
FDG-PET Response Prediction in Pediatric Hodgkin’s Lymphoma: Impact of Metabolically Defined Tumor Volumes and Individualized SUV Measurements on the Positive Predictive Value

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients

{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Patients (n = 54) |
|---|---|
| Sex Male | 33 |
| Female | 21 |
| Age mean (years) | 14.6 |
| range (years) | 5.9–17.8 |
| Histology | |
| Nodular sclerosis (n) | 38 |
| Mixed cellularity (n) | 13 |
| Lymphocyte rich (n) | 2 |
| no final subtype (n) | 1 |
| Stage | |
| I (n) | 3 |
| II (n) | 26 |
| III (n) | 12 |
| IV (n) | 13 |
| Extra-nodal disease | 20 |
| Therapy groups | |
| TG1 (n) | 17 |
| TG2 (n) | 13 |
| TG3 (n) | 24 |
| Follow-up (months) | 65 |
| Range (months) | 27–112 |
| Recurrences | 6 |
2.2. PET: Acquisition
2.3. Image Reconstruction
2.4. Image Analysis
2.4.1. Visual Analysis
2.4.2. Semi-Quantitative Analysis
2.5. Standard of Reference
2.6. Sample Size Estimation
2.7. Statistical Analysis
3. Results
3.1. Visual Assessment
3.2. Semi-Quantitative Assessment—Response Prediction Using PET1
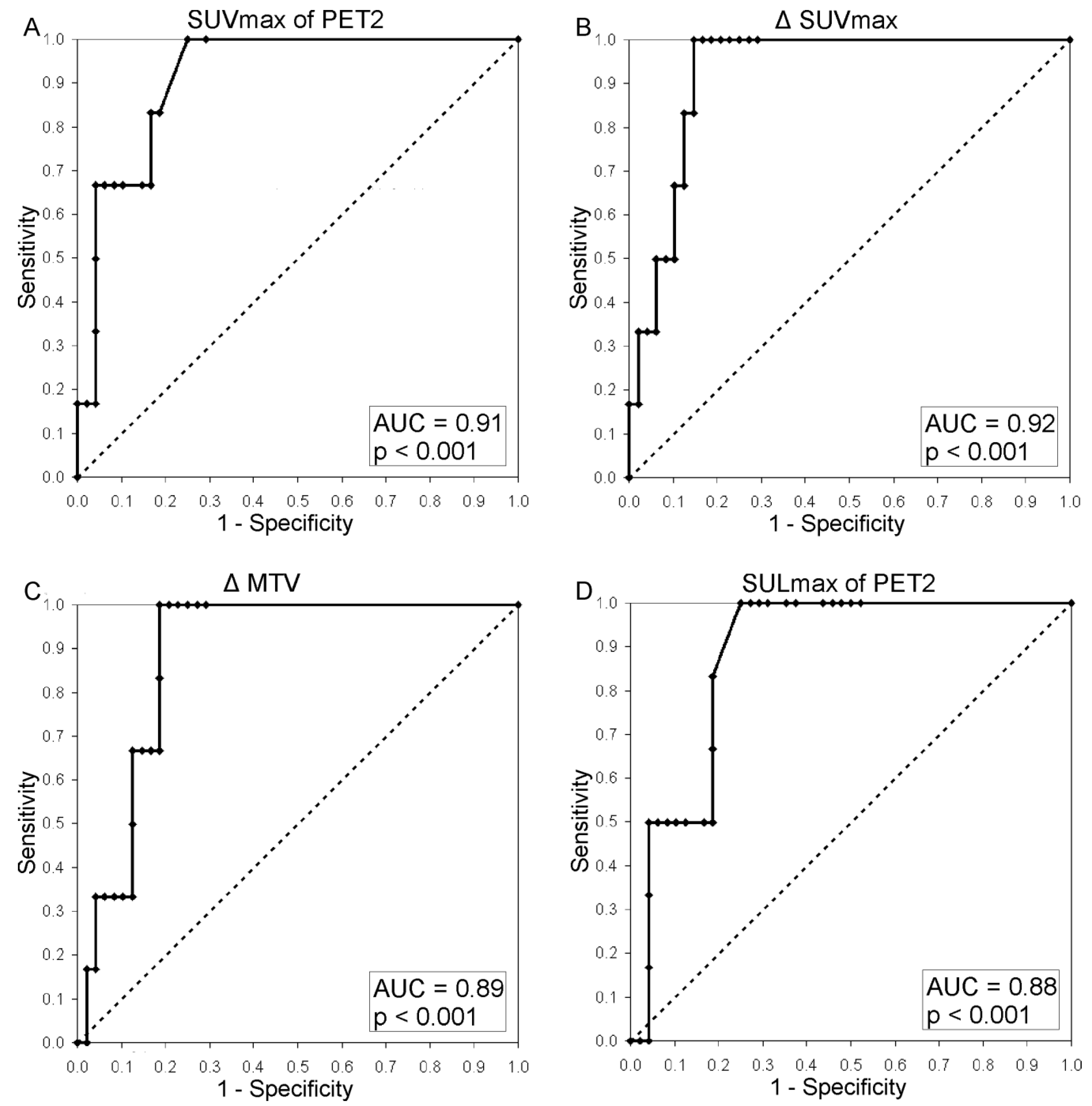
3.3. Semi-Quantitative Assessment—Response Prediction Using PET2
3.4. Semi-Quantitative Assessment—Response Prediction Using Δ-Analyses (PET1-PET2)
| Visual Assessment | No. | AUC | 95% CI (%) | p Value | Cut-off (Absolute) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | TP | TN | FP | FN | Accuracy (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 54 | 0.69 | 0.47 | 0.044 (n.s.) | 66.7 | 70.8 | 22.2 | 94.4 | 4 | 34 | 14 | 2 | 70.4 | |||
| SUV | SUVmax2 | 54 | 0.91 | 0.83–1 | <0.0001 | >2.5 | 100 | 75.0 | 33.3 | 100 | 6 | 36 | 12 | 0 | 77.8 |
| SUVmean2 | 54 | 0.90 | 0.80–0.99 | <0.0001 | >2.5 | 100 | 75.0 | 33.3 | 100 | 6 | 36 | 12 | 0 | 77.8 | |
| MTV2 | 54 | 0.90 | 0.80–1 | <0.0001 | >0 mL | 100 | 70.8 | 30.0 | 100 | 6 | 34 | 14 | 0 | 74.1 | |
| TLGmean2 | 54 | 0.90 | 0.81–1 | <0.0001 | >0.3 g | 100 | 75.0 | 33.3 | 100 | 6 | 36 | 12 | 0 | 77.8 | |
| ΔSUV | ΔSUVmax | 54 | 0.92 | 0.85–1 | <0.0001 | <78.0% | 100 | 85.4 | 46.2 | 100 | 6 | 41 | 7 | 0 | 87.0 |
| ΔSUVmean | 54 | 0.90 | 0.81–0.98 | <0.0001 | <48.0% | 100 | 81.3 | 40.0 | 100 | 6 | 39 | 9 | 0 | 83.3 | |
| ΔMTV | 54 | 0.89 | 0.79–0.98 | <0.0001 | <99.9% | 100 | 81.3 | 40.0 | 100 | 6 | 39 | 9 | 0 | 83.3 | |
| ΔTLGmean | 54 | 0.90 | 0.81–0.99 | <0.0001 | <99.95% | 100 | 81.3 | 40.0 | 100 | 6 | 39 | 9 | 0 | 83.3 | |
| SUL | SULmax2 | 54 | 0.88 | 0.78–0.98 | <0.0001 | >2.1 | 100 | 75.0 | 33.3 | 100 | 6 | 36 | 12 | 0 | 77.8 |
| SULmean2 | 54 | 0.86 | 0.76–0.97 | <0.0001 | >1.8 | 83.3 | 85.4 | 41.7 | 97.6 | 5 | 41 | 7 | 1 | 85.2 | |
| MTV2_liver_cor. | 54 | 0.81 | 0.65–0.98 | <0.0001 | >4.1 mL | 83.3 | 77.1 | 31.3 | 97.4 | 5 | 37 | 11 | 1 | 77.8 | |
| TLGmean2_liver_cor. | 54 | 0.83 | 0.67–0.99 | <0.0001 | >0 g | 100 | 47.9 | 19.4 | 100 | 6 | 23 | 25 | 0 | 53.7 | |
| ΔSUL | ΔSULmax | 54 | 0.86 | 0.75–0.98 | <0.0001 | <83.3% | 100 | 66.7 | 27.3 | 100 | 6 | 32 | 16 | 0 | 70.4 |
| ΔSULmean | 54 | 0.84 | 0.73–0.95 | <0.0001 | <45.2% | 100 | 75.0 | 33.3 | 100 | 6 | 36 | 12 | 1 | 77.8 | |
| ΔMTV_liver_cor. | 54 | 0.79 | 0.63–0.95 | 0,0002 | <99.9% | 100 | 56.3 | 22.2 | 100 | 6 | 27 | 21 | 0 | 61.1 | |
| ΔTLGmean_liver_cor. | 54 | 0.79 | 0.62–0.95 | <0.0003 | <99.93 | 100 | 56.3 | 22.2 | 100 | 6 | 27 | 21 | 0 | 61.1 | |



4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Gallamini, A.; Hutchings, M.; Rigacci, L.; Specht, L.; Merli, F.; Hansen, M.; Patti, C.; Loft, A.; di Raimondo, F.; DʼAmore, F.; et al. Early interim 2-[18F]fluoro-2-deoxy-D-glucose positron emission tomography is prognostically superior to international prognostic score in advanced-stage Hodgkinʼs lymphoma: A report from a joint Italian-Danish study. J. Clin. Oncol. 2007, 25, 3746–3752. [Google Scholar] [PubMed]
- Hutchings, M.; Loft, A.; Hansen, M.; Pedersen, L.M.; Buhl, T.; Jurlander, J.; Buus, S.; Keiding, S.; DʼAmore, F.; Boesen, A.M.; et al. FDG-PET after two cycles of chemotherapy predicts treatment failure and progression-free survival in Hodgkin lymphoma. Blood 2006, 107, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Kobe, C.; Dietlein, M.; Franklin, J.; Markova, J.; Lohri, A.; Amthauer, H.; Klutmann, S.; Knapp, W.H.; Zijlstra, J.M.; Bockisch, A.; et al. Positron emission tomography has a high negative predictive value for progression or early relapse for patients with residual disease after first-line chemotherapy in advanced-stage Hodgkin lymphoma. Blood 2008, 112, 3989–3994. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised response criteria for malignant lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Juweid, M.E.; Wiseman, G.A.; Vose, J.M.; Ritchie, J.M.; Menda, Y.; Wooldridge, J.E.; Mottaghy, F.M.; Rohren, E.M.; Blumstein, N.M.; Stolpen, A.; et al. Response assessment of aggressive non-Hodgkinʼs lymphoma by integrated International Workshop Criteria and fluorine-18-fluorodeoxyglucose positron emission tomography. J. Clin. Oncol. 2005, 23, 4652–4661. [Google Scholar] [CrossRef] [PubMed]
- Furth, C.; Meseck, R.M.; Steffen, I.G.; Schoenberger, S.; Denecke, T.; Henze, G.; Hautzel, H.; Hofheinz, F.; Grosser, O.; Hundsdoerfer, P.; et al. SUV-measurements and patient-specific corrections in pediatric Hodgkin-lymphoma: Is there a benefit for PPV in early response assessment by FDG-PET? Pediatr. Blood Cancer 2012, 59, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Furth, C.; Amthauer, H.; Hautzel, H.; Steffen, I.G.; Ruf, J.; Schiefer, J.; Schonberger, S.; Henze, G.; Grandt, R.; Hundsdoerfer, P.; et al. Evaluation of interim PET response criteria in paediatric Hodgkinʼs lymphoma—Results for dedicated assessment criteria in a blinded dual-centre read. Ann. Oncol. 2011, 22, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Furth, C.; Steffen, I.G.; Amthauer, H.; Ruf, J.; Misch, D.; Schonberger, S.; Kobe, C.; Denecke, T.; Stover, B.; Hautzel, H.; et al. Early and late therapy response assessment with [18F]fluorodeoxyglucose positron emission tomography in pediatric Hodgkinʼs lymphoma: Analysis of a prospective multicenter trial. J. Clin. Oncol. 2009, 27, 4385–4391. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, M.M.; Delbeke, D.; Whitlock, J.A.; Martin, W.; Kuttesch, J.F.; Frangoul, H.A.; Shankar, S. Utility of FDG-PET/CT in follow-up of children treated for Hodgkin and non-Hodgkin lymphoma. J. Pediatr. Hematol. Oncol. 2006, 28, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Francis, R.J.; Byrne, M.J.; van der Schaaf, A.A.; Boucek, J.A.; Nowak, A.K.; Phillips, M.; Price, R.; Patrikeos, A.P.; Musk, A.W.; Millward, M.J. Early prediction of response to chemotherapy and survival in malignant pleural mesothelioma using a novel semiautomated 3-dimensional volume-based analysis of serial 18F-FDG PET scans. J. Nucl. Med. 2007, 48, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Hyun, S.H.; Choi, J.Y.; Shim, Y.M.; Kim, K.; Lee, S.J.; Cho, Y.S.; Lee, J.Y.; Lee, K.H.; Kim, B.T. Prognostic value of metabolic tumor volume measured by 18F-fluorodeoxyglucose positron emission tomography in patients with esophageal carcinoma. Ann. Surg. Oncol. 2010, 17, 115–122. [Google Scholar] [CrossRef]
- Berkowitz, A.; Basu, S.; Srinivas, S.; Sankaran, S.; Schuster, S.; Alavi, A. Determination of whole-body metabolic burden as a quantitative measure of disease activity in lymphoma: A novel approach with fluorodeoxyglucose-PET. Nucl. Med. Commun. 2008, 29, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Krak, N.C.; Boellaard, R.; Hoekstra, O.S.; Twisk, J.W.; Hoekstra, C.J.; Lammertsma, A.A. Effects of ROI definition and reconstruction method on quantitative outcome and applicability in a response monitoring trial. Eur. J. Nucl. Med. Mol. Imag. 2005, 32, 294–301. [Google Scholar] [CrossRef]
- Minn, H.; Zasadny, K.R.; Quint, L.E.; Wahl, R.L. Lung cancer: Reproducibility of quantitative measurements for evaluating 2-[F-18]-fluoro-2-deoxy-d-glucose uptake at PET. Radiology 1995, 196, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Nahmias, C.; Wahl, L.M. Reproducibility of standardized uptake value measurements determined by 18F-FDG PET in malignant tumors. J. Nucl. Med. 2008, 49, 1804–1808. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, Y.; Zasadny, K.R.; Minn, H.; Wahl, R.L. Reproducibility of common semi-quantitative parameters for evaluating lung cancer glucose metabolism with positron emission tomography using 2-deoxy-2-[18F]fluoro-d-glucose. Mol. Imag. Biol. 2002, 4, 171–178. [Google Scholar] [CrossRef]
- Weber, W.A.; Ziegler, S.I.; Thodtmann, R.; Hanauske, A.R.; Schwaiger, M. Reproducibility of metabolic measurements in malignant tumors using FDG PET. J. Nucl. Med. 1999, 40, 1771–1777. [Google Scholar] [PubMed]
- Shankar, L.K.; Hoffman, J.M.; Bacharach, S.; Graham, M.M.; Karp, J.; Lammertsma, A.A.; Larson, S.; Mankoff, D.A.; Siegel, B.A.; van den Abbeele, A.; et al. Consensus recommendations for the use of 18F-FDG PET as an indicator of therapeutic response in patients in National Cancer Institute Trials. J. Nucl. Med. 2006, 47, 1059–1066. [Google Scholar] [PubMed]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving considerations for PET response criteria in solid tumors. J. Nucl. Med. 2009, 50, 122S–150S. [Google Scholar] [CrossRef] [PubMed]
- Zasadny, K.R.; Wahl, R.L. Standardized uptake values of normal tissues at PET with 2-[fluorine-18]-fluoro-2-deoxy-D-glucose: Variations with body weight and a method for correction. Radiology 1993, 189, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Paquet, N.; Albert, A.; Foidart, J.; Hustinx, R. Within-patient variability of (18)F-FDG: Standardized uptake values in normal tissues. J. Nucl. Med. 2004, 45, 784–788. [Google Scholar] [PubMed]
- Meignan, M.; Itti, E.; Gallamini, A.; Haioun, C. Interim 18F-fluorodeoxyglucose positron emission tomography in diffuse large B-cell lymphoma: Qualitative or quantitative interpretation—Where do we stand? Leuk. Lymphoma 2009, 50, 1753–1756. [Google Scholar] [CrossRef] [PubMed]
- UICC. International Union Against Cancer TNM Classification of Malignant Tumours; John Wiley & Sons: New York, NY, USA, 2012. [Google Scholar]
- National Cancer Institute at National Instutes of Health. Combination Chemotherapy in Treating Young Patients with Hodgkinʼs Lymphoma, Clinical Trials (PDQ®); National Cancer Institute at National Instutes of Health: Bethesda, MD, USA, 2007. [Google Scholar]
- Dorffel, W.; Luders, H.; Ruhl, U.; Albrecht, M.; Marciniak, H.; Parwaresch, R.; Potter, R.; Schellong, G.; Schwarze, E.W.; Wickmann, L. Preliminary results of the multicenter trial GPOH-HD 95 for the treatment of Hodgkinʼs disease in children and adolescents: Analysis and outlook. Klin. Padiatr. 2003, 215, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Kluge, R.; Korholz, D. Role of FDG-PET in staging and therapy of children with Hodgkin lymphoma. Klin. Padiatr. 2011, 223, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Korholz, D.; Kluge, R.; Wickmann, L.; Hirsch, W.; Luders, H.; Lotz, I.; Dannenberg, C.; Hasenclever, D.; Dorffel, W.; Sabri, O. Importance of F18-fluorodeoxy-D-2-glucose positron emission tomography (FDG-PET) for staging and therapy control of Hodgkinʼs lymphoma in childhood and adolescence—Consequences for the GPOH-HD 2003 protocol. Onkologie 2003, 26, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Korholz, D.; Claviez, A.; Hasenclever, D.; Kluge, R.; Hirsch, W.; Kamprad, F.; Dorffel, W.; Wickmann, L.; Papsdorf, K.; Dieckmann, K.; et al. The concept of the GPOH-HD 2003 therapy study for pediatric Hodgkinʼs disease: Evolution in the tradition of the DAL/GPOH studies. Klin. Padiatr. 2004, 216, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Furth, C.; Denecke, T.; Steffen, I.; Ruf, J.; Voelker, T.; Misch, D.; Vondran, F.; Plotkin, M.; Stover, B.; Henze, G.; et al. Correlative imaging strategies implementing CT, MRI, and PET for staging of childhood Hodgkin disease. J. Pediatr. Hematol. Oncol. 2006, 28, 501–512. [Google Scholar] [CrossRef] [PubMed]
- De Long, E.R.; de Long, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Hautzel, H.; Hussien, A.E.M.; Furth, C. AUC-analyses of PET1-based parameters. Department of Nuclear Medicine (KME), ForschungszentrumJülich, Medical Faculty, Heinrich-Heine-University Düsseldorf, Jülich, Germany. Unpublished Data. 2014. [Google Scholar]
- Boellaard, R.; Krak, N.C.; Hoekstra, O.S.; Lammertsma, A.A. Effects of noise, image resolution, and ROI definition on the accuracy of standard uptake values: A simulation study. J. Nucl. Med. 2004, 45, 1519–1527. [Google Scholar] [PubMed]
- Boellaard, R. Standards for PET image acquisition and quantitative data analysis. J. Nucl. Med. 2009, 50, 11S–20S. [Google Scholar] [CrossRef]
- Vriens, D.; Visser, E.P.; de Geus-Oei, L.F.; Oyen, W.J. Methodological considerations in quantification of oncological FDG PET studies. Eur. J. Nucl. Med. Mol. Imag. 2010, 37, 1408–1425. [Google Scholar] [CrossRef]
- Hasenclever, D.; Kurch, L.; Mauz-Korholz, C.; Elsner, A.; Georgi, T.; Wallace, H.; Landman-Parker, J.; Moryl-Bujakowska, A.; Cepelova, M.; Karlen, J.; et al. qPET—A quantitative extension of the Deauville scale to assess response in interim FDG-PETscans in lymphoma. Eur. J. Nucl. Med. Mol. Imag. 2014, 41, 1301–1308. [Google Scholar] [CrossRef]
- Erlandsson, K.; Buvat, I.; Pretorius, P.H.; Thomas, B.A.; Hutton, B.F. A review of partial volume correction techniques for emission tomography and their applications in neurology, cardiology and oncology. Phys. Med. Biol. 2012, 57, R119–R159. [Google Scholar] [CrossRef] [PubMed]
- Avril, N.; Bense, S.; Ziegler, S.I.; Dose, J.; Weber, W.; Laubenbacher, C.; Romer, W.; Janicke, F.; Schwaiger, M. Breast imaging with fluorine-18-FDG PET: Quantitative image analysis. J. Nucl. Med. 1997, 38, 1186–1191. [Google Scholar] [PubMed]
- Hickeson, M.; Yun, M.; Matthies, A.; Zhuang, H.; Adam, L.E.; Lacorte, L.; Alavi, A. Use of a corrected standardized uptake value based on the lesion size on CT permits accurate characterization of lung nodules on FDG-PET. Eur. J. Nucl. Med. Mol. Imag. 2002, 29, 1639–1647. [Google Scholar] [CrossRef]
- Menda, Y.; Bushnell, D.L.; Madsen, M.T.; McLaughlin, K.; Kahn, D.; Kernstine, K.H. Evaluation of various corrections to the standardized uptake value for diagnosis of pulmonary malignancy. Nucl. Med. Commun. 2001, 22, 1077–1081. [Google Scholar] [CrossRef] [PubMed]
- Vesselle, H.; Turcotte, E.; Wiens, L.; Schmidt, R.; Takasugi, J.E.; Lalani, T.; Vallieres, E.; Wood, D.E. Relationship between non-small cell lung cancer fluorodeoxyglucose uptake at positron emission tomography and surgical stage with relevance to patient prognosis. Clin. Cancer Res. 2004, 10, 4709–4716. [Google Scholar] [CrossRef] [PubMed]
- Hatt, M.; le Pogam, A.; Visvikis, D.; Pradier, O.; Cheze Le, R.C. Impact of partial-volume effect correction on the predictive and prognostic value of baseline 18F-FDG PET images in esophageal cancer. J. Nucl. Med. 2012, 53, 12–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maisonobe, J.A.; Garcia, C.A.; Necib, H.; Vanderlinden, B.; Hendlisz, A.; Flamen, P.; Buvat, I. Comparison of PET metabolic indices for the early assessment of tumour response in metastatic colorectal cancer patients treated by polychemotherapy. Eur. J. Nucl. Med. Mol. Imag. 2013, 40, 166–174. [Google Scholar] [CrossRef]
- Ruhl, U.; Albrecht, M.; Dieckmann, K.; Luders, H.; Marciniak, H.; Schellenberg, D.; Wickmann, L.; Dorffel, W. Response-adapted radiotherapy in the treatment of pediatric Hodgkinʼs disease: An interim report at 5 years of the German GPOH-HD 95 trial. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussien, A.E.M.; Furth, C.; Schönberger, S.; Hundsdoerfer, P.; Steffen, I.G.; Amthauer, H.; Müller, H.-W.; Hautzel, H. FDG-PET Response Prediction in Pediatric Hodgkin’s Lymphoma: Impact of Metabolically Defined Tumor Volumes and Individualized SUV Measurements on the Positive Predictive Value. Cancers 2015, 7, 287-304. https://doi.org/10.3390/cancers7010287
Hussien AEM, Furth C, Schönberger S, Hundsdoerfer P, Steffen IG, Amthauer H, Müller H-W, Hautzel H. FDG-PET Response Prediction in Pediatric Hodgkin’s Lymphoma: Impact of Metabolically Defined Tumor Volumes and Individualized SUV Measurements on the Positive Predictive Value. Cancers. 2015; 7(1):287-304. https://doi.org/10.3390/cancers7010287
Chicago/Turabian StyleHussien, Amr Elsayed M., Christian Furth, Stefan Schönberger, Patrick Hundsdoerfer, Ingo G. Steffen, Holger Amthauer, Hans-Wilhelm Müller, and Hubertus Hautzel. 2015. "FDG-PET Response Prediction in Pediatric Hodgkin’s Lymphoma: Impact of Metabolically Defined Tumor Volumes and Individualized SUV Measurements on the Positive Predictive Value" Cancers 7, no. 1: 287-304. https://doi.org/10.3390/cancers7010287
APA StyleHussien, A. E. M., Furth, C., Schönberger, S., Hundsdoerfer, P., Steffen, I. G., Amthauer, H., Müller, H. -W., & Hautzel, H. (2015). FDG-PET Response Prediction in Pediatric Hodgkin’s Lymphoma: Impact of Metabolically Defined Tumor Volumes and Individualized SUV Measurements on the Positive Predictive Value. Cancers, 7(1), 287-304. https://doi.org/10.3390/cancers7010287