
Lithium and Erectile Dysfunction: An Overview



Abstract
:1. Introduction
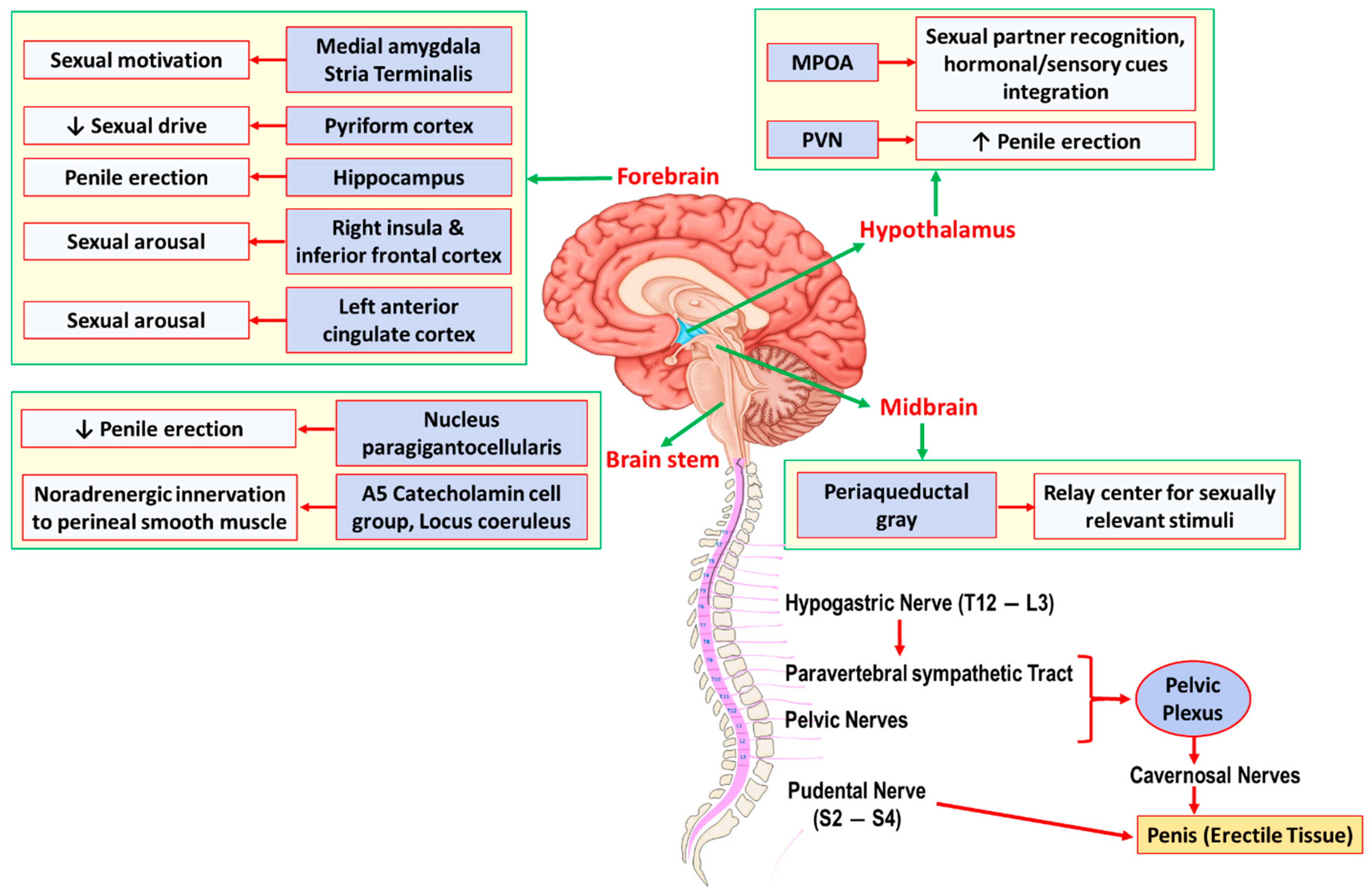
2. Neuroanatomy and Physiology of Erectile Function
3. Lithium and Sexual Dysfunction
3.1. Epidemiology
3.2. Underlying Mechanisms
3.2.1. Central Mechanisms
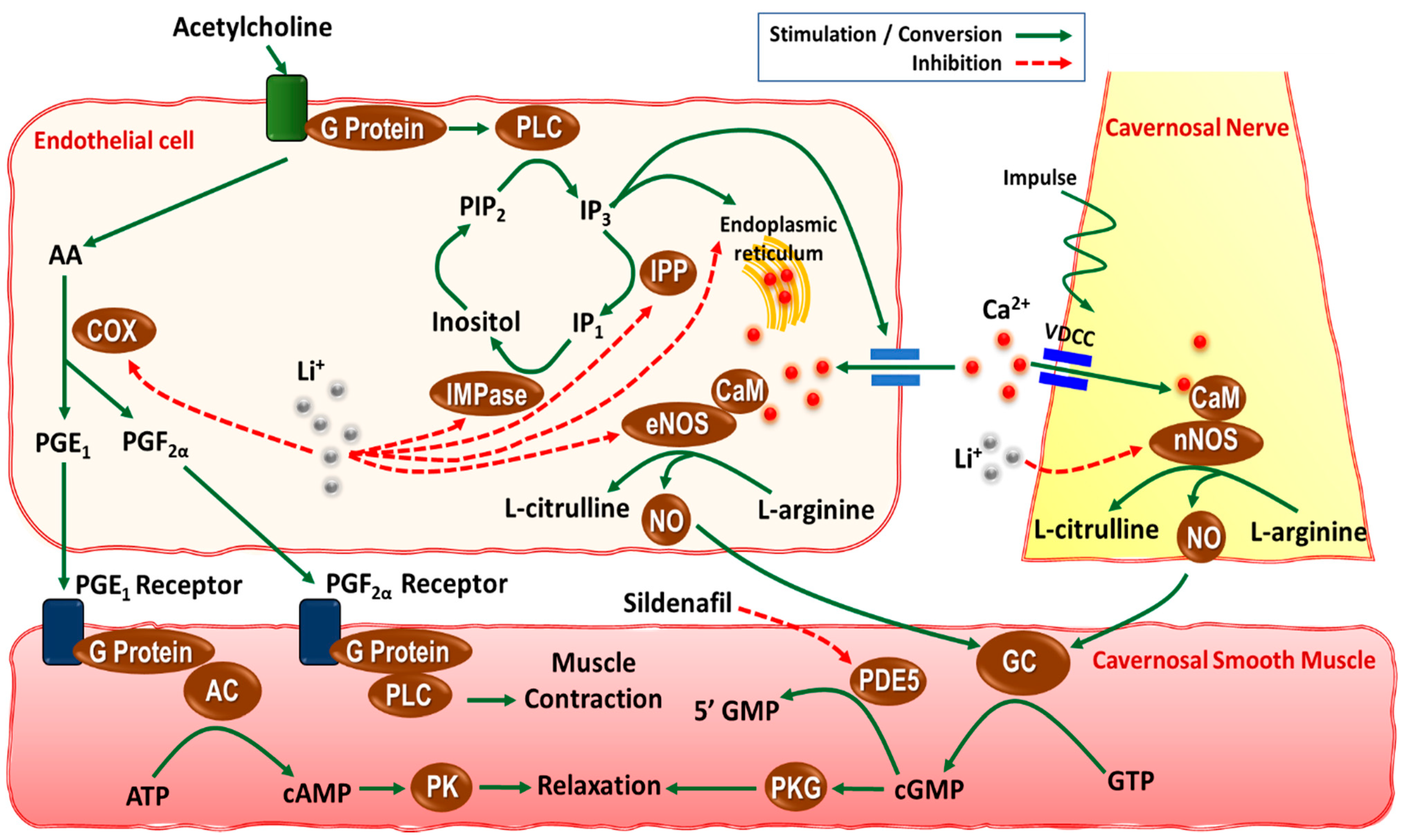
3.2.2. Peripheral Mechanisms
3.3. Therapeutic Approaches
4. Conclusions and Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Oruch, R.; Elderbi, M.A.; Khattab, H.A.; Pryme, I.F.; Lund, A. Lithium: A review of pharmacology, clinical uses, and toxicity. Eur. J. Pharmacol. 2014, 740, 464–473. [Google Scholar] [CrossRef]
- Aprahamian, I.; Sousa, R.T.d.; Valiengo, L.; Machado-Vieira, R.; Forlenza, O.V. Lithium safety and tolerability in mood disorders: A critical review. Rev. De Psiquiatr. Clin. 2014, 41, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Cade, J.F. Lithium salts in the treatment of psychotic excitement. Med. J. Aust. 1949, 2, 349–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geddes, J.R.; Burgess, S.; Hawton, K.; Jamison, K.; Goodwin, G.M. Long-term lithium therapy for bipolar disorder: Systematic review and meta-analysis of randomized controlled trials. Am. J. Psychiatry 2004, 161, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Pretty, H.; Hawton, K.; Geddes, J.R. Lithium in the prevention of suicidal behavior and all-cause mortality in patients with mood disorders: A systematic review of randomized trials. Am. J. Psychiatry 2005, 162, 1805–1819. [Google Scholar] [CrossRef]
- Ohgami, H.; Terao, T.; Shiotsuki, I.; Ishii, N.; Iwata, N. Lithium levels in drinking water and risk of suicide. Br. J. Psychiatry J. Ment. Sci. 2009, 194, 464–465; discussion 446, discussion 446. [Google Scholar] [CrossRef] [Green Version]
- Ghasemi, M.; Dehpour, A.R. The NMDA receptor/nitric oxide pathway: A target for the therapeutic and toxic effects of lithium. Trends Pharmacol. Sci. 2011, 32, 420–434. [Google Scholar] [CrossRef]
- Lenox, R.H.; Wang, L. Molecular basis of lithium action: Integration of lithium-responsive signaling and gene expression networks. Mol. Psychiatry 2003, 8, 135–144. [Google Scholar] [CrossRef]
- Scheuch, K.; Höltje, M.; Budde, H.; Lautenschlager, M.; Heinz, A.; Ahnert-Hilger, G.; Priller, J. Lithium modulates tryptophan hydroxylase 2 gene expression and serotonin release in primary cultures of serotonergic raphe neurons. Brain Res. 2010, 1307, 14–21. [Google Scholar] [CrossRef]
- Yin, L.; Wang, J.; Klein, P.S.; Lazar, M.A. Nuclear receptor Rev-erbalpha is a critical lithium-sensitive component of the circadian clock. Science 2006, 311, 1002–1005. [Google Scholar] [CrossRef] [Green Version]
- Toledano, E.; Ogryzko, V.; Danchin, A.; Ladant, D.; Mechold, U. 3′-5′ phosphoadenosine phosphate is an inhibitor of PARP-1 and a potential mediator of the lithium-dependent inhibition of PARP-1 in vivo. Biochem. J. 2012, 443, 485–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi, M.; Sadeghipour, H.; Mosleh, A.; Sadeghipour, H.R.; Mani, A.R.; Dehpour, A.R. Nitric oxide involvement in the antidepressant-like effects of acute lithium administration in the mouse forced swimming test. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2008, 18, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, M.; Sadeghipour, H.; Poorheidari, G.; Dehpour, A.R. A role for nitrergic system in the antidepressant-like effects of chronic lithium treatment in the mouse forced swimming test. Behav. Brain Res. 2009, 200, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, M.; Raza, M.; Dehpour, A.R. NMDA receptor antagonists augment antidepressant-like effects of lithium in the mouse forced swimming test. J. Psychopharmacol. 2010, 24, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Einat, H.; Kofman, O.; Itkin, O.; Lewitan, R.J.; Belmaker, R.H. Augmentation of lithium’s behavioral effect by inositol uptake inhibitors. J. Neural Transm. 1998, 105, 31–38. [Google Scholar] [CrossRef]
- Belmaker, R.H.; Kofman, O. Lithium research: State of the art. Biol. Psychiatry 1990, 27, 1279–1281. [Google Scholar] [CrossRef]
- Belmaker, R.H.; Bersudsky, Y.; Agam, G.; Levine, J.; Kofman, O. How does lithium work on manic depression? Clinical and psychological correlates of the inositol theory. Annu. Rev. Med. 1996, 47, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Bunney, W.E., Jr.; Pert, A.; Rosenblatt, J.; Pert, C.B.; Gallaper, D. Mode of action of lithium: Some biological considerations. Arch. Gen. Psychiatry 1979, 36, 898–901. [Google Scholar] [CrossRef]
- Chokhawala, K.; Lee, S.; Saadabadi, A. Lithium. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. [Google Scholar]
- Aizenberg, D.; Sigler, M.; Zemishlany, Z.; Weizman, A. Lithium and male sexual function in affective patients. Clin. Neuropharmacol. 1996, 19, 515–519. [Google Scholar] [CrossRef]
- Grover, S.; Ghosh, A.; Sarkar, S.; Chakrabarti, S.; Avasthi, A. Sexual dysfunction in clinically stable patients with bipolar disorder receiving lithium. J. Clin. Psychopharmacol. 2014, 34, 475–482. [Google Scholar] [CrossRef]
- Giuliano, F.; Rampin, O. Central neural regulation of penile erection. Neurosci. Biobehav. Rev. 2000, 24, 517–533. [Google Scholar] [CrossRef]
- Panaro, M.A.; Benameur, T.; Porro, C. Hypothalamic Neuropeptide Brain Protection: Focus on Oxytocin. J. Clin. Med. 2020, 9, 1534. [Google Scholar] [CrossRef]
- Courtois, F.; Carrier, S.; Charvier, K.; Guertin, P.A.; Journel, N.M. The control of male sexual responses. Curr. Pharm. Des. 2013, 19, 4341–4356. [Google Scholar] [CrossRef] [PubMed]
- Shindel, A.L.; Lue, T.F. Physiology of penile erection and pathophysiology of erectile dysfunction. In Campbell-Walsh Urology 12th Edition Review, 3rd ed.; Partin, A.W., Peters, C.A., Kavoussi, L.R., Dmochowski, R.R., Wein, A.J., Eds.; Elsevier: Philladelphia, PA, USA, 2020; pp. 253–256. [Google Scholar]
- Argiolas, A.; Melis, M.R. Neuropeptides and central control of sexual behaviour from the past to the present: A review. Prog. Neurobiol. 2013, 108, 80–107. [Google Scholar] [CrossRef] [PubMed]
- Marson, L.; List, M.S.; McKenna, K.E. Lesions of the nucleus paragigantocellularis alter ex copula penile reflexes. Brain Res. 1992, 592, 187–192. [Google Scholar] [CrossRef]
- Martínez-Salamanca, J.I.; Martínez-Ballesteros, C.; Portillo, L.; Gabancho, S.; Moncada, I.; Carballido, J. Physiology of erection. Arch. Esp. Urol. 2010, 63, 581–588. [Google Scholar]
- Lue, T.F. Erectile dysfunction. New Engl. J. Med. 2000, 342, 1802–1813. [Google Scholar] [CrossRef] [PubMed]
- Ignarro, L.J. Nitric oxide as a unique signaling molecule in the vascular system: A historical overview. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2002, 53, 503–514. [Google Scholar]
- Andersson, K.E. Erectile physiological and pathophysiological pathways involved in erectile dysfunction. J. Urol. 2003, 170, S6–S14. [Google Scholar] [CrossRef]
- Sadeghipour, H.; Ghasemi, M.; Nobakht, M.; Ebrahimi, F.; Dehpour, A.R. Effect of chronic lithium administration on endothelium-dependent relaxation of rat corpus cavernosum: The role of nitric oxide and cyclooxygenase pathways. BJU Int. 2007, 99, 177–182. [Google Scholar] [CrossRef]
- Kirkeby, H.J.; Fahrenkrug, J.; Holmquist, F.; Ottesen, B. Vasoactive intestinal polypeptide (VIP) and peptide histidine methionine (PHM) in human penile corpus cavernosum tissue and circumflex veins: Localization and in vitro effects. Eur. J. Clin. Investig. 1992, 22, 24–30. [Google Scholar] [CrossRef]
- Morrison, J.F.; Dhanasekaran, S.; Howarth, F.C. Neuropeptides in the rat corpus cavernosum and seminal vesicle: Effects of age and two types of diabetes. Auton. Neurosci. Basic Clin. 2009, 146, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, M.; Sadeghipour, H.; Mani, A.R.; Tavakoli, S.; Hajrasouliha, A.R.; Ebrahimi, F.; Dehpour, A.R. Effect of anandamide on nonadrenergic noncholinergic-mediated relaxation of rat corpus cavernosum. Eur. J. Pharmacol. 2006, 544, 138–145. [Google Scholar] [CrossRef]
- Ghasemi, M.; Sadeghipour, H.; Shafaroodi, H.; Nezami, B.G.; Gholipour, T.; Hajrasouliha, A.R.; Tavakoli, S.; Nobakht, M.; Moore, K.P.; Mani, A.R.; et al. Role of the nitric oxide pathway and the endocannabinoid system in neurogenic relaxation of corpus cavernosum from biliary cirrhotic rats. Br. J. Pharmacol. 2007, 151, 591–601. [Google Scholar] [CrossRef]
- Vinarová, E.; Uhlír, O.; Stika, L.; Vinar, O. Side effects of lithium administration. Act. Nerv. Super. 1972, 14, 105–107. [Google Scholar]
- Hollister, L.E. Drugs and sexual behavior in man. Life Sci. 1975, 17, 661–667. [Google Scholar] [CrossRef]
- Lorimy, F.; Lôo, H.; Deniker, P. Clinical effects of long-term lithium treatment on sleep, appetite and sexuality. L’Encephale 1977, 3, 227–239. [Google Scholar]
- Blay, S.L.; Ferraz, M.P.; Calil, H.M. Lithium-induced male sexual impairment: Two case reports. J. Clin. Psychiatry 1982, 43, 497–498. [Google Scholar]
- Kristensen, E.; Jørgensen, P. Sexual function in lithium-treated manic-depressive patients. Pharmacopsychiatry 1987, 20, 165–167. [Google Scholar] [CrossRef] [PubMed]
- Ghadirian, A.M.; Annable, L.; Bélanger, M.C. Lithium, benzodiazepines, and sexual function in bipolar patients. Am. J. Psychiatry 1992, 149, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Zuncheddu, C.; Carpiniello, B. Sexual dysfunctions and bipolar disorder: A study of patients submitted to a long- term lithium treatment. La Clin. Ter. 2006, 157, 419–424. [Google Scholar]
- García-Blanco, A.; García-Portilla, M.P.; Fuente-Tomás, L.; Batalla, M.; Sánchez-Autet, M.; Arranz, B.; Safont, G.; Arqués, S.; Livianos, L.; Sierra, P. Sexual Dysfunction and Mood Stabilizers in Long-Term Stable Patients With Bipolar Disorder. J. Sex. Med. 2020, 17, 930–940. [Google Scholar] [CrossRef] [PubMed]
- Dehpour, A.R.; Samini, M.; Sharifzadeh, M.; Hasan-Mazandarani, H. Effects of chronic lithium pretreatment on apomorphine-induced penile erection. Gen. Pharmacol. 1995, 26, 1015–1020. [Google Scholar] [CrossRef]
- Gower, A.J.; Berendsen, H.G.; Princen, M.M.; Broekkamp, C.L. The yawning-penile erection syndrome as a model for putative dopamine autoreceptor activity. Eur. J. Pharmacol. 1984, 103, 81–89. [Google Scholar] [CrossRef]
- Pehek, E.A.; Thompson, J.T.; Hull, E.M. The effects of intracranial administration of the dopamine agonist apomorphine on penile reflexes and seminal emission in the rat. Brain Res. 1989, 500, 325–332. [Google Scholar] [CrossRef]
- Sandoughdaran, S.; Sadeghipour, H.; Sadeghipour, H.R. Effect of acute lithium administration on penile erection: Involvement of nitric oxide system. Int. J. Reprod. Biomed. 2016, 14, 109–116. [Google Scholar] [CrossRef]
- Wegener, G.; Bandpey, Z.; Heiberg, I.L.; Volke, V.; Trabace, L.; Rosenberg, R.; Harvey, B.H. Combined chronic treatment with citalopram and lithium does not modify the regional neurochemistry of nitric oxide in rat brain. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2004, 55, 575–586. [Google Scholar]
- Haj-Mirzaian, A.; Amiri, S.; Kordjazy, N.; Momeny, M.; Razmi, A.; Rahimi-Balaei, M.; Amini-Khoei, H.; Haj-Mirzaian, A.; Marzban, H.; Mehr, S.E.; et al. Lithium attenuated the depressant and anxiogenic effect of juvenile social stress through mitigating the negative impact of interlukin-1β and nitric oxide on hypothalamic-pituitary-adrenal axis function. Neuroscience 2016, 315, 271–285. [Google Scholar] [CrossRef]
- Maruta, S.; Suzuki, E.; Yokoyama, M.; Sato, T.; Inada, K.; Watanabe, S.; Miyaoka, H. Effects of intraperitoneally injected lithium, imipramine and diazepam on nitrate levels in rat amygdala. Psychiatry Clin. Neurosci. 2005, 59, 358–361. [Google Scholar] [CrossRef]
- Bhalla, P.; Singla, N.; Dhawan, D.K. Potential of lithium to reduce aluminium-induced cytotoxic effects in rat brain. Biometals Int. J. Role Met. Ions Biol. Biochem. Med. 2010, 23, 197–206. [Google Scholar] [CrossRef]
- Hashioka, S.; Klegeris, A.; Monji, A.; Kato, T.; Sawada, M.; McGeer, P.L.; Kanba, S. Antidepressants inhibit interferon-gamma-induced microglial production of IL-6 and nitric oxide. Exp. Neurol. 2007, 206, 33–42. [Google Scholar] [CrossRef]
- Kita, I.; Yoshida, Y.; Nishino, S. An activation of parvocellular oxytocinergic neurons in the paraventricular nucleus in oxytocin-induced yawning and penile erection. Neurosci. Res. 2006, 54, 269–275. [Google Scholar] [CrossRef]
- Peiffer, A.; Veilleux, S.; Barden, N. Antidepressant and other centrally acting drugs regulate glucocorticoid receptor messenger RNA levels in rat brain. Psychoneuroendocrinology 1991, 16, 505–515. [Google Scholar] [CrossRef]
- Allagui, M.S.; Hfaiedh, N.; Croute, F.; Guermazi, F.; Vincent, C.; Soleilhavoup, J.P.; El Feki, A. Side effects of low serum lithium concentrations on renal, thyroid, and sexual functions in male and female rats. Comptes Rendus Biol. 2005, 328, 900–911. [Google Scholar] [CrossRef] [PubMed]
- Sadeghipour, H.; Ghasemi, M.; Ebrahimi, F.; Dehpour, A.R. Effect of lithium on endothelium-dependent and neurogenic relaxation of rat corpus cavernosum: Role of nitric oxide pathway. Nitric Oxide Biol. Chem. 2007, 16, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Sadeghipour, H.; Dehghani, M.; Ghasemi, M.; Riazi, K.; Asadi, S.; Ebrahimi, F.; Honar, H.; Hajrasouliha, A.R.; Tavakoli, S.; Sianati, S.; et al. The nonadrenergic noncholinergic-mediated relaxation of corpus cavernosum was impaired in chronic lithium-treated rats: Improvement with l-arginine. Eur. J. Pharmacol. 2008, 586, 300–305. [Google Scholar] [CrossRef]
- Ghasemi, M.; Farrokhi-Khajeh-Pasha, Y.; Ostovaneh, M.R.; Dehpour, A.R. Lithium decreased endothelium-mediated, but not nonadrenergic noncholinergic, relaxation of guinea pig corpus cavernosum in vitro: A role for nitrergic system. Fundam. Clin. Pharmacol. 2011, 25, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, U.; Comerma-Steffensen, S.; Andersson, K.E. Modulation of Dopaminergic Pathways to Treat Erectile Dysfunction. Basic Clin. Pharmacol. Toxicol. 2016, 119 (Suppl. S3), 63–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, G.; Chen, J.; Yang, B.; Yu, W.; Chen, Y.; Dai, Y. Dopamine D2 receptors in the basolateral amygdala modulate erectile function in a rat model of nonorganic erectile dysfunction. Andrologia 2019, 51, e13160. [Google Scholar] [CrossRef]
- Friedman, E.; Gershon, S. Effect of lithium on brain dopamine. Nature 1973, 243, 520–521. [Google Scholar] [CrossRef]
- Corrodi, H.; Fuxe, K.; Schou, M. The effect of prolonged lithium administration on cerebral monoamine neurons in the rat. Life Sci. 1969, 8, 643–651. [Google Scholar] [CrossRef]
- Gambarana, C.; Ghiglieri, O.; Masi, F.; Scheggi, S.; Tagliamonte, A.; De Montis, M.G. The effects of long-term administration of rubidium or lithium on reactivity to stress and on dopamine output in the nucleus accumbens in rats. Brain Res. 1999, 826, 200–209. [Google Scholar] [CrossRef]
- Ichikawa, J.; Dai, J.; Meltzer, H.Y. Lithium differs from anticonvulsant mood stabilizers in prefrontal cortical and accumbal dopamine release: Role of 5-HT(1A) receptor agonism. Brain Res. 2005, 1049, 182–190. [Google Scholar] [CrossRef]
- Can, A.; Frost, D.O.; Cachope, R.; Cheer, J.F.; Gould, T.D. Chronic lithium treatment rectifies maladaptive dopamine release in the nucleus accumbens. J. Neurochem. 2016, 139, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Leonard, B.E. Changes in rat brain monoamine metabolism following the acute administration of lithium chloride in combination with antidepressant drugs. Arch. Int. De Pharmacodyn. Ther. 1975, 215, 202–207. [Google Scholar]
- Hesketh, J.E.; Nicolaou, N.M.; Arbuthnott, G.W.; Wright, A.K. The effect of chronic lithium administration on dopamine metabolism in rat striatum. Psychopharmacology 1978, 56, 163–166. [Google Scholar] [CrossRef]
- Dziedzicka-Wasylewska, M.; Wedzony, K. The effect of prolonged administration of lithium on the level of dopamine D2 receptor mRNA in the rat striatum and nucleus accumbens. Acta Neurobiol. Exp. 1996, 56, 29–34. [Google Scholar]
- Kameda, K.; Miura, J.; Suzuki, K.; Kusumi, I.; Tanaka, T.; Koyama, T. Effects of lithium on dopamine D2 receptor expression in the rat brain striatum. J. Neural Transm. 2001, 108, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Flemenbaum, A. Lithium inhibition of norepinephrine and dopamine receptors. Biol. Psychiatry 1977, 12, 563–572. [Google Scholar] [PubMed]
- Schorderet, M. Lithium inhibition of cyclic AMP accumulation induced by dopamine in isolated retinae of the rabbit. Biochem. Pharmacol. 1977, 26, 167–170. [Google Scholar] [CrossRef]
- Friedman, S.D.; Dager, S.R.; Parow, A.; Hirashima, F.; Demopulos, C.; Stoll, A.L.; Lyoo, I.K.; Dunner, D.L.; Renshaw, P.F. Lithium and valproic acid treatment effects on brain chemistry in bipolar disorder. Biol. Psychiatry 2004, 56, 340–348. [Google Scholar] [CrossRef]
- Nonaka, S.; Hough, C.J.; Chuang, D.M. Chronic lithium treatment robustly protects neurons in the central nervous system against excitotoxicity by inhibiting N-methyl-D-aspartate receptor-mediated calcium influx. Proc. Natl. Acad. Sci. USA 1998, 95, 2642–2647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, R.; Hough, C.; Nakazawa, T.; Yamamoto, T.; Chuang, D.M. Lithium protection against glutamate excitotoxicity in rat cerebral cortical neurons: Involvement of NMDA receptor inhibition possibly by decreasing NR2B tyrosine phosphorylation. J. Neurochem. 2002, 80, 589–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wegener, G.; Bandpey, Z.; Heiberg, I.L.; Mørk, A.; Rosenberg, R. Increased extracellular serotonin level in rat hippocampus induced by chronic citalopram is augmented by subchronic lithium: Neurochemical and behavioural studies in the rat. Psychopharmacology 2003, 166, 188–194. [Google Scholar] [CrossRef]
- Haddjeri, N.; Szabo, S.T.; de Montigny, C.; Blier, P. Increased tonic activation of rat forebrain 5-HT(1A) receptors by lithium addition to antidepressant treatments. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2000, 22, 346–356. [Google Scholar] [CrossRef] [Green Version]
- Redrobe, J.P.; Bourin, M. Evidence of the activity of lithium on 5-HT1B receptors in the mouse forced swimming test: Comparison with carbamazepine and sodium valproate. Psychopharmacology 1999, 141, 370–377. [Google Scholar] [CrossRef]
- Mizuta, T.; Segawa, T. Chronic effects of imipramine and lithium on postsynaptic 5-HT1A and 5-HT1B sites and on presynaptic 5-HT3 sites in rat brain. Jpn. J. Pharmacol. 1988, 47, 107–113. [Google Scholar] [CrossRef]
- Bao, A.M.; Swaab, D.F. The human hypothalamus in mood disorders: The HPA axis in the center. IBRO Rep. 2019, 6, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Salvio, G.; Martino, M.; Giancola, G.; Arnaldi, G.; Balercia, G. Hypothalamic-Pituitary Diseases and Erectile Dysfunction. J. Clin. Med. 2021, 10, 2551. [Google Scholar] [CrossRef]
- Heck, A.L.; Thompson, M.K.; Uht, R.M.; Handa, R.J. Sex-Dependent Mechanisms of Glucocorticoid Regulation of the Mouse Hypothalamic Corticotropin-Releasing Hormone Gene. Endocrinology 2020, 161, bqz012. [Google Scholar] [CrossRef]
- Beaulieu, S.; Pelletier, G.; Vaudry, H.; Barden, N. Influence of the central nucleus of the amygdala on the content of corticotropin-releasing factor in the median eminence. Neuroendocrinology 1989, 49, 255–261. [Google Scholar] [CrossRef]
- Ghasemi, M.; Karimollah, A.R.; Dehpour, A.R. Nitric oxide involvement in the effect of acute lithium administration on the nonadrenergic noncholinergic-mediated relaxation of rat gastric fundus. Nitric Oxide Biol. Chem. 2007, 17, 152–159. [Google Scholar] [CrossRef]
- Karimollah, A.R.; Ghasemi, M.; Ghahremani, M.H.; Dehpour, A.R. Inhibition by lithium of the nitrergic relaxation of rat anococcygeus muscle. Nitric Oxide Biol. Chem. 2009, 20, 31–38. [Google Scholar] [CrossRef]
- Bosche, B.; Molcanyi, M.; Noll, T.; Rej, S.; Zatschler, B.; Doeppner, T.R.; Hescheler, J.; Müller, D.J.; Macdonald, R.L.; Härtel, F.V. A differential impact of lithium on endothelium-dependent but not on endothelium-independent vessel relaxation. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2016, 67, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Afsharimani, B.; Moezi, L.; Sadeghipour, H.; Rahimzadeh-Rofouyi, B.; Nobakht, M.; Sanatkar, M.; Ghahremani, M.H.; Dehpour, A.R. Effect of chronic lithium administration on endothelium-dependent relaxation of rat mesenteric bed: Role of nitric oxide. Can. J. Physiol. Pharmacol. 2007, 85, 1038–1046. [Google Scholar] [CrossRef] [PubMed]
- Rahimzadeh-Rofouyi, B.; Afsharimani, B.; Moezi, L.; Ebrahimi, F.; Mehr, S.E.; Mombeini, T.; Ghahremani, M.H.; Dehpour, A.R. Role of nitric oxide and prostaglandin systems in lithium modulation of acetylcholine vasodilation. J. Cardiovasc. Pharmacol. 2007, 50, 641–646. [Google Scholar] [CrossRef]
- Dehpour, A.R.; Ghafourifar, P.; Samenian, J.; Sadeghipour, H.R.; Sadr, S.S. The effect of lithium on endothelial-dependent relaxation in rat isolated aorta. Gen. Pharmacol. 1995, 26, 1003–1007. [Google Scholar] [CrossRef]
- Dehpour, A.R.; Aghadadashi, H.; Ghafourifar, P.; Roushanzamir, F.; Ghahremani, M.H.; Meysamee, F.; Rassaee, N.; Koucharian, A. Effect of chronic lithium administration on endothelium-dependent relaxation in rat aorta. Clin. Exp. Pharmacol. Physiol. 2000, 27, 55–59. [Google Scholar] [CrossRef]
- Vincent, M.B. Lithium inhibits substance P and vasoactive intestinal peptide-induced relaxations on isolated porcine ophthalmic artery. Headache 1992, 32, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Kadamur, G.; Ross, E.M. Mammalian phospholipase C. Annu. Rev. Physiol. 2013, 75, 127–154. [Google Scholar] [CrossRef] [Green Version]
- Dollins, D.E.; Xiong, J.-P.; Endo-Streeter, S.; Anderson, D.E.; Bansal, V.S.; Ponder, J.W.; Ren, Y.; York, J.D. A structural basis for lithium and substrate binding of an inositide phosphatase. J. Biol. Chem. 2021, 296, 100059. [Google Scholar] [CrossRef] [PubMed]
- Hiroi, T.; Wei, H.; Hough, C.; Leeds, P.; Chuang, D.M. Protracted lithium treatment protects against the ER stress elicited by thapsigargin in rat PC12 cells: Roles of intracellular calcium, GRP78 and Bcl-2. Pharm. J. 2005, 5, 102–111. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Zhou, Y.; Wang, Q.; Li, J.; Zheng, Z.; Chen, J.; Zhang, H.; Wang, Z.; Xu, H.; Xiao, J. Inhibiting endoplasmic reticulum stress by lithium chloride contributes to the integrity of blood-spinal cord barrier and functional recovery after spinal cord injury. Am. J. Transl. Res. 2017, 9, 1012–1024. [Google Scholar] [PubMed]
- Koenig, M.L.; Jope, R.S. Effects of lithium on synaptosomal Ca2+ fluxes. Psychopharmacology 1988, 96, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Bosche, B.; Schäfer, M.; Graf, R.; Härtel, F.V.; Schäfer, U.; Noll, T. Lithium prevents early cytosolic calcium increase and secondary injurious calcium overload in glycolytically inhibited endothelial cells. Biochem. Biophys. Res. Commun. 2013, 434, 268–272. [Google Scholar] [CrossRef]
- Nezamoleslami, S.; Sheibani, M.; Mumtaz, F.; Esmaeili, J.; Shafaroodi, H.; Dehpour, A.R. Lithium reverses the effect of opioids on eNOS/nitric oxide pathway in human umbilical vein endothelial cells. Mol. Biol. Rep. 2020, 47, 6829–6840. [Google Scholar] [CrossRef]
- Bassiouni, W.; Daabees, T.; Louedec, L.; Norel, X.; Senbel, A. Evaluation of some prostaglandins modulators on rat corpus cavernosum in-vitro: Is relaxation negatively affected by COX-inhibitors? Biomed. Pharmacother. 2019, 111, 1458–1466. [Google Scholar] [CrossRef]
- Angulo, J.; Cuevas, P.; La Fuente, J.M.; Pomerol, J.M.; Ruiz-Castañé, E.; Puigvert, A.; Gabancho, S.; Fernández, A.; Ney, P.; Sáenz De Tejada, I. Regulation of human penile smooth muscle tone by prostanoid receptors. Br. J. Pharmacol. 2002, 136, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Rapoport, S.I. Lithium and the other mood stabilizers effective in bipolar disorder target the rat brain arachidonic acid cascade. ACS Chem. Neurosci. 2014, 5, 459–467. [Google Scholar] [CrossRef]
- Bosetti, F.; Rintala, J.; Seemann, R.; Rosenberger, T.A.; Contreras, M.A.; Rapoport, S.I.; Chang, M.C. Chronic lithium downregulates cyclooxygenase-2 activity and prostaglandin E(2) concentration in rat brain. Mol. Psychiatry 2002, 7, 845–850. [Google Scholar] [CrossRef] [Green Version]
- Harvey, B.; Carstens, M.; Taljaard, J. Absence of an effect of the lithium-induced increase in cyclic GMP on the cyclic GMP-stimulated phosphodiesterase (PDE II). Evidence for cyclic AMP-specific hydrolysis. Neurochem. Res. 1993, 18, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Saroukhani, S.; Emami-Parsa, M.; Modabbernia, A.; Ashrafi, M.; Farokhnia, M.; Hajiaghaee, R.; Akhondzadeh, S. Aspirin for treatment of lithium-associated sexual dysfunction in men: Randomized double-blind placebo-controlled study. Bipolar Disord. 2013, 15, 650–656. [Google Scholar] [CrossRef]
- Gopalakrishnan, R.; Jacob, K.S.; Kuruvilla, A.; Vasantharaj, B.; John, J.K. Sildenafil in the treatment of antipsychotic-induced erectile dysfunction: A randomized, double-blind, placebo-controlled, flexible-dose, two-way crossover trial. Am. J. Psychiatry 2006, 163, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Bacconi, L.; Gressier, F. Efficacy and tolerance of PDE-5 in the treatment of erectile dysfunction in schizophrenic patients: A literature review. L’Encephale 2017, 43, 55–61. [Google Scholar] [CrossRef]
- Mazzilli, R.; Angeletti, G.; Olana, S.; Delfino, M.; Zamponi, V.; Rapinesi, C.; Del Casale, A.; Kotzalidis, G.D.; Elia, J.; Callovini, G.; et al. Erectile dysfunction in patients taking psychotropic drugs and treated with phosphodiesterase-5 inhibitors. Arch. Ital. Di Urol. Androl. 2018, 90, 44–48. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Lithium Treatment | Species | Measurement | Result | Ref |
|---|---|---|---|---|
| 600 mg/L in drinking water, 30 days | Male albino rats | Apomorphine (s.c.)-induced penile erection | ↓ | [45] |
| 0.5 and 1.0 mEq, i.p., 15 min prior oxytocin | Male Wistar rats | Oxytocin (i.c.v.)-induced penile erection & yawning | ↓ | [54] |
| 5 to 100 mg/kg, i.p., 30 min prior apomorphine | Male Sprague-Dawley rats | Apomorphine (s.c.)-induced penile erection | ↓ (at 50 & 100 mg/kg) | [48] |
| 6 mM/kg/day, i.p., 10 days | Male & female Sprague-Dawley rats | hypothalamic & hippocampal Type II glucocorticoid receptor mRNA levels | ↑ | [55] |
| 2 or 4 gr/kg food, 28 days | Male Wistar rats | Serum testosterone level & spermatogenesis | ↓ | [56] |
| Female Wistar rats | Serum estradiol level | ↑ | ||
| 0.5, 1, & 5 mM, in vitro, 45 min incubation | Male Sprague-Dawley rats | Neurogenic & endothelium (Ach)-mediated isolated cavernosal muscle relaxation | ↓ | [57] |
| 600 mg/L in drinking water, 30 days | Male Sprague-Dawley rats | Endothelium (Ach)-mediated isolated cavernosal muscle relaxation | ↓ | [32] |
| 600 mg/L in drinking water, 30 days | Male Sprague-Dawley rats | Neurogenic isolated cavernosal muscle relaxation | ↓ | [58] |
| 0.5, 1, & 5 mM, in vitro, 45 min incubation | Male guinea pigs | Endothelium (Ach)-mediated isolated cavernosal muscle relaxation | ↓ | [59] |
| Neurogenic isolated cavernosal muscle relaxation | ↔ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheibani, M.; Ghasemi, M.; Dehpour, A.R. Lithium and Erectile Dysfunction: An Overview. Cells 2022, 11, 171. https://doi.org/10.3390/cells11010171
Sheibani M, Ghasemi M, Dehpour AR. Lithium and Erectile Dysfunction: An Overview. Cells. 2022; 11(1):171. https://doi.org/10.3390/cells11010171
Chicago/Turabian StyleSheibani, Mohammad, Mehdi Ghasemi, and Ahmad Reza Dehpour. 2022. "Lithium and Erectile Dysfunction: An Overview" Cells 11, no. 1: 171. https://doi.org/10.3390/cells11010171
APA StyleSheibani, M., Ghasemi, M., & Dehpour, A. R. (2022). Lithium and Erectile Dysfunction: An Overview. Cells, 11(1), 171. https://doi.org/10.3390/cells11010171