ICU Admission Levels of Endothelial Biomarkers as Predictors of Mortality in Critically Ill COVID-19 Patients

 , , ,
, , ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of the Study Population
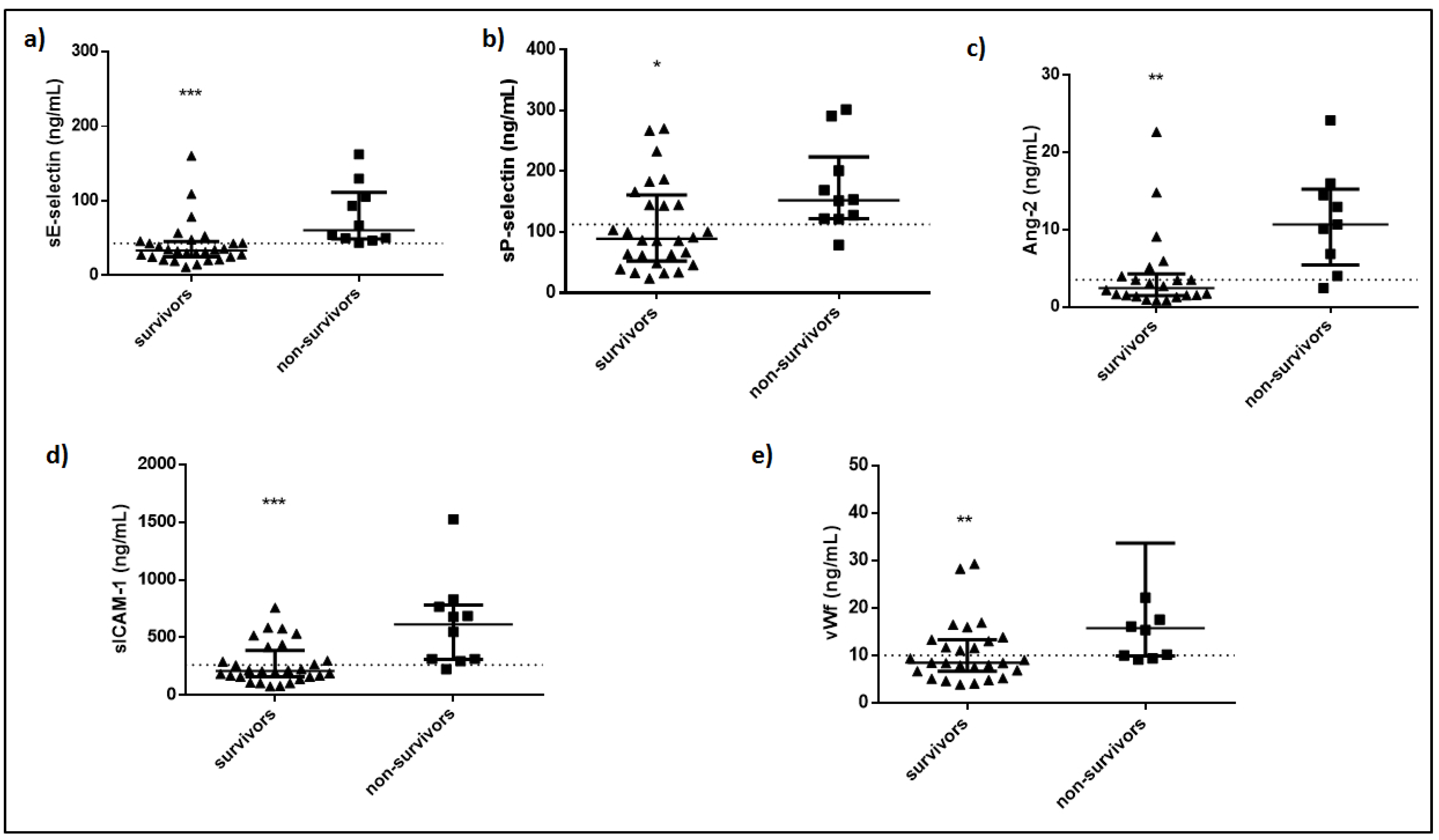
3.2. Baseline Levels of Soluble Endothelium-Related Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gustafson, D.; Raju, S.; Wu, R.; Ching, C.; Veitch, S.; Rathnakumar, K.; Boudreau, E.; Howe, K.L.; Fish, J.E. Overcoming Barriers: The Endothelium as a Linchpin of Coronavirus Disease 2019 Pathogenesis? Arter. Thromb. Vasc. Biol. 2020, 40, 1818–1829. [Google Scholar] [CrossRef] [PubMed]
- Chau, A.S.; Weber, A.G.; Maria, N.I.; Narain, S.; Liu, A.; Hajizadeh, N.; Malhotra, P.; Bloom, O.; Marder, G.; Kaplan, B. The Longitudinal Immune Response to Coronavirus Disease 2019: Chasing the Cytokine Storm. Arthritis Rheumatol. 2021, 73, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, M. COVID-19-driven endothelial damage: Complement, HIF-1, and ABL2 are potential pathways of damage and targets for cure. Ann. Hematol. 2020, 99, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Jung, F.; Krüger-Genge, A.; Franke, R.P.; Hufert, F.; Küpper, J.H. COVID-19 and the endothelium. Clin. Hemorheol. Microcirc. 2020, 75, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Goshua, G.; Pine, A.B.; Meizlish, M.L.; Chang, C.H.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, R.D.; Burns, A.J.; et al. Endotheliopathy in COVID-19-associated coagulopathy: Evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Hottz, E.D.; Azevedo-Quintanilha, I.G.; Palhinha, L.; Teixeira, L.; Barreto, E.A.; Pão, C.R.R.; Righy, C.; Franco, S.; Souza, T.M.L.; Kurtz, P.; et al. Platelet activation and platelet-monocyte aggregate formation trigger tissue factor expression in patients with severe COVID-19. Blood 2020, 136, 1330–1341. [Google Scholar] [CrossRef]
- Salamanna, F.; Maglio, M.; Landini, M.P.; Fini, M. Platelet functions and activities as potential hematologic parameters related to Coronavirus Disease 2019 (Covid-19). Platelets 2020, 31, 627–632. [Google Scholar] [CrossRef]
- Manne, B.K.; Denorme, F.; Middleton, E.A.; Portier, I.; Rowley, J.W.; Stubben, C.; Petrey, A.C.; Tolley, N.D.; Guo, L.; Cody, M.; et al. Platelet gene expression and function in patients with COVID-19. Blood 2020, 136, 1317–1329. [Google Scholar] [CrossRef]
- Zhang, S.; Liu, Y.; Wang, X.; Yang, L.; Li, H.; Wang, Y.; Liu, M.; Zhao, X.; Xie, Y.; Yang, Y.; et al. SARS-CoV-2 binds platelet ACE2 to enhance thrombosis in COVID-19. J. Hematol. Oncol. 2020, 13, 120. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Smadja, D.M.; Guerin, C.L.; Chocron, R.; Yatim, N.; Boussier, J.; Gendron, N.; Khider, L.; Hadjadj, J.; Goudot, G.; DeBuc, B.; et al. Angiopoietin-2 as a marker of endothelial activation is a good predictor factor for intensive care unit admission of COVID-19 patients. Angiogenesis 2020, 23, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Auld, S.C.; Caridi-Scheible, M.; Blum, J.M.; Robichaux, C.; Kraft, C.; Jacob, J.T.; Jabaley, C.S.; Carpenter, D.; Kaplow, R.; Hernandez-Romieu, A.C.; et al. ICU and Ventilator Mortality Among Critically Ill Adults With Coronavirus Disease 2019. Crit. Care Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Tu, L.; Zhu, P.; Mu, M.; Wang, R.; Yang, P.; Wang, X.; Hu, C.; Ping, R.; Hu, P.; et al. Clinical Features of 85 Fatal Cases of COVID-19 from Wuhan. A Retrospective Observational Study. Am. J. Respir. Crit. Care Med. 2020, 201, 1372–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, X.; Li, S.; Fang, M.; Hu, M.; Bian, Y.; Ling, J.; Yu, S.; Jing, L.; Li, D.; Huang, J. Acute Physiology and Chronic Health Evaluation II Score as a Predictor of Hospital Mortality in Patients of Coronavirus Disease 2019. Crit. Care Med. 2020, 48, e657–e665. [Google Scholar] [CrossRef] [PubMed]
- Maniatis, N.A.; Kotanidou, A.; Catravas, J.D.; Orfanos, S.E. Endothelial pathomechanisms in acute lung injury. Vasc. Pharmacol. 2008, 49, 119–133. [Google Scholar] [CrossRef]
- Vassiliou, A.G.; Kotanidou, A.; Dimopoulou, I.; Orfanos, S.E. Endothelial Damage in Acute Respiratory Distress Syndrome. Int. J. Mol. Sci. 2020, 21, 8793. [Google Scholar] [CrossRef]
- Karlsson, S.; Pettila, V.; Tenhunen, J.; Lund, V.; Hovilehto, S.; Ruokonen, E. Vascular Endothelial Growth Factor in Severe Sepsis and Septic Shock. Anesth. Analg. 2008, 106, 1820–1826. [Google Scholar] [CrossRef]
- Van der Flier, M.; van Leeuwen, H.J.; van Kessel, K.P.; Kimpen, J.L.; Hoepelman, A.I.; Geelen, S.P. Plasma vascular endothelial growth factor in severe sepsis. Shock 2005, 23, 35–38. [Google Scholar] [CrossRef]
- Zhang, R.Y.; Liu, Y.Y.; Li, L.; Cui, W.; Zhao, K.J.; Huang, W.C.; Gu, X.W.; Liu, W.; Wu, J.; Min, D.; et al. Increased Levels of Soluble Vascular Endothelial Cadherin are Associated with Poor Outcome in Severe Sepsis. J. Int. Med. Res. 2010, 38, 1497–1506. [Google Scholar] [CrossRef]
- Fiedler, U.; Augustin, H.G. Angiopoietins: A link between angiogenesis and inflammation. Trends Immunol. 2006, 27, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Roviezzo, F.; Tsigkos, S.; Kotanidou, A.; Bucci, M.; Brancaleone, V.; Cirino, G.; Papapetropoulos, A. Angiopoietin-2 Causes Inflammation in Vivo by Promoting Vascular Leakage. J. Pharmacol. Exp. Ther. 2005, 314, 738–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumpers, P.; Lukasz, A.; David, S.; Horn, R.; Hafer, C.; Faulhaber-Walter, R.; Fliser, D.; Haller, H.; Kielstein, J.T. Excess circulating angiopoietin-2 is a strong predictor of mortality in critically ill medical patients. Crit. Care 2008, 12, R147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricciuto, D.R.; Dos Santos, C.C.; Hawkes, M.; Toltl, L.J.; Conroy, A.L.; Rajwans, N.; Lafferty, E.I.; Cook, D.J.; Fox-Robichaud, A.; Kahnamoui, K.; et al. Angiopoietin-1 and angiopoietin-2 as clinically informative prognostic biomarkers of morbidity and mortality in severe sepsis. Crit. Care Med. 2011, 39, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Pine, A.B.; Meizlish, M.L.; Goshua, G.; Chang, C.H.; Zhang, H.; Bishai, J.; Bahel, P.; Patel, A.; Gbyli, R.; Kwan, J.M.; et al. Circulating markers of angiogenesis and endotheliopathy in COVID-19. Pulm. Circ. 2020, 10, 2045894020966547. [Google Scholar] [CrossRef] [PubMed]
- Muller, W.A. Leukocyte-endothelial-cell interactions in leukocyte transmigration and the inflammatory response. Trends Immunol. 2003, 24, 327–334. [Google Scholar] [CrossRef]
- Kayal, S.; Jais, J.P.; Aguini, N.; Chaudiere, J.; Labrousse, J. Elevated Circulating E-Selectin, Intercellular Adhesion Molecule 1, and von Willebrand Factor in Patients with Severe Infection. Am. J. Respir. Crit. Care Med. 1998, 157, 776–784. [Google Scholar] [CrossRef]
- Shapiro, N.I.; Schuetz, P.; Yano, K.; Sorasaki, M.; Parikh, S.M.; Jones, A.E.; Trzeciak, S.; Ngo, L.; Aird, W.C. The association of endothelial cell signaling, severity of illness, and organ dysfunction in sepsis. Crit. Care 2010, 14, R182. [Google Scholar] [CrossRef] [Green Version]
- Tong, M.; Jiang, Y.; Xia, D.; Xiong, Y.; Zheng, Q.; Chen, F.; Zou, L.; Xiao, W.; Zhu, Y. Elevated Expression of Serum Endothelial Cell Adhesion Molecules in COVID-19 Patients. J. Infect. Dis. 2020, 222, 894–898. [Google Scholar] [CrossRef]
- Tedder, T.F.; Steeber, D.A.; Chen, A.; Engel, P. The selectins: Vascular adhesion molecules. FASEB J. 1995, 9, 866–873. [Google Scholar] [CrossRef]
- Boldt, J.; Muller, M.; Kuhn, D.; Linke, L.C.; Hempelmann, G. Circulating adhesion molecules in the critically ill: A comparison between trauma and sepsis patients. Intensiv. Care Med. 1996, 22, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Boldt, J.; Wollbruck, M.; Kuhn, D.; Linke, L.C.; Hempelmann, G. Do plasma levels of circulating soluble adhesion molecules differ between surviving and nonsurviving critically ill patients? Chest 1995, 107, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Gearing, A.J.; Hemingway, I.; Pigott, R.; Hughes, J.; Rees, A.J.; Cashman, S.J. Soluble Forms of Vascular Adhesion Molecules, E-Selectin, ICAM-1, and VCAM-1: Pathological Significance. Ann. N. Y. Acad. Sci. 1992, 667, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Cugno, M.; Meroni, P.L.; Gualtierotti, R.; Griffini, S.; Grovetti, E.; Torri, A.; Lonati, P.; Grossi, C.; Borghi, M.O.; Novembrino, C.; et al. Complement activation and endothelial perturbation parallel COVID-19 severity and activity. J. Autoimmun. 2020, 116, 102560. [Google Scholar] [CrossRef] [PubMed]
- Sakamaki, F.; Ishizaka, A.; Handa, M.; Fujishima, S.; Urano, T.; Sayama, K.; Nakamura, H.; Kanazawa, M.; Kawashiro, T.; Katayama, M.; et al. Soluble form of P-selectin in plasma is elevated in acute lung injury. Am. J. Respir. Crit. Care Med. 1995, 151, 1821–1826. [Google Scholar] [CrossRef]
- Barrett, T.J.; Lee, A.H.; Xia, Y.; Lin, L.H.; Black, M.; Cotzia, P.; Hochman, J.; Berger, J.S. Platelet and Vascular Biomarkers Associate With Thrombosis and Death in Coronavirus Disease. Circ. Res. 2020, 127, 945–947. [Google Scholar] [CrossRef]
- Ladikou, E.E.; Sivaloganathan, H.; Milne, K.M.; Arter, W.E.; Ramasamy, R.; Saad, R.; Stoneham, S.M.; Philips, B.; Eziefula, A.C.; Chevassut, T. Von Willebrand factor (vWF): Marker of endothelial damage and thrombotic risk in COVID-19? Clin. Med. 2020, 20, e178–e182. [Google Scholar] [CrossRef]
- Rauch, A.; Labreuche, J.; Lassalle, F.; Goutay, J.; Caplan, M.; Charbonnier, L.; Rohn, A.; Jeanpierre, E.; Dupont, A.; Duhamel, A.; et al. Coagulation biomarkers are independent predictors of increased oxygen requirements in COVID-19. J. Thromb. Haemost. 2020, 18, 2942–2953. [Google Scholar] [CrossRef]
- Ward, S.E.; Curley, G.F.; Lavin, M.; Fogarty, H.; Karampini, E.; McEvoy, N.L.; Clarke, J.; Boylan, M.; Alalqam, R.; Worrall, A.P.; et al. Von Willebrand factor propeptide in severe coronavirus disease 2019 (COVID-19): Evidence of acute and sustained endothelial cell activation. Br. J. Haematol. 2020. [Google Scholar] [CrossRef]
- Fiedler, U.; Scharpfenecker, M.; Koidl, S.; Hegen, A.; Grunow, V.; Schmidt, J.M.; Kriz, W.; Thurston, G.; Augustin, H.G. The Tie-2 ligand Angiopoietin-2 is stored in and rapidly released upon stimulation from endothelial cell Weibel-Palade bodies. Blood 2004, 103, 4150–4156. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Survivors | Non–Survivors | p–Value | Reference Values |
|---|---|---|---|---|
| Number of patients, N | 28 | 10 | ||
| Vitals signs | ||||
| Heart rate (bpm), (mean ± SD) | 87 ± 17 | 102 ± 27 | 0.06 | |
| Mean arterial pressure (mmHg), (mean ± SD) | 81 ± 13 | 89 ± 23 | 0.2 | |
| Respiratory rate (breaths/min), (mean ± SD) | 21 ± 3 | 25 ± 4 | 0.004 * | |
| Temperature (°C), (mean ± SD) | 37.5 ± 0.9 | 37.3 ± 1.4 | 0.6 | |
| Laboratory data | ||||
| Hemoglobin, (mean ± SD) | 13 ± 2 | 13 ± 2 | 0.3 | 12–17.5 |
| Hematocrit, (mean ± SD) | 40 ± 4 | 39 ± 5 | 0.8 | 37–51 |
| White blood cell count (per μL), (mean ± SD) | 9121 ± 3982 | 12972 ± 5380 | 0.02 * | 4–10.5 × 103 |
| Neutrophlils (%), (mean ± SD) | 79.8 ± 7.1 | 84.2 ± 5.8 | 0.1 | 40–70 |
| Lymphocytes (%), (mean ± SD) | 13.9 ± 6.1 | 10.4 ± 4.6 | 0.1 | 25–45 |
| Platelets (per μL), (median, IQR) | 207,000 (144,000–258,000) | 267,000 (194,500–394,750) | 0.1 | 140–450 × 103 |
| PT (s), (median, IQR) | 13 (12–14) | 14 (13–14) | 0.9 | 11.0–12.5 |
| APTT (s), (mean ± SD) | 35 ± 6 | 35 ± 5 | 0.7 | 26–38 |
| INR, (median, IQR) | 1.08 (1.01–1.11) | 1.11 (1.04–1.17) | 0.3 | 0.8–1.1 |
| Creatinine (mg/dL), (mean ± SD) | 0.94 ± 0.28 | 1.21 ± 0.39 | 0.03 * | 0.6–1.4 |
| Glucose (mg/dL), (median, IQR) | 124 (109–189) | 178 (137–203) | 0.3 | 70–110 |
| Total bilirubin (mg/dL), (median, IQR) | 0.7 (0.4–0.8) | 0.6 (0.5–1.2) | 0.5 | <1 |
| Total protein (g/dL), (mean ± SD) | 6.3 ± 0.6 | 6.0 ± 1.0 | 0.2 | 6–8.2 |
| Albumin (g/dL), (mean ± SD) | 3.5 ± 0.6 | 3.2 ± 0.6 | 0.1 | 3.5–5.0 |
| Globulin (g/dL), (mean ± SD) | 2.7 ± 0.4 | 2.8 ± 0.7 | 0.8 | 2.3–3.5 |
| CKMB (IU/), (median, IQR) | 19 (16–37) | 24 (21–37) | 0.3 | 1–18 |
| CK (U/L), (median, IQR) | 166 (71–321) | 122 (67–575) | 0.8 | 10–173 |
| Fibrinogen (mg/dL), (mean ± SD) | 635 ± 165 | 626 ± 174 | 0.9 | 200–400 |
| D–dimers (µg/mL), (median, IQR) | 0.33 (0.20–0.59) | 0.52 (0.34–1.0) | 0.3 | <0.5 |
| CRP (mg/dL), (median, IQR) | 11.4 (5.9–19.0) | 13.5 (4.9–28.2) | 0.5 | <0.5 |
| γ–GT (IU/L), (median, IQR) | 47 (22–79) | 74 (26–175) | 0.2 | 7–49 |
| Urea (mg/dL), (median, IQR) | 31 (25–55) | 49 (30–93) | 0.1 | 10–50 |
| AST (IU/L), (median, IQR) | 42 (36–59) | 55 (33–70) | 0.3 | 5–37 |
| ALT (IU/L), (median, IQR) | 39 (23–56) | 48 (25–78) | 0.3 | 5–40 |
| Na+ (mEq/L), (mean ± SD) | 138 ± 5 | 142 ± 7 | 0.04 * | 135–147 |
| K+ (mEq/L), (mean ± SD) | 4.2 ± 0.5 | 4.4 ± 0.6 | 0.2 | 3.5–5.1 |
| ALP (U/L), (median, IQR) | 56 (43–76) | 91 (66–183) | 0.1 | 35–129 |
| LDH (U/L), (median, IQR) | 418 (335–629) | 533 (387–642) | 0.9 | <225 |
| Troponin (ng/mL), (median, IQR) | 12 (10–27) | 63 (13–133) | 0.2 | <14 |
| Amylase (U/L), (median, IQR) | 66 (53–114) | 66 (36–111) | 0.5 | 10–100 |
| Lactate (mmol/L), (mean ± SD) | 1.2 ± 0.4 | 1.2 ± 0.5 | 0.6 | <2.0 |
| Characteristics | Survivors | Non-Survivors | p-Value |
|---|---|---|---|
| Number of patients, N | 28 | 10 | |
| Age (years), (mean ± SD) | 62 ± 11 | 68 ± 10 | 0.2 |
| Sex, N (%) | 0.9 | ||
| Male | 23 (82.1%) | 8 (80.0%) | |
| Female | 5 (17.9%) | 2 (20.0%) | |
| Comorbidities, N (%) | 18 (64.3%) | 7 (70.0%) | 0.7 |
| Hypertension | 12 | 5 | |
| Diabetes | 3 | 2 | |
| CAD | 3 | 1 | |
| COPD | 1 | 0 | |
| Asthma | 0 | 1 | |
| Hyperlipidemia | 7 | 0 | |
| Hepatitis | 0 | 1 | |
| Sick days prior to ICU admission (mean ± SD) | 6 ± 3 | 7 ± 2 | 0.8 |
| Characteristics on ICU admission | |||
| APACHE II, (mean ± SD) SOFA, (mean ± SD) PaO2/FiO2 (mmHg), (mean ± SD) PCO2 (mmHg), (median, IQR) pH, (mean ± SD) HCO3 (mEq/L), (mean ± SD) | 14 ± 5 6 ± 3 202 ± 90 41 (33–47) 7.4 ± 0.1 25 ± 4 | 16 ± 4 9 ± 2 175 ± 71 48 (43–56) 7.3 ± 0.1 25 ± 5 | 0.2 0.02 * 0.5 0.06 0.04 * > 0.9 |
| Endothelial markers | |||
| sE-selectin (ng/mL), (median, IQR) sP-selectin (ng/mL), (median, IQR) Angiopoietin-1 (ng/mL), (median, IQR) Angiopoietin-2 (ng/mL), (median, IQR) Ang-2:Ang-1 (median, IQR) VEGF (ng/mL), (median, IQR) VE-cadherin (ng/mL), (median, IQR) sICAM (ng/mL), (median, IQR) vWf (ng/mL), (median, IQR) | 33.7 (25.0–45.5) 89.2 (52.4–161.2) 7.3 (3.2–22.4) 2.4 (1.5–4.3) 0.17 (0.04–0.35) 144.1 (118.2–269.6) 1337 (1005–1833) 211.2 (159.7–388.3) 8.52 (6.74–13.36) | 60.6 (49.2–111.6) 152.7 (122.1–223.7) 5.2 (1.5–22.4) 10.7 (5.4–15.2) 1.18 (0.18–2.80) 85.5 (45.9–265.8) 1238 (1125–2247) 614.5 (309.7–781.8) 15.76 (9.92–33.70) | <0.001 * 0.03 * 0.6 0.001 * 0.1 0.3 0.7 <0.001 * 0.008 * |
| COVID-19-targeted treatment | 28 (100.0%) | 10 (100.0%) | |
| Azithromycin/chloroquine/lopinavir/ritonavir Azithromycin/chloroquine Lopinavir/ritonavir/chloroquine Chloroquine Azithromycin Convalescent Plasma Other | 6 (21.4%) 9 (32.1%) 1 (3.6%) 2 (7.2%) 4 (14.3%) 3 (10.7%) 3 (10.7%) | 5 (50.0%) 2 (20.0%) 1 (10.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 2 (20.0%) | |
| Outcomes | |||
| LoS in the ICU (days), (median, IQR) Mechanical ventilation, N (%) Duration of mechanical ventilation (days), (median, IQR) | 14 (11–30) 20 (71.4%) 12 (4–35) | 29 (17–40) 10 (100.0%) 26 (17–40) | 0.5 0.06 0.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassiliou, A.G.; Keskinidou, C.; Jahaj, E.; Gallos, P.; Dimopoulou, I.; Kotanidou, A.; Orfanos, S.E. ICU Admission Levels of Endothelial Biomarkers as Predictors of Mortality in Critically Ill COVID-19 Patients. Cells 2021, 10, 186. https://doi.org/10.3390/cells10010186
Vassiliou AG, Keskinidou C, Jahaj E, Gallos P, Dimopoulou I, Kotanidou A, Orfanos SE. ICU Admission Levels of Endothelial Biomarkers as Predictors of Mortality in Critically Ill COVID-19 Patients. Cells. 2021; 10(1):186. https://doi.org/10.3390/cells10010186
Chicago/Turabian StyleVassiliou, Alice G., Chrysi Keskinidou, Edison Jahaj, Parisis Gallos, Ioanna Dimopoulou, Anastasia Kotanidou, and Stylianos E. Orfanos. 2021. "ICU Admission Levels of Endothelial Biomarkers as Predictors of Mortality in Critically Ill COVID-19 Patients" Cells 10, no. 1: 186. https://doi.org/10.3390/cells10010186
APA StyleVassiliou, A. G., Keskinidou, C., Jahaj, E., Gallos, P., Dimopoulou, I., Kotanidou, A., & Orfanos, S. E. (2021). ICU Admission Levels of Endothelial Biomarkers as Predictors of Mortality in Critically Ill COVID-19 Patients. Cells, 10(1), 186. https://doi.org/10.3390/cells10010186