

Role of Estrogens in Menstrual Migraine

 , and
, and
Abstract
:1. Introduction
2. Role of Estrogens and Estrogen Receptors in the Pathophysiology of Migraine
2.1. Estrogens and Estrogen Receptors
2.2. Estrogens and Neurotransmitter Systems
2.3. Estrogens and Oxytocin
2.4. Estrogens and the Trigeminovascular System
2.5. Estrogens, Calcitonin Gene-Related Peptide, and Neuroinflammation
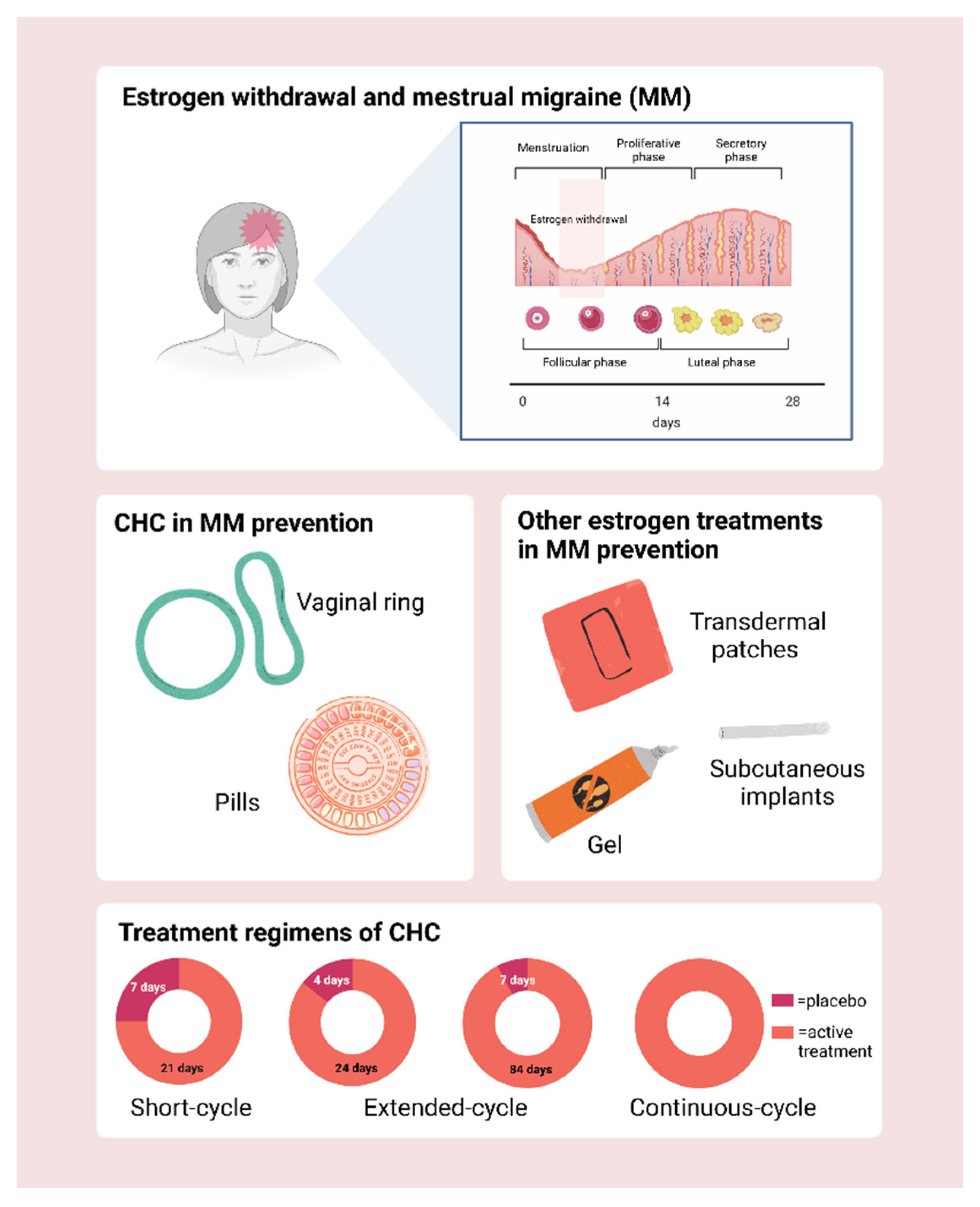
3. Estrogens in the Treatment of Menstrual Migraine
3.1. Combined Hormonal Contraception (CHC)
3.2. Short HFI
3.3. Estrogen Supplementation during the HFI
3.4. Extended and Continuous Regimens
3.5. Contraceptive Vaginal Ring
3.6. Other Treatments with Estrogens
3.7. Transdermal Patches
3.8. Add-Back Therapy
3.9. Transdermal Gel
3.10. Estradiol Implants
3.11. Phytoestrogens
3.12. Other Hormonal Treatments
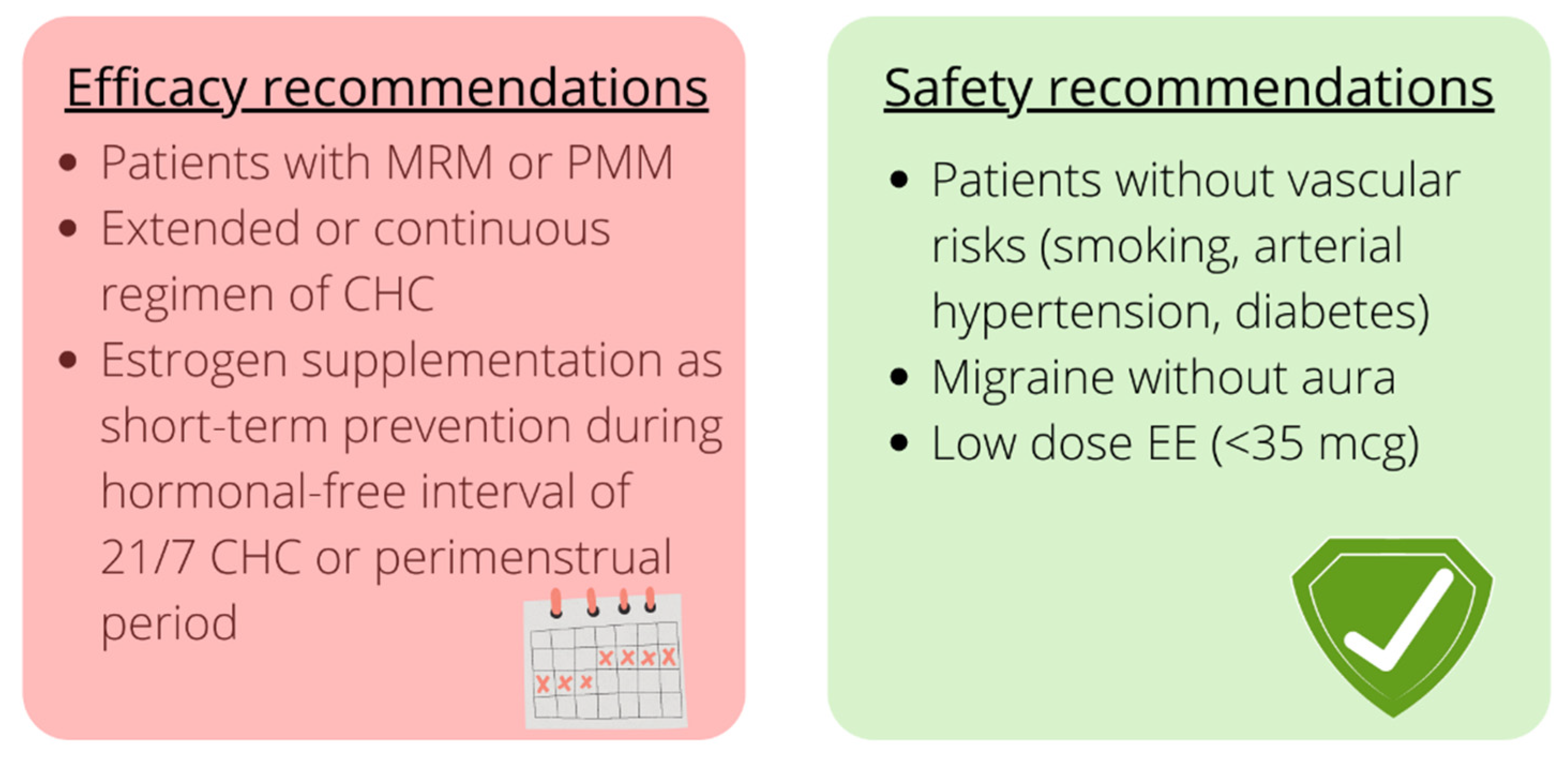
3.13. Clinical Guidance
3.14. Safety
4. Controversial Issues and Future Research Areas
4.1. Menstrual Migraine Definition
4.2. Use of Headache Diaries
4.3. Pathophysiological Insights
4.4. Future Studies on Efficacy and Safety
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vetvik, K.G.; MacGregor, E.A. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017, 16, 76–87. [Google Scholar] [CrossRef]
- Victor, T.W.; Hu, X.; Campbell, J.C.; Buse, D.C.; Lipton, R.B. Migraine prevalence by age and sex in the United States: A life-span study. Cephalalgia 2010, 30, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Bigal, M.E.; Diamond, M.; Freitag, F.; Reed, M.L.; Stewart, W.F.; AMPP Advisory Group. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007, 68, 343–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nappi, R.E.; Nappi, G. Neuroendocrine aspects of migraine in women. Gynecol. Endocrinol. 2012, 28 (Suppl. 1), 37–41. [Google Scholar] [CrossRef] [PubMed]
- Faubion, S.S.; Batur, P.; Calhoun, A.H. Migraine Throughout the Female Reproductive Life Cycle. Mayo Clin. Proc. 2018, 93, 639–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nappi, R.E.; Berga, S.L. Migraine and reproductive life. Handb. Clin. Neurol. 2010, 97, 303–322. [Google Scholar] [CrossRef] [PubMed]
- Chai, N.C.; Peterlin, B.L.; Calhoun, A.H. Migraine and estrogen. Curr. Opin. Neurol. 2014, 27, 315–324. [Google Scholar] [CrossRef] [Green Version]
- Sacco, S.; Ripa, P. Migraine in pregnancy. J. Headache Pain 2015, 16 (Suppl. 1), A24. [Google Scholar] [CrossRef] [Green Version]
- Nappi, R.E.; Sances, G.; Detaddei, S.; Ornati, A.; Chiovato, L.; Polatti, F. Hormonal management of migraine at menopause. Menopause Int. 2009, 15, 82–86. [Google Scholar] [CrossRef]
- Bushman, E.T.; Varner, M.W.; Digre, K.B. Headaches Through a Woman’s Life. Obstet. Gynecol. Surv. 2018, 73, 161–173. [Google Scholar] [CrossRef]
- Vetvik, K.G.; MacGregor, E.A. Menstrual migraine: A distinct disorder needing greater recognition. Lancet Neurol. 2021, 20, 304–315. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Reddy, N.; Desai, M.N.; Schoenbrunner, A.; Schneeberger, S.; Janis, J.E. The complex relationship between estrogen and migraines: A scoping review. Syst. Rev. 2021, 10, 72. [Google Scholar] [CrossRef] [PubMed]
- Somerville, B.W. The role of estradiol withdrawal in the etiology of menstrual migraine. Neurology 1972, 22, 355–365. [Google Scholar] [CrossRef]
- Lichten, E.M.; Lichten, J.B.; Whitty, A.; Pieper, D. The confirmation of a biochemical marker for women’s hormonal migraine: The depo-estradiol challenge test. Headache 1996, 36, 367–371. [Google Scholar] [CrossRef]
- Martin, V.T.; Behbehani, M. Ovarian hormones and migraine headache: Understanding mechanisms and pathogenesis—Part 2. Headache 2006, 46, 365–386. [Google Scholar] [CrossRef]
- Pavlović, J.M.; Allshouse, A.A.; Santoro, N.F.; Crawford, S.L.; Thurston, R.C.; Neal-Perry, G.S.; Lipton, R.B.; Derby, C.A. Sex hormones in women with and without migraine: Evidence of migraine-specific hormone profiles. Neurology 2016, 87, 49–56. [Google Scholar] [CrossRef]
- Boese, A.C.; Kim, S.C.; Yin, K.J.; Lee, J.P.; Hamblin, M.H. Sex differences in vascular physiology and pathophysiology: Estrogen and androgen signaling in health and disease. Am. J. Physiol. Heart Circ. Physiol. 2017, 313, H524–H545. [Google Scholar] [CrossRef]
- Cornil, C.A.; Ball, G.F.; Balthazart, J. Functional significance of the rapid regulation of brain estrogen action: Where do the estrogens come from? Brain Res. 2006, 1126, 2–26. [Google Scholar] [CrossRef] [Green Version]
- Hewitt, S.C.; Korach, K.S. Estrogen Receptors: New Directions in the New Millennium. Endocr. Rev. 2018, 39, 664–675. [Google Scholar] [CrossRef] [Green Version]
- Evinger, A.J., 3rd; Levin, E.R. Requirements for estrogen receptor alpha membrane localization and function. Steroids 2005, 70, 361–363. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.R.; Zhang, R.; Lian, Z.X.; Deng, S.L.; Yu, K. Estrogen-Receptor Expression and Function in Female Reproductive Disease. Cells 2019, 8, 1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, E.R. Extranuclear steroid receptors are essential for steroid hormone actions. Annu. Rev. Med. 2015, 66, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; McCarson, K.E.; Welch, K.M.; Berman, N.E. Mechanisms of pain modulation by sex hormones in migraine. Headache 2011, 51, 905–922. [Google Scholar] [CrossRef] [PubMed]
- Martin, V.T.; Behbehani, M. Ovarian hormones and migraine headache: Understanding mechanisms and pathogenesis—Part I. Headache 2006, 46, 3–23. [Google Scholar] [CrossRef]
- Burris, T.P.; Solt, L.A.; Wang, Y.; Crumbley, C.; Banerjee, S.; Griffett, K.; Lundasen, T.; Hughes, T.; Kojetin, D.J. Nuclear receptors and their selective pharmacologic modulators. Pharmacol. Rev. 2013, 65, 710–778. [Google Scholar] [CrossRef] [Green Version]
- Prossnitz, E.R.; Arterburn, J.B.; Sklar, L.A. GPR30: A G protein-coupled receptor for estrogen. Mol. Cell. Endocrinol. 2007, 265–266, 138–142. [Google Scholar] [CrossRef] [Green Version]
- Liverman, C.S.; Brown, J.W.; Sandhir, R.; McCarson, K.E.; Berman, N.E. Role of the oestrogen receptors GPR30 and ERalpha in peripheral sensitization: Relevance to trigeminal pain disorders in women. Cephalalgia 2009, 29, 729–741. [Google Scholar] [CrossRef] [Green Version]
- Pupo, M.; Vivacqua, A.; Perrotta, I.; Pisano, A.; Aquila, S.; Abonante, S.; Gasperi-Campani, A.; Pezzi, V.; Maggiolini, M. The nuclear localization signal is required for nuclear GPER translocation and function in breast Cancer-Associated Fibroblasts (CAFs). Mol. Cell. Endocrinol. 2013, 376, 23–32. [Google Scholar] [CrossRef]
- Filardo, E.J.; Quinn, J.A.; Frackelton, A.R., Jr.; Bland, K.I. Estrogen action via the G protein-coupled receptor, GPR30: Stimulation of adenylyl cyclase and cAMP-mediated attenuation of the epidermal growth factor receptor-to-MAPK signaling axis. Mol. Endocrinol. 2002, 16, 70–84. [Google Scholar] [CrossRef]
- Hewitt, S.C.; Winuthayanon, W.; Korach, K.S. What’s new in estrogen receptor action in the female reproductive tract. J. Mol. Endocrinol. 2016, 56, R55–R71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, K.A.; Carroll, J.S. Oestrogen-receptor-mediated transcription and the influence of co-factors and chromatin state. Nat. Rev. Cancer 2007, 7, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, M.E.; Karas, R.H. Rapid progress for non-nuclear estrogen receptor signaling. J. Clin. Investig. 2010, 120, 2277–2279. [Google Scholar] [CrossRef] [PubMed]
- Stirone, C.; Boroujerdi, A.; Duckles, S.P.; Krause, D.N. Estrogen receptor activation of phosphoinositide-3 kinase, akt, and nitric oxide signaling in cerebral blood vessels: Rapid and long-term effects. Mol. Pharmacol. 2005, 67, 105–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laflamme, N.; Nappi, R.E.; Drolet, G.; Labrie, C.; Rivest, S. Expression and neuropeptidergic characterization of estrogen receptors (ERalpha and ERbeta) throughout the rat brain: Anatomical evidence of distinct roles of each subtype. J. Neurobiol. 1998, 36, 357–378. [Google Scholar] [CrossRef]
- Krause, D.N.; Warfvinge, K.; Haanes, K.A.; Edvinsson, L. Hormonal influences in migraine—interactions of estrogen, oxytocin and CGRP. Nat. Rev. Neurol. 2021, 17, 621–633. [Google Scholar] [CrossRef]
- Borsook, D.; Erpelding, N.; Lebel, A.; Linnman, C.; Veggeberg, R.; Grant, P.E.; Buettner, C.; Becerra, L.; Burstein, R. Sex and the migraine brain. Neurobiol. Dis. 2014, 68, 200–214. [Google Scholar] [CrossRef] [Green Version]
- Warfvinge, K.; Krause, D.N.; Maddahi, A.; Edvinsson, J.C.A.; Edvinsson, L.; Haanes, K.A. Estrogen receptors α, β and GPER in the CNS and trigeminal system—Molecular and functional aspects. J. Headache Pain 2020, 21, 131. [Google Scholar] [CrossRef]
- Vanderhorst, V.G.; Gustafsson, J.A.; Ulfhake, B. Estrogen receptor-alpha and -beta immunoreactive neurons in the brainstem and spinal cord of male and female mice: Relationships to monoaminergic, cholinergic, and spinal projection systems. J. Comp. Neurol. 2005, 488, 152–179. [Google Scholar] [CrossRef]
- Zhang, J.Q.; Cai, W.Q.; Zhou, D.S.; Su, B.Y. Distribution and differences of estrogen receptor beta immunoreactivity in the brain of adult male and female rats. Brain Res. 2002, 935, 73–80. [Google Scholar] [CrossRef]
- Bereiter, D.A.; Cioffi, J.L.; Bereiter, D.F. Oestrogen receptor-immunoreactive neurons in the trigeminal sensory system of male and cycling female rats. Arch. Oral Biol. 2005, 50, 971–979. [Google Scholar] [CrossRef] [PubMed]
- de Vries, B.; Anttila, V.; Freilinger, T.; Wessman, M.; Kaunisto, M.A.; Kallela, M.; Artto, V.; Vijfhuizen, L.S.; Göbel, H.; Dichgans, M.; et al. Systematic re-evaluation of genes from candidate gene association studies in migraine using a large genome-wide association data set. Cephalalgia 2016, 36, 604–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherland, H.G.; Champion, M.; Plays, A.; Stuart, S.; Haupt, L.M.; Frith, A.; MacGregor, E.A.; Griffiths, L.R. Investigation of polymorphisms in genes involved in estrogen metabolism in menstrual migraine. Gene 2017, 607, 36–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Acevedo, A.J.; Smith, R.A.; Roy, B.; Sutherland, H.; Lea, R.A.; Frith, A.; MacGregor, E.A.; Griffiths, L.R. Genetic association and gene expression studies suggest that genetic variants in the SYNE1 and TNF genes are related to menstrual migraine. J. Headache Pain 2014, 15, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollock, C.E.; Sutherland, H.G.; Maher, B.H.; Lea, R.A.; Haupt, L.M.; Frith, A.; MacGregor, E.A.; Griffiths, L.R. The NRP1 migraine risk variant shows evidence of association with menstrual migraine. J. Headache Pain 2018, 19, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labruijere, S.; Stolk, L.; Verbiest, M.; de Vries, R.; Garrelds, I.M.; Eilers, P.H.; Danser, A.H.; Uitterlinden, A.G.; MaassenVanDenBrink, A. Methylation of migraine-related genes in different tissues of the rat. PLoS ONE 2014, 9, e87616. [Google Scholar] [CrossRef] [Green Version]
- Gundlah, C.; Pecins-Thompson, M.; Schutzer, W.E.; Bethea, C.L. Ovarian steroid effects on serotonin 1A, 2A and 2C receptor mRNA in macaque hypothalamus. Brain Res. Mol. Brain Res. 1999, 63, 325–339. [Google Scholar] [CrossRef]
- Pecins-Thompson, M.; Brown, N.A.; Kohama, S.G.; Bethea, C.L. Ovarian steroid regulation of tryptophan hydroxylase mRNA expression in rhesus macaques. J. Neurosci. 1996, 16, 7021–7029. [Google Scholar] [CrossRef]
- Bethea, C.L.; Lu, N.Z.; Gundlah, C.; Streicher, J.M. Diverse actions of ovarian steroids in the serotonin neural system. Front. Neuroendocrinol. 2002, 23, 41–100. [Google Scholar] [CrossRef]
- Pecins-Thompson, M.; Brown, N.A.; Bethea, C.L. Regulation of serotonin re-uptake transporter mRNA expression by ovarian steroids in rhesus macaques. Brain Res. Mol. Brain Res. 1998, 53, 120–129. [Google Scholar] [CrossRef]
- Nappi, R.E.; Sances, G.; Brundu, B.; De Taddei, S.; Sommacal, A.; Ghiotto, N.; Polatti, F.; Nappi, G. Estradiol supplementation modulates neuroendocrine response to M-chlorophenylpiperazine in menstrual status migrainosus triggered by oral contraception-free interval. Hum. Reprod. 2005, 20, 3423–3428. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.D.; Cole, N.B.; Segal, M. Brain-derived neurotrophic factor mediates estradiol-induced dendritic spine formation in hippocampal neurons. Proc. Natl. Acad. Sci. USA 1998, 95, 11412–11417. [Google Scholar] [CrossRef] [Green Version]
- Shughrue, P.J.; Merchenthaler, I. Estrogen is more than just a “sex hormone”: Novel sites for estrogen action in the hippocampus and cerebral cortex. Front. Neuroendocrinol. 2000, 21, 95–101. [Google Scholar] [CrossRef] [PubMed]
- González, S.L.; Meyer, L.; Raggio, M.C.; Taleb, O.; Coronel, M.F.; Patte-Mensah, C.; Mensah-Nyagan, A.G. Allopregnanolone and Progesterone in Experimental Neuropathic Pain: Former and New Insights with a Translational Perspective. Cell Mol. Neurobiol. 2019, 39, 523–537. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, F.; Martignoni, E.; Gallai, V.; Micieli, G.; Petraglia, F.; Nappi, G.; Genazzani, A.R. Neuroendocrine evaluation of central opiate activity in primary headache disorders. Pain 1988, 34, 29–33. [Google Scholar] [CrossRef]
- Amandusson, A.; Hallbeck, M.; Hallbeck, A.L.; Hermanson, O.; Blomqvist, A. Estrogen-induced alterations of spinal cord enkephalin gene expression. Pain 1999, 83, 243–248. [Google Scholar] [CrossRef]
- Gordon, F.T.; Soliman, M.R. The effects of estradiol and progesterone on pain sensitivity and brain opioid receptors in ovariectomized rats. Horm. Behav. 1996, 30, 244–250. [Google Scholar] [CrossRef]
- Facchinetti, F.; Martignoni, E.; Sola, D.; Petraglia, F.; Nappi, G.; Genazzani, A.R. Transient failure of central opioid tonus and premenstrual symptoms. J. Reprod. Med. 1988, 33, 633–638. [Google Scholar]
- Smith, Y.R.; Stohler, C.S.; Nichols, T.E.; Bueller, J.A.; Koeppe, R.A.; Zubieta, J.K. Pronociceptive and antinociceptive effects of estradiol through endogenous opioid neurotransmission in women. J. Neurosci. 2006, 26, 5777–5785. [Google Scholar] [CrossRef]
- Tassorelli, C.; Sandrini, G.; Cecchini, A.P.; Nappi, R.E.; Sances, G.; Martignoni, E. Changes in nociceptive flexion reflex threshold across the menstrual cycle in healthy women. Psychosom. Med. 2002, 64, 621–626. [Google Scholar] [CrossRef]
- Puri, V.; Cui, L.; Liverman, C.S.; Roby, K.F.; Klein, R.M.; Welch, K.M.; Berman, N.E. Ovarian steroids regulate neuropeptides in the trigeminal ganglion. Neuropeptides 2005, 39, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Poisbeau, P.; Grinevich, V.; Charlet, A. Oxytocin Signaling in Pain: Cellular, Circuit, System, and Behavioral Levels. Curr. Top. Behav. Neurosci. 2018, 35, 193–211. [Google Scholar] [CrossRef] [PubMed]
- Tzabazis, A.; Kori, S.; Mechanic, J.; Miller, J.; Pascual, C.; Manering, N.; Carson, D.; Klukinov, M.; Spierings, E.; Jacobs, D.; et al. Oxytocin and Migraine Headache. Headache 2017, 57 (Suppl. 2), 64–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warfvinge, K.; Krause, D.; Edvinsson, L. The distribution of oxytocin and the oxytocin receptor in rat brain: Relation to regions active in migraine. J. Headache Pain 2020, 21, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warfvinge, K.; Krause, D.N.; Maddahi, A.; Grell, A.S.; Edvinsson, J.C.; Haanes, K.A.; Edvinsson, L. Oxytocin as a regulatory neuropeptide in the trigeminovascular system: Localization, expression and function of oxytocin and oxytocin receptors. Cephalalgia 2020, 40, 1283–1295. [Google Scholar] [CrossRef]
- Engel, S.; Klusmann, H.; Ditzen, B.; Knaevelsrud, C.; Schumacher, S. Menstrual cycle-related fluctuations in oxytocin concentrations: A systematic review and meta-analysis. Front. Neuroendocrinol. 2019, 52, 144–155. [Google Scholar] [CrossRef]
- Hrabovszky, E.; Kalló, I.; Steinhauser, A.; Merchenthaler, I.; Coen, C.W.; Petersen, S.L.; Liposits, Z. Estrogen receptor-beta in oxytocin and vasopressin neurons of the rat and human hypothalamus: Immunocytochemical and in situ hybridization studies. J. Comp. Neurol. 2004, 473, 315–333. [Google Scholar] [CrossRef]
- Messlinger, K.; Russo, A.F. Current understanding of trigeminal ganglion structure and function in headache. Cephalalgia 2019, 39, 1661–1674. [Google Scholar] [CrossRef]
- Edvinsson, J.C.A.; Viganò, A.; Alekseeva, A.; Alieva, E.; Arruda, R.; De Luca, C.; D’Ettore, N.; Frattale, I.; Kurnukhina, M.; Macerola, N.; et al. The fifth cranial nerve in headaches. J. Headache Pain 2020, 21, 65. [Google Scholar] [CrossRef]
- Edvinsson, L. Tracing neural connections to pain pathways with relevance to primary headaches. Cephalalgia 2011, 31, 737–747. [Google Scholar] [CrossRef]
- Liu, Y.; Broman, J.; Zhang, M.; Edvinsson, L. Brainstem and thalamic projections from a craniovascular sensory nervous centre in the rostral cervical spinal dorsal horn of rats. Cephalalgia 2009, 29, 935–948. [Google Scholar] [CrossRef] [PubMed]
- Marciszewski, K.K.; Meylakh, N.; Di Pietro, F.; Mills, E.P.; Macefield, V.G.; Macey, P.M.; Henderson, L.A. Changes in Brainstem Pain Modulation Circuitry Function over the Migraine Cycle. J. Neurosci. 2018, 38, 10479–10488. [Google Scholar] [CrossRef] [PubMed]
- De Icco, R.; Cucinella, L.; De Paoli, I.; Martella, S.; Sances, G.; Bitetto, V.; Sandrini, G.; Nappi, G.; Tassorelli, C.; Nappi, R.E. Modulation of nociceptive threshold by combined hormonal contraceptives in women with oestrogen-withdrawal migraine attacks: A pilot study. J. Headache Pain 2016, 17, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, R.; Tassorelli, C.; Mangione, A.S.; Smeraldi, A.; Allena, M.; Sandrini, G.; Nappi, G.; Nappi, R.E. Effect of sex and estrogens on neuronal activation in an animal model of migraine. Headache 2013, 53, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Kitazawa, T.; Hamada, E.; Kitazawa, K.; Gaznabi, A.K. Non-genomic mechanism of 17 beta-oestradiol-induced inhibition of contraction in mammalian vascular smooth muscle. J. Physiol. 1997, 499 Pt 2, 497–511. [Google Scholar] [CrossRef]
- McNeill, A.M.; Zhang, C.; Stanczyk, F.Z.; Duckles, S.P.; Krause, D.N. Estrogen increases endothelial nitric oxide synthase via estrogen receptors in rat cerebral blood vessels: Effect preserved after concurrent treatment with medroxyprogesterone acetate or progesterone. Stroke 2002, 33, 1685–1691. [Google Scholar] [CrossRef]
- Sandweiss, A.J.; Cottier, K.E.; McIntosh, M.I.; Dussor, G.; Davis, T.P.; Vanderah, T.W.; Largent-Milnes, T.M. 17-β-Estradiol induces spreading depression and pain behavior in alert female rats. Oncotarget 2017, 8, 114109–114122. [Google Scholar] [CrossRef] [Green Version]
- Somjen, G.G. Mechanisms of spreading depression and hypoxic spreading depression-like depolarization. Physiol. Rev. 2001, 81, 1065–1096. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Levy, D.; Kainz, V.; Noseda, R.; Jakubowski, M.; Burstein, R. Activation of central trigeminovascular neurons by cortical spreading depression. Ann. Neurol. 2011, 69, 855–865. [Google Scholar] [CrossRef] [Green Version]
- Yamanaka, G.; Suzuki, S.; Morishita, N.; Takeshita, M.; Kanou, K.; Takamatsu, T.; Suzuki, S.; Morichi, S.; Watanabe, Y.; Ishida, Y.; et al. Role of Neuroinflammation and Blood-Brain Barrier Permutability on Migraine. Int. J. Mol. Sci. 2021, 22, 8929. [Google Scholar] [CrossRef]
- Chauvel, V.; Multon, S.; Schoenen, J. Estrogen-dependent effects of 5-hydroxytryptophan on cortical spreading depression in rat: Modelling the serotonin-ovarian hormone interaction in migraine aura. Cephalalgia 2018, 38, 427–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Casteren, D.S.; Verhagen, I.E.; van der Arend, B.W.H.; van Zwet, E.W.; MaassenVanDenBrink, A.; Terwindt, G.M. Comparing Perimenstrual and Nonperimenstrual Migraine Attacks Using an e-Diary. Neurology 2021, 97, e1661–e1671. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, S.; Ossipov, M.H.; Johnson, K.W. The role of calcitonin gene-related peptide in peripheral and central pain mechanisms including migraine. Pain 2017, 158, 543–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramachandran, R. Neurogenic inflammation and its role in migraine. Semin. Immunopathol. 2018, 40, 301–314. [Google Scholar] [CrossRef]
- Dagistan, Y.; Kilinc, E.; Balci, C.N. Cervical sympathectomy modulates the neurogenic inflammatory neuropeptides following experimental subarachnoid hemorrhage in rats. Brain Res. 2019, 1722, 146366. [Google Scholar] [CrossRef]
- Cetinkaya, A.; Kilinc, E.; Camsari, C.; Ogun, M.N. Effects of estrogen and progesterone on the neurogenic inflammatory neuropeptides: Implications for gender differences in migraine. Exp. Brain Res. 2020, 238, 2625–2639. [Google Scholar] [CrossRef]
- Frederiksen, S.D.; Bekker-Nielsen Dunbar, M.; Snoer, A.H.; Deen, M.; Edvinsson, L. Serotonin and Neuropeptides in Blood From Episodic and Chronic Migraine and Cluster Headache Patients in Case-Control and Case-Crossover Settings: A Systematic Review and Meta-Analysis. Headache 2020, 60, 1132–1164. [Google Scholar] [CrossRef]
- Valdemarsson, S.; Edvinsson, L.; Hedner, P.; Ekman, R. Hormonal influence on calcitonin gene-related peptide in man: Effects of sex difference and contraceptive pills. Scand. J. Clin. Lab. Investig. 1990, 50, 385–388. [Google Scholar] [CrossRef]
- Stevenson, J.C.; Macdonald, D.W.; Warren, R.C.; Booker, M.W.; Whitehead, M.I. Increased concentration of circulating calcitonin gene related peptide during normal human pregnancy. Br. Med. J. 1986, 293, 1329–1330. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.; Harte, A.; Sturdee, D.W.; Sharma, A.; Barnett, A.H.; Kumar, S.; McTernan, P.G. Effects of menopausal status on circulating calcitonin gene-related peptide and adipokines: Implications for insulin resistance and cardiovascular risks. Climacteric 2008, 11, 364–372. [Google Scholar] [CrossRef] [Green Version]
- Edvinsson, L.; Haanes, K.A.; Warfvinge, K.; Krause, D.N. CGRP as the target of new migraine therapies—Successful translation from bench to clinic. Nat. Rev. Neurol. 2018, 14, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Eftekhari, S.; Salvatore, C.A.; Calamari, A.; Kane, S.A.; Tajti, J.; Edvinsson, L. Differential distribution of calcitonin gene-related peptide and its receptor components in the human trigeminal ganglion. Neuroscience 2010, 169, 683–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labastida-Ramírez, A.; Rubio-Beltrán, E.; Villalón, C.M.; MaassenVanDenBrink, A. Gender aspects of CGRP in migraine. Cephalalgia 2019, 39, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Wyon, Y.; Frisk, J.; Lundeberg, T.; Theodorsson, E.; Hammar, M. Postmenopausal women with vasomotor symptoms have increased urinary excretion of calcitonin gene-related peptide. Maturitas 1998, 30, 289–294. [Google Scholar] [CrossRef]
- Wang, D.; Zhao, J.; Wang, J.; Li, J.; Yu, S.; Guo, X. Deficiency of female sex hormones augments PGE2 and CGRP levels within midbrain periaqueductal gray. J. Neurol. Sci. 2014, 346, 107–111. [Google Scholar] [CrossRef]
- Aggarwal, M.; Puri, V.; Puri, S. Effects of estrogen on the serotonergic system and calcitonin gene-related peptide in trigeminal ganglia of rats. Ann. Neurosci. 2012, 19, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Sarajari, S.; Oblinger, M.M. Estrogen effects on pain sensitivity and neuropeptide expression in rat sensory neurons. Exp. Neurol. 2010, 224, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Kawai, T.; Akira, S. The role of pattern-recognition receptors in innate immunity: Update on Toll-like receptors. Nat. Immunol. 2010, 11, 373–384. [Google Scholar] [CrossRef]
- Xing, D.; Feng, W.; Miller, A.P.; Weathington, N.M.; Chen, Y.F.; Novak, L.; Blalock, J.E.; Oparil, S. Estrogen modulates TNF-alpha-induced inflammatory responses in rat aortic smooth muscle cells through estrogen receptor-beta activation. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H2607–H2612. [Google Scholar] [CrossRef]
- Cupini, L.M.; Corbelli, I.; Sarchelli, P. Menstrual migraine: What it is and does it matter? J. Neurol. 2021, 268, 2355–2363. [Google Scholar] [CrossRef]
- MacGregor, E.A. Differences Between Perimenstrual Migraine Attacks and Migraine Attacks at Other Times of the Cycle. Neurology 2021, 97, e1753–e1756. [Google Scholar] [CrossRef] [PubMed]
- Granella, F.; Sances, G.; Allais, G.; Nappi, R.E.; Tirelli, A.; Benedetto, C.; Brundu, B.; Facchinetti, F.; Nappi, G. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia 2004, 24, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Nappi, R.E.; Merki-Feld, G.S.; Terreno, E.; Pellegrinelli, A.; Viana, M. Hormonal contraception in women with migraine: Is progestogen-only contraception a better choice? J. Headache Pain 2013, 14, 66. [Google Scholar] [CrossRef] [Green Version]
- Tepper, N.K.; Whiteman, M.K.; Zapata, L.B.; Marchbanks, P.A.; Curtis, K.M. Safety of hormonal contraceptives among women with migraine: A systematic review. Contraception 2016, 94, 630–640. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.; Merki-Feld, G.S.; Ægidius, K.L.; Bitzer, J.; Canonico, M.; Kurth, T.; Lampl, C.; Lidegaard, Ø.; MacGregor, E.A.; MaassenVanDenBrink, A.; et al. Hormonal contraceptives and risk of ischemic stroke in women with migraine: A consensus statement from the European Headache Federation (EHF) and the European Society of Contraception and Reproductive Health (ESC). J. Headache Pain 2017, 18, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allais, G.; Chiarle, G.; Sinigaglia, S.; Airola, G.; Schiapparelli, P.; Bergandi, F.; Benedetto, C. Treating migraine with contraceptives. Neurol. Sci. 2017, 38 (Suppl. 1), 85–89. [Google Scholar] [CrossRef] [PubMed]
- MacGregor, E.A. Migraine, menopause and hormone replacement therapy. Post. Reprod. Health 2018, 24, 11–18. [Google Scholar] [CrossRef]
- Sacco, S.; Merki-Feld, G.S.; Ægidius, K.L.; Bitzer, J.; Canonico, M.; Gantenbein, A.R.; Kurth, T.; Lampl, C.; Lidegaard, Ø.; MacGregor, E.A.; et al. Effect of exogenous estrogens and progestogens on the course of migraine during reproductive age: A consensus statement by the European Headache Federation (EHF) and the European Society of Contraception and Reproductive Health (ESCRH). J. Headache Pain 2018, 19, 76. [Google Scholar] [CrossRef]
- MacGregor, E.A.; Frith, A.; Ellis, J.; Aspinall, L.; Hackshaw, A. Incidence of migraine relative to menstrual cycle phases of rising and falling estrogen. Neurology 2006, 67, 2154–2158. [Google Scholar] [CrossRef]
- Benagiano, G.; Bastianelli, C.; Farris, M. Contraception today. Ann. N. Y. Acad. Sci. 2006, 1092, 1–32. [Google Scholar] [CrossRef]
- Maguire, K.; Westhoff, C. The state of hormonal contraception today: Established and emerging noncontraceptive health benefits. Am. J. Obstet. Gynecol. 2011, 205, S4–S8. [Google Scholar] [CrossRef] [PubMed]
- Sitruk-Ware, R.; Nath, A. The use of newer progestins for contraception. Contraception 2010, 82, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Morimont, L.; Haguet, H.; Dogné, J.M.; Gaspard, U.; Douxfils, J. Combined Oral Contraceptives and Venous Thromboembolism: Review and Perspective to Mitigate the Risk. Front. Endocrinol. (Lausanne) 2021, 12, 769187. [Google Scholar] [CrossRef] [PubMed]
- Voedisch, A.J.; Fok, W.K. Oestrogen component of COCs: Have we finally found a replacement for ethinyl estradiol? Curr. Opin. Obstet. Gynecol. 2021, 33, 433–439. [Google Scholar] [CrossRef]
- Sitruk-Ware, R.; Nath, A. Metabolic effects of contraceptive steroids. Rev. Endocr. Metab. Disord. 2011, 12, 63–75. [Google Scholar] [CrossRef]
- Shrader, S.P.; Dickerson, L.M. Extended- and continuous-cycle oral contraceptives. Pharmacotherapy 2008, 28, 1033–1040. [Google Scholar] [CrossRef]
- De Leo, V.; Scolaro, V.; Musacchio, M.C.; Di Sabatino, A.; Morgante, G.; Cianci, A. Combined oral contraceptives in women with menstrual migraine without aura. Fertil. Steril. 2011, 96, 917–920. [Google Scholar] [CrossRef]
- Nappi, R.E.; Terreno, E.; Sances, G.; Martini, E.; Tonani, S.; Santamaria, V.; Tassorelli, C.; Spinillo, A. Effect of a contraceptive pill containing estradiol valerate and dienogest (E2V/DNG) in women with menstrually-related migraine (MRM). Contraception 2013, 88, 369–375. [Google Scholar] [CrossRef]
- Calhoun, A.H. A novel specific prophylaxis for menstrual-associated migraine. South. Med. J. 2004, 97, 819–822. [Google Scholar] [CrossRef]
- Macgregor, E.A.; Hackshaw, A. Prevention of migraine in the pill-free interval of combined oral contraceptives: A double-blind, placebo-controlled pilot study using natural oestrogen supplements. J. Fam. Plann. Reprod. Health Care 2002, 28, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Coffee, A.L.; Sulak, P.J.; Hill, A.J.; Hansen, D.J.; Kuehl, T.J.; Clark, J.W. Extended cycle combined oral contraceptives and prophylactic frovatriptan during the hormone-free interval in women with menstrual-related migraines. J. Women’s Health (Larchmt.) 2014, 23, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Sulak, P.; Willis, S.; Kuehl, T.; Coffee, A.; Clark, J. Headaches and oral contraceptives: Impact of eliminating the standard 7-day placebo interval. Headache 2007, 47, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Roumen, F.J.; Mishell, D.R., Jr. The contraceptive vaginal ring, NuvaRing(®), a decade after its introduction. Eur. J. Contracept. Reprod. Health Care 2012, 17, 415–427. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, M.W.; van Bragt, A.J.; Alnabawy, A.K.; Kaptein, M.C. Comparison of ethinylestradiol pharmacokinetics in three hormonal contraceptive formulations: The vaginal ring, the transdermal patch and an oral contraceptive. Contraception 2005, 72, 168–174. [Google Scholar] [CrossRef]
- Calhoun, A.; Ford, S.; Pruitt, A. The impact of extended-cycle vaginal ring contraception on migraine aura: A retrospective case series. Headache 2012, 52, 1246–1253. [Google Scholar] [CrossRef]
- Donaghy, M.; Chang, C.L.; Poulter, N.; European Collaborators of The World Health Organisation Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Duration, frequency, recency, and type of migraine and the risk of ischaemic stroke in women of childbearing age. J. Neurol. Neurosurg. Psychiatry 2002, 73, 747–750. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, J.C. Type and route of estrogen administration. Climacteric 2009, 12 (Suppl. 1), 86–90. [Google Scholar] [CrossRef]
- Files, J.; Kling, J.M. Transdermal delivery of bioidentical estrogen in menopausal hormone therapy: A clinical review. Expert Opin. Drug Deliv. 2020, 17, 543–549. [Google Scholar] [CrossRef]
- Tassorelli, C.; Greco, R.; Allena, M.; Terreno, E.; Nappi, R.E. Transdermal hormonal therapy in perimenstrual migraine: Why, when and how? Curr. Pain Headache Rep. 2012, 16, 467–473. [Google Scholar] [CrossRef]
- Smite, M.G.; van der Meer, Y.G.; Pfeil, J.P.; Rijnierse, J.J.; Vos, A.J. Perimenstrual migraine: Effect of Estraderm TTS and the value of contingent negative variation and exteroceptive temporalis muscle suppression test. Headache 1994, 34, 103–106. [Google Scholar] [CrossRef]
- Almén-Christensson, A.; Hammar, M.; Lindh-Åstrand, L.; Landtblom, A.M.; Brynhildsen, J. Prevention of menstrual migraine with perimenstrual transdermal 17-β-estradiol: A randomized, placebo-controlled, double-blind crossover study. Fertil. Steril. 2011, 96, 498–500.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guidotti, M.; Mauri, M.; Barrilà, C.; Guidotti, F.; Belloni, C. Frovatriptan vs. transdermal oestrogens or naproxen sodium for the prophylaxis of menstrual migraine. J. Headache Pain 2007, 8, 283–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, S.C.; Muse, K.N. Effective treatment of severe menstrual migraine headaches with gonadotropin-releasing hormone agonist and “add-back” therapy. Fertil. Steril. 1997, 67, 390–393. [Google Scholar] [CrossRef]
- Martin, V.; Wernke, S.; Mandell, K.; Zoma, W.; Bean, J.; Pinney, S.; Liu, J.; Ramadan, N.; Rebar, R. Medical oophorectomy with and without estrogen add-back therapy in the prevention of migraine headache. Headache 2003, 43, 309–321. [Google Scholar] [CrossRef] [PubMed]
- de Lignières, B.; Vincens, M.; Mauvais-Jarvis, P.; Mas, J.L.; Touboul, P.J.; Bousser, M.G. Prevention of menstrual migraine by percutaneous oestradiol. Br. Med. J. (Clin. Res. Ed.) 1986, 293, 1540. [Google Scholar] [CrossRef] [Green Version]
- Dennerstein, L.; Morse, C.; Burrows, G.; Oats, J.; Brown, J.; Smith, M. Menstrual migraine: A double-blind trial of percutaneous estradiol. Gynecol. Endocrinol. 1988, 2, 113–120. [Google Scholar] [CrossRef]
- MacGregor, E.A.; Frith, A.; Ellis, J.; Aspinall, L.; Hackshaw, A. Prevention of menstrual attacks of migraine: A double-blind placebo-controlled crossover study. Neurology 2006, 67, 2159–2163. [Google Scholar] [CrossRef]
- Magos, A.L.; Zilkha, K.J.; Studd, J.W. Treatment of menstrual migraine by oestradiol implants. J. Neurol. Neurosurg. Psychiatry 1983, 46, 1044–1046. [Google Scholar] [CrossRef] [Green Version]
- Ferrante, F.; Fusco, E.; Calabresi, P.; Cupini, L.M. Phyto-oestrogens in the prophylaxis of menstrual migraine. Clin. Neuropharmacol. 2004, 27, 137–140. [Google Scholar] [CrossRef]
- Burke, B.E.; Olson, R.D.; Cusack, B.J. Randomized, controlled trial of phytoestrogen in the prophylactic treatment of menstrual migraine. Biomed. Pharmacother. 2002, 56, 283–288. [Google Scholar] [CrossRef]
- Merki-Feld, G.S.; Imthurn, B.; Gantenbein, A.R.; Sandor, P. Effect of desogestrel 75 µg on headache frequency and intensity in women with migraine: A prospective controlled trial. Eur. J. Contracept. Reprod. Health Care 2019, 24, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Morotti, M.; Remorgida, V.; Venturini, P.L.; Ferrero, S. Progestin-only contraception compared with extended combined oral contraceptive in women with migraine without aura: A retrospective pilot study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 183, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Merki-Feld, G.S.; Imthurn, B.; Seifert, B.; Merki, L.L.; Agosti, R.; Gantenbein, A.R. Desogestrel-only contraception may reduce headache frequency and improve quality of life in women suffering from migraine. Eur. J. Contracept. Reprod. Health Care 2013, 18, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Merki-Feld, G.S.; Imthurn, B.; Langner, R.; Sándor, P.S.; Gantenbein, A.R. Headache frequency and intensity in female migraineurs using desogestrel-only contraception: A retrospective pilot diary study. Cephalalgia 2013, 33, 340–346. [Google Scholar] [CrossRef]
- Nappi, R.E.; Sances, G.; Allais, G.; Terreno, E.; Benedetto, C.; Vaccaro, V.; Polatti, F.; Facchinetti, F. Effects of an estrogen-free, desogestrel-containing oral contraceptive in women with migraine with aura: A prospective diary-based pilot study. Contraception 2011, 83, 223–228. [Google Scholar] [CrossRef]
- Vetvik, K.G.; MacGregor, E.A.; Lundqvist, C.; Russell, M.B. Contraceptive-induced amenorrhoea leads to reduced migraine frequency in women with menstrual migraine without aura. J. Headache Pain 2014, 15, 30. [Google Scholar] [CrossRef]
- Bushnell, C.D. Oestrogen and stroke in women: Assessment of risk. Lancet Neurol. 2005, 4, 743–751. [Google Scholar] [CrossRef]
- Glaser, R.; Dimitrakakis, C.; Trimble, N.; Martin, V. Testosterone pellet implants and migraine headaches: A pilot study. Maturitas 2012, 71, 385–388. [Google Scholar] [CrossRef]
- Eikermann-Haerter, K.; Baum, M.J.; Ferrari, M.D.; van den Maagdenberg, A.M.; Moskowitz, M.A.; Ayata, C. Androgenic suppression of spreading depression in familial hemiplegic migraine type 1 mutant mice. Ann. Neurol. 2009, 66, 564–568. [Google Scholar] [CrossRef]
- Nappi, R.E.; Wawra, K.; Schmitt, S. Hypoactive sexual desire disorder in postmenopausal women. Gynecol Endocrinol. 2006, 22, 318–323. [Google Scholar] [CrossRef]
- Neri, I.; Granella, F.; Nappi, R.; Manzoni, G.C.; Facchinetti, F.; Genazzani, A.R. Characteristics of headache at menopause: A clinico-epidemiologic study. Maturitas 1993, 17, 31–37. [Google Scholar] [CrossRef]
- MacGregor, E.A. Menstrual and perimenopausal migraine: A narrative review. Maturitas 2020, 142, 24–30. [Google Scholar] [CrossRef] [PubMed]
- MacGregor, E.A. Perimenopausal migraine in women with vasomotor symptoms. Maturitas 2012, 71, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Nappi, R.E.; Cagnacci, A.; Granella, F.; Piccinini, F.; Polatti, F.; Facchinetti, F. Course of primary headaches during hormone replacement therapy. Maturitas 2001, 38, 157–163. [Google Scholar] [CrossRef]
- Facchinetti, F.; Nappi, R.E.; Tirelli, A.; Polatti, F.; Nappi, G.; Sances, G. Hormone supplementation differently affects migraine in postmenopausal women. Headache 2002, 42, 924–929. [Google Scholar] [CrossRef]
- Nappi, R.E.; Sances, G.; Sommacal, A.; Detaddei, S.; Facchinetti, F.; Cristina, S.; Polatti, F.; Nappi, G. Different effects of tibolone and low-dose EPT in the management of postmenopausal women with primary headaches. Menopause 2006, 13, 818–825. [Google Scholar] [CrossRef]
- Kurth, T.; Chabriat, H.; Bousser, M.G. Migraine and stroke: A complex association with clinical implications. Lancet Neurol. 2012, 11, 92–100. [Google Scholar] [CrossRef]
- Sacco, S.; Ricci, S.; Degan, D.; Carolei, A. Migraine in women: The role of hormones and their impact on vascular diseases. J. Headache Pain 2012, 13, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Sacco, S.; Ricci, S.; Carolei, A. Migraine and vascular diseases: A review of the evidence and potential implications for management. Cephalalgia 2012, 32, 785–795. [Google Scholar] [CrossRef]
- Sacco, S.; Kurth, T. Migraine and the risk for stroke and cardiovascular disease. Curr. Cardiol. Rep. 2014, 16, 524. [Google Scholar] [CrossRef]
- Lauritzen, M.; Skyhøj Olsen, T.; Lassen, N.A.; Paulson, O.B. Changes in regional cerebral blood flow during the course of classic migraine attacks. Ann. Neurol. 1983, 13, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Pezzini, A.; Grassi, M.; Lodigiani, C.; Patella, R.; Gandolfo, C.; Zini, A.; Delodovici, M.L.; Paciaroni, M.; Del Sette, M.; Toriello, A.; et al. Predictors of long-term recurrent vascular events after ischemic stroke at young age: The Italian Project on Stroke in Young Adults. Circulation 2014, 129, 1668–1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ornello, R.; Canonico, M.; Merki-Feld, G.S.; Kurth, T.; Lidegaard, Ø.; MacGregor, E.A.; Lampl, C.; Nappi, R.E.; Martelletti, P.; Sacco, S. Migraine, low-dose combined hormonal contraceptives, and ischemic stroke in young women: A systematic review and suggestions for future research. Expert. Rev. Neurother. 2020, 20, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Kurth, T.; Winter, A.C.; Eliassen, A.H.; Dushkes, R.; Mukamal, K.J.; Rimm, E.B.; Willett, W.C.; Manson, J.E.; Rexrode, K.M. Migraine and risk of cardiovascular disease in women: Prospective cohort study. BMJ 2016, 353, i2610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lidegaard, O. Oral contraceptives, pregnancy and the risk of cerebral thromboembolism: The influence of diabetes, hypertension, migraine and previous thrombotic disease. Br. J. Obstet. Gynaecol. 1995, 102, 153–159. [Google Scholar] [CrossRef] [PubMed]
- MacClellan, L.R.; Giles, W.; Cole, J.; Wozniak, M.; Stern, B.; Mitchell, B.D.; Kittner, S.J. Probable migraine with visual aura and risk of ischemic stroke: The stroke prevention in young women study. Stroke 2007, 38, 2438–2445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allais, G.; Chiarle, G.; Sinigaglia, S.; Airola, G.; Schiapparelli, P.; Benedetto, C. Estrogen, migraine, and vascular risk. Neurol. Sci. 2018, 39 (Suppl. 1), 11–20. [Google Scholar] [CrossRef]
- Correia, P.; Machado, S.; Meyer, I.; Amiguet, M.; Eskandari, A.; Michel, P. Ischemic stroke on hormonal contraceptives: Characteristics, mechanisms and outcome. Eur. Stroke J. 2021, 6, 205–212. [Google Scholar] [CrossRef]
- No authors listed. Oral contraceptives and stroke in young women. Associated risk factors. JAMA 1975, 231, 718–722. [Google Scholar] [CrossRef]
- Tzourio, C.; Tehindrazanarivelo, A.; Iglésias, S.; Alpérovitch, A.; Chedru, F.; d’Anglejan-Chatillon, J.; Bousser, M.G. Case-control study of migraine and risk of ischaemic stroke in young women. BMJ 1995, 310, 830–833. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, S.M.; Petitti, D.B.; Siscovick, D.S.; Longstreth, W.T.; Sidney, S.; Raghunathan, T.E.; Quesenberry, C.P., Jr.; Kelaghan, J. Stroke and use of low-dose oral contraceptives in young women: A pooled analysis of two US studies. Stroke 1998, 29, 2277–2284. [Google Scholar] [CrossRef] [Green Version]
- Champaloux, S.W.; Tepper, N.K.; Monsour, M.; Curtis, K.M.; Whiteman, M.K.; Marchbanks, P.A.; Jamieson, D.J. Use of combined hormonal contraceptives among women with migraines and risk of ischemic stroke. Am. J. Obstet. Gynecol. 2017, 216, e1–e489. [Google Scholar] [CrossRef]
- Chang, C.L.; Donaghy, M.; Poulte, N. Migraine and stroke in young women: Case-control study. The World Health Organisation Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. BMJ 1999, 318, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Nightingale, A.L.; Farmer, R.D. Ischemic stroke in young women: A nested case-control study using the UK General Practice Research Database. Stroke 2004, 35, 1574–1578. [Google Scholar] [CrossRef] [Green Version]
- Milhaud, D.; Bogousslavsky, J.; van Melle, G.; Liot, P. Ischemic stroke and active migraine. Neurology 2001, 57, 1805–1811. [Google Scholar] [CrossRef]
- Pezzini, A.; Grassi, M.; Lodigiani, C.; Patella, R.; Gandolfo, C.; Casoni, F.; Musolino, R.; Calabrò, R.S.; Bovi, P.; Adami, A.; et al. Predictors of migraine subtypes in young adults with ischemic stroke: The Italian project on stroke in young adults. Stroke 2011, 42, 17–21. [Google Scholar] [CrossRef] [Green Version]
- MacGregor, E.A.; Hackshaw, A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology 2004, 63, 351–353. [Google Scholar] [CrossRef]
- Steiner, T.J.; Stovner, L.J.; Jensen, R.; Uluduz, D.; Katsarava, Z. Lifting The Burden: The Global Campaign against Headache. Migraine remains second among the world’s causes of disability, and first among young women: Findings from GBD2019. J. Headache Pain 2020, 21, 137. [Google Scholar] [CrossRef]
- Vetvik, K.G.; Macgregor, E.A.; Lundqvist, C.; Russell, M.B. Prevalence of menstrual migraine: A population-based study. Cephalalgia 2014, 34, 280–288. [Google Scholar] [CrossRef] [Green Version]
- MacGregor, E.A. “Menstrual” migraine: Towards a definition. Cephalalgia 1996, 16, 11–21. [Google Scholar] [CrossRef]
- Pavlovic, J.M.; Paemeleire, K.; Göbel, H.; Bonner, J.; Rapoport, A.; Kagan, R.; Zhang, F.; Picard, H.; Mikol, D.D. Efficacy and safety of erenumab in women with a history of menstrual migraine. J. Headache Pain 2020, 21, 95. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, P. Hormonal factors in migraine: A population-based study of women aged 40 to 74 years. Headache 2003, 43, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Lipton, R.B.; Chee, E.; Sawyer, J.; Silberstein, S.D. Menstrual cycle and headache in a population sample of migraineurs. Neurology 2000, 55, 1517–1523. [Google Scholar] [CrossRef]
- Johannes, C.B.; Linet, M.S.; Stewart, W.F.; Celentano, D.D.; Lipton, R.B.; Szklo, M. Relationship of headache to phase of the menstrual cycle among young women: A daily diary study. Neurology 1995, 45, 1076–1082. [Google Scholar] [CrossRef]
- Nappi, G.; Jensen, R.; Nappi, R.E.; Sances, G.; Torelli, P.; Olesen, J. Diaries and calendars for migraine. A review. Cephalalgia 2006, 26, 905–916. [Google Scholar] [CrossRef] [PubMed]
- Tassorelli, C.; Jensen, R.; Allena, M.; De Icco, R.; Katsarava, Z.; Miguel Lainez, J.; Leston, J.A.; Fadic, R.; Spadafora, S.; Pagani, M.; et al. The added value of an electronic monitoring and alerting system in the management of medication-overuse headache: A controlled multicentre study. Cephalalgia 2017, 37, 1115–1125. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.; Tassorelli, C.; Rossi, P.; Allena, M.; Osipova, V.; Steiner, T.; Sandrini, G.; Olesen, J.; Nappi, G.; Basic Diagnostic Headache Diary Study Group. A basic diagnostic headache diary (BDHD) is well accepted and useful in the diagnosis of headache. a multicentre European and Latin American study. Cephalalgia 2011, 31, 1549–1560. [Google Scholar] [CrossRef]
- Pinkerman, B.; Holroyd, K. Menstrual and nonmenstrual migraines differ in women with menstrually-related migraine. Cephalalgia 2010, 30, 1187–1194. [Google Scholar] [CrossRef]
- Marcus, D.A.; Bernstein, C.D.; Sullivan, E.A.; Rudy, T.E. A prospective comparison between ICHD-II and probability menstrual migraine diagnostic criteria. Headache 2010, 50, 539–550. [Google Scholar] [CrossRef]
- Noutsios, C.D.; Boisvert-Plante, V.; Perez, J.; Hudon, J.; Ingelmo, P. Telemedicine Applications for the Evaluation of Patients with Non-Acute Headache: A Narrative Review. J. Pain Res. 2021, 14, 1533–1542. [Google Scholar] [CrossRef]
- Barra, M.; Dahl, F.A.; Vetvik, K.G.; MacGregor, E.A. A Markov chain method for counting and modelling migraine attacks. Sci. Rep. 2020, 10, 3631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, I.; Singh, D. Progesterone in the treatment of migraine. Lancet 1947, 1, 745–747. [Google Scholar] [CrossRef]
- Beckham, J.C.; Krug, L.M.; Penzien, D.B.; Johnson, C.A.; Mosley, T.H.; Meeks, G.R.; Pbert, L.A.; Prather, R.C. The relationship of ovarian steroids, headache activity and menstrual distress: A pilot study with female migraineurs. Headache 1992, 32, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Calhoun, A.H.; Gill, N. Presenting a New, Non-Hormonally Mediated Cyclic Headache in Women: End-Menstrual Migraine. Headache 2017, 57, 17–20. [Google Scholar] [CrossRef]
- Gür-Özmen, S.; Karahan-Özcan, R. Iron Deficiency Anemia Is Associated with Menstrual Migraine: A Case-Control Study. Pain Med. 2016, 17, 596–605. [Google Scholar] [CrossRef] [Green Version]
- Chabbert-Buffet, N.; Gerris, J.; Jamin, C.; Lello, S.; Lete, I.; Lobo, P.; Nappi, R.E.; Pintiaux, A. Toward a new concept of “natural balance” in oral estroprogestin contraception. Gynecol. Endocrinol. 2013, 29, 891–896. [Google Scholar] [CrossRef]
- Lete, I.; Chabbert-Buffet, N.; Jamin, C.; Lello, S.; Lobo, P.; Nappi, R.E.; Pintiaux, A. Haemostatic and metabolic impact of estradiol pills and drospirenone-containing ethinylestradiol pills vs. levonorgestrel-containing ethinylestradiol pills: A literature review. Eur. J. Contracept. Reprod. Health Care 2015, 20, 329–343. [Google Scholar] [CrossRef]
- Dinger, J.; Do Minh, T.; Heinemann, K. Impact of estrogen type on cardiovascular safety of combined oral contraceptives. Contraception 2016, 94, 328–339. [Google Scholar] [CrossRef]
- Reed, S.; Koro, C.; DiBello, J.; Becker, K.; Bauerfeind, A.; Franke, C.; Heinemann, K. Prospective controlled cohort study on the safety of a monophasic oral contraceptive containing nomegestrol acetate (2.5 mg) and 17β-oestradiol (1.5 mg) (PRO-E2 study): Risk of venous and arterial thromboembolism. Eur. J. Contracept. Reprod. Health Care 2021, 26, 439–446. [Google Scholar] [CrossRef]
- Douxfils, J.; Klipping, C.; Duijkers, I.; Kinet, V.; Mawet, M.; Maillard, C.; Jost, M.; Rosing, J.; Foidart, J.M. Evaluation of the effect of a new oral contraceptive containing estetrol and drospirenone on hemostasis parameters. Contraception 2020, 102, 396–402. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Year | Type of Study | Type of Migraine | Type of Treatment | Treatment Regimen | Treatment Duration, N Menstrual Cycles/Months | Sample Size | Age, Years ± SD or Range | Efficacy (Yes/No) |
|---|---|---|---|---|---|---|---|---|
| Oral | ||||||||
| De Leo et al., 2011 [117] | RCT | PMM | EE 20 μg + DRSP 3 mg | 21/7 vs. 24/4 | 3 | 60 | 28.15 ± 6.96 27.77 ± 7.44 | Yes (24/4 superior to 21/7) |
| Nappi et al., 2013 [118] | open label | MRM | step-down E2V + step-up DNG | 26/2 | 6 | 28 | 40.6 ± 3.5 | Yes |
| Calhoun et al., 2004 [119] | open label | MRM | COCs with EE 20 μg + 0.9 mg CEE | 21/7 COCs + short prevention for 7 days (22–28) | 2 | 11 | 41 (28–50) | Yes |
| MacGregor et al., 2002 [120] | crossover PL-controlled trial | migraine during the HFI | COCs with different doses of EE + 50 μg E2 patches | 21/7 COCs + short prevention for 7 days (22–28) | 4 | 13 | 33 (24–42) | No |
| Coffee et al., 2014 [121] | RCT | MRM | EE 30 μg + LNG 150 μg | 21/7 COCs vs. 168 extended-cycle regimen | 6 | 32 (21 no prior COCs users; 11 prior COCs users) | 33.5 ± 6.8 no prior COCs users; 33.9 ± 6.7 prior COCs users | Yes |
| Transvaginal ring | ||||||||
| Calhoun et al., 2012 [125] | open label | MRM with aura | EE 15 μg + ENG 0.120 mg + E2 75 μg transdermal patches | 84/7 + short prevention for 7 days (from 85 to 91) | 3 | 23 | 32.4 (19–55) | Yes |
| Study Year | Type of Study | Type of Migraine | Type of Treatment | Treatment Regimen | Treatment Duration, N of Menstrual Cycles/Months | Sample Size | Age, Years ± SD or Range | Efficacy (Yes/No) |
|---|---|---|---|---|---|---|---|---|
| Estradiol patches | ||||||||
| Smite et al., 1994 [130] | PL cross over trial | PMM | E2 50 μg transdermal patches | short-term (from −2 to day +5) | 3 | 20 | (30–48) | No |
| Almen-Christensson et al., 2011 [131] | PL controlled RCT | PMM | E2 100 μg transdermal patches | short-term (from −7 to day +7) | 3 | 27 | 39.6 ± 4.3 | No |
| Guidotti et al., 2007 [132] | open label | MM | E2 25 μg patches, frovatriptan 2.5 mg, naproxen sodium 500 mg | short-term (from −2 to day +4) | NA | 38 (14 frovatriptan; 20 E2 patches, 14 naproxen sodium) | 29 ± 4 (E2 patches arm) | No |
| Add-back therapies | ||||||||
| Murray et al., 1997 [133] | open label | PMM | GnRH-A 3.75 mg, E2 100 μg + MPA 2.5 mg | 10 months with GnRH-A (4 alone +6 with hormonal treatment) | 15 | 5 | NA | Yes |
| Estradiol gel | ||||||||
| de Lignieres et al., 1986 [135] | crossover PL-controlled trial | PMM | E2 1.5 mg | short-term (from −2 to day +5) | 3 | 20 | 42.5 (32–53) | Yes |
| Dennerstein et al., 1988 [136] | crossover PL-controlled trial | PMM | E2 1.5 mg | short-term (from −2 to day +5) | 4 | 22 | 39.8 ± 3.95 | Yes |
| MacGregor et al., 2006 [137] | crossover PL-controlled trial | PMM or MRM | E2 1.5 mg | short-term (from −6 to day +2) | 6 | 35 | 43 (29–50) | Yes |
| Estradiol implants | ||||||||
| Magos et al., 1983 [138] | open label | PMM | E2 implants: 100 mg/75 mg/50 mg + NETA 5 mg | Continuous estrogens + 7 days progestogen | up to 5 years | 24 | 40.6 (32–51) | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nappi, R.E.; Tiranini, L.; Sacco, S.; De Matteis, E.; De Icco, R.; Tassorelli, C. Role of Estrogens in Menstrual Migraine. Cells 2022, 11, 1355. https://doi.org/10.3390/cells11081355
Nappi RE, Tiranini L, Sacco S, De Matteis E, De Icco R, Tassorelli C. Role of Estrogens in Menstrual Migraine. Cells. 2022; 11(8):1355. https://doi.org/10.3390/cells11081355
Chicago/Turabian StyleNappi, Rossella E., Lara Tiranini, Simona Sacco, Eleonora De Matteis, Roberto De Icco, and Cristina Tassorelli. 2022. "Role of Estrogens in Menstrual Migraine" Cells 11, no. 8: 1355. https://doi.org/10.3390/cells11081355
APA StyleNappi, R. E., Tiranini, L., Sacco, S., De Matteis, E., De Icco, R., & Tassorelli, C. (2022). Role of Estrogens in Menstrual Migraine. Cells, 11(8), 1355. https://doi.org/10.3390/cells11081355