | 189 (11.1) | 0.001 |
| Symptomatic Lymphocele (n, %) | 0.001 | ||
| No | 567 (100) | 1663 (97.8) | |
| Yes | 0 (0) | 37 (2.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gamal, A.; Moschovas, M.C.; Jaber, A.R.; Saikali, S.; Sandri, M.; Patel, E.; Patel, E.; Rogers, T.; Patel, V. Peritoneal Flap Following Lymph Node Dissection in Robotic Radical Prostatectomy: A Novel “Bunching” Technique. Cancers 2024, 16, 1547. https://doi.org/10.3390/cancers16081547
Gamal A, Moschovas MC, Jaber AR, Saikali S, Sandri M, Patel E, Patel E, Rogers T, Patel V. Peritoneal Flap Following Lymph Node Dissection in Robotic Radical Prostatectomy: A Novel “Bunching” Technique. Cancers. 2024; 16(8):1547. https://doi.org/10.3390/cancers16081547
Chicago/Turabian StyleGamal, Ahmed, Marcio Covas Moschovas, Abdel Rahman Jaber, Shady Saikali, Marco Sandri, Ela Patel, Evan Patel, Travis Rogers, and Vipul Patel. 2024. "Peritoneal Flap Following Lymph Node Dissection in Robotic Radical Prostatectomy: A Novel “Bunching” Technique" Cancers 16, no. 8: 1547. https://doi.org/10.3390/cancers16081547
APA StyleGamal, A., Moschovas, M. C., Jaber, A. R., Saikali, S., Sandri, M., Patel, E., Patel, E., Rogers, T., & Patel, V. (2024). Peritoneal Flap Following Lymph Node Dissection in Robotic Radical Prostatectomy: A Novel “Bunching” Technique. Cancers, 16(8), 1547. https://doi.org/10.3390/cancers16081547