
Nephrotoxicity as a Dose-Limiting Factor in a High-Dose Cisplatin-Based Chemoradiotherapy Regimen for Head and Neck Carcinomas

Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Ethical Considerations
2.3. Chemotherapy
2.4. Radiotherapy
2.5. Evaluation
2.6. Renal Function
2.7. Food and Fluid Intake
2.8. Statistical Analyses
3. Results
3.1. Patient Characteristics

{kind=link}
| Sex | |
| Male | 152 (73%) |
| Female | 56 (27%) |
| Age | |
| Median (range) | 59 (32–79) |
| Mean (sd) | 58 (8.9) |
| Tumor location | |
| Oral cavity | 24 (12%) |
| Oropharynx | 106 (51%) |
| Nasopharynx | 17 (8%) |
| Hypopharynx | 40 (19%) |
| Larynx | 10 (5%) |
| Paranasal sinus | 9 (4%) |
| Parotic gland | 2 (1%) |
| Tumor-stage * | |
| T1 | 25 (12%) |
| T2 | 55 (26%) |
| T3 | 65 (31%) |
| T4 | 62 (30%) |
| Tx | 1 (0%) |
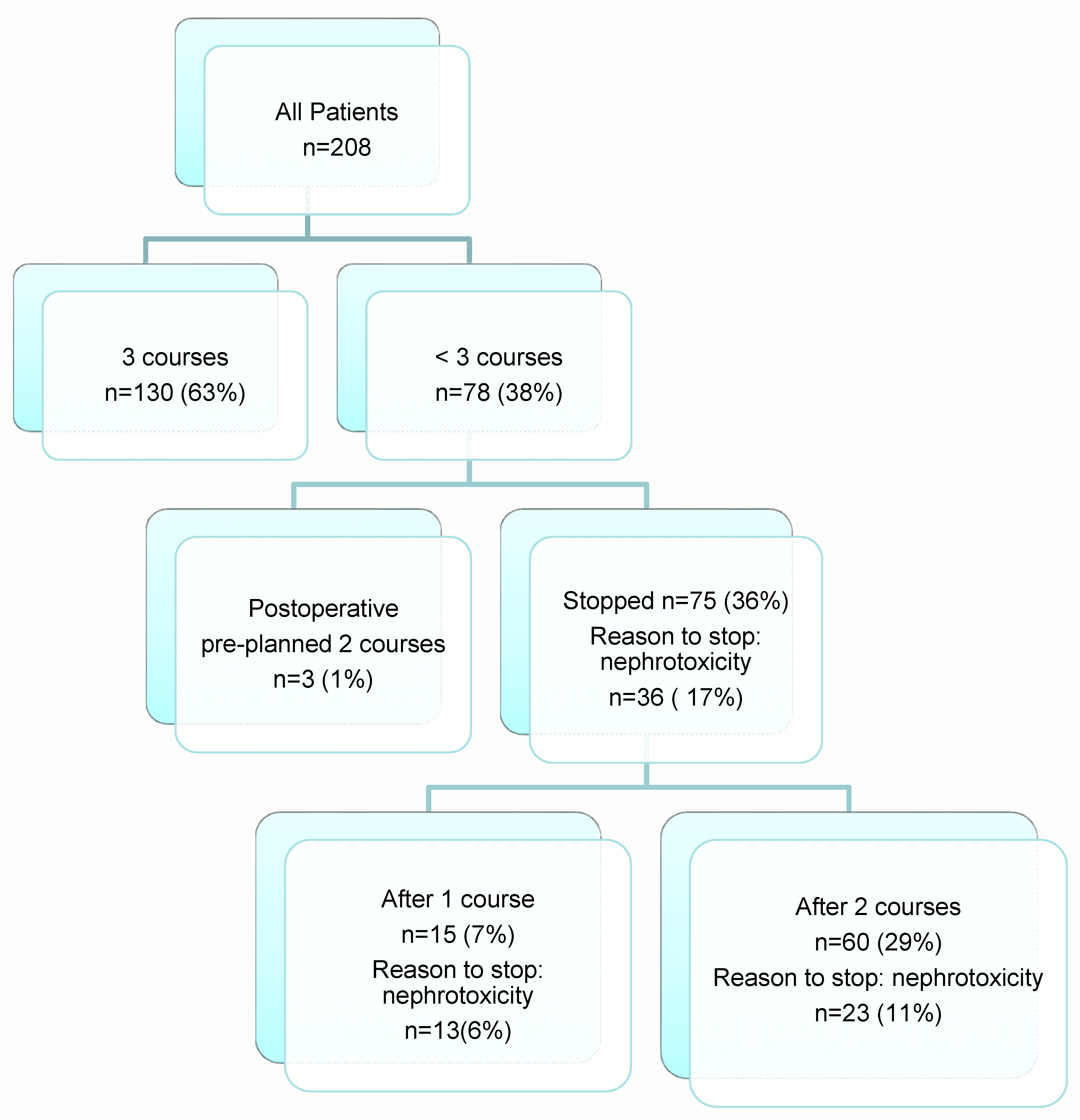
3.2. Treatment Characteristics
| Treatment Intent | N (%) |
|---|---|
| Definitive | 189 (91%) |
| Postoperative | 19 (9%) |
| Cisplatin courses | |
| 1 | 15 (7%) |
| 2 | 63 (30%) |
| 3 | 130 (63%) |
| Mean cisplatin dose mg/m2 (sd) | 254 (62.3) |
| Radiotherapy Median total dose Gy (sd) | 70 |

3.3. Evaluation of Renal Function
| GFR | Serum | GFR | Serum Creatinine | |
|---|---|---|---|---|
| 59–30 mL/min →59–50 mL/min * →49–30 mL/min ** | creatinine 2–3× above baseline | <29–15 mL/min | >3× above baseline or creatinine increase >35 µmol/L | |
| Grade 2 *** | Grade 2 *** | Grade 3 *** | Grade 3 *** | |
| Before therapy N = 208 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| After 1 course N = 208 | 22 (11%) →10 (5%) →12 (6%) | 3 (1%) | 8 (4%) | 4 (2%) |
| After 2 courses N = 193 **** | 31 (16%) →5 (2%) →26 (13%) | 8 (4%) | 8 (4%) | 7(4%) |
| After 3 months N = 202 ***** | 42 (21%) →12 (6%) →30 (14%) | 14 (7%) | 4 (2%) | 4 (2%) |
| All Patients N = 208 | Stop Chemotherapy after 1 Course, Due to Nephrotoxicity N = 13 | Stop Chemotherapy after 2 Courses, Due to Nephrotoxicity N = 23 | |
|---|---|---|---|
| Start: GFR median (range) | 101( 57–235) | 88 (60–119) | 84 (62–124) |
| After 3 months: GFR | 80 (4–225) | 68 (27–111) | 88 (28–203) |
4. Discussion
Author Contributions
Conflicts of Interest
References
- Furness, S.; Glenny, A.M.; Worthington, H.V.; Pavitt, S.; Oliver, R.; Clarkson, J.E.; Macluskey, M.; Chan, K.K.; Conway, D.I. Interventions for the treatment of oral cavity and oropharyngeal cancer: Chemotherapy. Cochrane Database Syst. Rev. 2010, 4, CD006386. [Google Scholar] [CrossRef]
- Pignon, J.P.; le Maître, A.; Maillard, E.; Bourhis, J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Bourhis, J.; Sire, C.; Graff, P.; Grégoire, V.; Maingon, P.; Calais, G.; Gery, B.; Martin, L.; Alfonsi, M.; Desprez, P.; et al. Concomitant chemoradiotherapy versus acceleration of radiotherapy with or without concomitant chemotherapy in locally advanced head and neck carcinoma (GORTEC 99-02): An open-label phase 3 randomised trial. Lancet Oncol. 2012, 13, 145–153. [Google Scholar] [CrossRef]
- Pignon, J.P.; Bourhis, J.; Domenge, C.; Designé, L. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: Three meta-analyses of updated individual data. Lancet 2000, 355, 949–955. [Google Scholar] [CrossRef]
- Budach, W.; Hehr, T.; Budach, V.; Belka, C.; Dietz, K. A meta-analysis of hyperfractionated and accelerated radiotherapy and combined chemotherapy and radiotherapy regimens in unresected locally advanced squamous cell carcinoma of the head and neck. BMC Cancer 2006, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Adelstein, D.J.; Li, Y.; Adams, G.L.; Wagner, H., Jr.; Kish, J.A.; Ensley, J.F.; Schuller, D.E.; Forastiere, A.A. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J. Clin. Oncol. 2003, 21, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.A.; Goepfert, H.; Maor, M.; Pajak, T.F.; Weber, R.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; Chao, C.; et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef] [PubMed]
- Browman, G.P.; Hodson, D.I.; Mackenzie, R.J.; Bestic, N.; Zuraw, L. Cancer Care Ontario Practice Guideline Initiative Head and Neck Cancer Disease Site Group, Choosing a concomitant chemotherapy and radiotherapy regimen for squamous cell head and neck cancer: A systematic review of the published literature with subgroup analysis. Head Neck 2001, 23, 579–589. [Google Scholar] [PubMed]
- Fan, K.Y.; Gogineni, H.; Zaboli, D.; Lake, S.; Zahurak, M.L.; Best, S.R.; Levine, M.A.; Tang, M.; Zinreich, E.S.; Saunders, J.R.; et al. Comparison of acute toxicities in two primary chemoradiation regimens in the treatment of advanced head and neck squamous cell carcinoma. Ann. Surg. Oncol. 2012, 19, 1980–1987. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Kronemann, S.; Meyners, T.; Bohlen, G.; Tribius, S.; Kazic, N.; Schroeder, U.; Hakim, S.G.; Schild, S.E.; Dunst, J. Comparison of four cisplatin-based radiochemotherapy regimens for nonmetastatic stage III/IV squamous cell carcinoma of the head and neck. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Rasch, C.R.; Hauptmann, M.; Balm, A.J. Intra-arterial chemotherapy for head and neck cancer: Is there a verdict? Cancer 2011, 117, 874. [Google Scholar] [CrossRef] [PubMed]
- Espeli, V.; Zucca, E.; Ghielmini, M.; Giannini, O.; Salatino, A.; Martucci, F.; Richetti, A. Weekly and 3-weekly cisplatin concurrent with intensity-modulated radiotherapy in locally advanced head and neck squamous cell cancer. Oral Oncol. 2012, 48, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, N.A.; Carvalho Rodrigues, M.A.; Martins, N.M.; dos Santos, A.C. Cisplatin-induced nephrotoxicity and targets of nephroprotection: An update. Arch Toxicol 2012, 86, 1233–1250. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Fehlauer, F.; Sheikh-Sarraf, M.; Kazic, N.; Basic, H.; Poorter, R.; Hakim, S.G.; Schild, S.E.; Dunst, J. Toxicity of two cisplatin-based radiochemotherapy regimens for the treatment of patients with stage III/IV head and neck cancer. Head Neck 2008, 30, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Strojan, P.; Vermorken, J.B.; Beitler, J.J.; Saba, N.F.; Haigentz, M.; Bossi, P., Jr.; Worden, F.P.; Langendijk, J.A.; Eisbruch, A.; Mendenhall, W.M.; et al. Cumulative cisplatin dose in concurrent chemoradiotherapy for head and neck cancer: A systematic review. Head Neck 2015. [Google Scholar] [CrossRef] [PubMed]
- Hoebers, F.J.; Heemsbergen, W.; Balm, A.J.; van Zanten, M.; Schornagel, J.H.; Rasch, C.R. Concurrent chemoradiation with daily low dose cisplatin for advanced stage head and neck carcinoma. Radiother. Oncol. 2007, 85, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Santoso, J.T.; Lucci, J.A., 3rd; Coleman, R.L.; Schafer, I.; Hannigan, E.V. Saline, mannitol, and furosemide hydration in acute cisplatin nephrotoxicity: A randomized trial. Cancer Chemother. Pharmacol. 2003, 52, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Romesser, P.B.; Romanyshyn, J.C.; Schupak, K.D.; Setton, J.; Riaz, N.; Wolden, S.L.; Gelblum, D.Y.; Sherman, E.J.; Kraus, D.; Lee, N.Y. Percutaneous endoscopic gastrostomy in oropharyngeal cancer patients treated with intensity-modulated radiotherapy with concurrent chemotherapy. Cancer 2012, 118, 6072–6078. [Google Scholar] [CrossRef] [PubMed]
- Muraki, K.; Koyama, R.; Honma, Y.; Yagishita, S.; Shukuya, T.; Ohashi, R.; Takahashi, F.; Kido, K.; Iwakami, S.; Sasaki, S.; et al. Hydration with magnesium and mannitol without furosemide prevents the nephrotoxicity induced by cisplatin and pemetrexed in patients with advanced non-small cell lung cancer. J. Thorac. Dis. 2012, 4, 562–568. [Google Scholar] [PubMed]
- Morgan, K.P.; Buie, L.W.; Savage, S.W. The role of mannitol as a nephroprotectant in patients receiving cisplatin therapy. Ann. Pharmacother. 2012, 46, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Morgan, K.P.; Snavely, A.C.; Wind, L.S.; Buie, L.W.; Grilley-Olson, J.; Walko, C.M.; Weiss, J. Rates of renal toxicity in cancer patients receiving cisplatin with and without mannitol. Ann. Pharmacother. 2014. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Guo, D.; Dong, Z.; Zhang, W.; Zhang, L.; Huang, S.M.; Polli, J.E.; Shu, Y. Ondansetron can enhance cisplatin-induced nephrotoxicity via inhibition of multiple toxin and extrusion proteins (MATEs). Toxicol. Appl. Pharmacol. 2013, 273, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Rubera, I.; Duranton, C.; Melis, N.; Cougnon, M.; Mograbi, B.; Tauc, M. Role of CFTR in oxidative stress and suicidal death of renal cells during cisplatin-induced nephrotoxicity. Cell Death Dis. 2013, 4, e817. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoek, J.; Bloemendal, K.M.; Van der Velden, L.-A.A.; Van Diessen, J.N.A.; Van Werkhoven, E.; Klop, W.M.C.; Tesselaar, M.E.T. Nephrotoxicity as a Dose-Limiting Factor in a High-Dose Cisplatin-Based Chemoradiotherapy Regimen for Head and Neck Carcinomas. Cancers 2016, 8, 21. https://doi.org/10.3390/cancers8020021
Hoek J, Bloemendal KM, Van der Velden L-AA, Van Diessen JNA, Van Werkhoven E, Klop WMC, Tesselaar MET. Nephrotoxicity as a Dose-Limiting Factor in a High-Dose Cisplatin-Based Chemoradiotherapy Regimen for Head and Neck Carcinomas. Cancers. 2016; 8(2):21. https://doi.org/10.3390/cancers8020021
Chicago/Turabian StyleHoek, Jantien, Karen M. Bloemendal, Lilly-Ann A. Van der Velden, Judi N.A. Van Diessen, Erik Van Werkhoven, Willem M.C. Klop, and Margot E.T. Tesselaar. 2016. "Nephrotoxicity as a Dose-Limiting Factor in a High-Dose Cisplatin-Based Chemoradiotherapy Regimen for Head and Neck Carcinomas" Cancers 8, no. 2: 21. https://doi.org/10.3390/cancers8020021
APA StyleHoek, J., Bloemendal, K. M., Van der Velden, L. -A. A., Van Diessen, J. N. A., Van Werkhoven, E., Klop, W. M. C., & Tesselaar, M. E. T. (2016). Nephrotoxicity as a Dose-Limiting Factor in a High-Dose Cisplatin-Based Chemoradiotherapy Regimen for Head and Neck Carcinomas. Cancers, 8(2), 21. https://doi.org/10.3390/cancers8020021