
Targeting Myeloid-Derived Suppressor Cells in Ovarian Cancer


Abstract
:1. Introduction
2. Definition of MDSC
3. Functions of MDSCs
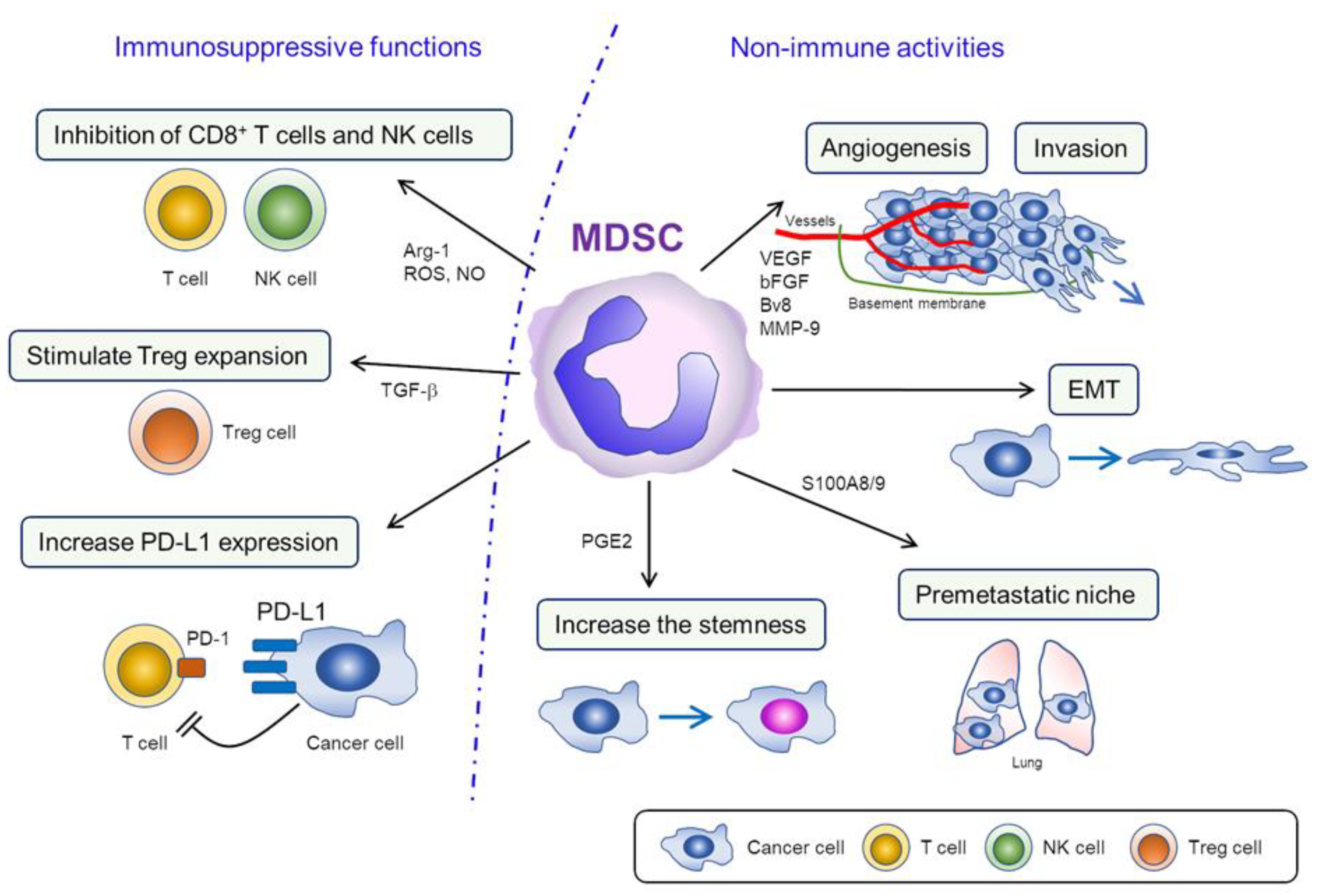
3.1. Immunosuppressive Functions of MDSCs
3.2. Nonimmune Activities of MDSC
4. MDSC Generation and Recruitment
4.1. MDSC Generation and Activation
4.2. Recruitment of MDSC into TME
5. The Clinical Significance of MDSC in Ovarian Cancer Patients
5.1. The Frequency of MDSCs as a Prognostic Indicator or a Biomarker of Tumor Progression in Ovarian Cancer Patients
5.2. In Vitro and In Vivo Investigation of MDSC in Ovarian Cancer
6. Targeting MDSCs in Ovarian Cancer
6.1. Preclinical Investigation of MDSC-Targeting Therapies
6.2. Strategy to Inhibit Human MDSCs
6.3. Clinical Trials Targeting MDSCs in Cancer Patients
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matulonis, U.A.; Sood, A.K.; Fallowfield, L.; Howitt, B.E.; Sehouli, J.; Karlan, B.Y. Ovarian cancer. Nat. Rev. Dis. Primers 2016, 2, 16061. [Google Scholar] [CrossRef]
- Jayson, G.C.; Kohn, E.C.; Kitchener, H.C.; Ledermann, J.A. Ovarian cancer. Lancet 2014, 384, 1376–1388. [Google Scholar] [CrossRef]
- Mahoney, K.M.; Rennert, P.D.; Freeman, G.J. Combination cancer immunotherapy and new immunomodulatory targets. Nat. Rev. Drug Discov. 2015, 14, 561–584. [Google Scholar] [CrossRef] [PubMed]
- Zamarin, D.; Burger, R.A.; Sill, M.W.; Powell, D.J., Jr.; Lankes, H.A.; Feldman, M.D.; Zivanovic, O.; Gunderson, C.; Ko, E.; Mathews, C.; et al. Randomized Phase II Trial of Nivolumab Versus Nivolumab and Ipilimumab for Recurrent or Persistent Ovarian Cancer: An NRG Oncology Study. J. Clin. Oncol. 2020, 38, 1814–1823. [Google Scholar] [CrossRef]
- Paijens, S.T.; Leffers, N.; Daemen, T.; Helfrich, W.; Boezen, H.M.; Cohlen, B.J.; Melief, C.J.; de Bruyn, M.; Nijman, H.W. Antigen-specific active immunotherapy for ovarian cancer. Cochrane Database Syst. Rev. 2018, 9, CD007287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Conejo-Garcia, J.R.; Katsaros, D.; Gimotty, P.A.; Massobrio, M.; Regnani, G.; Makrigiannakis, A.; Gray, H.; Schlienger, K.; Liebman, M.N.; et al. Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N. Engl. J. Med. 2003, 348, 203–213. [Google Scholar] [CrossRef] [Green Version]
- Dunn, G.P.; Bruce, A.T.; Ikeda, H.; Old, L.J.; Schreiber, R.D. Cancer immunoediting: From immunosurveillance to tumor escape. Nat. Immunol. 2002, 3, 991–998. [Google Scholar] [CrossRef]
- Sonnenfeld, A. Leukamische reaktiones bei carcinoma. Zeitschrift f Klin Med 1929, 111, 108. [Google Scholar]
- Gabrilovich, D.I.; Bronte, V.; Chen, S.H.; Colombo, M.P.; Ochoa, A.; Ostrand-Rosenberg, S.; Schreiber, H. The terminology issue for myeloid-derived suppressor cells. Cancer Res. 2007, 67, 425, author reply 426. [Google Scholar] [CrossRef] [Green Version]
- Bronte, V.; Brandau, S.; Chen, S.H.; Colombo, M.P.; Frey, A.B.; Greten, T.F.; Mandruzzato, S.; Murray, P.J.; Ochoa, A.; Ostrand-Rosenberg, S.; et al. Recommendations for myeloid-derived suppressor cell nomenclature and characterization standards. Nat. Commun. 2016, 7, 12150. [Google Scholar] [CrossRef] [Green Version]
- Condamine, T.; Dominguez, G.A.; Youn, J.I.; Kossenkov, A.V.; Mony, S.; Alicea-Torres, K.; Tcyganov, E.; Hashimoto, A.; Nefedova, Y.; Lin, C.; et al. Lectin-type oxidized LDL receptor-1 distinguishes population of human polymorphonuclear myeloid-derived suppressor cells in cancer patients. Sci. Immunol. 2016, 1, aaf8943. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.N.; Yi, N.; Zhang, T.W.; Zhang, L.L.; Wu, X.; Liu, M.; Fu, Y.J.; He, S.J.; Jiang, Y.J.; Ding, H.B.; et al. Myeloid-Derived Suppressor Cells Associated With Disease Progression in Primary HIV Infection: PD-L1 Blockade Attenuates Inhibition. J. Acquir. Immune Defic. Syndr. 2017, 76, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Mabuchi, S.; Matsumoto, Y.; Kawano, M.; Minami, K.; Seo, Y.; Sasano, T.; Takahashi, R.; Kuroda, H.; Hisamatsu, T.; Kakigano, A.; et al. Uterine cervical cancer displaying tumor-related leukocytosis: A distinct clinical entity with radioresistant feature. J. Natl. Cancer Inst. 2014, 106, dju147. [Google Scholar] [CrossRef] [Green Version]
- Sasano, T.; Mabuchi, S.; Kozasa, K.; Kuroda, H.; Kawano, M.; Takahashi, R.; Komura, N.; Yokoi, E.; Matsumoto, Y.; Hashimoto, K.; et al. The Highly Metastatic Nature of Uterine Cervical/Endometrial Cancer Displaying Tumor-Related Leukocytosis: Clinical and Preclinical Investigations. Clin. Cancer Res. 2018, 24, 4018–4029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mabuchi, S.; Komura, N.; Sasano, T.; Shimura, K.; Yokoi, E.; Kozasa, K.; Kuroda, H.; Takahashi, R.; Kawano, M.; Matsumoto, Y.; et al. Pretreatment tumor-related leukocytosis misleads positron emission tomography-computed tomography during lymph node staging in gynecological malignancies. Nat. Commun. 2020, 11, 1364. [Google Scholar] [CrossRef] [PubMed]
- Komura, N.; Mabuchi, S.; Shimura, K.; Yokoi, E.; Kozasa, K.; Kuroda, H.; Takahashi, R.; Sasano, T.; Kawano, M.; Matsumoto, Y.; et al. The role of myeloid-derived suppressor cells in increasing cancer stem-like cells and promoting PD-L1 expression in epithelial ovarian cancer. Cancer Immunol. Immunother. 2020, 69, 2477–2499. [Google Scholar] [CrossRef]
- Solito, S.; Marigo, I.; Pinton, L.; Damuzzo, V.; Mandruzzato, S.; Bronte, V. Myeloid-derived suppressor cell heterogeneity in human cancers. Ann. N. Y. Acad. Sci. 2014, 1319, 47–65. [Google Scholar] [CrossRef]
- Vasquez-Dunddel, D.; Pan, F.; Zeng, Q.; Gorbounov, M.; Albesiano, E.; Fu, J.; Blosser, R.L.; Tam, A.J.; Bruno, T.; Zhang, H.; et al. STAT3 regulates arginase-I in myeloid-derived suppressor cells from cancer patients. J. Clin. Investig. 2013, 124, 1580–1589. [Google Scholar] [CrossRef] [Green Version]
- Waight, J.D.; Netherby, C.; Hencen, M.L.; Miller, A.; Hu, Q.; Liu, S.; Bogner, P.N.; Farren, M.R.; Lee, K.P.; Liu, K.; et al. Myeloid-derived suppressor cell development is regulated by a STAT/IRF-8 axis. J. Clin. Investig. 2013, 123, 4464–4478. [Google Scholar] [CrossRef]
- Sonda, N.; Simonato, F.; Peranzoni, E.; Calì, B.; Bortoluzzi, S.; Bisognin, A.; Wang, E.; Marincola, F.M.; Naldini, L.; Gentner, B.; et al. miR-142-3p prevents macrophage differentiation during cancer-induced myelopoiesis. Immunity 2013, 38, 1236–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Ubreva, J.; Català-Moll, F.; Obermajer, N.; Álvarez-Errico, D.; Ramirez, R.N.; Company, C.; Vento-Tormo, R.; Moreno-Bueno, G.; Edwards, R.P.; Mortazavi, A.; et al. Prostaglandin E2 Leads to the Acquisition of DNMT3A-Dependent Tolerogenic Functions in Human Myeloid-Derived Suppressor Cells. Cell Rep. 2017, 21, 154–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Wang, J.; Wu, W.; Gao, H.; Liu, N.; Zhan, G.; Li, L.; Han, L.; Guo, X. Myeloid-derived suppressor cells promote epithelial ovarian cancer cell stemness by inducing the CSF2/p-STAT3 signalling pathway. FEBS J. 2020, 287, 5128–5235. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Botesteanu, D.A.; Tomita, Y.; Yuno, A.; Lee, M.J.; Kohn, E.C.; Annunziata, C.M.; Matulonis, U.; MacDonald, L.A.; Nair, J.R.; et al. Patients with BRCA mutated ovarian cancer may have fewer circulating MDSC and more peripheral CD8+ T cells compared with women with BRCA wild-type disease during the early disease course. Oncol. Lett. 2019, 18, 3914–3924. [Google Scholar] [CrossRef] [Green Version]
- Coosemans, A.; Baert, T.; Ceusters, J.; Busschaert, P.; Landolfo, C.; Verschuere, T.; Van Rompuy, A.S.; Vanderstichele, A.; Froyman, W.; Neven, P.; et al. Myeloid-derived suppressor cells at diagnosis may discriminate between benign and malignant ovarian tumors. Int. J. Gynecol. Cancer. 2019, 29, 1381–1388. [Google Scholar] [CrossRef]
- Okła, K.; Czerwonka, A.; Wawruszak, A.; Bobiński, M.; Bilska, M.; Tarkowski, R.; Bednarek, W.; Wertel, I.; Kotarski, J. Clinical Relevance and Immunosuppressive Pattern of Circulating and Infiltrating Subsets of Myeloid-Derived Suppressor Cells (MDSCs) in Epithelial Ovarian Cancer. Front. Immunol. 2019, 10, 691. [Google Scholar] [CrossRef] [Green Version]
- Santegoets, S.J.A.M.; de Groot, A.F.; Dijkgraaf, E.M.; Simões, A.M.C.; van der Noord, V.E.; van Ham, J.J.; Welters, M.J.P.; Kroep, J.R.; van der Burg, S.H. The blood mMDSC to DC ratio is a sensitive and easy to assess independent predictive factor for epithelial ovarian cancer survival. Oncoimmunology 2018, 7, e1465166. [Google Scholar] [CrossRef] [Green Version]
- Taki, M.; Abiko, K.; Baba, T.; Hamanishi, J.; Yamaguchi, K.; Murakami, R.; Yamanoi, K.; Horikawa, N.; Hosoe, Y.; Nakamura, E.; et al. Snail promotes ovarian cancer progression by recruiting myeloid-derived suppressor cells via CXCR2 ligand upregulation. Nat. Commun. 2018, 9, 1685. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Wang, L.; Li, J.; Fan, Z.; Yang, L.; Zhang, Z.; Zhang, C.; Yue, D.; Qin, G.; Zhang, T.; et al. Metformin-Induced Reduction of CD39 and CD73 Blocks Myeloid-Derived Suppressor Cell Activity in Patients with Ovarian Cancer. Cancer Res. 2018, 78, 1779–1791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horikawa, N.; Abiko, K.; Matsumura, N.; Hamanishi, J.; Baba, T.; Yamaguchi, K.; Yoshioka, Y.; Koshiyama, M.; Konishi, I. Expression of Vascular Endothelial Growth Factor in Ovarian Cancer Inhibits Tumor Immunity through the Accumulation of Myeloid-Derived Suppressor Cells. Clin. Cancer Res. 2017, 23, 587–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.; Deng, Z.; Peng, Y.; Han, L.; Liu, J.; Wang, L.; Li, B.; Zhao, J.; Jiao, S.; Wei, H. Ascites-derived IL-6 and IL-10 synergistically expand CD14+HLA-DR−/low myeloid-derived suppressor cells in ovarian cancer patients. Oncotarget 2017, 8, 76843–76856. [Google Scholar] [CrossRef] [Green Version]
- Cui, T.X.; Kryczek, I.; Zhao, L.; Zhao, E.; Kuick, R.; Roh, M.H.; Vatan, L.; Szeliga, W.; Mao, Y.; Thomas, D.G.; et al. Myeloid-derived suppressor cells enhance stemness of cancer cells by inducing microRNA101 and suppressing the corepressor CtBP2. Immunity 2013, 39, 611–621. [Google Scholar] [CrossRef] [Green Version]
- Obermajer, N.; Muthuswamy, R.; Odunsi, K.; Edwards, R.P.; Kalinski, P. PGE(2)-induced CXCL12 production and CXCR4 expression controls the accumulation of human MDSCs in ovarian cancer environment. Cancer Res. 2011, 71, 7463–7470. [Google Scholar] [CrossRef] [Green Version]
- Tew, W.P.; Lacchetti, C.; Ellis, A.; Maxian, K.; Banerjee, S.; Bookman, M.; Jones, M.B.; Lee, J.M.; Lheureux, S.; Liu, J.F.; et al. PARP Inhibitors in the Management of Ovarian Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 38, 3468–3493. [Google Scholar] [CrossRef]
- Horikawa, N.; Abiko, K.; Matsumura, N.; Baba, T.; Hamanishi, J.; Yamaguchi, K.; Murakami, R.; Taki, M.; Ukita, M.; Hosoe, Y.; et al. Anti-VEGF therapy resistance in ovarian cancer is caused by GM-CSF-induced myeloid-derived suppressor cell recruitment. Br. J. Cancer 2020, 122, 778–788. [Google Scholar] [CrossRef]
- Zeng, Y.; Li, B.; Liang, Y.; Reeves, P.M.; Qu, X.; Ran, C.; Liu, Q.; Callahan, M.V.; Sluder, A.E.; Gelfand, J.A.; et al. Dual blockade of CXCL12-CXCR4 and PD-1-PD-L1 pathways prolongs survival of ovarian tumor-bearing mice by prevention of immunosuppression in the tumor microenvironment. FASEB J. 2019, 33, 6596–6608. [Google Scholar] [CrossRef]
- Baert, T.; Vankerckhoven, A.; Riva, M.; Van Hoylandt, A.; Thirion, G.; Holger, G.; Mathivet, T.; Vergote, I.; Coosemans, A. Myeloid Derived Suppressor Cells: Key Drivers of Immunosuppression in Ovarian Cancer. Front. Immunol. 2019, 10, 1273. [Google Scholar] [CrossRef] [PubMed]
- Soong, R.S.; Anchoori, R.K.; Yang, B.; Yang, A.; Tseng, S.H.; He, L.; Tsai, Y.C.; Roden, R.B.; Hung, C.F. RPN13/ADRM1 inhibitor reverses immunosuppression by myeloid-derived suppressor cells. Oncotarget 2016, 7, 68489–68502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, E.T.; Minton, A.R.; Peters, M.C.; van Ryn, J.; Gilmour, S.K. Thrombin inhibition and cisplatin block tumor progression in ovarian cancer by alleviating the immunosuppressive microenvironment. Oncotarget 2016, 7, 85291–85305. [Google Scholar] [CrossRef]
- Lamichhane, P.; Karyampudi, L.; Shreeder, B.; Krempski, J.; Bahr, D.; Daum, J.; Kalli, K.R.; Goode, E.L.; Block, M.S.; Cannon, M.J.; et al. IL10 Release upon PD-1 Blockade Sustains Immunosuppression in Ovarian Cancer. Cancer Res. 2017, 77, 6667–6678. [Google Scholar] [CrossRef] [Green Version]
- Walton, J.; Blagih, J.; Ennis, D.; Leung, E.; Dowson, S.; Farquharson, M.; Tookman, L.A.; Orange, C.; Athineos, D.; Mason, S.; et al. CRISPR/Cas9-Mediated Trp53 and Brca2 Knockout to Generate Improved Murine Models of Ovarian High-Grade Serous Carcinoma. Cancer Res. 2016, 76, 6118–6129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, E.; Kapoor, V.; Jassar, A.S.; Kaiser, L.R.; Albelda, S.M. Gemcitabine selectively eliminates splenic Gr-1+/CD11b+ myeloid suppressor cells in tumor-bearing animals and enhances antitumor immune activity. Clin. Cancer Res. 2005, 11, 6713–6721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.; Mignot, G.; Chalmin, F.; Ladoire, S.; Bruchard, M.; Chevriaux, A.; Martin, F.; Apetoh, L.; Rébé, C.; Ghiringhelli, F. 5-Fluorouracil selectively kills tumor-associated myeloid-derived suppressor cells resulting in enhanced T cell-dependent antitumor immunity. Cancer Res. 2010, 70, 3052–3061. [Google Scholar] [CrossRef] [Green Version]
- Arrieta, O.; González-De la Rosa, C.H.; Aréchaga-Ocampo, E.; Villanueva-Rodríguez, G.; Cerón-Lizárraga, T.L.; Martínez-Barrera, L.; Vázquez-Manríquez, M.E.; Ríos-Trejo, M.A.; Alvarez-Avitia, M.A.; Hernández-Pedro, N.; et al. Randomized phase II trial of All-trans-retinoic acid with chemotherapy based on paclitaxel and cisplatin as first-line treatment in patients with advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 3463–3471. [Google Scholar] [CrossRef]
- Tseng, C.W.; Hung, C.F.; Alvarez, R.D.; Trimble, C.; Huh, W.K.; Kim, D.; Chuang, C.M.; Lin, C.T.; Tsai, Y.C.; He, L.; et al. Pretreatment with cisplatin enhances E7-specific CD8+ T-Cell-mediated antitumor immunity induced by DNA vaccination. Clin. Cancer Res. 2008, 14, 3185–3192. [Google Scholar] [CrossRef] [Green Version]
- Kodumudi, K.N.; Woan, K.; Gilvary, D.L.; Sahakian, E.; Wei, S.; Djeu, J.Y. A novel chemoimmunomodulating property of docetaxel: Suppression of myeloid-derived suppressor cells in tumor bearers. Clin. Cancer Res. 2010, 16, 4583–4594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuroda, H.; Mabuchi, S.; Kozasa, K.; Yokoi, E.; Matsumoto, Y.; Komura, N.; Kawano, M.; Hashimoto, K.; Sawada, K.; Kimura, T. PM01183 inhibits myeloid-derived suppressor cells in vitro and in vivo. Immunotherapy 2017, 9, 805–817. [Google Scholar] [CrossRef]
- Ko, J.S.; Rayman, P.; Ireland, J.; Swaidani, S.; Li, G.; Bunting, K.D.; Rini, B.; Finke, J.H.; Cohen, P.A. Direct and differential suppression of myeloid-derived suppressor cell subsets by sunitinib is compartmentally constrained. Cancer Res. 2010, 70, 3526–3536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heine, A.; Schilling, J.; Grünwald, B.; Krüger, A.; Gevensleben, H.; Held, S.A.; Garbi, N.; Kurts, C.; Brossart, P.; Knolle, P.; et al. The induction of human myeloid derived suppressor cells through hepatic stellate cells is dose-dependently inhibited by the tyrosine kinase inhibitors nilotinib, dasatinib and sorafenib, but not sunitinib. Cancer Immunol. Immunother. 2016, 65, 273–282. [Google Scholar] [CrossRef]
- Sumida, K.; Wakita, D.; Narita, Y.; Masuko, K.; Terada, S.; Watanabe, K.; Satoh, T.; Kitamura, H.; Nishimura, T. Anti-IL-6 receptor mAb eliminates myeloid-derived suppressor cells and inhibits tumor growth by enhancing T-cell responses. Eur. J. Immunol. 2012, 42, 2060–2072. [Google Scholar] [CrossRef]
- Xu, J.; Escamilla, J.; Mok, S.; David, J.; Priceman, S.; West, B.; Bollag, G.; McBride, W.; Wu, L. CSF1R signaling blockade stanches tumor-infiltrating myeloid cells and improves the efficacy of radiotherapy in prostate cancer. Cancer Res. 2013, 73, 2782–2794. [Google Scholar] [CrossRef] [Green Version]
- DeNardo, D.G.; Brennan, D.J.; Rexhepaj, E.; Ruffell, B.; Shiao, S.L.; Madden, S.F.; Gallagher, W.M.; Wadhwani, N.; Keil, S.D.; Junaid, S.A.; et al. Leukocyte complexity predicts breast cancer survival and functionally regulates response to chemotherapy. Cancer Discov. 2011, 1, 54–67. [Google Scholar] [CrossRef] [Green Version]
- Shen, L.; Sundstedt, A.; Ciesielski, M.; Miles, K.M.; Celander, M.; Adelaiye, R.; Orillion, A.; Ciamporcero, E.; Ramakrishnan, S.; Ellis, L.; et al. Tasquinimod modulates suppressive myeloid cells and enhances cancer immunotherapies in murine models. Cancer Immunol. Res. 2015, 3, 136–148. [Google Scholar] [CrossRef] [Green Version]
- Schilling, B.; Sucker, A.; Griewank, K.; Zhao, F.; Weide, B.; Görgens, A.; Giebel, B.; Schadendorf, D.; Paschen, A. Vemurafenib reverses immunosuppression by myeloid derived suppressor cells. Int. J. Cancer 2013, 133, 1653–1663. [Google Scholar] [CrossRef]
- Melani, C.; Sangaletti, S.; Barazzetta, F.M.; Werb, Z.; Colombo, M.P. Amino-biphosphonate-mediated MMP-9 inhibition breaks the tumor-bone marrow axis responsible for myeloid-derived suppressor cell expansion and macrophage infiltration in tumor stroma. Cancer Res. 2007, 67, 11438–11446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serafini, P.; Meckel, K.; Kelso, M.; Noonan, K.; Califano, J.; Koch, W.; Dolcetti, L.; Bronte, V.; Borrello, I. Phosphodiesterase-5 inhibition augments endogenous antitumor immunity by reducing myeloid-derived suppressor cell function. J. Exp. Med. 2006, 203, 2691–2702. [Google Scholar] [CrossRef]
- Kujawski, M.; Kortylewski, M.; Lee, H.; Herrmann, A.; Kay, H.; Yu, H. Stat3 mediates myeloid cell-dependent tumor angiogenesis in mice. J. Clin. Investig. 2008, 118, 3367–3377. [Google Scholar] [CrossRef] [PubMed]
- Bu, L.L.; Li, Y.C.; Yu, G.T.; Liu, J.F.; Deng, W.W.; Zhang, W.F.; Zhang, L.; Sun, Z.J. Targeting phosphorylation of STAT3 delays tumor growth in HPV-negative anal squamous cell carcinoma mouse model. Sci. Rep. 2017, 7, 6629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poschke, I.; Mougiakakos, D.; Hansson, J.; Masucci, G.V.; Kiessling, R. Immature immunosuppressive CD14+HLA-DR−/low cells in melanoma patients are Stat3hi and overexpress CD80, CD83, and DC-sign. Cancer Res. 2010, 70, 4335–4345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.; Zhao, Y.; Wang, H.; Li, Y.; Shao, L.; Wang, R.; Lu, J.; Yang, Z.; Wang, J.; Zhao, Y. mTOR masters monocytic myeloid-derived suppressor cells in mice with allografts or tumors. Sci. Rep. 2016, 6, 20250. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.J.; Moore, E.C.; Clavijo, P.E.; Friedman, J.; Cash, H.; Chen, Z.; Silvin, C.; Van Waes, C.; Allen, C. Anti-PD-L1 Efficacy Can Be Enhanced by Inhibition of Myeloid-Derived Suppressor Cells with a Selective Inhibitor of PI3Kδ/γ. Cancer Res. 2017, 77, 2607–2619. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Shen, L.; Liu, Q.; Hou, L.; Huang, L. Inhibiting PI3 kinase-γ in both myeloid and plasma cells remodels the suppressive tumor microenvironment in desmoplastic tumors. J. Control. Release 2019, 309, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Veltman, J.D.; Lambers, M.E.; van Nimwegen, M.; Hendriks, R.W.; Hoogsteden, H.C.; Aerts, J.G.; Hegmans, J.P. COX-2 inhibition improves immunotherapy and is associated with decreased numbers of myeloid-derived suppressor cells in mesothelioma. Celecoxib influences MDSC function. BMC Cancer 2010, 10, 464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wesolowski, R.; Markowitz, J.; Carson, W.E., III. Myeloid derived suppressor cells—A new therapeutic target in the treatment of cancer. J. Immunother. Cancer 2013, 1, 10. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, A.; Fukumoto, T.; Zhang, R.; Gabrilovich, D. Selective targeting of different populations of myeloid-derived suppressor cells by histone deacetylase inhibitors. Cancer Immunol. Immunother. 2020, 69, 1929–1936. [Google Scholar] [CrossRef] [PubMed]
- Maeda, A.; Eguchi, H.; Nakahata, K.; Lo, P.C.; Yamanaka, K.; Kawamura, T.; Matsuura, R.; Sakai, R.; Asada, M.; Okuyama, H.; et al. Monocytic MDSCs regulate macrophage-mediated xenogenic cytotoxicity. Transpl. Immunol. 2015, 33, 140–145. [Google Scholar] [CrossRef]
- Li, B.H.; Garstka, M.A.; Li, Z.F. Chemokines and their receptors promoting the recruitment of myeloid-derived suppressor cells into the tumor. Mol. Immunol. 2020, 117, 201–215. [Google Scholar] [CrossRef]
- Flores-Toro, J.A.; Luo, D.; Gopinath, A.; Sarkisian, M.R.; Campbell, J.J.; Charo, I.F.; Singh, R.; Schall, T.J.; Datta, M.; Jain, R.K.; et al. CCR2 inhibition reduces tumor myeloid cells and unmasks a checkpoint inhibitor effect to slow progression of resistant murine gliomas. Proc. Natl. Acad. Sci. USA 2020, 117, 1129–1138. [Google Scholar] [CrossRef] [PubMed]
- Nefedova, Y.; Fishman, M.; Sherman, S.; Wang, X.; Beg, A.A.; Gabrilovich, D.I. Mechanism of all-trans retinoic acid effect on tumor-associated myeloid-derived suppressor cells. Cancer Res. 2007, 67, 11021–11028. [Google Scholar] [CrossRef] [Green Version]
- Lathers, D.M.; Clark, J.I.; Achille, N.J.; Young, M.R. Phase 1B study to improve immune responses in head and neck cancer patients using escalating doses of 25-hydroxyvitamin D3. Cancer Immunol. Immunother. 2004, 53, 422–430. [Google Scholar] [CrossRef]
- Cheng, P.; Kumar, V.; Liu, H.; Youn, J.I.; Fishman, M.; Sherman, S.; Gabrilovich, D. Effects of notch signaling on regulation of myeloid cell differentiation in cancer. Cancer Res. 2014, 74, 141–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCT04022616, NCT02868255, NCT02735512, NCT02664883, NCT04387682, NCT02669173, NCT01803152, NCT03525925, NCT02637531, NCT03161431. Clinical Trials.gov. A Service of the U.S. National Institute of Health. Available online: http://www.clinicaltrials.gov (accessed on 21 November 2020).


{kind=link}
| Author/Year | Histology | Samples Examined | Findings from Patient-Derived Samples |
|---|---|---|---|
| Komura et al. 2020 [17] | EOC | PBMC, Tumor | The proportion of MDSC in the peripheral blood or ovarian tumor was positively associated with the number of leukocytes and tumor G-CSF expression. |
| Li et al. 2020 [23] | Benign ovarian tumor EOC | PBMC | PMN-MDSC and M-MDSC were increased in ovarian cancer patients. |
| Lee et al. 2019 [24] | Stage III/IV or recurrent HGSOC | PBMC | gBRCAm was associated with increased CD8+ T cells and decreased MDSC. |
| Coosemans et al. 2019 [25] | Benign/borderline ovarian tumor or invasive EOC | PBMC | Increased MDSC was found to be an independent predictor of malignant disease. |
| Okta et al. 2019 [26] | Healthy donner EOC | PBMC, Tumor, Ascites | PMN-MDSC and M-MDSC were increased in ovarian cancer patients. Increased tumor-infiltrating M-MDSC was associated with advanced stage and decreased survival. |
| Santegoets et al. 2018 [27] | Healthy donner EOC | PBMC | M-MDSC was increased in ovarian cancer patients. Increased M-MDSC was associated with decreased survival. |
| Taki et al. 2018 [28] | EOC | Tumor | Increased tumor-infiltrating MDSC was associated with the high Snail expression. |
| Li et al. 2018 [29] | Healthy donner EOC | PBMC | Metformin treatment correlated with longer survival in diabetic patients with ovarian cancer, which was accompanied by a reduction in the circulating MDSC and a concomitant increase in the CD8+ T cells. |
| Rodrıguez-Ubreva et al. 2017 [22] | EOC | PBMC, Ascites | MDSC from patients displayed the MDSC-specific hypermethylation signatures. |
| Horikawa et al. 2017 [30] | HGSOC | Ascites | Increased MDSC was significantly associated with decreased intratumoral CD8+ T-cell infiltration and shorter survival. |
| Wu et al. 2017 [31] | Healthy donner EOC | PBMC, Ascites | M-MDSC was increased in the blood and ascites of ovarian cancer patients. Increased M-MDSC was associated with advanced stage, decreased survival, and increased serum IL-6/IL-10 concentration. |
| Cui et al. 2013 [32] | EOC | Tumor | Increased tumor-infiltrating MDSC was significantly associated with shorter survival. |
| Obermajer et al. 2011. [33] | EOC | Ascites | M-MDSC was increased in the ascites of ovarian cancer patients. |
| Author/Year | Experimental Models Employed | Findings from in vitro/in vivo Studies | |
|---|---|---|---|
| Komura et al. 2020 [17] | Cell line | A2780, HM-1 cells | MDSC inhibited the activity of CD8+ T cells. PGE2 produced by tumor-derived G-CSF-induced MDSC increased the stem cell-like properties and tumor PD-L1 expression in ovarian cancer. Anti-Gr-1 antibody decreased serum PGE2 levels, MDSC in tumor, and cancer stem cells. |
| Mouse type | BALB/c nude mice, B6C3F1 | ||
| MDSC | Mouse and Patient-derived MDSC | ||
| Li et al. 2020 [23] | Cell line | ES-2, SKOV3 and HO-8910 | MDSC enhanced the stemness by activating CSF2/STAT3 pathway |
| Mouse type | Not used | ||
| MDSC | Patient-derived MDSC | ||
| Horikawa et al. 2020 [35] | Cell line | HM-1, ID-8 cells | Anti-VEGF therapy induced tumor hypoxia and GM-CSF expression, which recruited MDSC and inhibited tumor immunity. Anti-GM-CSF therapy reduced MDSC and improved the efficacy of anti-VEGF therapy. |
| Mouse type | C57BL/6 | ||
| MDSC | Mouse MDSC | ||
| Zeng et al. 2019 [36] | Cell line | ID-8 cells | Inhibition of CXCL12-CXCR4 by a CXCR4 antagonist decreased tumor-infiltrating MDSC. Dual blockade of CXCL12-CXCR4 and PD-1-PD-L1 pathways prolonged survival. |
| Mouse type | C57BL/6J | ||
| MDSC | Mouse MDSC | ||
| Baert et al. 2019 [37] | Cell line | I-D8 cells | MDSC inhibited the activity of CD8+ T cells. Depletion of MDSC by anti-Gr-1 antibody improved survival. |
| Mouse type | C57BL/6 | ||
| MDSC | Mouse MDSC | ||
| Taki et al. 2018 [28] | Cell line | HM-1, OVCAR8, OVCA433, A1847, JHOS2 | Snail induced cancer progression via upregulation of CXCR2 and recruitment of MDSC. CXCR2 antagonist inhibited MDSC infiltration and delayed tumor growth. |
| Mouse type | B6C3F1 | ||
| MDSC | Mouse and Patient-derived MDSC | ||
| Li et al. 2018 [29] | Cell line | Patient-derived ovarian cancer | Metformin blocked the suppressive function of MDSC by downregulating the expression and ectoenzymatic activity of CD39 and CD73 on MDSC. |
| Mouse type | BALB/c-nu | ||
| MDSC | Mouse and Patient-derived MDSC | ||
| Horikawa et al. 2017 [30] | Cell line | HM-1, ID-8 cells | MDSC migration and differentiation were augmented by VEGF signaling. Anti-Gr-1 antibody delayed the growth of tumor. |
| Mouse type | C57BL/6 mice | ||
| MDSC | Mouse and Patient-derived | ||
| Wu et al. 2017 [31] | Cell line | Not used | Ascites-derived IL-6 and IL-10 synergistically expanded M-MDSC in ovarian cancer. |
| Mouse type | Not used | ||
| MDSC | Patient-derived MDSC | ||
| Rodrıguez-Ubreva et al. 2017 [22] | Cell line | Not used | MDSC-Specific hypermethylation signature was mediated by PGE2-dependent DNMT3A overexpression in tumor. |
| Mouse type | Not used | ||
| MDSC | Patient-derived MDSC | ||
| Alexander et al. 2016 [38] | Cell line | ID-8 | Dabigatran, a direct thrombin inhibitor, in combination with cisplatin decreased MDSC. Dabigatran augmented the antitumor activity of cisplatin. |
| Mouse type | C57/Bl6 | ||
| MDSC | Mouse MDSC | ||
| Soong et al. 2016 [39] | Cell line | ID-8 | Bis-benzylidine piperidone RA190 inhibited the activity of MDSC via the inhibition of STAT3 expression. MDSC-inhibition by RA190 delayed tumor growth, and prolonged survival. |
| Mouse type | C57/Bl6 | ||
| MDSC | Mouse MDSC | ||
| Lamichhane et al. 2017 [40] | Cell line | ID-8 | Combination of PD-1 blockade and IL-10 neutralization decreased tumor-infiltrating MDSC, delayed tumor growth, and prolonged survival. |
| Mouse type | C57BL/6J | ||
| MDSC | Mouse MDSC | ||
| Cui et al. 2013 [32] | Cell line | Patient-derived ovarian cancer | MDSC inhibited the activity of CD8+ T cells. MDSC enhanced stemness of cancer cells by inducing microRNA101. |
| Mouse type | NSG (NOD/Scid/IL2Rγ) | ||
| MDSC | Patient-derived MDSC | ||
| Obermajer et al. 2011 [33] | Cell line | Not used | PGE2 attracted MDSC into TME through the CXCL12-CXCR4 axis. PGE2 or COX2 inhibition blocked CXCL12 production and attenuated its ability to attract MDSC. |
| Mouse type | Not used | ||
| MDSC | Patient-derived MDSC | ||
| Treatment Strategies | Comments | |
|---|---|---|
| (1) Depletion of MDSC. | ||
| Induction of MDSC apoptosis | Chemotherapeutic agents | Gemcitabine [42], 5-FU [43], paclitaxel [44], cisplatin [45], docetaxel [46], and lurbinectedin [47] |
| Tyrosine kinase inhibitors | Sunitinib [48] and sorafenib [49] | |
| Inhibition of MDSC generation | IL-6 inhibitors | Anti-IL-6R mAb [50] |
| CSF1R antagonists | GW2580 [51] and PLX3397 [52] | |
| S100A9 inhibitors | Tasquinimod [53] | |
| Diabetes drugs | Metformin [29] | |
| Thrombin inhibitor | Dabigatran [39] | |
| (2) Inhibition of MDSC functions. | ||
| B-Raf inhibitor | Vemurafenib [54] | |
| Bisphosphonates | Zoledronic acid [55] | |
| PDE-5 inhibitors | Sildenafil, tadalafil, and vardenafil [56] | |
| STAT3 inhibitors | Stattic [19], CPA7 [57], S3I-201 [58], and AG490 [59] | |
| mTOR inhibitors | Rapamycin [60] | |
| PI3K inhibitors | IPI-145 [61] and IPI-549 [62] | |
| COX2 inhibitors | Celecoxib [63] | |
| NSAID | Nitroaspirin [64] | |
| HDAC inhibitor | Entinostat [65] | |
| IDO inhibitor | Indoximod [66] | |
| (3) Prevention of MDSC recruitment into TME. | ||
| Chemokine receptor antagonists | AZD5069 (CXCR2) [67], Reparixin (CXCR2) [67], SX-682 (CXCR2) [67], AMD3100 (CXCR4) [67], CCX872 (CCR2) [68], and Maraviroc (CCR5) [67] | |
| (4) Promoting the differentiation of MDSC into mature, nonsuppressive cells. | ||
| Vitamin A | ATRA [69] | |
| Vitamin D | 1,25(OH)2D3 [70] | |
| Casein kinase inhibitor | Tetrabromocinnamic acid [71] | |
| Chemotherapeutic agents | Paclitaxel [44] and docetaxel [46] | |
| Trial Number * | Purpose/Design of the Study | Conditions | Interventions |
|---|---|---|---|
| NCT04022616 | Examine MDSC frequency | Breast cancer | Specimen collection procedure |
| NCT02868255 | Examine MDSC frequency | Hepatocellular carcinoma Ovarian cancer | Specimen collection procedure |
| NCT02735512 | Examine MDSC frequency | Bladder cancer | Specimen collection procedure |
| NCT02664883 | Examine MDSC frequency | Renal cell cancer | Specimen collection procedure |
| NCT04387682 | Examine MDSC frequency | Oral squamous cell carcinoma | Specimen collection procedure |
| NCT02669173 | A phase I study investigating that suppression of MDSCs with low dose capecitabine is safe and feasible. | Glioblastoma | Capecitabine plus bevacizumab |
| NCT01803152 | A phase I study consisting with 2 parts: after the dose escalation study of dendritic cell (DC) vaccination, the safety, feasibility and the effect of MDSC inhibition using gemcitabine concurrently with DC vaccination will be evaluated. | Sarcoma | DC vaccine, gemcitabine, imiquimod |
| NCT03525925 | A phase I trial evaluating the safety of ibrutinib and nivolumab combination therapy and determine the effect of ibrutinib on circulating levels of MDSC. | Metastatic malignant solid neoplasm | Ibrutinib plus nivolumab |
| NCT02637531 | A phase I study evaluating the safety and the tolerability of IPI-549 in combination with nivolumab. | Advanced solid tumors with increased MDSC | IPI-549 plus nivolumab |
| NCT03161431 | A phase I study evaluating the optimal dose of SX-682 with or without pembrolizumab, and the inhibitory effect of SX-682 on MDSC. | Melanoma | SX-682 and pembrolizumab |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mabuchi, S.; Sasano, T.; Komura, N. Targeting Myeloid-Derived Suppressor Cells in Ovarian Cancer. Cells 2021, 10, 329. https://doi.org/10.3390/cells10020329
Mabuchi S, Sasano T, Komura N. Targeting Myeloid-Derived Suppressor Cells in Ovarian Cancer. Cells. 2021; 10(2):329. https://doi.org/10.3390/cells10020329
Chicago/Turabian StyleMabuchi, Seiji, Tomoyuki Sasano, and Naoko Komura. 2021. "Targeting Myeloid-Derived Suppressor Cells in Ovarian Cancer" Cells 10, no. 2: 329. https://doi.org/10.3390/cells10020329
APA StyleMabuchi, S., Sasano, T., & Komura, N. (2021). Targeting Myeloid-Derived Suppressor Cells in Ovarian Cancer. Cells, 10(2), 329. https://doi.org/10.3390/cells10020329