

Scarring and Skin Fibrosis Reversal with Regenerative Surgery and Stem Cell Therapy

Abstract
:1. Introduction
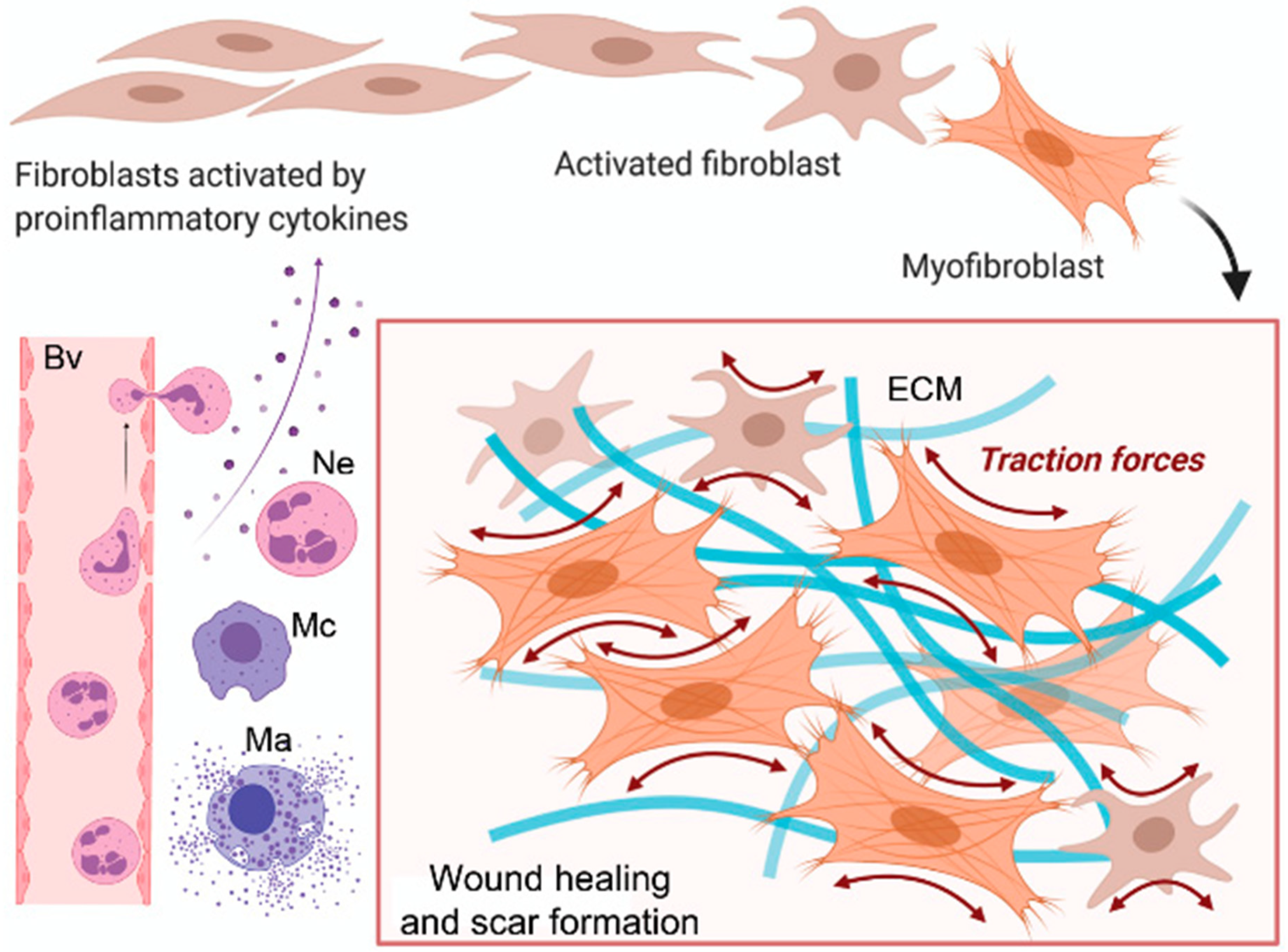
1.1. Cellular Dysfunction in Fibrosis and Scarring
1.2. Conventional Therapies for Fibrosis and Scarring
1.3. Cellular Therapy for Fibrosis and Scarring
2. Aim of the Study
3. Types of Adipose Stem Cell-Based Therapies
3.1. Fat Grafting
3.2. ASCs and SVF
3.3. Combined Approaches
Fat Grafting Mixed with PRP
4. Application in Fibrotic Skin Conditions
4.1. Hypertrophic Scars
4.2. Burns
4.3. Radiation-Induced Fibrosis (RF)
4.4. Dupuytren’s Disease
4.5. Lichen Sclerosus
4.6. Scleroderma
5. Discussion
5.1. Mechanism of Action of ASCs-Based Therapies in Dermal Fibrosis
5.2. Surgical Variability
5.3. Limitations of the Application of ASCs
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Walraven, M.; Hinz, B. Therapeutic approaches to control tissue repair and fibrosis. Matrix Biol. 2018, 71–72, 205–224. [Google Scholar] [CrossRef]
- Rockey, D.C.; Bell, P.D.; Hill, J.A. Fibrosis—A common pathway to organ injury and failure. N. Engl. J. Med. 2015, 12, 1138–1149. [Google Scholar] [CrossRef]
- Borthwick, L.A.; Wynn, T.A.; Fisher, A.J. Cytokine mediated tissue fibrosis. Biochim. Biophys. Acta 2013, 1832, 1049–1060. [Google Scholar] [CrossRef]
- Luzina, I.G.; Atamas, S.P. Fibrotic Skin Diseases. In Clinical and Basic Immunodermatology; Gaspari, A.A., Tyring, S.K., Eds.; Springer: London, UK, 2008. [Google Scholar]
- Karppinen, S.M.; Heljasvaara, R.; Gullberg, D.; Tasanen, K.; Pihlajaniemi, T. Toward understanding scarless skin wound healing and pathological scarring. F1000Research 2019, 8, 787. [Google Scholar] [CrossRef]
- Wynn, T.A. Cellular and molecular mechanisms of fibrosis. J. Pathol. 2008, 214, 199–210. [Google Scholar] [CrossRef]
- Jones, R.E.; Foster, D.S.; Hu, M.S.; Longaker, M.T. Wound healing and fibrosis: Current stem cell therapies. Transfusion 2019, 59, 884–892. [Google Scholar] [CrossRef]
- Tsou, P.-S. Cellular Mechanisms of Tissue Fibrosis. 8. Current and future drug targets in fibrosis: Focus on Rho GTPase-regulated gene transcription. Am. J. Physiol. Cell Physiol. 2014, 307, C2–C13. [Google Scholar] [CrossRef]
- Wynn, T.A.; Ramalingam, T.R. Mechanisms of fibrosis: Therapeutic translation for fibrotic disease. Nat. Med. 2012, 18, 1028–1040. [Google Scholar] [CrossRef]
- Wells, J.M.; Gaggar, A.; Blalock, J.E. MMP generated matrikines. Matrix Biol. 2015, 44, 122–129. [Google Scholar] [CrossRef]
- Fertala, J.; Wang, M.L.; Rivlin, M.; Beredjiklian, P.K.; Abboud, J.; Arnold, W.V.; Fertala, A. Extracellular Targets to Reduce Excessive Scarring in Response to Tissue Injury. Biomolecules 2023, 13, 758. [Google Scholar] [CrossRef]
- Garg, S.P.; Weissman, J.P.; Reddy, N.K.; Varghese, J.; Ellis, M.F.; Kim, J.Y.S.; Galiano, R.D. Patient-reported outcomes of scar impact: Comparing of abdominoplasty, breast surgery, and facial surgery patients. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4574. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Burns. Available online: www.who.int/mediacentre/factsheets/fs365/en/ (accessed on 12 January 2024).
- Peck, M.D. Epidemiology of burns throughout the world. Part I: Distribution and risk factors. Burns 2011, 37, 1087–1100. [Google Scholar] [CrossRef]
- Moiemen, N.; Mathers, J.; Jones, L.; Bishop, J.; Kinghorn, P.; Monahan, M.; Calvert, M.; Slinn, G.; Gardiner, F.; Bamford, A.; et al. Pressure garment to prevent abnormal scarring after burn injury in adults and children: The PEGASUS feasibility RCT and mixed-methods study. Health Technol. Assess. 2018, 22, 1–162. [Google Scholar] [CrossRef]
- Gangemi, E.N.; Gregori, D.; Berchialla, P.; Zingarelli, E.; Cairo, M.; Bollero, D.; Ganem, J.; Capocelli, R.; Cuccuru, F.; Cassano, P.; et al. Epidemiology and risk factors for pathologic scarring after burn wounds. Arch. Facial Plast. Surg. 2008, 10, 93–102. [Google Scholar] [CrossRef]
- Wynn, T.A. Fibrotic disease and the TH1/TH2 paradigm. Nat. Rev. Immunol. 2004, 4, 583–594. [Google Scholar] [CrossRef]
- Finnerty, C.C.; Jeschke, M.G.; Branski, L.K.; Barret, J.P.; Dziewulski, P.; Herndon, D.N. Hypertrophic scarring: The greatest unmet challenge after burn injury. Lancet 2016, 388, 1427–1436. [Google Scholar] [CrossRef]
- Candy, L.H.; Cecilia, L.T.; Ping, Z.Y. Effect of different pressure magnitudes on hypertrophic scar in a Chinese population. Burns 2010, 36, 1234–1241. [Google Scholar] [CrossRef]
- Engrav, L.H.; Heimbach, D.M.; Rivara, F.P.; Moore, M.L.; Wang, J.; Carrougher, G.J.; Costa, B.; Numhom, S.; Calderon, J.; Gibran, N.S. 12-Year within-wound study of the effectiveness of custom pressure garment therapy. Burns 2010, 36, 975–983. [Google Scholar] [CrossRef]
- Arno, A.I.; Gauglitz, G.G.; Barret, J.P.; Jeschke, M.G. Up-to-date approach to manage keloids and hypertrophic scars: A useful guide. Burns 2014, 40, 1255–1266. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.J.; Williams, E.A.; Pham, C.H.; Collier, Z.J.; Dang, J.; Yenikomshian, H.A.; Gillenwater, T.J. Fractional CO2 laser treatment for burn scar improvement: A systematic review and meta-analysis. Burns 2021, 47, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.; Brieva, T.; Raviv, L.; Rowley, J.; Niss, K.; Brandwein, H.; Oh, S.; Karnieli, O. Concise Review: Process Development Considerations for Cell Therapy. Stem Cells Transl. Med. 2015, 4, 1155–1163. [Google Scholar] [CrossRef]
- Mason, C.; Brindley, D.A.; Culme-Seymour, E.J.; Davie, N.L. Cell therapy industry: Billion dollar global business with unlimited potential. Regen. Med. 2011, 6, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Gimble, J.M.; Bunnell, B.A.; Chiu, E.S.; Guilak, F. Concise review: Adipose-derived stromal vascular fraction cells and stem cells: Let’s not get lost in translation. Stem Cells 2011, 29, 749–754. [Google Scholar] [CrossRef]
- Raafat, N.; Abdel Aal, S.M.; Abdo, F.K.; El Ghonaimy, N.M. Mesenchymal stem cells: In vivo therapeutic application ameliorates carbon tetrachloride induced liver fibrosis in rats. Int. J. Biochem. Cell Biol. 2015, 68, 109–118. [Google Scholar] [CrossRef]
- Barczyk, M. Stem Cell-Based Therapy in Idiopathic Pulmonary Fibrosis. Stem Cell Rev. Rep. 2015, 11, 598–620. [Google Scholar] [CrossRef]
- Fatkhudinov, T. Bone Marrow-Derived Multipotent Stromal Cells Promote Myocardial Fibrosis and Reverse Remodeling of the Left Ventricle. Stem Cells Int. 2015, 2015, 746873. [Google Scholar] [CrossRef]
- Da Silva, A.F. Bone Marrow-Derived Mesenchymal Stem Cells and Their Conditioned Medium Attenuate Fibrosis in an Irreversible Model of Unilateral Ureteral Obstruction. Cell Transplant. 2015, 24, 2657–2666. [Google Scholar] [CrossRef]
- Dong, L.-H. The anti-fibrotic effects of mesenchymal stem cells on irradiated lungs via stimulating endogenous secretion of HGF and PGE2. Sci. Rep. 2015, 5, 8713. [Google Scholar] [CrossRef]
- Lindroos, B.; Suuronen, R.; Miettinen, S. The Potential of Adipose Stem Cells in Regenerative Medicine. Stem Cell Rev. Rep. 2011, 7, 269–291. [Google Scholar] [CrossRef]
- Zuk, P.A.; Zhu, M.; Ashjian, P.; De Ugarte, D.A.; Huang, J.I.; Mizuno, H.; Alfonso, Z.C.; Fraser, J.K.; Benhaim, P.; Hedrick, M.H. Human adipose tissue is a source of multipotent stem cells. Mol. Cell 2002, 13, 4279–4295. [Google Scholar] [CrossRef]
- Gimble, J.M.; Katz, A.J.; Bunnell, B.A. Adipose- derived stem cells for regenerative medicine. Circ. Res. 2007, 100, 1249–1260. [Google Scholar] [CrossRef]
- Gimble, J.; Guilak, F. Adipose-derived adult stem cells: Isolation, characterization, and differentiation potential. Cytotherapy 2003, 5, 362–369. [Google Scholar] [CrossRef]
- Lynn, J.V.; Ranganathan, K.; Luby, A.O.; Urlaub, K.M.; Donneys, A.; Nelson, N.S.; Buchman, S.R. Therapeutic efficacy of adipose-derived stem cells versus bone marrow stromal cells for irradiated mandibular fracture repair. Ann. Plast. Surg. 2022, 89, 459–464. [Google Scholar] [CrossRef]
- Coleman, S.R. Structural fat grafts: The ideal filler? Clin. Plast. Surg. 2001, 28, 111–119. [Google Scholar] [CrossRef]
- Tonnard, P.; Verpaele, A.; Peeters, G.; Hamdi, M.; Cornelissen, M.; Declercq, H. Nanofat Grafting. Plast. Reconstr. Surg. 2013, 132, 1017–1026. [Google Scholar] [CrossRef]
- Sesé, B.; Sanmartín, J.M.; Ortega, B.; Matas-Palau, A.; Llull, R. Nanofat Cell Aggregates. Plast. Reconstr. Surg. 2019, 144, 1079–1088. [Google Scholar] [CrossRef]
- Serra-Mestre, J.M.; Serra-Renom, J.M.; Martinez, L.; Almadori, A.; D’Andrea, F. Platelet-Rich Plasma Mixed-Fat Grafting: A Reasonable Prosurvival Strategy for Fat GraftS? Aesth Plast. Surg. 2014, 38, 1041–1049. [Google Scholar] [CrossRef]
- Zhang, X.; Li, G. Effectiveness of fat grafting in scar reduction: A systematic review and meta-analysis. J. Cosmet. Dermatol. 2022, 21, 5804–5810. [Google Scholar] [CrossRef]
- Zhengcai, W. Effect of Nanofat on Wound Healing in Rats with Diabetes. Master’s Thesis, Zhejiang University, Hangzhou, China, 2019. [Google Scholar]
- Kemaloğlu, C.A.; Özyazgan, İ.; Gönen, Z.B. Immediate fat and nanofat-enriched fat grafting in breast reduction for scar management. J. Plast. Surg. Hand Surg. 2021, 55, 173–180. [Google Scholar] [CrossRef]
- Zou, Y.L.; Tan, X.; Tian, T.; Li, L.; Li, Z.X.; Cheng, W.; Wang, Z.X. Clinical effect of nano-fat mixed granule fat transplantation in the treatment of cicatricial facial depression and atrophy and the related experimental mechanism. Chin. J. Burns 2019, 04, 266–276. [Google Scholar]
- Cervelli, V.; Nicoli, F.; Spallone, D.; Verardi, S.; Sorge, R.; Nicoli, M.; Balzani, A. Treatment of traumatic scars using fat grafts mixed with platelet-rich plasma, and resurfacing of skin with the 1540 nm nonablative laser. Clin. Exp. Dermatol. 2012, 37, 55–61. [Google Scholar] [CrossRef]
- Rageh, M.A.; Tawfik, A.A.; Abdallah, N.; Ibrahim, S.M.A. Fractional CO2 laser combined with autologous nanofat injection versus fractional CO2 laser combined with platelet-rich plasma in the treatment of atrophic acne scars: A split-face comparative study with optical skin imaging. Dermatol. Surg. 2024, 50, 75–80. [Google Scholar] [CrossRef]
- Goel, A.; Shrivastava, P. Post-burn scars and scar contractures. Indian. J. Plast. Surg. 2010, 43, S63–S71. [Google Scholar] [CrossRef]
- Seo, B.F.; Jung, S.N. The Immunomodulatory Effects of Mesenchymal Stem Cells in Prevention or Treatment of Excessive Scars. Stem Cells Int. 2016, 2016, 6937976. [Google Scholar] [CrossRef]
- Condé-Green, A.; Marano, A.A.; Lee, E.S.; Reisler, T.; Price, L.A.; Milner, S.M.; Granick, M.S. Fat Grafting and Adipose-Derived Regenerative Cells in Burn Wound Healing and Scarring: A Systematic Review of the Literature. Plast. Reconstr. Surg. 2016, 137, 302–312. [Google Scholar] [CrossRef]
- Klinger, M.; Marazzi, M.; Vigo, D.; Torre, M. Fat injection for cases of severe burn outcomes: A new perspective of scar remodeling and reduction. Aesthetic Plast. Surg. 2008, 32, 465–469. [Google Scholar] [CrossRef]
- Brongo, S.; Nicoletti, G.F.; La Padula, S.; Mele, C.M.; D’Andrea, F. Use of lipofilling for the treatment of severe burn outcomes. Plast. Reconstr. Surg. 2012, 130, 374e–376e. [Google Scholar] [CrossRef]
- Viard, R.; Bouguila, J.; Voulliaume, D.; Comparin, J.-P.; Dionyssopoulos, A.; Foyatier, J.-L. La lipostructure dans les séquelles de brülures facials. Ann. Chir. Plast. Esthétique 2011, 57, 217–229. [Google Scholar] [CrossRef]
- Byrne, M. Early experience with fat grafting as an adjunct for secondary burn reconstruction in the hand: Technique, hand function assessment and aesthetic outcomes. Burns 2016, 42, 356–365. [Google Scholar] [CrossRef]
- Sultan, S.M.; Barr, J.S.; Butala, P.; Davidson, E.H.; Weinstein, A.L.; Knobel, D.; Saadeh, P.B.; Warren, S.M.; Coleman, S.R.; Hazen, A. Fat grafting accelerates revascularisation and decreases fibrosis following thermal injury. J. Plast. Reconstr. Aesthetic Surg. 2011, 65, 219–227. [Google Scholar] [CrossRef]
- Gu, Z.; Li, Y.; Li, H. Use of Condensed Nanofat Combined with Fat Grafts to Treat Atrophic Scars. JAMA Facial Plast. Surg. 2018, 20, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Jan, S.N.; Bashir, M.M.; Khan, F.A.; Hidayat, Z.; Ansari, H.H.; Sohail, M.; Bajwa, A.B.; Shami, H.B.; Hanif, A.; Aziz, F.; et al. Unfiltered Nanofat Injections Rejuvenate Postburn Scars of Face. Ann. Plast. Surg. 2019, 82, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Rohani Ivari, J.; Mahdipour, E. Adipose tissue versus stem cell-derived small extracellular vesicles to enhance the healing of acute burns. Regen. Med. 2021, 16, 629–641. [Google Scholar] [CrossRef]
- Carstens, M.H.; Correa, D.; Llull, R.; Gomez, A.; Turner, E.; Valladares, L.S. Subcutaneous reconstruction of hand dorsum and fingers for late sequelae of burn scars using adipose-derived stromal vascular fraction (SVF). CellR4 2015, 3, e1675. [Google Scholar]
- Elkahky, H.O.; Fathy, G.; Abu-Zahra, F.A.; Afify, A.A. Autologous adipose-derived adult stem cells injection versus platelet-rich plasma injection in the treatment of rolling postacne scars. J. Egypt. Womens Dermatol. Soc. 2016, 13, 165–172. [Google Scholar] [CrossRef]
- Gentile, P.; Scioli, M.G.; Bielli, A.; Orlandi, A.; Cervelli, V. Comparing different nanofat procedures on scars: Role of the stromal vascular fraction and its clinical implications. Regen. Med. 2017, 12, 939–952. [Google Scholar] [CrossRef] [PubMed]
- Carstens, M.H.; Pérez, M.; Briceño, H.; Valladares, S.; Correa, D. Treatment of late sequelae of burn scar fibrosis with adipose derived stromal vascular fraction (SVF) cells: A case series. CellR4 2017, 5, e2404. [Google Scholar]
- Shawn Loder, B.A. Wound Healing Immediately Post-Thermal Injury Is Improved by Fat and Adipose Derived Stem Cell Isografts. J. Burn Care Res. 2015, 36, 70–76. [Google Scholar] [CrossRef]
- Denham, J.; Hauer-Jensen, M. The radiotherapeutic injury–A complex “wound”. Radiother. Oncol. 2002, 63, 129–145. [Google Scholar] [CrossRef] [PubMed]
- Rigotti, G.; Marchi, A.; Mirco, G.; Guido, B.; Donatella, B.; Mauro, K.; Annalisa, P.; Andrea, S. Clinical Treatment of Radiotherapy Tissue Damage by Lipoaspirate Transplant: A Healing Process Mediated by Adipose-Derived Adult Stem Cells. Plast. Reconstr. Surg. 2007, 119, 1409–1422. [Google Scholar] [CrossRef]
- Griffin, M.F.; Drago, J.; Almadori, A.; Kalavrezos, N.; Butler, P.E. Evaluation of the efficacy of lipotransfer to manage radiation-induced fibrosis and volume defects in head and neck oncology. Head Neck 2019, 41, 3647–3655. [Google Scholar] [CrossRef]
- Salgarello, M.; Visconti, G.; Farallo, E. Autologous fat graft in radiated tissue prior to alloplastic reconstruction of the breast: Report of two cases. Aesthetic Plast. Surg. 2010, 34, 5–10. [Google Scholar] [CrossRef]
- Salgarello, M.; Visconti, G.; Barone-Adesi, L. Fat grafting and breast reconstruction with implant: Another option for irradiated breast cancer patients. Plast. Reconstr. Surg. 2012, 129, 317–329. [Google Scholar] [CrossRef]
- Serra-Renom, J.M.; Muñoz-Olmo, J.L.; Serra-Mestre, J.M. Fat grafting in postmastectomy breast reconstruction with expanders and prostheses in patients who have received radiotherapy: Formation of new subcutaneous tissue. Plast. Reconstr. Surg. 2010, 125, 12–18. [Google Scholar] [CrossRef]
- Panettiere, P.; Marchetti, L.; Accorsi, D. The serial free fat transfer in irradiated prosthetic breast reconstructions. Aesthetic Plast. Surg. 2009, 33, 695–700. [Google Scholar] [CrossRef]
- Sarfati, I.; Ihrai, T.; Kaufman, G.; Nos, C.; Clough, K.B. Adipose-tissue grafting to the post-mastectomy irradiated chest wall: Preparing the ground for implant reconstruction. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, 1161–1166. [Google Scholar] [CrossRef]
- Sarfati, I.; Ihrai, T.; Duvernay, A.; Nos, C.; Clough, K. Transfert de tissu adipeux autologue préalable a la reconstruction mammaire par implant après mastectomie et irradiation: A propos d’une série de 68 cas. Ann. Chir. Plast. Esthétique 2013, 58, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Phulpin, B.; Gangloff, P.; Tran, N.; Bravetti, P.; Merlin, J.L.; Dolivet, G. Rehabilitation of Irradiated Head and Neck Tissues by Autologous Fat Transplantation. Plast. Reconstr. Surg. 2009, 123, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.M.; Stern, C.S.; Allen Jr, R.J.; Thanik, V.D.; Chang, C.C.; Nguyen, P.D.; Canizares, O.; Szpalski, C.; Saadeh, P.B.; Warren, S.M.; et al. Human Fat Grafting Alleviates Radiation Skin Damage in a Murine Model. Plast. Reconstr. Surg. 2011, 128, 363–372. [Google Scholar] [CrossRef]
- Luan, A.; Duscher, D.; Whittam, A.J.; Paik, K.J.; Zielins, E.R.; Brett, E.A.; Atashroo, D.A.; Hu, M.S.; Lee, G.K.; Gurtner, G.C.; et al. Cell-Assisted Lipotransfer Improves Volume Retention in Irradiated Recipient Sites and Rescues Radiation-Induced Skin Changes. Stem Cells 2016, 34, 668–673. [Google Scholar] [CrossRef]
- Yao, C.; Zhou, Y.; Wang, H.; Deng, F.; Chen, Y.; Zhu, X.; Kong, Y.; Pan, L.; Xue, L.; Zhou, X.; et al. Adipose-derived stem cells alleviate radiation-induced dermatitis by suppressing apoptosis and downregulating cathepsin F expression. Stem Cell Res. Ther. 2021, 12, 447. [Google Scholar] [CrossRef]
- Yu, D.; Zhang, S.; Mo, W.; Jiang, Z.; Wang, M.; An, L.; Wang, Y.; Liu, Y.; Jiang, S.; Wu, A.; et al. Transplantation of the stromal vascular fraction (SVF) mitigates severe radiation-induced skin injury. Radiat. Res. 2021, 196, 250–260. [Google Scholar] [CrossRef]
- Chen, Y.; Niu, Z.; Xue, Y.; Yuan, F.; Fu, Y.; Bai, N. Improvement in the repair of defects in maxillofacial soft tissue in irradiated minipigs by a mixture of adipose-derived stem cells and platelet-rich fibrin. Br. J. Oral Maxillofac. Surg. 2014, 52, 740–745. [Google Scholar] [CrossRef]
- Rehman, S.; Goodacre, R.; Day, P.J.; Bayat, A.; Westerhoff, H.V. Dupuytren’s: A systems biology disease. Arthritis Res. Ther. 2011, 13, 238. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, A.M.P.; Kirkpatrick, J.J.R.; Naylor, I.L. Dupuytren’s disease—The way forward? J. Hand Surg. Br. Eur. Vol. 1999, 24, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Au-Yong, I.T.H.; Wildin, C.J.; Dias, J.J.; Page, R.E. A review of common practice in Dupuytren surgery. Tech. Hand Extrem. Surg. 2005, 9, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Badalamente, M.A.; Hurst, L.C.; Hentz, V.R. Collagen as a clinical target: Nonoperative treatment of Dupuytren’s disease. J. Hand Surg. 2002, 27, 788–798. [Google Scholar] [CrossRef] [PubMed]
- Gilpin, D.; Coleman, S.; Hall, S.; Houston, A.; Karrasch, J.; Jones, N. Injectable collagenase Clostridium histolyticum: A new nonsurgical treatment for Dupuytren’s disease. J. Hand Surg. Am. 2010, 35, 2027–2038. [Google Scholar] [CrossRef] [PubMed]
- Hovius, S.E.R.; Kan, H.J.; Smit, X.; Selles, R.W.; Cardoso, E.; Khouri, R.K. Extensive Percutaneous Aponeurotomy and Lipografting: A New Treatment for Dupuytren Disease. Plast. Reconstr. Surg. 2011, 128, 221–228. [Google Scholar] [CrossRef]
- Verhoekx, J.S.N.; Mudera, V.; Walbeehm, E.T.; Hovius, S.E.R. Adipose-Derived Stem Cells Inhibit the Contractile Myofibroblast in Dupuytren’s Disease. Plast. Reconstr. Surg. 2013, 132, 1139–1148. [Google Scholar] [CrossRef]
- De Luca, D.A.; Papara, C.; Vorobyev, A.; Staiger, H.; Bieber, K.; Thaçi, D.; Ludwig, R.J. Lichen sclerosus: The 2023 update. Front. Med. 2023, 10, 1106318. [Google Scholar] [CrossRef]
- Almadori, A.; Hansen, E.; Boyle, D.; Zenner, N.; Swale, V.; Reid, W.; Maclane, A.; Butler, P.E.M. Fat Grafting Improves Fibrosis and Scarring in Vulvar Lichen Sclerosus: Results From a Prospective Cohort Study. J. Low. Genit. Tract Dis. 2020, 24, 305–310. [Google Scholar] [CrossRef]
- Boero, V.; Brambilla, M.; Sipio, E.; Liverani, C.A.; Di Martino, M.; Agnoli, B.; Libutti, G.; Cribiù, F.M.; Del Gobbo, A.; Ragni, E.; et al. Vulvar lichen sclerosus: A new regenerative approach through fat grafting. Gynecol. Oncol. 2015, 139, 471–475. [Google Scholar] [CrossRef]
- Casabona, F.; Priano, V.; Vallerino, V.; Cogliandro, A.; Lavagnino, G. New surgical approach to lichen sclerosus of the vulva: The role of adipose-derived mesenchymal cells and platelet-rich plasma in tissue regeneration. Plast. Reconstr. Surg. 2010, 126, 210e–211e. [Google Scholar] [CrossRef]
- Tamburino, S.; Lombardo, G.A.; Tarico, M.S.; Perrotta, R.E. The Role of Nanofat Grafting in Vulvar Lichen Sclerosus: A Preliminary Report. Arch. Plast. Surg. 2016, 43, 93–95. [Google Scholar] [CrossRef]
- Gutierrez-Ontalvilla, P.; Giner, F.; Vidal, L.; Iborra, M. The Effect of Lipofilling and Platelet-Rich Plasma on Patients with Moderate-Severe Vulvar Lichen Sclerosus who were Non-Responders to Topical Clobetasol Propionate: A Randomized Pilot Study. Aesthetic Plast. Surg. 2022, 46, 2469–2479. [Google Scholar] [CrossRef]
- Monreal, J. Safety and Efficacy of Stromal Vascular Fraction Enriched Fat Grafting Therapy for Vulvar Lichen Sclerosus. Cureus 2020, 12, e7096. [Google Scholar] [CrossRef]
- Giuseppina Onesti, M.; Carella, S.; Ceccarelli, S.; Marchese, C.; Scuderi, N. The Use of Human Adipose-Derived Stem Cells in the Treatment of Physiological and Pathological Vulvar Dystrophies. Stem Cells Int. 2016, 2016, 2561461. [Google Scholar] [CrossRef]
- Newman, N.; Rogowski, N.; Newman, D.; Talavera-Adame, D. Autologous Adipose-Derived Stem Cell Treatment for Women with Genital Lichen Sclerosus. Gynecol. Reprod. Health 2018, 2, 1–4. [Google Scholar] [CrossRef]
- Jinnin, M. Mechanisms of skin fibrosis in systemic sclerosis. J. Dermatol. 2010, 37, 11–25. [Google Scholar] [CrossRef]
- Matucci-Cerinic, M. The complexity of managing systemic sclerosis: Screening and diagnosis. Rheumatology 2009, 8 (Suppl. 3), iii8–iii13. [Google Scholar] [CrossRef]
- Almadori, A.; Griffin, M.; Ryan, C.M.; Hunt, D.F.; Hansen, E.; Kumar, R.; Abraham, D.J.; Denton, C.P.; Butler, P.E.M. Stem cell enriched lipotransfer reverses the effects of fibrosis in systemic sclerosis. PLoS ONE 2019, 14, e0218068. [Google Scholar] [CrossRef]
- Strong, A.L.; Adidharma, W.; Brown, O.H.; Cederna, P.S. Fat Grafting Subjectively Improves Facial Skin Elasticity and Hand Function of Scleroderma Patients. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3373. [Google Scholar] [CrossRef]
- Pignatti, M.; Spinella, A.; Cocchiara, E.; Boscaini, G.; Lusetti, I.L.; Citriniti, G.; Lumetti, F.; Setti, G.; Dominici, M.; Salvarani, C.; et al. Autologous Fat Grafting for the Oral and Digital Complications of Systemic Sclerosis: Results of a Prospective Study. Aesthetic Plast. Surg. 2020, 44, 1820–1832. [Google Scholar] [CrossRef]
- Blezien, O.; D’Andrea, F.; Nicoletti, G.F.; Ferraro, G.A. Effects of Fat Grafting Containing Stem Cells in Microstomia and Microcheilia Derived from Systemic Sclerosis. Aesthetic Plast. Surg. 2017, 41, 839–844. [Google Scholar] [CrossRef]
- Del Papa, N.; Caviggioli, F.; Sambataro, D.; Zaccara, E.; Vinci, V.; Di Luca, G.; Parafioriti, A.; Armiraglio, E.; Maglione, W.; Polosa, R.; et al. Autologous fat grafting in the treatment of fibrotic perioral changes in patients with systemic sclerosis. Cell Transplant. 2015, 24, 63–72. [Google Scholar] [CrossRef]
- Sautereau, N.; Daumas, A.; Truillet, R.; Jouve, E.; Magalon, J.; Veran, J.; Casanova, D.; Frances, Y.; Magalon, G.; Granel, B. Efficacy of Autologous Microfat Graft on Facial Handicap in Systemic Sclerosis Patients. Plast. Reconstr. Surg. Glob. Open 2016, 4, e660. [Google Scholar] [CrossRef]
- Onesti, M.G.; Fioramonti, P.; Carella, S.; Fino, P.; Marchese, C.; Scuderi, N. Improvement of Mouth Functional Disability in Systemic Sclerosis Patients over One Year in a Trial of Fat Transplantation versus Adipose-Derived Stromal Cells. Stem Cells Int. 2016, 2016, 2416192. [Google Scholar] [CrossRef]
- Virzì, F.; Bianca, P.; Giammona, A.; Apuzzo, T.; Di Franco, S.; Mangiapane, L.R.; Colorito, M.L.; Catalano, D.; Scavo, E.; Nicotra, A.; et al. Combined platelet-rich plasma and lipofilling treatment provides great improvement in facial skin-induced lesion regeneration for scleroderma patients. Stem Cell Res. Ther. 2017, 8, 236. [Google Scholar] [CrossRef]
- Maria, A.T. Human adipose mesenchymal stem cells as potent anti-fibrosis therapy for systemic sclerosis. J. Autoimmun. 2016, 70, 31–39. [Google Scholar] [CrossRef]
- Serratrice, N.; Bruzzese, L.; Magalon, J.; Véran, J.; Giraudo, L.; Aboudou, H.; Ould-Ali, D.; Nguyen, P.S.; Bausset, O.; Daumas, A.; et al. New fat-derived products for treating skin-induced lesions of scleroderma in nude mice. Stem Cell Res. Ther. 2014, 5, 138. [Google Scholar] [CrossRef]
- Usunier, B.; Benderitter, M.; Tamarat, R.; Chapel, A. Management of fibrosis: The mesenchymal stromal cells breakthrough. Stem Cells Int. 2014, 2014, 340257. [Google Scholar] [CrossRef]
- Sun, W.; Ni, X.; Sun, S.; Cai, L.; Yu, J.; Wang, J.; Nie, B.; Sun, Z.; Ni, X.; Cao, X. Adipose-Derived Stem Cells Alleviate Radiation-Induced Muscular Fibrosis by Suppressing the Expression of TGF-beta1. Stem Cells Int. 2016, 2016, 5638204. [Google Scholar] [CrossRef]
- Hiwatashi, N.; Bing, R.; Kraja, I.; Branski, R.C. Mesenchymal stem cells have antifibrotic effects on trans- forming growth factor-β1-stimulated vocal fold fibroblasts. Laryngoscope 2017, 127, E35–E41. [Google Scholar] [CrossRef]
- Mahmoud, M.; Abdel-Rasheed, M.; Galal, E.R.; El-Awady, R.R. Factors Defining Human Adipose Stem/Stromal Cell Immunomodulation in Vitro. Stem Cell Rev. Rep. 2023, 20, 175–205. [Google Scholar] [CrossRef]
- Panina, Y.A.; Yakimov, A.S.; Komleva, Y.K.; Morgun, A.V.; Lopatina, O.L.; Malinovskaya, N.A.; Shuvaev, A.N.; Salmin, V.V.; Taranushenko, T.E.; Salmina, A.B. Plasticity of Adipose Tissue-Derived Stem Cells and Regulation of Angiogenesis. Front. Physiol. 2018, 9, 1656. [Google Scholar] [CrossRef]
- Nguyen, P.S.; Desouches, C.; Gay, A.M.; Hautier, A.; Magalon, G. Development of micro-injection as an innovative autologous fat graft technique: The use of adipose tissue as dermal filler. J. Plast. Reconstr. Aesthetic Surg. 2012, 65, 1692–1699. [Google Scholar] [CrossRef]
- Gir, P.; Brown, S.A.; Oni, G.; Kashefi, N.; Mojallal, A.; Rohrich, R.J. Fat grafting: Evidence-based review on autologous fat harvesting, processing, reinjection, and storage. Plast. Reconstr. Surg. 2012, 130, 249–258. [Google Scholar] [CrossRef]
- Kølle, S.-F.T.; Duscher, D.; Taudorf, M.; Fischer-Nielsen, A.; Svalgaard, J.D.; Munthe-Fog, L.; Jønsson, B.; Selvig, P.B.; Mamsen, F.P.; Katz, A.J. Ex vivo-expanded autologous adipose tissue-derived stromal cells ensure enhanced fat graft retention in breast augmentation: A randomized controlled clinical trial. Stem Cells Transl. Med. 2020, 9, 1277–1286. [Google Scholar] [CrossRef]
- Waldner, M.; Zhang, W.; James, I.B.; Allbright, K.; Havis, E.; Bliley, J.M.; Almadori, A.; Schweizer, R.; Plock, J.A.; Washington, K.M.; et al. Characteristics and Immunomodulating Functions of Adipose-Derived and Bone Marrow-Derived Mesenchymal Stem Cells Across Defined Human Leukocyte Antigen Barriers. Front. Immunol. 2018, 9, 1642. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Etiology | Type of ASCs-BT | Proposed Effect | References |
|---|---|---|---|---|
| Hypertrophic scar | Trauma; Iatrogenic | Macro-fat; Emulsified fat/m-SVF; Macro-fat mixed with PRP; Emulsified fat/m-SVF combined with CO2 laser | ECM remodeling | [40,41,42,43,44,45] |
| Burns | Trauma | Macro-fat; Emulsified fat/m-SVF; e-SVF | ECM remodeling; Neo-angiogenesis | [48,49,50,51,52,53,54,55,56,57,58,59,60,61] |
| Radiation-induced fibrosis | Iatrogenic | Macro-fat | ECM remodeling; Neo-angiogenesis; Immunomodulation; Mechanical effect: increase in thickness of subcutaneous tissue | [63,64,65,66,67,68,69,70,71,72,73,74,75,76] |
| Dupuytren’s disease | Unknown (?genetic) | Macro-fat; ASCs | Myofibroblast proliferation inhibition; α-smooth muscle actin protein expression reduction; Angiogenesis; Immunomodulation | [82,83] |
| Lichen sclerosus | Unknown (?genetic) | Macro-fat; Emulsified fat/m-SVF; Fat mixed with PRP; ASCs | ECM remodeling; Immunomodulation | [85,86,87,88,89,90,91,92] |
| Scleroderma | Autoimmune | Macro-fat; Micro-fat; Emulsified fat/m-SVF; ASCs; ASCs mixed with PRP; Micro-fat mixed with m-SVF; Micro-fat mixed with PRP; Emulsified fat/m-SVF mixed with PRP | ECM remodeling; Neo-angiogenesis; Immunomodulation | [95,96,97,98,99,100,101,102,103,104] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almadori, A.; Butler, P.E. Scarring and Skin Fibrosis Reversal with Regenerative Surgery and Stem Cell Therapy. Cells 2024, 13, 443. https://doi.org/10.3390/cells13050443
Almadori A, Butler PE. Scarring and Skin Fibrosis Reversal with Regenerative Surgery and Stem Cell Therapy. Cells. 2024; 13(5):443. https://doi.org/10.3390/cells13050443
Chicago/Turabian StyleAlmadori, Aurora, and Peter EM Butler. 2024. "Scarring and Skin Fibrosis Reversal with Regenerative Surgery and Stem Cell Therapy" Cells 13, no. 5: 443. https://doi.org/10.3390/cells13050443
APA StyleAlmadori, A., & Butler, P. E. (2024). Scarring and Skin Fibrosis Reversal with Regenerative Surgery and Stem Cell Therapy. Cells, 13(5), 443. https://doi.org/10.3390/cells13050443