
Formulation and Evaluation of Hydrophilic Polymer Based Methotrexate Patches: In Vitro and In Vivo Characterization

 , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Formulation of Transdermal Patches of Methotrexate
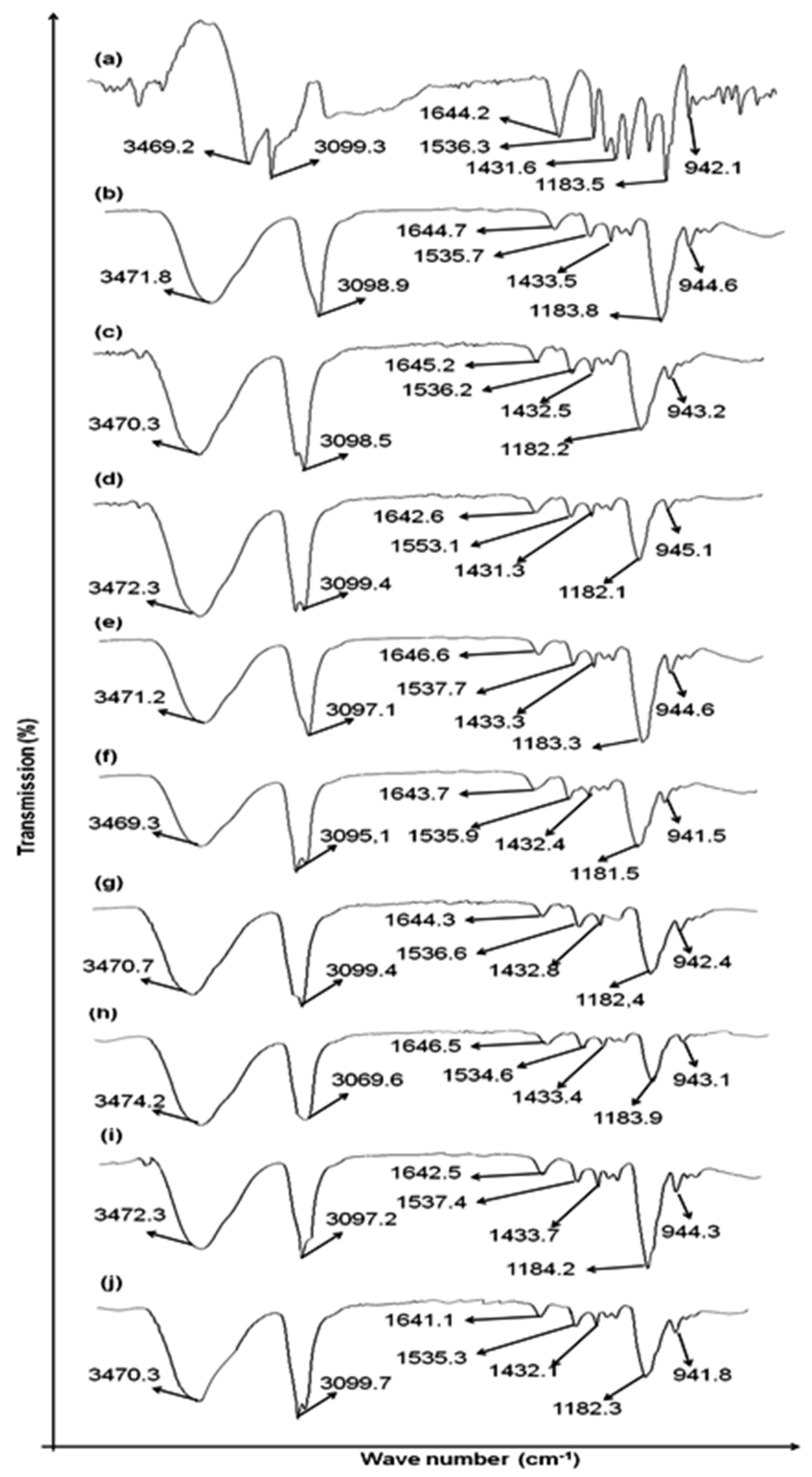
2.3. Compatibility Studies (Preformulation Study)
2.4. Physicochemical Evaluation of MTX Loaded Patches
2.4.1. Surface pH
2.4.2. Physical Appearance
2.4.3. Measurement of Thickness
2.4.4. Weight Variation
2.4.5. Folding Endurance
2.4.6. Tensile Strength (Kg/cm2)
2.4.7. Percent Moisture Content (%)
2.4.8. Evaluation of Swelling Index
2.4.9. Estimation of Drug Content
2.4.10. Water Vapor Transmission Rate
2.5. Stability Study
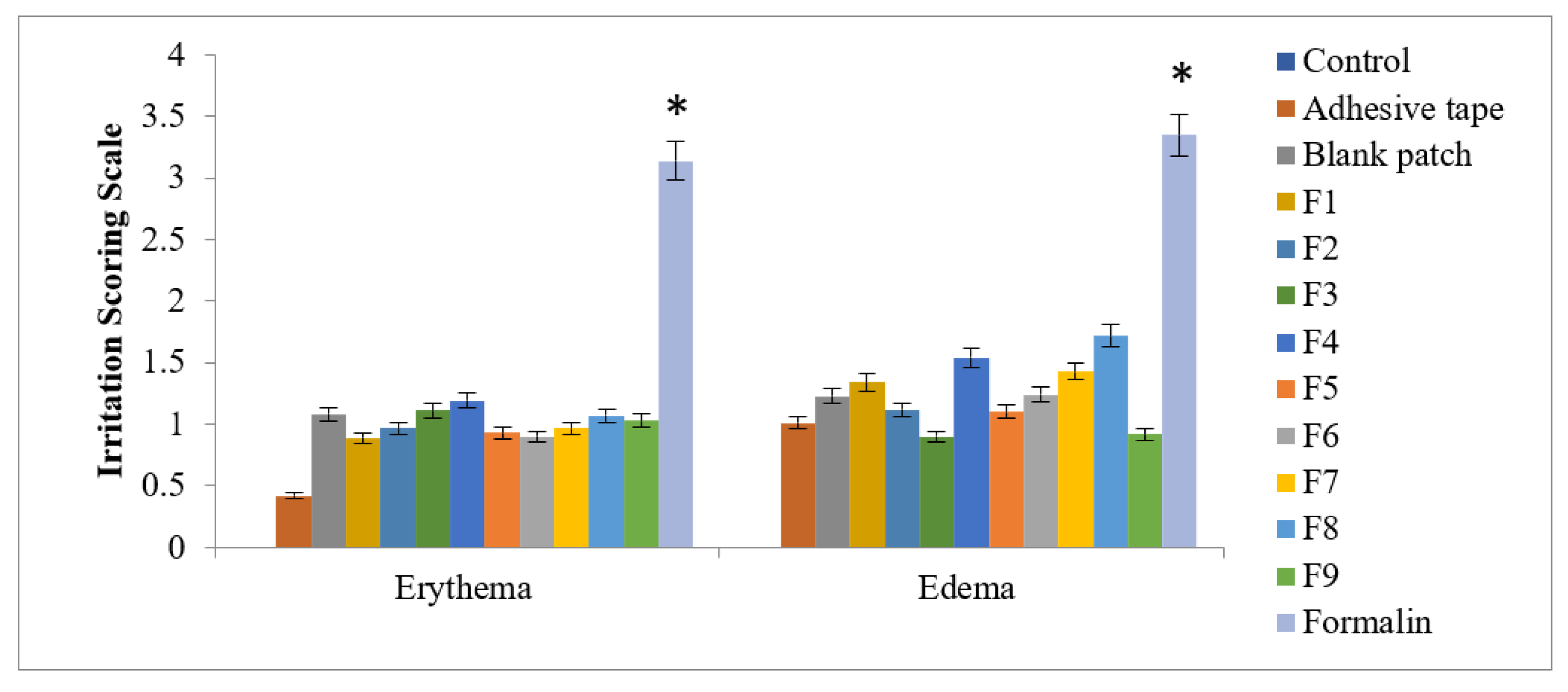
2.6. Skin Irritation Study
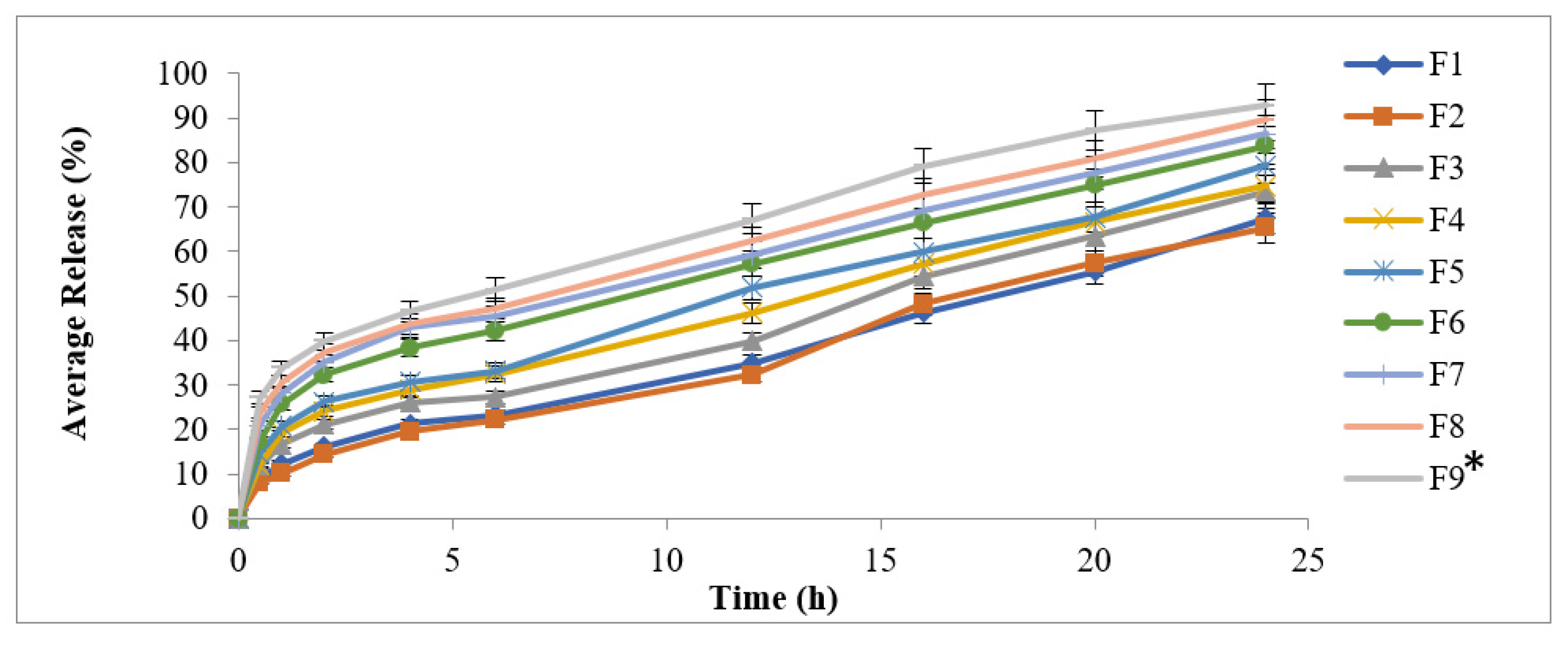
2.7. In Vitro Drug Release Study
2.8. Kinetics of Drug Release
2.8.1. Zero Order Kinetics
2.8.2. First Order Kinetics
2.8.3. Hixon Crowell Model
2.8.4. Higuchi Model
2.8.5. Power Law Equation
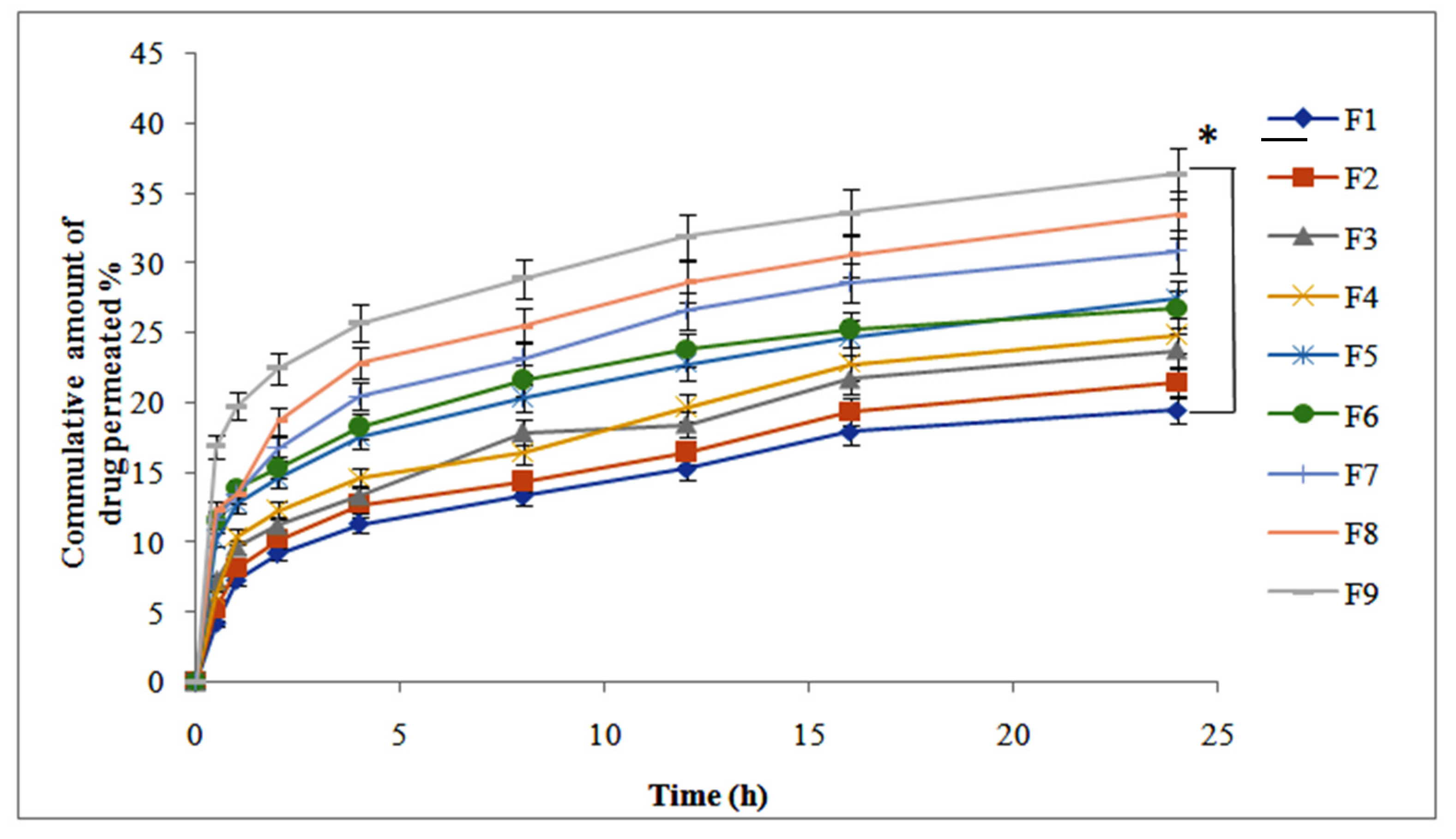
2.9. The Ex Vivo Permeation Study
Preparation of Rabbit Skin
2.10. Drug Retention Study
2.11. Skin ATR-FTIR Spectroscopy
2.12. In Vivo Studies
2.13. Statistical Analysis
3. Results
3.1. Drug Excipients Compatibility Studies (Preformulation Study)
3.2. Physicochemical Assessment of Methotrexate-Loaded Transdermal Patches

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Amount of Polymers | Amount of Solvents (v/v) mL | ||||||
|---|---|---|---|---|---|---|---|
| Batch | Amount of MTX (mg) | CMC-Na (mg) | HPMC (mg) | Combination CMC-Na/HPMC | Plasticizer PEG400 (%) | Ethanol | Distilled Water |
| F1 (Control) | 5 | 100 | 100 | 1:1 | 30 | 10 | 10 |
| F2 | 5 | 100 | 200 | 1:2 | 30 | 10 | 10 |
| F3 | 5 | 100 | 300 | 1:3 | 30 | 10 | 10 |
| F4 | 5 | 100 | 400 | 1:4 | 30 | 10 | 10 |
| F5 | 5 | 100 | 500 | 1:5 | 30 | 10 | 10 |
| F6 | 5 | 200 | 100 | 2:1 | 30 | 10 | 10 |
| F7 | 5 | 300 | 100 | 3:1 | 30 | 10 | 10 |
| F8 | 5 | 400 | 100 | 4:1 | 30 | 10 | 10 |
| F9 | 5 | 500 | 100 | 5:1 | 30 | 10 | 10 |
| Characteristics | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| F Codes | pH | Thickness (mm) | Weight Variation (mg) | Folding Endurance | Tensile Strength kg/cm2 | % Moisture Content | % Swelling Index | % Drug Content | Water Transmission Rateg/m2/24 h |
| F1 | 5.2 | 0.51 ± 0.02 | 73.86 ± 0.03 | 62 ± 2.21 | 9.62 ± 0.43 | 9.26 ± 1.52 | 37.16 ± 0.17 | 95.75 ± 4.22 | 3.23 ± 0.15 |
| F2 | 5.4 | 0.59 ± 0.03 | 75.34 ± 0.04 | 64 ± 3.14 | 10.37 ± 0.26 | 10.21 ± 1.16 | 42.65 ± 1.46 | 96.80 ± 3.32 | 3.34 ± 0.26 |
| F3 | 5.4 | 0.63 ± 0.01 | 77.88 ± 0.03 | 63 ± 1.43 | 12.32 ± 0.47 | 10.27 ± 1.25 | 47.43 ± 0.58 | 93.57 ± 5.34 | 3.68 ± 0.38 |
| F4 | 5.6 | 0.72 ± 0.05 | 79.75 ± 0.03 | 67 ± 3.23 | 11.72 ± 0.57 | 10.35 ± 1.45 | 57.02 ± 0.25 | 97.50 ± 3.21 | 3.92 ± 0.29 |
| F5 | 5.9 | 0.73 ± 0.06 | 80.33 ± 0.04 | 69 ± 2.55 | 9.42 ± 0.52 | 10.89 ± 1.71 | 62.58 ± 1.89 | 94.15 ± 4.23 | 4.15 ± 0.33 |
| F6 | 5.7 | 0.62 ± 0.03 | 78.54 ± 0.05 | 71 ± 1.34 | 10.25 ± 0.92 | 10.85 ± 1.50 | 48.73 ± 0.54 | 97.12 ± 2.43 | 4.27 ± 0.46 |
| F7 | 5.4 | 0.69 ± 0.02 | 87.66 ± 0.03 | 73 ± 3.21 | 9.57 ± 0.13 | 11.25 ± 1.23 | 57.85 ± 1.15 | 96.23 ± 3.32 | 4.48 ± 0.72 |
| F8 | 5.5 | 0.78 ± 0.04 | 96.54 ± 0.21 | 76 ± 4.23 | 11.14 ± 0.28 | 11.63 ± 1.50 | 65.61 ± 0.21 | 97.39 ± 2.35 | 4.79 ± 0.64 |
| F9 | 5.7 | 0.87 ± 0.06 | 103.33 ± 0.15 | 78 ± 1.54 | 12.33 ± 0.72 | 11.85 ± 1.56 | 76.24 ± 1.37 | 98.19 ± 1.56 | 4.92 ± 0.78 |
3.3. Stability Study
3.4. Skin Irritation Study
3.5. In Vitro Drug Release Study
3.6. Drug Release Kinetics
3.7. Ex Vivo Drug Permeation Study
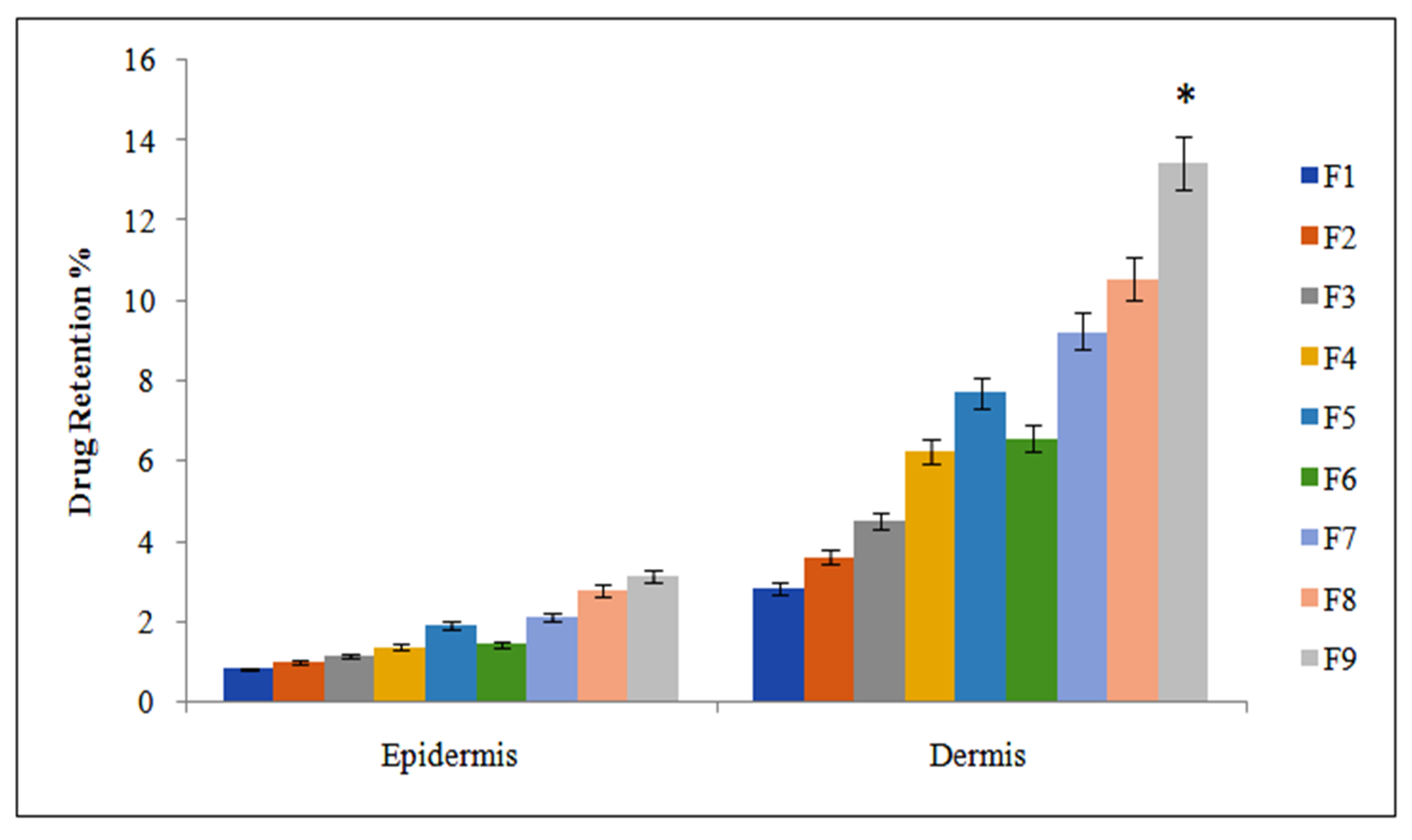
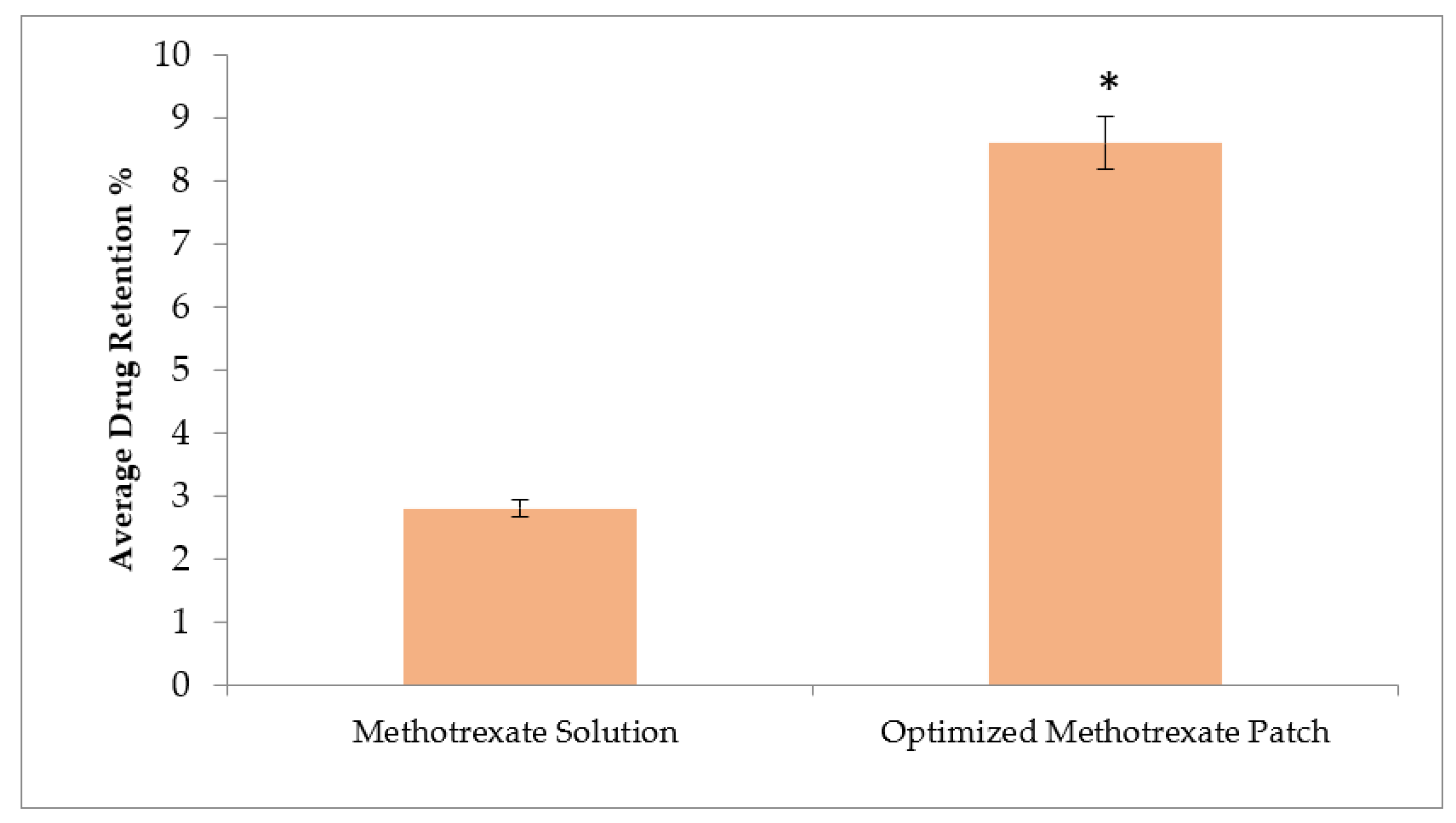
3.8. Drug Retention
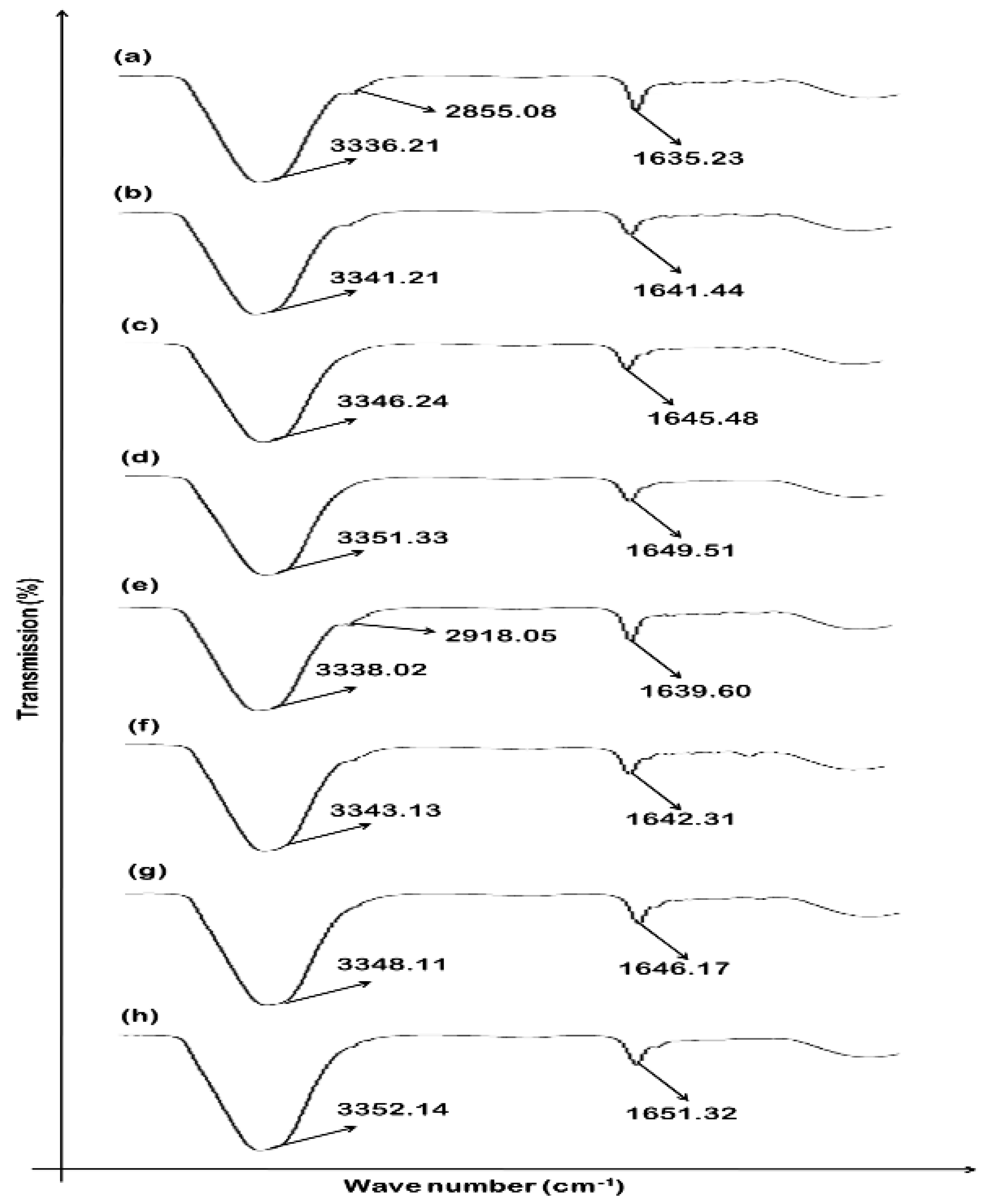
3.9. Effect of MTX-Loaded Patch Formulations on Skin Structure
3.10. In Vivo Studies
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hussan, J.R.; Hunter, P.J. Our natural “makeup” reveals more than it hides: Modeling the skin and its microbiome. WIREs Mech. Dis. 2021, 13, e1497. [Google Scholar] [CrossRef]
- Lawton, S. Skin 1: The structure and functions of the skin. Nurs. Times 2019, 115, 30–33. [Google Scholar]
- Chen, Z.; Ceballos-Francisco, D.; Guardiola, F.A.; Esteban, M.Á. Influence of skin wounds on the intestinal inflammatory response and barrier function: Protective role of dietary Shewanella putrefaciens SpPdp11 administration to gilthead seabream (Sparus aurata L.). Fish Shellfish Immunol. 2020, 99, 414–423. [Google Scholar] [CrossRef]
- Boireau-Adamezyk, E.; Baillet-Guffroy, A.; Stamatas, G.N. The stratum corneum water content and natural moisturization factor composition evolve with age and depend on body site. Int. J. Dermatol. 2021, 60, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Sapkota, R.; Dash, A.K. Liposomes and transferosomes: A breakthrough in topical and transdermal delivery. Ther. Deliv. 2021, 12, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Furue, M.; Furue, K.; Tsuji, G.; Nakahara, T. Interleukin-17A and keratinocytes in psoriasis. Int. J. Mol. Sci. 2020, 21, 1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Adamio, S.; Silvaggio, D.; Massaro, A.; Lombardo, P.; Bianchi, L.; Talamonti, M.; Galluzzo, M. Pharmacotherapeutic management of psoriasis in adolescents and children. Expert Opin. Pharmacother. 2019, 20, 1777–1785. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Liu, H.; Lu, C.; Deng, J.; Yan, Y.; Chen, H.; Wang, Y.; Liang, C.L.; Wei, J.; Han, L. Kaempferol attenuates imiquimod-induced psoriatic skin inflammation in a mouse model. Clin. Exp. Immunol. 2019, 198, 403–415. [Google Scholar] [CrossRef]
- Liu, L.C.; Jin, X.H.; Sun, C.; Xia, J.X. Two cases of refractory erythrodermic psoriasis effectively treated with secukinumab and a review of the literature. Dermatol. Ther. 2021, 34, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Nayak, R.R.; Alexander, M.; Deshpande, I.; Stapleton-Gray, K.; Rimal, B.; Patterson, A.D.; Ubeda, C.; Scher, J.U.; Turnbaugh, P.J. Methotrexate impacts conserved pathways in diverse human gut bacteria leading to decreased host immune activation. Cell Host Microbe 2021, 29, 362–377.e311. [Google Scholar] [CrossRef] [PubMed]
- Dehshahri, A.; Kumar, A.; Madamsetty, V.S.; Uzieliene, I.; Tavakol, S.; Azedi, F.; Fekri, H.S.; Zarrabi, A.; Mohammadinejad, R.; Thakur, V.K. New horizons in hydrogels for methotrexate delivery. Gels 2021, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.Y.; Kwon, M.; Choi, H.E.; Kim, K.S. Recent advances in transdermal drug delivery systems: A review. Biomater. Res. 2021, 25, 24. [Google Scholar] [CrossRef] [PubMed]
- Alam, A.; Machale, M.U.; Yadav, R.P.; Sharma, M.; Patel, A.K. Role of Transdermal Drug Delivery System. Asian J. Pharm. Res. Dev. 2021, 9, 137–143. [Google Scholar] [CrossRef]
- Stefanov, S.R.; Andonova, V.Y. Lipid Nanoparticulate Drug Delivery Systems: Recent Advances in the Treatment of Skin Disorders. Pharmaceuticals 2021, 14, 1083. [Google Scholar] [CrossRef]
- Ahsan, A.; Tian, W.-X.; Farooq, M.A.; Khan, D.H. An overview of hydrogels and their role in transdermal drug delivery. Int. J. Polym. Mater. Polym. Biomater. 2021, 70, 574–584. [Google Scholar] [CrossRef]
- Latif, M.S.; Azad, A.K.; Nawaz, A.; Rashid, S.A.; Rahman, M.; Al Omar, S.Y.; Bungau, S.G.; Aleya, L.; Abdel-Daim, M.M. Ethyl Cellulose and Hydroxypropyl Methyl Cellulose Blended Methotrexate-Loaded Transdermal Patches: In Vitro and Ex Vivo. Polymers 2021, 13, 3455. [Google Scholar] [CrossRef]
- Lengyel, M.; Kállai-Szabó, N.; Antal, V.; Laki, A.J.; Antal, I. Microparticles, microspheres, and microcapsules for advanced drug delivery. Sci. Pharm. 2019, 87, 20. [Google Scholar] [CrossRef] [Green Version]
- Zeb, A.; Qureshi, O.S.; Kim, H.-S.; Cha, J.-H.; Kim, H.-S.; Kim, J.-K. Improved skin permeation of methotrexate via nanosized ultradeformable liposomes. Int. J. Nanomed. 2016, 11, 3813. [Google Scholar]
- Ullah, W.; Nawaz, A.; Akhlaq, M.; Shah, K.U.; Latif, M.S.; Alfatama, M. Transdermal delivery of gatifloxacin carboxymethyl cellulose-based patches: Preparation and characterization. J. Drug Deliv. Sci. Technol. 2021, 66, 102783. [Google Scholar] [CrossRef]
- Kulkarni, S. Formulation and evaluation of transdermal patch for atomoxetine hydrochloride. J. Drug Deliv. Ther. 2019, 9, 32–35. [Google Scholar]
- Rao, M.; Rao, Y. Characterization and Ex Vivo Studies of Nanoparticle Incorporated Transdermal Patch of Itraconazole. Indian J. Pharm. Sci. 2020, 82, 809–818. [Google Scholar] [CrossRef]
- Chandra, A.; Aggarwal, G.; Manchanda, S.; Narula, A. Development of topical gel of methotrexate incorporated ethosomes and salicylic acid for the treatment of psoriasis. Pharm. Nanotechnol. 2019, 7, 362–374. [Google Scholar] [CrossRef]
- Yu, M.; Lu, Z.; Shi, Y.; Du, Y.; Chen, X.; Kong, M. Systematic comparisons of dissolving and swelling hyaluronic acid microneedles in transdermal drug delivery. Int. J. Biol. Macromol. 2021, 191, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.P.; Patel, G.; Patel, H.; Baria, A. Formulation and evaluation of transdermal patch of aceclofenac. Res. J. Pharm. Dos. Technol. 2009, 1, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Oxley, J.A.; Ellis, C.F.; McBride, E.A.; McCormick, W.D. A survey of rabbit handling methods within the United Kingdom and the Republic of Ireland. J. Appl. Anim. Welf. Sci. 2019, 22, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Mulleria, S.S.; Marina, K.; Ghetia, S.M. Formulation, Optimization and in vitro Evaluation of Apremilast Nanoemulgel for Topical Delivery. Int. J. Pharm. Investig. 2021, 11, 230–237. [Google Scholar] [CrossRef]
- Azad, A.K.; Doolaanea, A.A.; Al-Mahmood, S.M.A.; Kennedy, J.F.; Chatterjee, B.; Bera, H. Electro-hydrodynamic assisted synthesis of lecithin-stabilized peppermint oil-loaded alginate microbeads for intestinal drug delivery. Int. J. Biol. Macromol. 2021, 185, 861–875. [Google Scholar] [CrossRef] [PubMed]
- Bera, H.; Abbasi, Y.F.; Gajbhiye, V.; Liew, K.F.; Kumar, P.; Tambe, P.; Azad, A.K.; Cun, D.; Yang, M. Carboxymethyl fenugreek galactomannan-g-poly (N-isopropylacrylamide-co-N, N’-methylene-bis-acrylamide)-clay based pH/temperature-responsive nanocomposites as drug-carriers. Mater. Sci. Eng. C 2020, 110, 110628. [Google Scholar] [CrossRef]
- Ahmed, O.A.; Badr-Eldin, S.M. Development of an optimized avanafil-loaded invasomal transdermal film: Ex vivo skin permeation and in vivo evaluation. Int. J. Pharm. 2019, 570, 118657. [Google Scholar] [CrossRef] [PubMed]
- Imtiaz, M.S.; Shoaib, M.H.; Yousuf, R.I.; Ali, F.R.; Saleem, M.T.; Khan, M.Z.; Sikandar, M. Formulation development and evaluation of drug-in-adhesive-type transdermal patch of metoclopramide HCl. Polym. Bull. 2021, 79, 1187–1200. [Google Scholar] [CrossRef]
- Keller, J.D. Sodium carboxymethylcellulose (CMC). In Food Hydrocolloids; CRC Press: Boca Raton, FL, USA, 2020; pp. 43–109. [Google Scholar]
- Arshad, M.S.; Fatima, S.; Nazari, K.; Ali, R.; Farhan, M.; Muhammad, S.A.; Abbas, N.; Hussain, A.; Kucuk, I.; Chang, M.-W. Engineering and characterisation of BCG-loaded polymeric microneedles. J. Drug Target. 2020, 28, 525–532. [Google Scholar] [CrossRef]
- Arca, H.C.; Mosquera-Giraldo, L.I.; Bi, V.; Xu, D.; Taylor, L.S.; Edgar, K.J. Pharmaceutical applications of cellulose ethers and cellulose ether esters. Biomacromolecules 2018, 19, 2351–2376. [Google Scholar] [CrossRef] [PubMed]
- Rohith, G.; Satheesha Babu, B. Influence of chitosan thioglycolic acid conjugate in improving bioavailability of an antiparkinson drug; Rasagiline Mesylate from transdermal patch. Drug Dev. Ind. Pharm. 2021, 47, 963–976. [Google Scholar] [CrossRef] [PubMed]
- Garhy, D.M.; Ismail, S.; Ibrahim, H.K.; Ghorab, M.M. Buccoadhesive gel of carvedilol nanoparticles for enhanced dissolution and bioavailability. J. Drug Deliv. Sci. Technol. 2018, 47, 151–158. [Google Scholar] [CrossRef]
- Rajput, R.L.; Narkhede, J.S.; Mujumdar, A.; Naik, J.B. Synthesis and evaluation of luliconazole loaded biodegradable nanogels prepared by pH-responsive Poly (acrylic acid) grafted Sodium Carboxymethyl Cellulose using amine based cross linker for topical targeting: In vitro and Ex vivo assessment. Polym. Plast. Technol. Mater. 2020, 59, 1654–1666. [Google Scholar] [CrossRef]
- Mishra, B.; Bonde, G.V. Transdermal drug delivery. In Controlled Drug Delivery Systems; CRC Press: Boca Raton, FL, USA, 2020; pp. 239–275. [Google Scholar]
- Sivasankarapillai, V.; Das, S.; Sabir, F.; Sundaramahalingam, M.; Colmenares, J.; Prasannakumar, S.; Rajan, M.; Rahdar, A.; Kyzas, G. Progress in natural polymer engineered biomaterials for transdermal drug delivery systems. Mater. Today Chem. 2021, 19, 100382. [Google Scholar] [CrossRef]
- Rashid, S.A.; Bashir, S.; Naseem, F.; Farid, A.; Rather, I.A.; Hakeem, K.R. Olive Oil Based Methotrexate Loaded Topical Nanoemulsion Gel for the Treatment of Imiquimod Induced Psoriasis-like Skin Inflammation in an Animal Model. Biology 2021, 10, 1121. [Google Scholar] [CrossRef]







| F Code | Initial % Drug Content | 25 ± 2C (60 ± 5%RH) | 40 ± 2C (75 ± 5%RH) | ||||
|---|---|---|---|---|---|---|---|
| 15 Days | 30 Days | 60 Days | 15 Days | 30 Days | 60 Days | ||
| F1 | 95.75 ± 4.22 | 95.54 ± 3.65 | 95.23 ± 3.56 | 94.87 ± 4.43 | 95.65 ± 4.55 | 94.32 ± 3.87 | 92.10 ± 4.47 |
| F2 | 96.80 ± 3.32 | 96.45 ± 2.44 | 95.84 ± 2.43 | 95.34 ± 3.35 | 96.30 ± 3.43 | 95.67 ± 4.45 | 94.84 ± 2.65 |
| F3 | 93.57 ± 5.34 | 93.26 ± 3.34 | 92.91 ± 4.76 | 99.42 ± 1.67 | 93.53 ± 3.26 | 93.05 ± 4.34 | 92.56 ± 3.58 |
| F4 | 97.50 ± 3.21 | 96.76 ± 4.65 | 96.41 ± 3.46 | 96.11 ± 2.65 | 97.23 ± 2.43 | 96.75 ± 3.24 | 96.18 ± 4.62 |
| F5 | 94.05 ± 4.23 | 93.69 ± 3.45 | 93.21 ± 4.81 | 92.79 ± 5.45 | 93.66 ± 4.54 | 93.34 ± 2.31 | 92.88 ± 2.16 |
| F6 | 97.12 ± 2.43 | 96.77 ± 2.34 | 96.20 ± 2.13 | 95.14 ± 4.34 | 96.91 ± 3.12 | 95.64 ± 4.34 | 95.21 ± 1.63 |
| F7 | 98.09 ± 1.56 | 97.67 ± 1.54 | 97.32 ± 1.26 | 96.77 ± 3.22 | 98.02 ± 1.21 | 97.87 ± 1.32 | 97.36 ± 3.73 |
| F8 | 97.39 ± 2.35 | 97.08 ± 2.23 | 96.88 ± 3.25 | 96.65 ± 4.34 | 97.16 ± 2.24 | 93.82 ± 2.37 | 93.46 ± 1.48 |
| F9 | 96.23 ± 3.32 | 95.74 ± 1.12 | 95.43 ± 1.22 | 94.52 ± 3.21 | 96.04 ± 1.43 | 95.64 ± 1.46 | 95.12 ± 1.52 |
| F Code | Zero-Order | 1st-Order | Higuchi | Hixon–Crowell | Korsmeyer–Peppas | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| K ± SD | R2 | K ± SD | R2 | K ± SD | R2 | K ± SD | R2 | K ± SD | R2 | n | |
| F1 | 6.083 ± 1.028 | 0.956 | 0.079 ± 0.121 | 0.932 | 5.661 ± 1.327 | 0.956 | 0.111 ± 0.095 | 0.942 | 2.578 ± 0.003 | 0.945 | 0.583 |
| F2 | 5.931 ± 1.125 | 0.945 | 0.074 ± 0.124 | 0.928 | 5.523 ± 1.424 | 0.945 | 0.104 ± 0.100 | 0.935 | 3.389 ± 0.896 | 0.926 | 0.693 |
| F3 | 7.094 ± 0.313 | 0.952 | 0.098 ± 0.107 | 0.932 | 6.392 ± 0.809 | 0.952 | 0.013 ± 0.077 | 0.942 | 1.865 ± 1.035 | 0.964 | 0.734 |
| F4 | 7.518 ± 0.013 | 0.955 | 0.109 ± 0.099 | 0.945 | 6.639 ± 0.635 | 0.955 | 0.150 ± 0.068 | 0.954 | 3.648 ± 1.462 | 0.978 | 0.843 |
| F5 | 7.991 ± 0.320 | 0.956 | 0.121 ± 0.091 | 0.942 | 7.043 ± 0.349 | 0.956 | 0.164 ± 0.057 | 0.953 | 1.564 ± 2.865 | 0.923 | 0.648 |
| F6 | 8.952 ± 1.004 | 0.951 | 0.148 ± 0.072 | 0.950 | 7.676 ± 0.097 | 0.950 | 0.197 ± 0.034 | 0.960 | 2.685 ± 3.865 | 0.895 | 0.567 |
| F7 | 9.413 ± 1.326 | 0.946 | 0.164 ± 0.060 | 0.949 | 7.995 ± 0.323 | 0.946 | 0.216 ± 0.021 | 0.961 | 3.234 ± 1.145 | 0.923 | 0.634 |
| F8 | 9.867 ± 1.677 | 0.941 | 0.181 ± 0.048 | 0.942 | 8.337 ± 0.565 | 0.941 | 0.235 ± 0.008 | 0.958 | 2.647 ± 2.235 | 0.914 | 0.589 |
| F9 | 10.495 ± 2.09 | 0.926 | 0.209 ± 0.028 | 0.938 | 8.783 ± 0.880 | 0.926 | 0.263 ± 0.012 | 0.953 | 1.564 ± 1.852 | 0.895 | 0.517 |
| SNo | Parameters | Methotrexate-Optimized Formulation |
|---|---|---|
| 1 | Cmax (ng/mL) | 177.38 ± 4.7 |
| 2 | Tmax (h) | 12 |
| 3 | K (h−1) | 0.041 ± 0.03 |
| 4 | t1/2 | 17.3 ± 2.21 |
| 5 | AUC0-24 (ng/mL.h) | 2856.51 ± 123.2 |
| 6 | MRT | 12.56 ± 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Latif, M.S.; Al-Harbi, F.F.; Nawaz, A.; Rashid, S.A.; Farid, A.; Mohaini, M.A.; Alsalman, A.J.; Hawaj, M.A.A.; Alhashem, Y.N. Formulation and Evaluation of Hydrophilic Polymer Based Methotrexate Patches: In Vitro and In Vivo Characterization. Polymers 2022, 14, 1310. https://doi.org/10.3390/polym14071310
Latif MS, Al-Harbi FF, Nawaz A, Rashid SA, Farid A, Mohaini MA, Alsalman AJ, Hawaj MAA, Alhashem YN. Formulation and Evaluation of Hydrophilic Polymer Based Methotrexate Patches: In Vitro and In Vivo Characterization. Polymers. 2022; 14(7):1310. https://doi.org/10.3390/polym14071310
Chicago/Turabian StyleLatif, Muhammad Shahid, Fatemah F. Al-Harbi, Asif Nawaz, Sheikh Abdur Rashid, Arshad Farid, Mohammad Al Mohaini, Abdulkhaliq J. Alsalman, Maitham A. Al Hawaj, and Yousef N. Alhashem. 2022. "Formulation and Evaluation of Hydrophilic Polymer Based Methotrexate Patches: In Vitro and In Vivo Characterization" Polymers 14, no. 7: 1310. https://doi.org/10.3390/polym14071310
APA StyleLatif, M. S., Al-Harbi, F. F., Nawaz, A., Rashid, S. A., Farid, A., Mohaini, M. A., Alsalman, A. J., Hawaj, M. A. A., & Alhashem, Y. N. (2022). Formulation and Evaluation of Hydrophilic Polymer Based Methotrexate Patches: In Vitro and In Vivo Characterization. Polymers, 14(7), 1310. https://doi.org/10.3390/polym14071310