
Immune Checkpoint Inhibitors in People Living with HIV/AIDS: Facts and Controversies


 ,
,  ,
,
Abstract
:1. Introduction
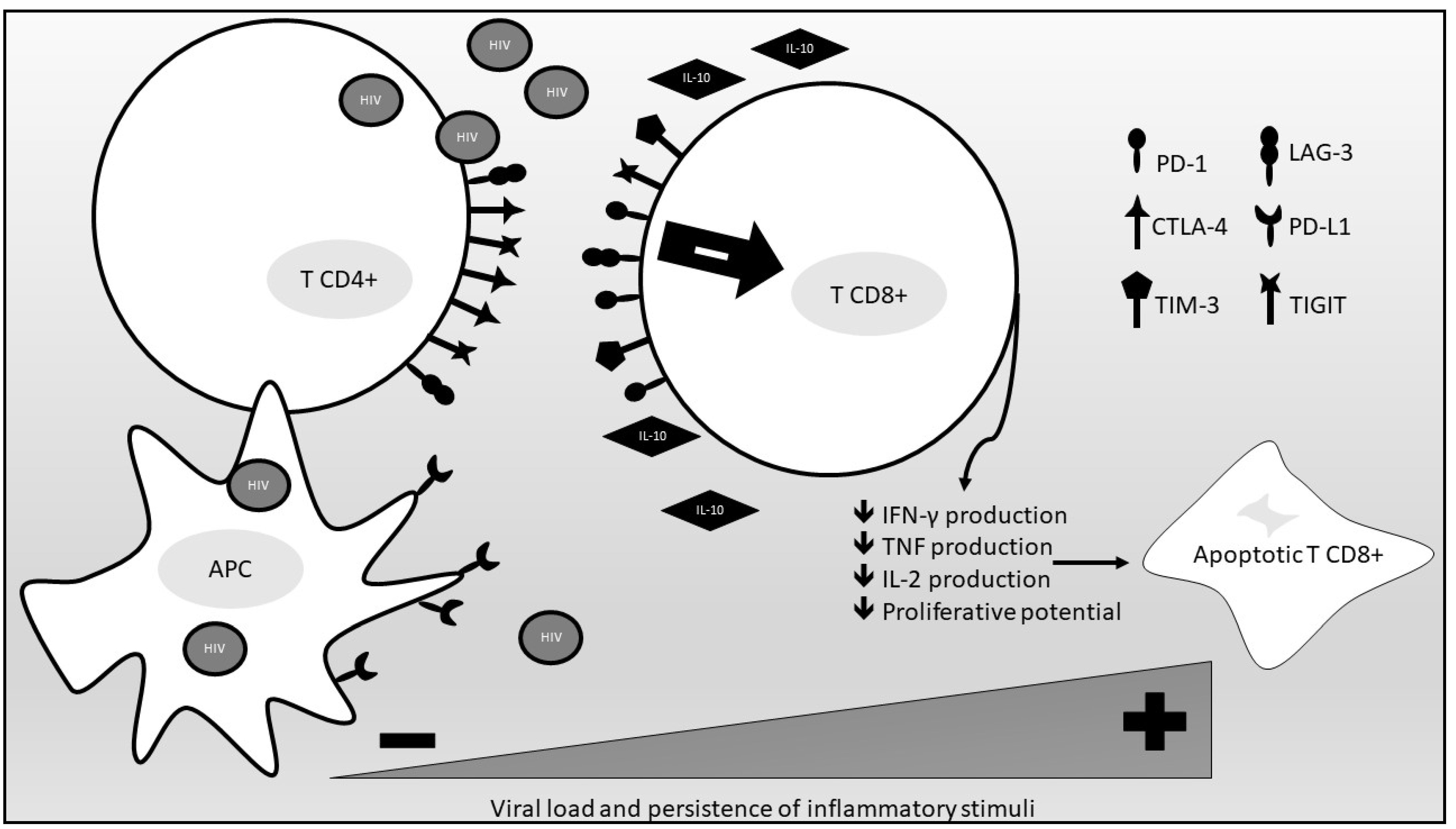
2. The Immunologic Background
3. The Impact of ICIs on HIV Replication
4. Safety and Efficacy of ICIs in PLWHIV
5. ICIs and Opportunistic Infections
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Food and Drug Administration (FDA). Drug Approval Package: YERVOY (ipilimumab) Injection. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2011/125377Orig1s000TOC.cfm (accessed on 23 April 2021).
- FDA Approves New, Targeted Treatment for Bladder Cancer | FDA. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-new-targeted-treatment-bladder-cancer (accessed on 24 April 2021).
- FDA Approves First Treatment for Rare Form of Skin Cancer | FDA. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-rare-form-skin-cancer (accessed on 24 April 2021).
- Food and Drug Administration. Drug Approval Package: LIBTAYO (cemiplimab-rwlc) Injection. 2021. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/761097s007lbl.pdf (accessed on 24 April 2021).
- FDA Grants Accelerated Approval to Dostarlimab-Gxly for dMMR Endometrial Cancer|FDA. Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-grants-accelerated-approval-dostarlimab-gxly-dmmr-endometrial-cancer (accessed on 24 April 2021).
- FDA Approves Durvalumab after Chemoradiation for Unresectable Stage III NSCLC | FDA. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-durvalumab-after-chemoradiation-unresectable-stage-iii-nsclc (accessed on 24 April 2021).
- Center for Drug Evaluation and Research Approval Package for: Nivolumab. 2014. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/125527Orig1s000Approv.pdf (accessed on 24 April 2021).
- FDA Pembrolizumab Label. 2014. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125514s096lbl.pdf (accessed on 24 April 2021).
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.-L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonia, S.J.; Borghaei, H.; Ramalingam, S.S.; Horn, L.; De Castro Carpeño, J.; Pluzanski, A.; Burgio, M.A.; Garassino, M.; Chow, L.Q.M.; Gettinger, S.; et al. Four-year survival with nivolumab in patients with previously treated advanced non-small-cell lung cancer: A pooled analysis. Lancet Oncol. 2019, 20, 1395–1408. [Google Scholar] [CrossRef]
- Garon, E.B.; Hellmann, M.D.; Rizvi, N.A.; Carcereny, E.; Leighl, N.B.; Ahn, M.J.; Eder, J.P.; Balmanoukian, A.S.; Aggarwal, C.; Horn, L.; et al. Five-year overall survival for patients with advanced non-small-cell lung cancer treated with pembrolizumab: Results from the phase i KEYNOTE-001 study. J. Clin. Oncol. 2019, 37, 2518–2527. [Google Scholar] [CrossRef] [PubMed]
- Vora, K.B.; Awad, M.M. Exclusion rates of patients living with HIV from cancer immunotherapy clinical trials. J. Clin. Oncol. 2020, 38, e19035. [Google Scholar] [CrossRef]
- Moskophidis, D.; Lechner, F.; Pircher, H.; Zinkernagel, R.M. Virus persistence in acutely infected immunocompetent mice by exhaustion of antiviral cytotoxic effector T cells. Nature 1993, 362, 758–761. [Google Scholar] [CrossRef] [PubMed]
- Gallimore, A.; Glithero, A.; Godkin, A.; Tissot, A.C.; Plückthun, A.; Elliott, T.; Hengartner, H.; Zinkernagel, R. Induction and Exhaustion of Lymphocytic Choriomeningitis Virus–specific Cytotoxic T Lymphocytes Visualized Using Soluble Tetrameric Major Histocompatibility Complex Class I–Peptide Complexes. J. Exp. Med. 1998, 187, 1383–1393. [Google Scholar] [CrossRef]
- Zajac, A.J.; Blattman, J.N.; Murali-Krishna, K.; Sourdive, D.J.D.; Suresh, M.; Altman, J.D.; Ahmed, R. Viral Immune Evasion Due to Persistence of Activated T Cells Without Effector Function. J. Exp. Med. 1998, 188, 2205–2213. [Google Scholar] [CrossRef] [PubMed]
- Klenerman, P.; Hill, A. T cells and viral persistence: Lessons from diverse infections. Nat. Immunol. 2005, 6, 873–879. [Google Scholar] [CrossRef]
- Blank, C.; Mackensen, A. Contribution of the PD-L1/PD-1 pathway to T-cell exhaustion: An update on implications for chronic infections and tumor evasion. Cancer Immunol. Immunother. 2007, 56, 739–745. [Google Scholar] [CrossRef]
- Wherry, E.J.; Kurachi, M. Molecular and cellular insights into T cell exhaustion. Nat. Rev. Immunol. 2015, 15, 486–499. [Google Scholar] [CrossRef]
- Kahan, S.M.; Wherry, E.J.; Zajac, A.J. T cell exhaustion during persistent viral infections. Virology 2015, 479–480, 180–193. [Google Scholar] [CrossRef]
- Parry, R.V.; Chemnitz, J.M.; Frauwirth, K.A.; Lanfranco, A.R.; Braunstein, I.; Kobayashi, S.V.; Linsley, P.S.; Thompson, C.B.; Riley, J.L. CTLA-4 and PD-1 Receptors Inhibit T-Cell Activation by Distinct Mechanisms. Mol. Cell. Biol. 2005, 25, 9543–9553. [Google Scholar] [CrossRef] [Green Version]
- Wherry, E.J. T cell exhaustion. Nat. Immunol. 2011, 12, 492–499. [Google Scholar] [CrossRef]
- Fenwick, C.; Joo, V.; Jacquier, P.; Noto, A.; Banga, R.; Perreau, M.; Pantaleo, G. T-cell exhaustion in HIV infection. Immunol. Rev. 2019, 292, 149–163. [Google Scholar] [CrossRef]
- Douek, D.C.; Brenchley, J.M.; Betts, M.R.; Ambrozak, D.R.; Hill, B.J.; Okamoto, Y.; Casazza, J.P.; Kuruppu, J.; Kunstman, K.; Wolinsky, S.; et al. HIV preferentially infects HIV-specific CD4+ T cells. Nature 2002, 417, 95–98. [Google Scholar] [CrossRef]
- Papagno, L.; Spina, C.A.; Marchant, A.; Salio, M.; Rufer, N.; Little, S.; Dong, T.; Chesney, G.; Waters, A.; Easterbrook, P.; et al. Immune activation and CD8+ T-cell differentiation towards senescence in HIV-1 infection. PLoS Biol. 2004, 2, e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The HIV-CAUSAL Collaboration. The effect of combined antiretroviral therapy on the overall mortality of HIV-infected individuals. Aids 2010, 24, 123–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, E.M.P.; Sereti, I. Immune restoration after antiretroviral therapy: The pitfalls of hasty or incomplete repairs. Immunol. Rev. 2013, 254, 343–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, M.; Pantazis, N.; Martin, G.E.; Hickling, S.; Hurst, J.; Meyerowitz, J.; Willberg, C.B.; Robinson, N.; Brown, H.; Fisher, M.; et al. Exhaustion of Activated CD8 T Cells Predicts Disease Progression in Primary HIV-1 Infection. PLoS Pathog. 2016, 12, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Trautmann, L.; Janbazian, L.; Chomont, N.; Said, E.A.; Gimmig, S.; Bessette, B.; Boulassel, M.-R.; Delwart, E.; Sepulveda, H.; Balderas, R.S.; et al. Upregulation of PD-1 expression on HIV-specific CD8+ T cells leads to reversible immune dysfunction. Nat. Med. 2006, 12, 1198–1202. [Google Scholar] [CrossRef] [PubMed]
- Day, C.L.; Kaufmann, D.E.; Kiepiela, P.; Brown, J.A.; Moodley, E.S.; Reddy, S.; Mackey, E.W.; Miller, J.D.; Leslie, A.J.; DePierres, C.; et al. PD-1 expression on HIV-specific T cells is associated with T-cell exhaustion and disease progression. Nature 2006, 443, 350–354. [Google Scholar] [CrossRef]
- Steiner, K.; Waase, I.; Rau, T.; Dietrich, M.; Fleischer, B.; Bröker, B.M. Enhanced expression of CTLA-4 (CD152) on CD4+ T cells in HIV infection. Clin. Exp. Immunol. 1999, 115, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, D.E.; Kavanagh, D.G.; Pereyra, F.; Zaunders, J.J.; Mackey, E.W.; Miura, T.; Palmer, S.; Brockman, M.; Rathod, A.; Piechocka-Trocha, A.; et al. Upregulation of CTLA-4 by HIV-specific CD4+ T cells correlates with disease progression and defines a reversible immune dysfunction. Nat. Immunol. 2007, 8, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.B.; Ndhlovu, L.C.; Barbour, J.D.; Sheth, P.M.; Jha, A.R.; Long, B.R.; Wong, J.C.; Satkunarajah, M.; Schweneker, M.; Chapman, J.M.; et al. Tim-3 expression defines a novel population of dysfunctional T cells with highly elevated frequencies in progressive HIV-1 infection. J. Exp. Med. 2008, 205, 2763–2779. [Google Scholar] [CrossRef] [PubMed]
- Rallón, N.; García, M.; García-Samaniego, J.; Cabello, A.; Álvarez, B.; Restrepo, C.; Nistal, S.; Górgolas, M.; Benito, J.M. Expression of PD-1 and tim-3 markers of T-cell exhaustion is associated with CD4 dynamics during the course of untreated and treated HIV infection. PLoS ONE 2018, 13, e0193829. [Google Scholar] [CrossRef]
- Tian, X.; Zhang, A.; Qiu, C.; Wang, W.; Yang, Y.; Qiu, C.; Liu, A.; Zhu, L.; Yuan, S.; Hu, H.; et al. The Upregulation of LAG-3 on T Cells Defines a Subpopulation with Functional Exhaustion and Correlates with Disease Progression in HIV-Infected Subjects. J. Immunol. 2015, 194, 3873–3882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chew, G.M.; Fujita, T.; Webb, G.M.; Burwitz, B.J.; Wu, H.L.; Reed, J.S.; Hammond, K.B.; Clayton, K.L.; Ishii, N.; Abdel-Mohsen, M.; et al. TIGIT Marks Exhausted T Cells, Correlates with Disease Progression, and Serves as a Target for Immune Restoration in HIV and SIV Infection. PLoS Pathog. 2016, 12, e1005349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brockman, M.A.; Kwon, D.S.; Tighe, D.P.; Pavlik, D.F.; Rosato, P.C.; Sela, J.; Porichis, F.; Le Gall, S.; Waring, M.T.; Moss, K.; et al. IL-10 is up-regulated in multiple cell types during viremic HIV infection and reversibly inhibits virus-specific T cells. Blood 2009, 114, 346–356. [Google Scholar] [CrossRef] [Green Version]
- Burke, M.M.; Kluger, H.M.; Golden, M.; Heller, K.N.; Hoos, A.; Sznol, M. Case Report: Response to Ipilimumab in a Patient with HIV with Metastatic Melanoma. J. Clin. Oncol. 2011, 29, e792–e794. [Google Scholar] [CrossRef]
- Morris, V.K.; Salem, M.E.; Nimeiri, H.; Iqbal, S.; Singh, P.; Ciombor, K.; Polite, B.; Deming, D.; Chan, E.; Wade, J.L.; et al. Nivolumab for previously treated unresectable metastatic anal cancer (NCI9673): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.; Cook, M.R. Safety and Efficacy of Immune Checkpoint Inhibitor Therapy in Patients with HIV Infection and Advanced-Stage Cancer: A Systematic Review. JAMA Oncol. 2019, 5, 1049–1053. [Google Scholar]
- Spano, J.P.; Veyri, M.; Gobert, A.; Guihot, A.; Perré, P.; Kerjouan, M.; Brosseau, S.; Cloarec, N.; Montaudié, H.; Helissey, C.; et al. Immunotherapy for cancer in people living with HIV: Safety with an efficacy signal from the series in real life experience. Aids 2019, 33, F13–F19. [Google Scholar] [CrossRef]
- Rico, G.T.; Chan, M.M.; Loo, K.F. The safety and efficacy of immune checkpoint inhibitors in patients with advanced cancers and pre-existing chronic viral infections (Hepatitis B/C, HIV): A review of the available evidence. Cancer Treat. Rev. 2020, 86, 102011. [Google Scholar] [CrossRef]
- Letizia, A.G.; Ge, Y.; Vangeti, S.; Goforth, C.; Weir, D.L.; Kuzmina, N.A.; Balinsky, C.A.; Chen, H.W.; Ewing, D.; Soares-Schanoski, A.; et al. SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: A prospective cohort study. Lancet Respir. Med. 2021, 2600, 1–9. [Google Scholar] [CrossRef]
- Chomont, N.; El-Far, M.; Ancuta, P.; Trautmann, L.; Procopio, F.A.; Yassine-Diab, B.; Boucher, G.; Boulassel, M.R.; Ghattas, G.; Brenchley, J.M.; et al. HIV reservoir size and persistence are driven by T cell survival and homeostatic proliferation. Nat. Med. 2009, 15, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Banga, R.; Rebecchini, C.; Procopio, F.A.; Noto, A.; Munoz, O.; Ioannidou, K.; Fenwick, C.; Ohmiti, K.; Cavassini, M.; Corpataux, J.M.; et al. Lymph node migratory dendritic cells modulate HIV-1 transcription through PD-1 engagement. PLoS Pathog. 2019, 15, e1007918. [Google Scholar] [CrossRef] [Green Version]
- Troeger, C.E.; Blacker, B.F.; Khalil, I.A.; Zimsen, S.R.M.; Albertson, S.B.; Abate, D.; Abdela, J.; Adhikari, T.B.; Aghayan, S.A.; Agrawal, S.; et al. Mortality, morbidity, and hospitalisations due to influenza lower respiratory tract infections, 2017: An analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2019, 7, 69–89. [Google Scholar] [CrossRef] [Green Version]
- Wightman, F.; Solomon, A.; Kumar, S.S.; Urriola, N.; Gallagher, K.; Hiener, B.; Palmer, S.; McNeil, C.; Garsia, R.; Lewin, S.R. Effect of ipilimumab on the HIV reservoir in an HIV-infected individual with metastatic melanoma. Aids 2015, 29, 504–506. [Google Scholar] [CrossRef] [Green Version]
- Guihot, A.; Marcelin, A.G.; Massiani, M.A.; Samri, A.; Soulié, C.; Autran, B.; Spano, J.P. Drastic decrease of the HIV reservoir in a patient treated with nivolumab for lung cancer. Ann. Oncol. 2018, 29, 517–518. [Google Scholar] [CrossRef] [Green Version]
- Abbar, B.; Baron, M.; Katlama, C.; Marcelin, A.G.; Veyri, M.; Autran, B.; Guihot, A.; Spano, J.P. Immune checkpoint inhibitors in people living with HIV: What about anti-HIV effects? Aids 2020, 34, 167–175. [Google Scholar] [CrossRef]
- Fromentin, R.; DaFonseca, S.; Costiniuk, C.T.; El-Far, M.; Procopio, F.A.; Hecht, F.M.; Hoh, R.; Deeks, S.G.; Hazuda, D.J.; Lewin, S.R.; et al. PD-1 blockade potentiates HIV latency reversal ex vivo in CD4 + T cells from ART-suppressed individuals. Nat. Commun. 2019, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Reuss, J.E.; Stern, D.; Foster, J.C.; Ramaswami, R.; Lurain, K.; Chen, H.X.; Streicher, H.; Kem, R.; Little, R.F.; Sharon, E. Assessment of Cancer Therapy Evaluation Program Advocacy and Inclusion Rates of People Living With HIV in Anti-PD1/PDL1 Clinical Trials. JAMA Netw. Open 2020, 3, e2027110. [Google Scholar] [CrossRef]
- Park, S.; Sacco, A.G.; Cohen, E.E.W.; Daniels, G.A. Safety and efficacy of checkpoint inhibition (CI) in cancer patients (pts) with concurrent human immunodeficiency virus (HIV) infection. J. Clin. Oncol. 2018, 36, 136. [Google Scholar] [CrossRef]
- Uldrick, T.S.; Gonçalves, P.H.; Abdul-Hay, M.; Claeys, A.J.; Emu, B.; Ernstoff, M.S.; Fling, S.P.; Fong, L.; Kaiser, J.C.; Lacroix, A.M.; et al. Assessment of the Safety of Pembrolizumab in Patients with HIV and Advanced Cancer—A Phase 1 Study. JAMA Oncol. 2019, 5, 1332–1339. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Church, C.; Alexander, N.A.; Shinohara, M.M.; Paulson, K.G.; Lewis, K.D.; Lee, N.S.; Nghiem, P. Immune checkpoint inhibitor therapy in HIV-associated Merkel cell carcinoma: A case series of 3 patients. JAAD Case Rep. 2021, 8, 28–33. [Google Scholar] [CrossRef]
- Galanina, N.; Goodman, A.M.; Cohen, P.R.; Frampton, G.M.; Kurzrock, R. Successful Treatment of HIV-associated Kaposi’s Sarcoma with Immune Checkpoint Blockade. Cancer Immunol Res. 2018, 176, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Bari, S.; Chan, A.; Jain, S.R.; Hostler, C.J. Outcomes of programmed cell death protein 1 (PD-1) and programmed death-ligand 1(PD-L1) inhibitor therapy in HIV patients with advanced cancer. J. Oncol. 2019, 2019, 1–5. [Google Scholar] [CrossRef] [Green Version]
- ClinicalTrials.gov Identifier: NCT02595866. Available online: https://clinicaltrials.gov/ct2/show/NCT02595866 (accessed on 24 April 2021).
- ClinicalTrials.gov Identifier: NCT03354936. Available online: https://clinicaltrials.gov/ct2/show/NCT03354936 (accessed on 24 April 2021).
- ClinicalTrials.gov Identifier: NCT02408861. Available online: https://clinicaltrials.gov/ct2/show/NCT02408861 (accessed on 24 April 2021).
- Haanen, J.B.A.G.; Carbonnel, F.; Robert, C.; Kerr, K.M.; Peters, S.; Larkin, J.; Jordan, K. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv264–iv266. [Google Scholar] [CrossRef]
- Ford, A.C.; Peyrin-Biroulet, L. Opportunistic infections with anti-tumor necrosis factor-α therapy in inflammatory bowel disease: Meta-analysis of randomized controlled trials. Am. J. Gastroenterol. 2013, 108, 1268–1276. [Google Scholar] [CrossRef]
- Klein, N.C.; Go, C.H.U.; Cunha, B.A. Infections associated with steroid use. Infect. Dis. Clin. N. Am. 2001, 15, 423–432. [Google Scholar] [CrossRef]
- Kyi, C.; Hellmann, M.D.; Wolchok, J.D.; Chapman, P.B.; Postow, M.A. Opportunistic infections in patients treated with immunotherapy for cancer. J. Immunother. Cancer 2014, 2, 2–4. [Google Scholar] [CrossRef] [Green Version]
- Uslu, U.; Agaimy, A.; Hundorfean, G.; Harrer, T.; Schuler, G.; Heinzerling, L. Autoimmune Colitis and Subsequent CMV-induced Hepatitis After Treatment With Ipilimumab. J. Immunother. 2015, 38, 212–215. [Google Scholar] [CrossRef]
- Arriola, E.; Wheater, M.; Krishnan, R.; Smart, J.; Foria, V.; Ottensmeier, C. Immunosuppression for ipilimumab-related toxicity can cause pneumocystis pneumonia but spare antitumor immune control. Oncoimmunology 2015, 4, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Del Castillo, M.; Romero, F.A.; Argüello, E.; Kyi, C.; Postow, M.A.; Redelman-Sidi, G. The spectrum of serious infections among patients receiving immune checkpoint blockade for the treatment of melanoma. Clin. Infect. Dis. 2016, 63, 1490–1493. [Google Scholar] [CrossRef] [Green Version]
- Fujita, K.; Kim, Y.H.; Kanai, O.; Yoshida, H.; Mio, T.; Hirai, T. Emerging concerns of infectious diseases in lung cancer patients receiving immune checkpoint inhibitor therapy. Respir. Med. 2019, 146, 66–70. [Google Scholar] [CrossRef]
- Lee, J.J.X.; Chan, A.; Tang, T. Tuberculosis reactivation in a patient receiving anti-programmed death-1 (PD-1) inhibitor for relapsed Hodgkin’s lymphoma. Acta Oncol. 2016, 55, 519–520. [Google Scholar] [CrossRef] [Green Version]
- Langan, E.A.; Graetz, V.; Allerheiligen, J.; Zillikens, D.; Rupp, J.; Terheyden, P. Immune checkpoint inhibitors and tuberculosis: An old disease in a new context. Lancet Oncol. 2020, 21, e55–e65. [Google Scholar] [CrossRef]
- Zaemes, J.; Kim, C. Immune checkpoint inhibitor use and tuberculosis: A systematic review of the literature. Eur. J. Cancer 2020, 132, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Uchida, N.; Fujita, K.; Nakatani, K.; Mio, T. Acute progression of aspergillosis in a patient with lung cancer receiving nivolumab. Respirol. Case Rep. 2018, 6, 3–5. [Google Scholar] [CrossRef]
- Su, Q.; Zhu, E.C.; Wu, J.B.; Li, T.; Hou, Y.L.; Wang, D.Y.; Gao, Z.H. Risk of pneumonitis and pneumonia associated with immune checkpoint inhibitors for solid tumors: A systematic review and meta-analysis. Front. Immunol. 2019, 10, 108. [Google Scholar] [CrossRef] [Green Version]
- Sadek, M.; Loizidou, A.; Drowart, A.; Van den Wijngaert, S.; Gomez-Galdon, M.; Aspeslagh, S. Pneumocystis infection in two patients treated with both immune checkpoint inhibitor and corticoids. J. Immunother. Precis. Oncol. 2020, 3, 27–30. [Google Scholar] [CrossRef]
- Slevin, F.; Mulatero, C.; Marples, M. Pneumocystis jirovecii pneumonia in a patient with melanoma treated with infliximab and corticosteroids for ipilimumab-associated colitis. Glob. Dermatol. 2016, 3, 381–384. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, M.; Kocher, F.; Niedersuess-Beke, D.; Rudzki, J.; Hochmair, M.; Widmann, G.; Hilbe, W.; Pircher, A. Immunosuppression for Immune Checkpoint-related Toxicity Can Cause Pneumocystis jirovecii Pneumonia (PJP) in Non-small-cell Lung Cancer (NSCLC): A Report of 2 Cases. Clin. Lung Cancer 2019, 20, E247–E250. [Google Scholar] [CrossRef] [PubMed]
- Omene, A.A.; Ferguson, R.P. Absolute lymphocyte count as a predictor of Pneumocystis pneumonia in patients previously unknown to have HIV. J. Community Hosp. Intern. Med. Perspect. 2012, 2, 15696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadranel, J.; Canellas, A.; Matton, L.; Darrason, M.; Parrot, A.; Naccache, J.-M.; Lavole, A.; Ruppert, A.-M.; Fallet, V. Pulmonary complications of immune checkpoint inhibitors in patients with nonsmall cell lung cancer. Eur. Respir. Rev. 2019, 28, 190058. [Google Scholar] [CrossRef]
- Better, J.; Matt, U. Pneumocystis pneumonia: Checkpoint inhibition to the rescue? Am. J. Respir. Cell Mol. Biol. 2020, 62, 674–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Drug | Target | Year of Approval (FDA) | Cancer/s |
|---|---|---|---|
| Atezolizumab | PD-L1 | 2016 | Bladder cancer, breast cancer, liver cancer, lung cancer, and melanoma |
| Avelumab | PD-L1 | 2017 | Bladder cancer, kidney cancer, and Merkel cell carcinoma |
| Cemiplimab | PD-1 | 2018 | Squamous cell skin cancer |
| Dostarlimab | PD-1 | 2021 | Endometrial cancer |
| Durvalumab | PD-1 | 2018 | Lung cancer |
| Ipilimumab | CTLA-4 | 2011 | Melanoma, mesothelioma, liver cancer, and lung cancer |
| Nivolumab | PD-1 | 2014 | Bladder cancer, colorectal cancer, esophageal cancer, gastric cancer, head and neck cancer, kidney cancer, liver cancer, lung cancer, lymphoma, melanoma, and mesothelioma |
| Pembrolizumab | PD-1 | 2014 | Bladder cancer, breast cancer, cervical cancer, colorectal cancer, cutaneous squamous cell carcinoma, esophageal cancer, head and neck cancer, kidney cancer, liver cancer, lung cancer, lymphoma, melanoma, Merkel cell carcinoma, and stomach cancer |
| RCT | Study Title | Phase | Cancer | ICI | Primary Objective/s |
|---|---|---|---|---|---|
| NCT03354936 | ANRS CO24 OncoVIHAC (Onco VIH Anti Checkpoint) | Observational | Any | Any | To evaluate clinical and biological safety of the use of immune checkpoint inhibitors in HIV infected patients with cancer treated by ICIs |
| NCT04514484 | Testing the Combination of the Anti-cancer Drugs XL184 (Cabozantinib) and Nivolumab in Patients WITH Advanced Cancer and HIV | 1 | Advanced solid tumors | Nivolumab | To determine the safety of combined nivolumab and cabozantinib s-malate (XL184) in PLWHIV with advanced solid tumors To determine the feasibility to deliver the combined nivolumab and XL184 for a minimum of 4 cycles in at least 75% of the subjects or to achieve a confirmed objective response |
| NCT03304093 | Immunotherapy by Nivolumab for HIV+ Patients (CHIVA2) | 2 | NSCLC Metastatic NSCLC Stage IIIB | Nivolumab | Disease control rate at 8 weeks |
| NCT02408861 | Nivolumab and Ipilimumab in Treating Patients With HIV Associated Relapsed or Refractory Classical Hodgkin Lymphoma or Solid Tumors That Are Metastatic or Cannot Be Removed by Surgery | 1 | Advanced Malignant Solid Neoplasm Anal Carcinoma Kaposi Sarcoma Lung Carcinoma Metastatic Malignant Solid Neoplasm Recurrent Classic Hodgkin Lymphoma Refractory Classic Hodgkin Lymphoma Unresectable Solid Neoplasm | Nivolumab Ipilimumab | Maximum tolerated dose of nivolumab |
| NCT03316274 | Intra-lesional Nivolumab Therapy for Limited Cutaneous Kaposi Sarcoma | 1 | Kaposi Sarcoma | Intra-lesional injection of nivolumab | Number of dose limiting toxicity (6 months) Maximum tolerated dose (6 months) |
| NCT02595866 | Pembrolizumab in Treating Patients With HIV and Relapsed, Refractory, or Disseminated Malignant Neoplasms | 1 | Relapsed, Refractory, or Disseminated Malignant Neoplasms | Pembrolizumab | Frequency of observed adverse events Incidence of immune-related events of clinical interest Incidence of cART-related ECIs of grade 2 or higher AEs |
| NCT03094286 | Durvalumab in Solid Tumors | 2 | Solid tumors | Durvalumab | Number of HIV patients that receive durvalumab at least during 4 months |
| NCT04499053 | Durvalumab in Combination With Chemotherapy in Virus-infected Patients With Non-small Cell Lung Cancer | 2 | NSCLC Stage IV | Durvalumab | Adverse events Radiological response |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castelli, V.; Lombardi, A.; Palomba, E.; Bozzi, G.; Ungaro, R.; Alagna, L.; Mangioni, D.; Muscatello, A.; Bandera, A.; Gori, A. Immune Checkpoint Inhibitors in People Living with HIV/AIDS: Facts and Controversies. Cells 2021, 10, 2227. https://doi.org/10.3390/cells10092227
Castelli V, Lombardi A, Palomba E, Bozzi G, Ungaro R, Alagna L, Mangioni D, Muscatello A, Bandera A, Gori A. Immune Checkpoint Inhibitors in People Living with HIV/AIDS: Facts and Controversies. Cells. 2021; 10(9):2227. https://doi.org/10.3390/cells10092227
Chicago/Turabian StyleCastelli, Valeria, Andrea Lombardi, Emanuele Palomba, Giorgio Bozzi, Riccardo Ungaro, Laura Alagna, Davide Mangioni, Antonio Muscatello, Alessandra Bandera, and Andrea Gori. 2021. "Immune Checkpoint Inhibitors in People Living with HIV/AIDS: Facts and Controversies" Cells 10, no. 9: 2227. https://doi.org/10.3390/cells10092227
APA StyleCastelli, V., Lombardi, A., Palomba, E., Bozzi, G., Ungaro, R., Alagna, L., Mangioni, D., Muscatello, A., Bandera, A., & Gori, A. (2021). Immune Checkpoint Inhibitors in People Living with HIV/AIDS: Facts and Controversies. Cells, 10(9), 2227. https://doi.org/10.3390/cells10092227