
Minimal Residual Disease in Colorectal Cancer: Are We Finding the Needle in a Haystack?


Abstract
:1. Introduction
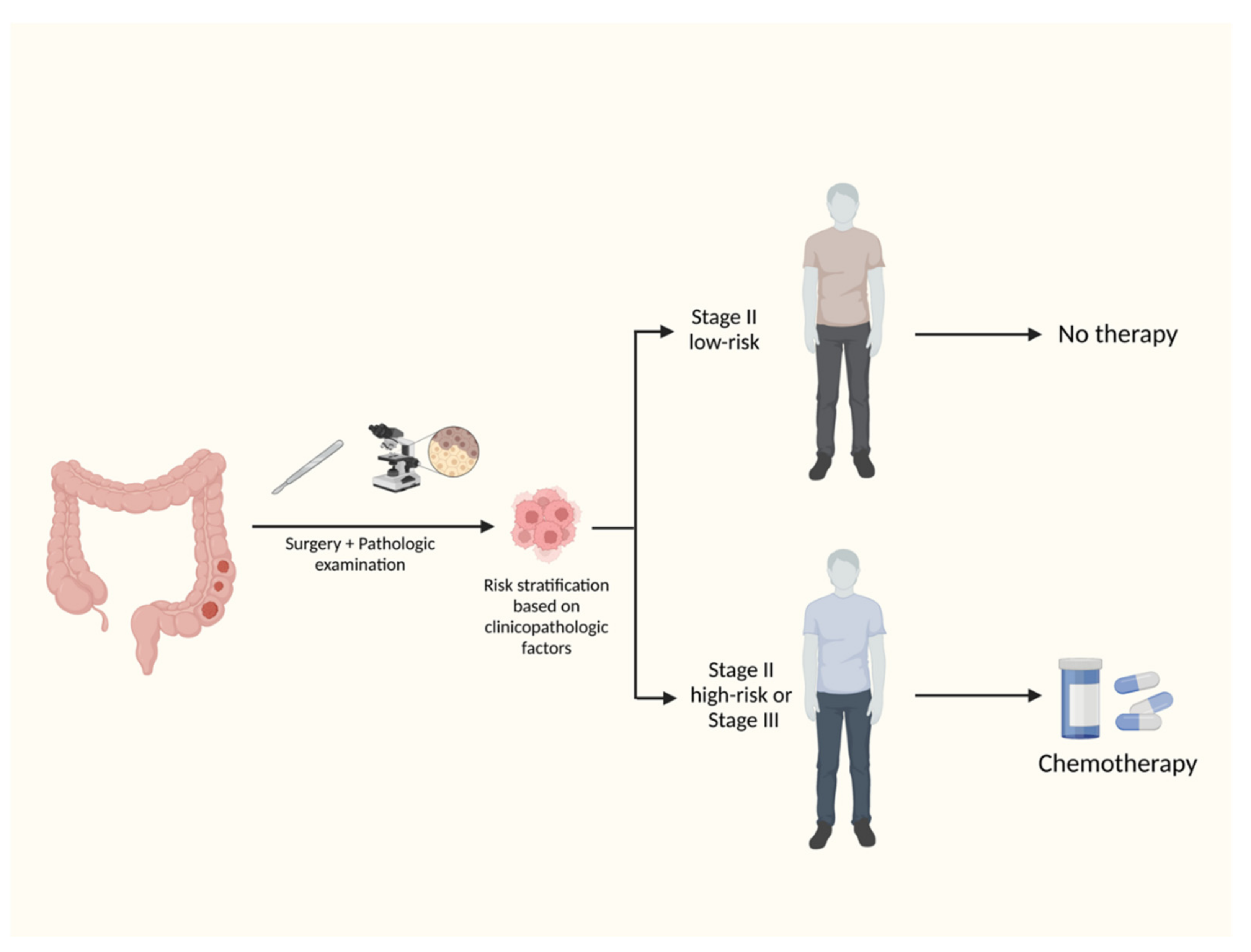
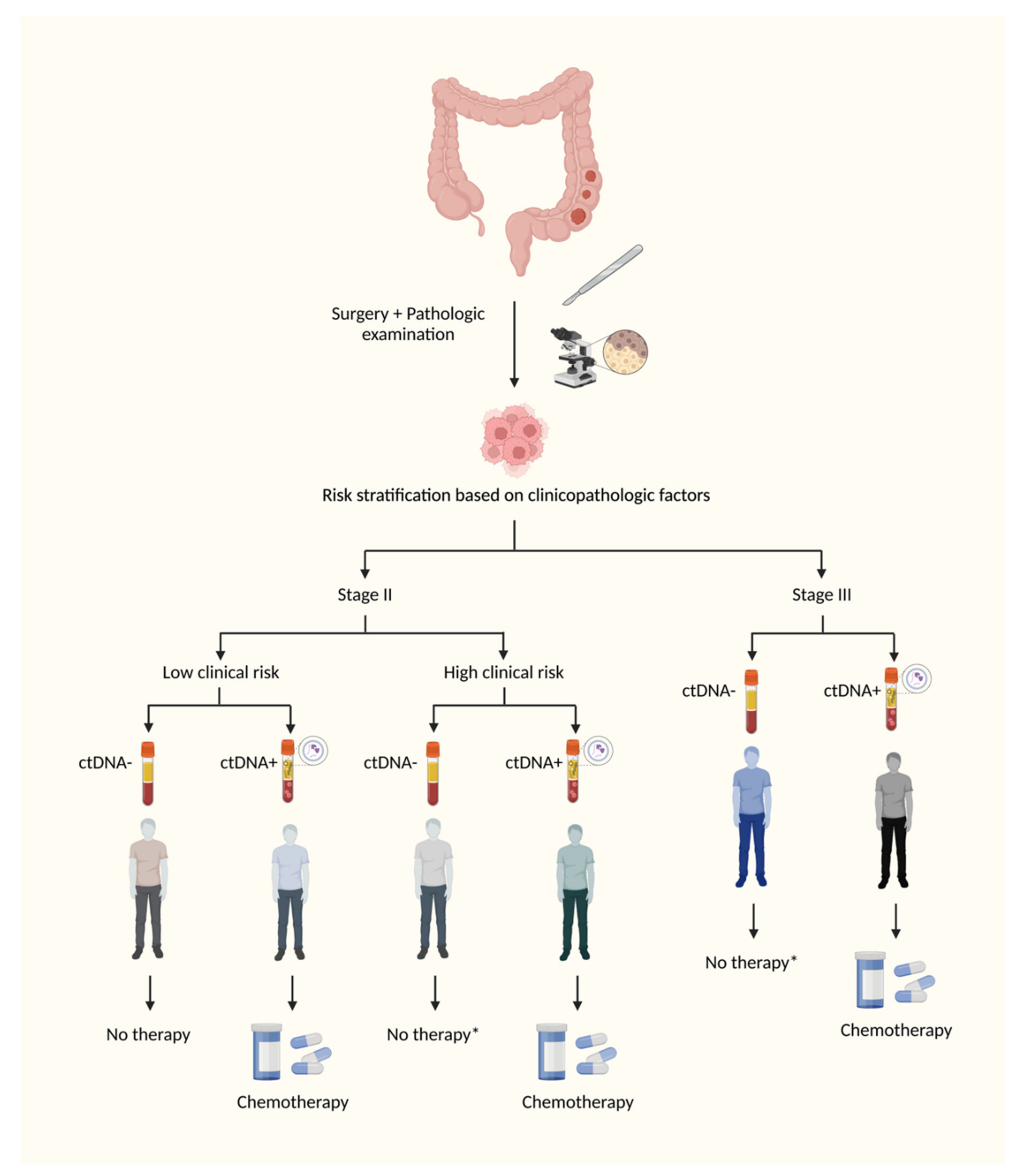
2. Standard of Care of Adjuvant Therapy of Colon Cancer
3. DNA Sequencing Methodologies
4. Completed Studies
5. MRD in Rectal Cancer
6. MRD in Metastatic Colorectal Cancer
7. Ongoing Clinical Trials
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Moertel, C.G. Accomplishments in surgical adjuvant therapy for large bowel cancer. Cancer 1992, 70 (Suppl. 5), 1364–1371. [Google Scholar] [CrossRef]
- André, T.; Boni, C.; Mounedji-Boudiaf, L.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Zaninelli, M.; Clingan, P.; Bridgewater, J.; et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N. Engl. J. Med. 2004, 350, 2343–2351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. NCCN guidelines insights: Colon cancer, version 2. J. Natl. Compr. Cancer Netw. 2018, 16, 359–369. [Google Scholar] [CrossRef] [Green Version]
- Baxter, N.N.; Kennedy, E.B.; Bergsland, E.; Berlin, J.; George, T.J.; Gill, S.; Gold, P.J.; Hantel, A.; Jones, L.; Lieu, C.; et al. Adjuvant therapy for stage II colon cancer: ASCO guideline update. J. Clin. Oncol. 2022, 40, 892–910. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L. Colon cancer, version 2.2021, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef]
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef]
- Weiser, M.R.; Gönen, M.; Chou, J.F.; Kattan, M.W.; Schrag, D. Predicting survival after curative colectomy for cancer: Individualizing colon cancer staging. J. Clin. Oncol. 2011, 29, 4796–4802. [Google Scholar] [CrossRef] [Green Version]
- Sargent, D.J.; Marsoni, S.; Monges, G.; Thibodeau, S.N.; Labianca, R.; Hamilton, S.R.; French, A.J.; Kabat, B.; Foster, N.R.; Torri, V.; et al. Defective mismatch repair as a predictive marker for lack of efficacy of fluorouracil-based adjuvant therapy in colon cancer. J. Clin. Oncol. 2010, 28, 3219–3226. [Google Scholar] [CrossRef] [Green Version]
- Sargent, D.J.; Marsoni, S.; Thibodeau, S.N.; Labianca, R.; Hamilton, S.R.; Torri, V.; Monges, G.; Ribic, C.; Grothey, A.; Gallinger, S. Confirmation of deficient mismatch repair (dMMR) as a predictive marker for lack of benefit from 5-FU based chemotherapy in stage II and III colon cancer (CC): A pooled molecular reanalysis of randomized chemotherapy trials. J. Clin. Oncol. 2008, 26 (Suppl. S15), 4008. [Google Scholar] [CrossRef]
- André, T.; Boni, C.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Bonetti, A.; Clingan, P.; Bridgewater, J.; Rivera, F.; et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J. Clin. Oncol. 2009, 27, 3109–3116. [Google Scholar] [CrossRef] [Green Version]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef]
- McCleary, N.J.; Meyerhardt, J.A.; Green, E.; Yothers, G.; De Gramont, A.; Van Cutsem, E.; O’Connell, M.; Twelves, C.J.; Saltz, L.B.; Haller, D.G.; et al. Impact of age on the efficacy of newer adjuvant therapies in patients with stage II/III colon cancer: Findings from the ACCENT database. J. Clin. Oncol. 2013, 31, 2600–2606. [Google Scholar] [CrossRef]
- Cohen, R.; Taieb, J.; Fiskum, J.; Yothers, G.; Goldberg, R.; Yoshino, T.; Alberts, S.; Allegra, C.; de Gramont, A.; Seitz, J.-F. Microsatellite instability in patients with stage III colon cancer receiving fluoropyrimidine with or without oxaliplatin: An ACCENT pooled analysis of 12 adjuvant trials. J. Clin. Oncol. 2021, 39, 642. [Google Scholar] [CrossRef]
- Tougeron, D.; Mouillet, G.; Trouilloud, I.; Lecomte, T.; Coriat, R.; Aparicio, T.; Des Guetz, G.; Lécaille, C.; Artru, P.; Sickersen, G. Efficacy of adjuvant chemotherapy in colon cancer with microsatellite instability: A large multicenter AGEO study. J. Natl. Cancer Inst. 2016, 108, djv438. [Google Scholar] [CrossRef]
- Fan, H.C.; Blumenfeld, Y.J.; Chitkara, U.; Hudgins, L.; Quake, S.R. Analysis of the size distributions of fetal and maternal cell-free DNA by paired-end sequencing. Clin. Chem. 2010, 56, 1279–1286. [Google Scholar] [CrossRef] [Green Version]
- Corcoran, R.B.; Chabner, B.A. Application of cell-free DNA analysis to cancer treatment. N. Engl. J. Med. 2018, 379, 1754–1765. [Google Scholar] [CrossRef] [Green Version]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef] [Green Version]
- Diaz, L.A., Jr.; Bardelli, A. Liquid biopsies: Genotyping circulating tumor DNA. J. Clin. Oncol. 2014, 32, 579–586. [Google Scholar] [CrossRef]
- Xie, M.; Lu, C.; Wang, J.; McLellan, M.D.; Johnson, K.J.; Wendl, M.C.; McMichael, J.F.; Schmidt, H.K.; Yellapantula, V.; Miller, C.A.; et al. Age-related mutations associated with clonal hematopoietic expansion and malignancies. Nat. Med. 2014, 20, 1472–1478. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.G.; Malapelle, U.; André, F.; Paz-Ares, L.; Schuler, M.; Thomas, D.M.; Vainer, G.; Yoshino, T.; Rolfo, C. Practical considerations for the use of circulating tumor DNA in the treatment of patients with cancer: A narrative review. JAMA Oncol. 2022, 8, 1830–1839. [Google Scholar] [CrossRef]
- Schøler, L.V.; Reinert, T.; Ørntoft, M.-B.W.; Kassentoft, C.G.; Árnadóttir, S.S.; Vang, S.; Nordentoft, I.; Knudsen, M.; Lamy, P.; Andreasen, D.; et al. Clinical Implications of Monitoring Circulating Tumor DNA in Patients with Colorectal Cancer. Clin. Cancer Res. 2017, 23, 5437–5445. [Google Scholar] [CrossRef] [Green Version]
- Reinert, T.; Henriksen, T.V.; Christensen, E.; Sharma, S.; Salari, R.; Sethi, H.; Knudsen, M.; Nordentoft, I.; Wu, H.-T.; Tin, A.S.; et al. Analysis of plasma cell-free DNA by ultradeep sequencing in patients with stages I to III colorectal cancer. JAMA Oncol. 2019, 5, 1124–1131. [Google Scholar] [CrossRef] [Green Version]
- Parikh, A.R.; Van Seventer, E.E.; Siravegna, G.; Hartwig, A.V.; Jaimovich, A.; He, Y.; Kanter, K.; Fish, M.G.; Fosbenner, K.D.; Miao, B.; et al. Minimal Residual Disease Detection using a Plasma-only Circulating Tumor DNA Assay in Patients with Colorectal Cancer. Clin. Cancer Res. 2021, 27, 5586–5594. [Google Scholar] [CrossRef]
- Taieb, J.; Taly, V.; Henriques, J.; Bourreau, C.; Mineur, L.; Bennouna, J.; Desrame, J.; Louvet, C.; Lepere, C.; Mabro, M.; et al. Prognostic Value and Relation with Adjuvant Treatment Duration of ctDNA in Stage III Colon Cancer: A Post Hoc Analysis of the PRODIGE-GERCOR IDEA-France Trial. Clin. Cancer Res. 2021, 27, 5638–5646. [Google Scholar] [CrossRef] [PubMed]
- Kotaka, M.; Shirasu, H.; Watanabe, J.; Yamazaki, K.; Hirata, K.; Akazawa, N.; Matsuhashi, N.; Yokota, M.; Ikeda, M.; Kato, K.; et al. Association of circulating tumor DNA dynamics with clinical outcomes in the adjuvant setting for patients with colorectal cancer from an observational GALAXY study in CIRCULATE-Japan. J. Clin. Oncol. 2022, 40, 9. [Google Scholar] [CrossRef]
- Tie, J.; Cohen, J.D.; Lahouel, K.; Lo, S.N.; Wang, Y.; Kosmider, S.; Wong, R.; Shapiro, J.; Lee, M.; Harris, S.; et al. Circulating tumor DNA analysis guiding adjuvant therapy in stage II colon cancer. N. Engl. J. Med. 2022, 386, 2261–2272. [Google Scholar] [CrossRef]
- Garrigou, S.; Perkins, G.; Garlan, F.; Normand, C.; Didelot, A.; Le Corre, D.; Peyvandi, S.; Mulot, C.; Niarra, R.; Aucouturier, P.; et al. A study of hypermethylated circulating tumor DNA as a universal colorectal cancer biomarker. Clin. Chem. 2016, 62, 1129–1139. [Google Scholar] [CrossRef] [Green Version]
- Laurent-Puig, P.; Bouché, O.; Niarra, R.; Aucouturier, P.; Benhaim, L.; Landi, B.; Berger, A.; Lecomte, T.; Normand, C.; Le Corre, D.; et al. Circulating tumor DNA as a prognostic marker in colorectal cancer: Preliminary results of a prospective trial. Cancer Res. 2015, 75 (Suppl. 15), 5235. [Google Scholar] [CrossRef]
- Zitt, M.; Müller, H.M.; Rochel, M.; Schwendinger, V.; Zitt, M.; Goebel, G.; DeVries, A.; Margreiter, R.; Oberwalder, M.; Zeillinger, R.; et al. Circulating cell-free DNA in plasma of locally advanced rectal cancer patients undergoing preoperative chemoradiation: A potential diagnostic tool for therapy monitoring. Dis. Markers 2008, 25, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Agostini, M.; Pucciarelli, S.; Enzo, M.V.; Del Bianco, P.; Briarava, M.; Bedin, C.; Maretto, I.; Friso, M.L.; Lonardi, S.; Mescoli, C.; et al. Circulating cell-free DNA: A promising marker of pathologic tumor response in rectal cancer patients receiving preoperative chemoradiotherapy. Ann. Surg. Oncol. 2011, 18, 2461–2468. [Google Scholar] [CrossRef]
- Sun, W.; Sun, Y.; Zhu, M.; Wang, Z.; Zhang, H.; Xin, Y.; Jiang, G.; Guo, X.; Zhang, Z.; Liu, Y. The role of plasma cell-free DNA detection in predicting preoperative chemoradiotherapy response in rectal cancer patients. Oncol. Rep. 2014, 31, 1466–1472. [Google Scholar] [CrossRef] [Green Version]
- Carpinetti, P.; Donnard, E.; Bettoni, F.; Asprino, P.; Koyama, F.; Rozanski, A.; Sabbaga, J.; Habr-Gama, A.; Parmigiani, R.B.; Galante, P.A.; et al. The use of personalized biomarkers and liquid biopsies to monitor treatment response and disease recurrence in locally advanced rectal cancer after neoadjuvant chemoradiation. Oncotarget 2015, 6, 38360–38371. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.-T.; Tufts, L.; Aggarwal, P.; Heller, F.; Weiser, M.R. Detection of methylated BCAT1 and IKZF1 in stage II/III rectal cancer receiving chemoradiation. J. Clin. Oncol. 2019, 37, 602. [Google Scholar] [CrossRef]
- Yang, L.; Wang, Y.; Bao, H.; Wan, J.; Fan, X.; Bao, H.; Shen, L.; Guan, Y.; Wu, X.; Shao, Y.; et al. ctDNA as a potential prognostic marker for locally advanced rectal cancer patients with ‘watch and wait’ approach. J. Clin. Oncol. 2019, 37, 3544. [Google Scholar] [CrossRef]
- Li, M.; Xiao, W.; Zhao, G.Q.; Guo, Z.; Yang, X.; Lin, S.; Ying, K.; Li, M.; Gao, Y.-H. Predictive value of circulating tumor DNA in locally advanced rectal cancer patients receiving neoadjuvant radiochemotherapy. J. Clin. Oncol. 2017, 35, e15125. [Google Scholar] [CrossRef]
- Shepherdson, M.; Symonds, E.L.; Byrne, S.; Gormly, K.; Karapetis, C.S.; Vatandoust, S.; Young, G.P.; Roy, A.C. Circulating tumor DNA and circumferential resection margin as key prognostic indicators for survival in rectal cancer. J. Clin. Oncol. 2021, 39, 3579. [Google Scholar] [CrossRef]
- Tie, J.; Cohen, J.D.; Wang, Y.; Li, L.; Christie, M.; Simons, K.; Elsaleh, H.; Kosmider, S.; Wong, R.; Yip, D.; et al. Serial circulating tumour DNA analysis during multimodality treatment of locally advanced rectal cancer: A prospective biomarker study. Gut 2019, 68, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Lin, G.; Gong, Y.; Zhang, Y.; Guan, Y.-F.; Xia, X.; Yi, X.; Xue, X.; Bai, X.; Yang, L. Serial ctDNA analysis as a real-time indicator of neoadjuvant chemoradiotherapy in rectal cancer. J. Clin. Oncol. 2019, 37, 3569. [Google Scholar] [CrossRef]
- Morris, E.J.A.; Forman, D.; Thomas, J.D.; Quirke, P.; Taylor, E.F.; Fairley, L.; Cottier, B.; Poston, G. Surgical management and outcomes of colorectal cancer liver metastases. Br. J. Surg. 2010, 97, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Guiguet, M.; Vaillant, J.C.; Balladur, P.; Boudjema, K.; Bachellier, P.; Jaeck, D. Surgical resection of colorectal carcinoma metastases to the liver: A prognostic scoring system to improve case selection, based on 1568 patients. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1996, 77, 1254–1262. [Google Scholar] [CrossRef]
- Tomlinson, J.S.; Jarnagin, W.R.; DeMatteo, R.P.; Fong, Y.; Kornprat, P.; Gonen, M.; Kemeny, N.; Brennan, M.F.; Blumgart, L.H.; D’Angelica, M. Actual 10-year survival after resection of colorectal liver metastases defines cure. J. Clin. Oncol. 2007, 25, 4575–4580. [Google Scholar] [CrossRef]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): Long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013, 14, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Kanemitsu, Y.; Shimizu, Y.; Mizusawa, J.; Inaba, Y.; Hamaguchi, T.; Shida, D.; Ohue, M.; Komori, K.; Shiomi, A.; Shiozawa, M.; et al. Hepatectomy followed by mFOLFOX6 versus hepatectomy alone for liver-only metastatic colorectal cancer (JCOG0603): A phase II or III randomized controlled trial. J. Clin. Oncol. 2021, 39, 3789–3799. [Google Scholar] [CrossRef]
- Loupakis, F.; Sharma, S.; Derouazi, M.; Murgioni, S.; Biason, P.; Rizzato, M.D.; Rasola, C.; Renner, D.; Shchegrova, S.; Koyen Malashevich, A.; et al. Detection of molecular residual disease using personalized circulating tumor DNA assay in patients with colorectal cancer undergoing resection of metastases. JCO Precis. Oncol. 2021, 5, 1166–1177. [Google Scholar] [CrossRef]
- Wang, D.-S.; Yang, H.; Liu, X.-Y.; Chen, Z.-G.; Wang, Y.; Fong, W.P.; Hu, M.-T.; Zheng, Y.-C.; Zheng, Y.; Li, B.-K.; et al. Dynamic monitoring of circulating tumor DNA to predict prognosis and efficacy of adjuvant chemotherapy after resection of colorectal liver metastases. Theranostics 2021, 11, 7018–7028. [Google Scholar] [CrossRef]
- Tie, J.; Wang, Y.; Cohen, J.; Li, L.; Hong, W.; Christie, M.; Wong, H.L.; Kosmider, S.; Wong, R.; Thomson, B.; et al. Circulating tumor DNA dynamics and recurrence risk in patients undergoing curative intent resection of colorectal cancer liver metastases: A prospective cohort study. PLoS Med. 2021, 18, e1003620. [Google Scholar] [CrossRef]
- Marmorino, F.; Prisciandaro, M.; Giordano, M.; Ortolan, E.; Crucitta, S.; Manca, P.; Antoniotti, C.; Valenti, M.M.; Danesi, R.; Conca, V.; et al. Circulating Tumor DNA as a Marker of Minimal Residual Disease After Radical Resection of Colorectal Liver Metastases. JCO Precis. Oncol. 2022, 6, e2200244. [Google Scholar] [CrossRef] [PubMed]
- Reinert, T.; Petersen, L.M.S.; Henriksen, T.V.; Larsen, M.Ø.; Rasmussen, M.H.; Johansen, A.F.B.; Øgaard, N.; Knudsen, M.; Nordentoft, I.; Vang, S.; et al. Circulating tumor DNA for prognosis assessment and postoperative management after curative-intent resection of colorectal liver metastases. Int. J. Cancer 2022, 150, 1537–1548. [Google Scholar] [CrossRef]
- Nishioka, Y.; Chun, Y.S.; Overman, M.J.; Cao, H.S.T.; Tzeng, C.-W.D.; Mason, M.C.; Kopetz, S.W.; Bauer, T.W.; Vauthey, J.-N.; Newhook, T.E. Effect of co-mutation of RAS and TP53 on postoperative ctDNA detection and early recurrence after hepatectomy for colorectal liver metastases. J. Am. Coll. Surg. 2022, 234, 474–483. [Google Scholar] [CrossRef]
- Boysen, A.K.; Pallisgaard, N.; Andersen, C.S.A.; Spindler, K.-L.G. Circulating tumor DNA as a marker of minimal residual disease following local treatment of metastases from colorectal cancer. Acta Oncol. 2020, 59, 1424–1429. [Google Scholar] [CrossRef]
- Morris, V.K.; Overman, M.J.; Lam, M.; Parseghian, C.M.; Johnson, B.; Dasari, A.; Raghav, K.; Kee, B.K.; Huey, R.; Wolff, R.A. Bintrafusp Alfa, an Anti-PD-L1: TGFβ Trap Fusion Protein, in Patients with ctDNA-positive, Liver-limited Metastatic Colorectal Cancer. Cancer Res. Commun. 2022, 2, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Wang, Y.; Tomasetti, C.; Li, L.; Springer, S.; Kinde, I.; Silliman, N.; Tacey, M.; Wong, H.-L.; Christie, M.; et al. Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer. Sci. Transl. Med. 2016, 8, 346ra92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarazona, N.; Gimeno-Valiente, F.; Gambardella, V.; Zuñiga, S.; Rentero-Garrido, P.; Huerta, M.; Roselló, S.; Martinez-Ciarpaglini, C.; Carbonell-Asins, J.A.; Carrasco, F.; et al. Targeted next-generation sequencing of circulating-tumor DNA for tracking minimal residual disease in localized colon cancer. Ann. Oncol. 2019, 30, 1804–1812. [Google Scholar] [CrossRef] [Green Version]
- Tie, J.; Cohen, J.D.; Wang, Y.; Christie, M.; Simons, K.; Lee, M.; Wong, R.; Kosmider, S.; Ananda, S.; McKendrick, J.; et al. Circulating tumor DNA analyses as markers of recurrence risk and benefit of adjuvant therapy for stage III colon cancer. JAMA Oncol. 2019, 5, 1710–1717. [Google Scholar] [CrossRef]
- Li, Y.; Mo, S.; Zhang, L.; Ma, X.; Hu, X.; Huang, D.; Lu, B.; Luo, C.; Peng, H.; Cai, S.; et al. Postoperative circulating tumor DNA combined with consensus molecular subtypes can better predict outcomes in stage III colon cancers: A prospective cohort study. Eur. J. Cancer 2022, 169, 198–209. [Google Scholar] [CrossRef]
- Lonardi, S.; Nimeiri, H.; Xu, C.; Zollinger, D.R.; Madison, R.W.; Fine, A.D.; Gjoerup, O.; Rasola, C.; Angerilli, V.; Sharma, S.; et al. Comprehensive Genomic Profiling (CGP)-Informed Personalized Molecular Residual Disease (MRD) Detection: An Exploratory Analysis from the PREDATOR Study of Metastatic Colorectal Cancer (mCRC) Patients Undergoing Surgical Resection. Int. J. Mol. Sci. 2022, 23, 11529. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | N | Stage | Median Follow-up Time (m) | Assay | Risk of Recurrence in ctDNA+ Pts (n/N) | Risk of Recurrence in ctDNA- Pts (n/N) | HR RFS (95% CI) |
|---|---|---|---|---|---|---|---|
| Tie et al. [27] | 230 | II | 27.0 | Tumor-informed | 11/14 (79%) | 16/164 (10%) | 18.0 (7.9–40.0) |
| Reinert et al. [24] | 130 | I–III | 12.5 | Tumor-informed | 7/10 (70%) | 10/84 (12%) | 0.21 (0.06–0.69) |
| Tarazona et al. [28] | 150 | I–III | 24.7 | Tumor-informed | 8/14 (57%) | 9/55 (16%) | 11.6 (3.6–36.8) |
| Parikh et al. [25] | 103 | I–IV | 21.0 | Plasma-only | 15/17(88%) | 12/49 (25%) | 11.4 (NR) |
| Taieb et al. [26] | 1017 | III | 79.2 | Plasma-only | 93/140 (66%) | 673/877 (77%) | 1.5 (1.1–2.1) |
| Tie et al. [29] | 100 | III | 28.9 | Tumor-informed | 10/20 (50%) | 14/76 (18%) | 7.5 (3.5–16.1) |
| Kotaka et al. [30] | 1050 | I–IV | 11.4 | Tumor-informed | 91/188 (48%) | 52/852 (6%) | 15.3 (8.6–27.2) |
| Marmorino et al. [31] | 76 | IV | 77.0 | Tumor-informed | 33/39 (84%) | 20/37 (54%) | 1.8 (1.0–3.3) |
| Li et al. [32] | 165 | III | 33.5 | Tumor-informed | 13/24 (54%) | 26/127 (21%) | 5.5 (2.4–12.3) |
| Lonardi et al. [33] | 69 | IV | NR | Tumor-informed | 29/31 (94%) | 19/38 (50%) | 6.4 (3.0–14.0) |
| Tie et al. [34] | 455 | II | 37.0 | Tumor-informed | 8/45 (18%) | 15/246 (6%) | 1.8 (0.7–4.2) |
| Population | N | Intervention in ctDNA+ Pts | Primary Objective | Identifier |
|---|---|---|---|---|
| Single-arm studies | ||||
| I–III | 300 | None | Rate of ctDNA+ | NCT04726800 |
| II–IV | 15 | CB-NK cells + cetuximab | ctDNA clearance rate | NCT05040568 |
| II–IV | 17 | 3-month aspirin + vitamin D + diet + physical activity | ctDNA clearance rate | NCT05036109 |
| II–IV | 15 | Trifluridine/tipiracil | ctDNA clearance rate | NCT05343013 |
| II–IV | 15 | CXCR1/2 inhibitor (SX-682) + nivolumab (STOPTRAFFIC-1) | ctDNA clearance rate | NCT04599140 |
| II–IV with MRD after ACT | 22 | Trifluridine/tipiracil + irinotecan | Rate of ctDNA+ after CT | NCT04920032 |
| IV after hepatectomy | 120 | FOLFOX or FOLFIRI ± bevacizumab | 1-year RFS | NCT05062317 |
| Randomized studies | ||||
| II–III with MRD after 3-month ACT | 236 | 3-month FOLFOXIRI vs. 3-month FOLFOX/CAPOX | 3-year DFS rate | NCT05534087 |
| IIA (COBRA) | 1408 | 6-month FOLFOX/CAPOX s. active surveillance | ctDNA clearance rate | NCT04068103 |
| II–III with MRD after surgery (CIRCULATE-US) | 1912 | 6-month FOLFOX/CAPOX vs. 6-month FOLFIRINOX | ctDNA clearance rate | NCT05174169 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jácome, A.A.; Johnson, B. Minimal Residual Disease in Colorectal Cancer: Are We Finding the Needle in a Haystack? Cells 2023, 12, 1068. https://doi.org/10.3390/cells12071068
Jácome AA, Johnson B. Minimal Residual Disease in Colorectal Cancer: Are We Finding the Needle in a Haystack? Cells. 2023; 12(7):1068. https://doi.org/10.3390/cells12071068
Chicago/Turabian StyleJácome, Alexandre A., and Benny Johnson. 2023. "Minimal Residual Disease in Colorectal Cancer: Are We Finding the Needle in a Haystack?" Cells 12, no. 7: 1068. https://doi.org/10.3390/cells12071068
APA StyleJácome, A. A., & Johnson, B. (2023). Minimal Residual Disease in Colorectal Cancer: Are We Finding the Needle in a Haystack? Cells, 12(7), 1068. https://doi.org/10.3390/cells12071068