Children and Adults with Refractory Acute Graft-versus-Host Disease Respond to Treatment with the Mesenchymal Stromal Cell Preparation “MSC-FFM”—Outcome Report of 92 Patients

 ,
,  , ,
, ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Mesenchymal Stromal Cells-Frankfurt on Main (MSC-FFM)
2.2. Data Collection and Analysis
2.3. Definitions, Stratifications and Statistical Analysis
3. Results
3.1. Patients
3.2. MSC-FFM Treatment and Tolerability
3.3. aGvHD Outcomes
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Martin, P.J.; Rizzo, J.D.; Wingard, J.R.; Ballen, K.; Curtin, P.T.; Cutler, C.; Litzow, M.R.; Nieto, Y.; Savani, B.N.; Schriber, J.R.; et al. First- and second-line systemic treatment of acute graft-versus-host disease: Recommendations of the American Society of Blood and Marrow Transplantation. Biol. Blood Marrow Transplant. 2012, 18, 1150–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Cadenas, I.; Rivera, I.; Martino, R.; Esquirol, A.; Barba, P.; Novelli, S.; Orti, G.; Briones, J.; Brunet, S.; Valcarcel, D.; et al. Patterns of infection and infection-related mortality in patients with steroid-refractory acute graft versus host disease. Bone Marrow Transplant. 2017, 52, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Le Blanc, K.; Rasmusson, I.; Sundberg, B.; Götherström, C.; Hassan, M.; Uzunel, M.; Ringdén, O. Treatment of severe acute graft-versus-host disease with third party haploidentical mesenchymal stem cells. Lancet 2004, 363, 1439–1441. [Google Scholar] [CrossRef]
- Hashmi, S.; Ahmed, M.; Murad, M.H.; Litzow, M.R.; Adams, R.H.; Ball, L.M.; Prasad, V.K.; Kebriaei, P.; Ringden, O. Survival after mesenchymal stromal cell therapy in steroid-refractory acute graft-versus-host disease: Systematic review and meta-analysis. Lancet Haematol. 2016, 3, e45–e52. [Google Scholar] [CrossRef]
- Introna, M.; Lucchini, G.; Dander, E.; Galimberti, S.; Rovelli, A.; Balduzzi, A.; Longoni, D.; Pavan, F.; Masciocchi, F.; Algarotti, A.; et al. Treatment of graft versus host disease with mesenchymal stromal cells: A phase I study on 40 adult and pediatric patients. Biol. Blood Marrow Transplant. 2014, 20, 375–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Blanc, K.; Frassoni, F.; Ball, L.; Locatelli, F.; Roelofs, H.; Lewis, I.; Lanino, E.; Sundberg, B.; Bernardo, M.E.; Remberger, M.; et al. Mesenchymal stem cells for treatment of steroid-resistant, severe, acute graft-versus-host disease: A phase II study. Lancet 2008, 371, 1579–1586. [Google Scholar] [CrossRef]
- Lucchini, G.; Introna, M.; Dander, E.; Rovelli, A.; Balduzzi, A.; Bonanomi, S.; Salvadè, A.; Capelli, C.; Belotti, D.; Gaipa, G.; et al. Platelet-lysate-expanded mesenchymal stromal cells as a salvage therapy for severe resistant graft-versus-host disease in a pediatric population. Biol. Blood Marrow Transplant. 2010, 16, 1293–1301. [Google Scholar] [CrossRef] [Green Version]
- Prasad, V.K.; Lucas, K.G.; Kleiner, G.I.; Talano, J.A.M.; Jacobsohn, D.; Broadwater, G.; Monroy, R.; Kurtzberg, J. Efficacy and safety of ex vivo cultured adult human mesenchymal stem cells (Prochymal) in pediatric patients with severe refractory acute graft-versus-host disease in a compassionate use study. Biol. Blood Marrow Transplant. 2011, 17, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Resnick, I.B.; Barkats, C.; Shapira, M.Y.; Stepensky, P.; Bloom, A.I.; Shimoni, A.; Mankuta, D.; Varda-Bloom, N.; Rheingold, L.; Yeshurun, M.; et al. Treatment of severe steroid resistant acute GVHD with mesenchymal stromal cells (MSC). Am. J. Blood Res. 2013, 3, 225–238. [Google Scholar]
- Ringden, O.; Uzunel, M.; Rasmusson, I.; Remberger, M.; Sundberg, B.; Lönnies, H.; Marschall, H.U.; Dlugosz, A.; Szakos, A.; Hassan, Z.; et al. Mesenchymal stem cells for treatment of therapy-resistant graft-versus-host disease. Transplantation 2006, 81, 1390–1397. [Google Scholar] [CrossRef]
- Australian Public Assessment Report for Remestemcel-L, Ex Vivo Adult Human Mesenchymal Stem Cells. 2019. Available online: https://www.tga.gov.au/sites/default/files/auspar-remestemcel-l-150315.pdf (accessed on 14 October 2019).
- Dotoli, G.M.; De Santis, G.C.; Orellana, M.D.; de Lima Prata, K.; Caruso, S.R.; Fernandes, T.R.; Rensi Colturato, V.A.; Kondo, A.T.; Hamerschlak, N.; Simões, B.P.; et al. Mesenchymal stromal cell infusion to treat steroid-refractory acute GvHD III/IV after hematopoietic stem cell transplantation. Bone Marrow Transplant. 2017, 52, 859–862. [Google Scholar] [CrossRef] [PubMed]
- Salmenniemi, U.; Itala-Remes, M.; Nystedt, J.; Putkonen, M.; Niittyvuopio, R.; Vettenranta, K.; Korhonen, M. Good responses but high TRM in adult patients after MSC therapy for GvHD. Bone Marrow Transplant. 2017, 52, 606–608. [Google Scholar] [CrossRef] [PubMed]
- Te Boome, L.C.; Mansilla, C.; van der Wagen, L.E.; Lindemans, C.A.; Petersen, E.J.; Spierings, E.; Thus, K.A.; Westinga, K.; Plantinga, M.; Bierings, M.; et al. Biomarker profiling of steroid-resistant acute GVHD in patients after infusion of mesenchymal stromal cells. Leukemia 2015, 29, 1839–1846. [Google Scholar] [CrossRef] [PubMed]
- Von Dalowski, F.; Kramer, M.; Wermke, M.; Wehner, R.; Röllig, C.; Alakel, N.; Stölzel, F.; Parmentier, S.; Sockel, K.; Krech, M.; et al. Mesenchymal Stromal Cells for Treatment of Acute Steroid-Refractory Graft Versus Host Disease: Clinical Responses and Long-Term Outcome. Stem Cells 2016, 34, 357–366. [Google Scholar] [CrossRef] [Green Version]
- Elgaz, S.; Kuçi, Z.; Kuçi, S.; Bönig, H.; Bader, P. Clinical Use of Mesenchymal Stromal Cells in the Treatment of Acute Graft-versus-Host Disease. Transfus Med. Hemother. 2019, 46, 27–34. [Google Scholar] [CrossRef]
- Moll, G.; Jitschin, R.; von Bahr, L.; Rasmusson-Duprez, I.; Sundberg, B.; Lönnies, L.; Elgue, G.; Nilsson-Ekdahl, K.; Mougiakakos, D.; Lambris, J.D.; et al. Mesenchymal stromal cells engage complement and complement receptor bearing innate effector cells to modulate immune responses. PLoS. ONE 2011, 6, e21703. [Google Scholar] [CrossRef]
- Phinney, D.G.; Kopen, G.; Righter, W.; Webster, S.; Tremain, N.; Prockop, D.J. Donor variation in the growth properties and osteogenic potential of human marrow stromal cells. J. Cell Biochem. 1999, 75, 424–436. [Google Scholar] [CrossRef]
- Von Bahr, L.; Sundberg, B.; Lonnies, L.; Sander, B.; Karbach, H.; Hägglund, H.; Ljungman, P.; Gustafsson, B.; Karlsson, H.; Le Blanc, K.; et al. Long-term complications, immunologic effects, and role of passage for outcome in mesenchymal stromal cell therapy. Biol. Blood Marrow Transplant. 2012, 18, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Trento, C.; Bernardo, M.E.; Nagler, A.; Kuçi, S.; Bornhäuser, M.; Köhl, U.; Strunk, D.; Galleu, A.; Sanchez-Guijo, F.; Gaipa, G.; et al. Manufacturing Mesenchymal Stromal Cells for the Treatment of Graft-versus-Host Disease: A Survey among Centers Affiliated with the European Society for Blood and Marrow Transplantation. Biol. Blood Marrow Transplant. 2018, 24, 2365–2370. [Google Scholar] [CrossRef] [Green Version]
- Kuci, Z.; Bonig, H.; Kreyenberg, H.; Bunos, M.; Jauch, A.; Janssen, J.W.G.; Škifić, M.; Michel, K.; Eising, B.; Lucchini, G.; et al. Mesenchymal stromal cells from pooled mononuclear cells of multiple bone marrow donors as rescue therapy in pediatric severe steroid-refractory graft-versus-host disease: A multicenter survey. Haematologica 2016, 101, 985–994. [Google Scholar] [CrossRef]
- Von Bonin, M.; Stolzel, F.; Goedecke, A.; Richter, K.; Wuschek, N.; Hölig, K.; Platzbecker, U.; Illmer, T.; Schaich, M.; Schetelig, J.; et al. Treatment of refractory acute GVHD with third-party MSC expanded in platelet lysate-containing medium. Bone Marrow Transplant. 2009, 43, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar] [PubMed]
- Schallmoser, K.; Bartmann, C.; Rohde, E.; Reinisch, A.; Kashofer, K.; Stadelmeyer, E.; Drexler, C.; Lanzer, G.; Linkesch, W.; Strunk, D. Human platelet lysate can replace fetal bovine serum for clinical-scale expansion of functional mesenchymal stromal cells. Transfusion 2007, 47, 1436–1446. [Google Scholar] [CrossRef]
- Eichler, H.; Schrezenmeier, H.; Schallmoser, K.; Strunk, D.; Nystedt, J.; Kaartinen, T.; Korhonen, M.; Fleury-Cappellesso, S.; Sensebé, L.; Bönig, H.; et al. Donor selection and release criteria of cellular therapy products. Vox Sang. 2013, 104, 67–91. [Google Scholar] [CrossRef] [PubMed]
- Prentice, R.L.; Kalbfleisch, J.D.; Peterson, A.V.; Flournoy, N.; Farewell, V.T.; Breslow, N.E. The analysis of failure times in the presence of competing risks. Biometrics 1978, 34, 541–554. [Google Scholar] [CrossRef] [PubMed]
- Bader, P.; Kuci, Z.; Bakhtiar, S.; Basu, O.; Bug, G.; Dennis, M.; Greil, J.; Barta, A.; Kállay, K.M.; Lang, P.; et al. Effective treatment of steroid and therapy-refractory acute graft-versus-host disease with a novel mesenchymal stromal cell product (MSC-FFM). Bone Marrow Transplant. 2018, 53, 852–862. [Google Scholar] [CrossRef] [PubMed]
- Glucksberg, H.; Storb, R.; Fefer, A.; Buckner, C.D.; Neiman, P.E.; Clift, R.A.; Lerner, K.G.; Thomas, E.D. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation 1974, 18, 295–304. [Google Scholar] [CrossRef]
- Van Lint, M.T.; Uderzo, C.; Locasciulli, A.; Majolino, I.; Scimé, R.; Locatelli, F.; Giorgiani, G.; Arcese, W.; Iori, A.P.; Falda, M.; et al. Early treatment of acute graft-versus-host disease with high- or low-dose 6-methylprednisolone: A multicenter randomized trial from the Italian Group for Bone Marrow Transplantation. Blood 1998, 92, 2288–2293. [Google Scholar]
- R Core Team. R: A language and Environment for Statistical Computing. R Foundation for Statistical Computing, 2019. Available online: http://www.R-project.org/ (accessed on 14 October 2019).
- Koreth, J.; Antin, J.H. Current and future approaches for control of graft-versus-host disease. Expert Rev. Hematol. 2008, 1, 111. [Google Scholar] [CrossRef] [Green Version]
- Romieu-Mourez, R.; Francois, M.; Boivin, M.N.; Stagg, J.; Galipeau, J. Regulation of MHC class II expression and antigen processing in murine and human mesenchymal stromal cells by IFN-gamma, TGF-beta, and cell density. J. Immunol. 2007, 179, 1549–1558. [Google Scholar] [CrossRef] [Green Version]
- Dumler, J.S.; Beschorner, W.E.; Farmer, E.R.; Di Gennaro, K.A.; Saral, R.; Santos, G.W. Endothelial-cell injury in cutaneous acute graft-versus-host disease. Am. J. Pathol. 1989, 135, 1097–1103. [Google Scholar] [PubMed]
- Luft, T.; Dietrich, S.; Falk, C.; Conzelmann, M.; Hess, M.; Benner, A.; Neumann, F.; Isermann, B.; Hegenbart, U.; Ho, A.D.; et al. Steroid-refractory GVHD: T-cell attack within a vulnerable endothelial system. Blood 2011, 118, 1685–1692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeisbrich, M.; Becker, N.; Benner, A.; Radujkovic, A.; Schmitt, K.; Beimler, J.; Ho, A.D.; Zeier, M.; Dreger, P.; Luft, T. Transplant-associated thrombotic microangiopathy is an endothelial complication associated with refractoriness of acute GvHD. Bone Marrow Transplant. 2017, 52, 1399–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kale, V.P. Application of “Primed” Mesenchymal Stromal Cells in Hematopoietic Stem Cell Transplantation: Current Status and Future Prospects. Stem Cells Dev. 2019. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (Total = 92) | % | |
|---|---|---|
| Sex (f/m) | 31/61 | 34/66 |
| Diagnosis (malignant/non-malignant) | 69/23 | 75/25 |
| Age | ||
| ≤18 [Median (range)], years | 61 [7.7 (0.5–18.0)] | 66 |
| >18 [Median (range)], years | 31 [42.4 (18.4–65.6)] | 34 |
| Donor | ||
| Matched sibling donor | 21 | 23 |
| Matched unrelated donor | 56 | 61 |
| Mismatched unrelated donor | 1 | 1 |
| Haploidentical | 14 | 15 |
| Transplant source | ||
| Bone marrow | 41 | 45 |
| Peripheral blood stem cells | 49 | 53 |
| Umbilical cord blood | 2 | 2 |
| Conditioning | ||
| Total body irradiation based | 22 | 24 |
| Treosulfan based | 26 | 28 |
| Busulfan based | 21 | 23 |
| Fludarabine based | 21 | 23 |
| Others | 2 | 2 |
| Serotherapy | ||
| None | 29 | 32 |
| Anti-Thymocyte globulin (ATG) | 42 | 46 |
| Campath | 17 | 17 |
| Others | 4 | 4 |
| GvHD prophylaxis | ||
| None | 10 | 11 |
| Cyclosporin A (CSA) | 12 | 13 |
| CSA+methotrexate | 32 | 35 |
| CSA+mycophenolate mofetil (MMF) | 13 | 14 |
| Sirolimus+Tacrolimus | 5 | 5 |
| MMF+Tacrolimus | 5 | 5 |
| Others | 15 | 16 |
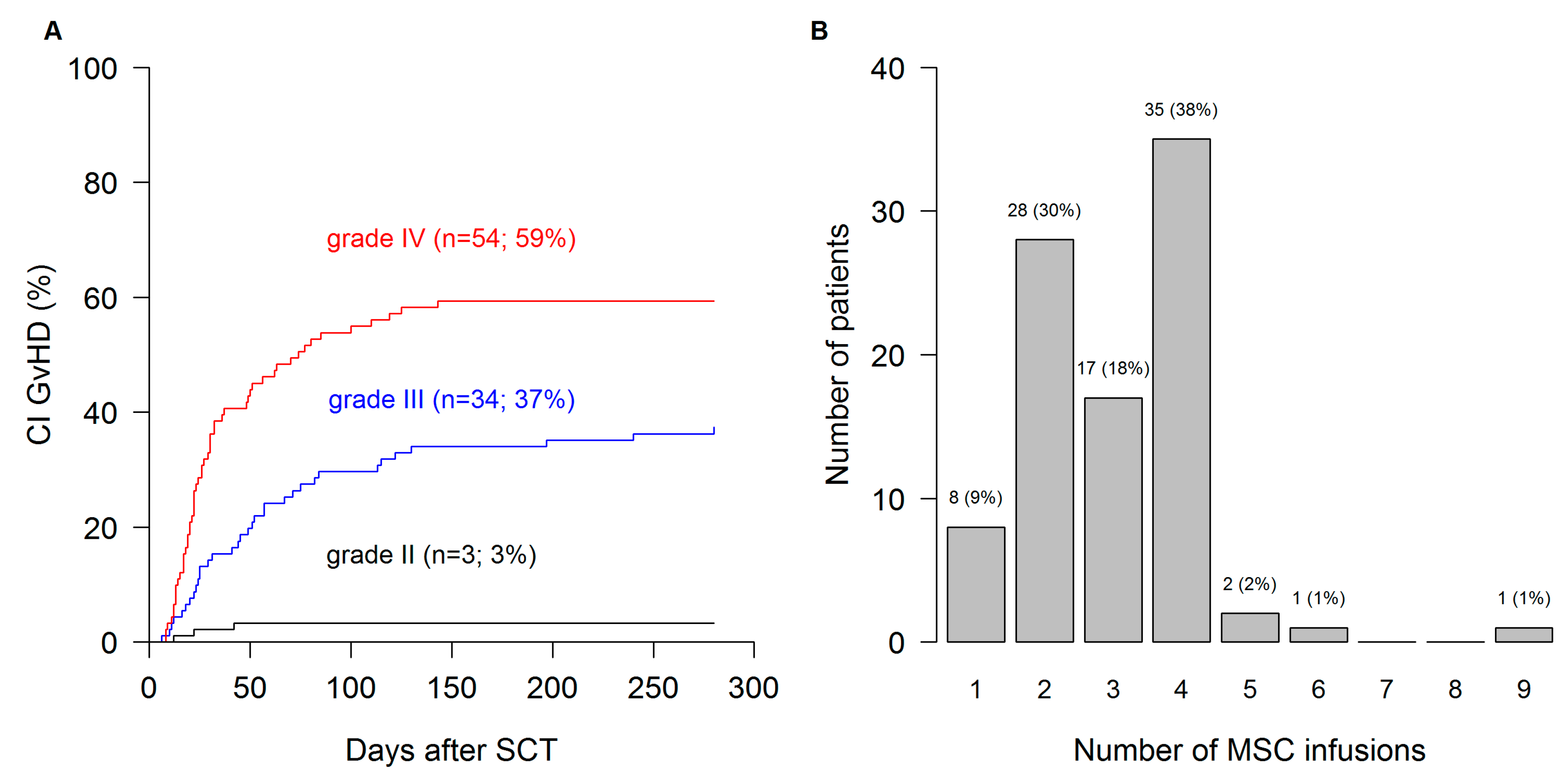
| aGvHD severity prior to MSC | ||
| grade II | 3 | 3 |
| grade III | 34 | 37 |
| grade IV | 54 | 59 |
| Not specified | 1 | 1 |
| # aGvHD therapies prior to 1st MSC dose | ||
| 1 | 8 | 9 |
| 2 | 17 | 18 |
| 3 | 31 | 34 |
| 4 | 16 | 17 |
| 5 | 12 | 13 |
| 6 | 4 | 4 |
| ≥7 | 4 | 4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonig, H.; Kuçi, Z.; Kuçi, S.; Bakhtiar, S.; Basu, O.; Bug, G.; Dennis, M.; Greil, J.; Barta, A.; Kállay, K.M.; et al. Children and Adults with Refractory Acute Graft-versus-Host Disease Respond to Treatment with the Mesenchymal Stromal Cell Preparation “MSC-FFM”—Outcome Report of 92 Patients. Cells 2019, 8, 1577. https://doi.org/10.3390/cells8121577
Bonig H, Kuçi Z, Kuçi S, Bakhtiar S, Basu O, Bug G, Dennis M, Greil J, Barta A, Kállay KM, et al. Children and Adults with Refractory Acute Graft-versus-Host Disease Respond to Treatment with the Mesenchymal Stromal Cell Preparation “MSC-FFM”—Outcome Report of 92 Patients. Cells. 2019; 8(12):1577. https://doi.org/10.3390/cells8121577
Chicago/Turabian StyleBonig, Halvard, Zyrafete Kuçi, Selim Kuçi, Shahrzad Bakhtiar, Oliver Basu, Gesine Bug, Mike Dennis, Johann Greil, Aniko Barta, Krisztián M. Kállay, and et al. 2019. "Children and Adults with Refractory Acute Graft-versus-Host Disease Respond to Treatment with the Mesenchymal Stromal Cell Preparation “MSC-FFM”—Outcome Report of 92 Patients" Cells 8, no. 12: 1577. https://doi.org/10.3390/cells8121577
APA StyleBonig, H., Kuçi, Z., Kuçi, S., Bakhtiar, S., Basu, O., Bug, G., Dennis, M., Greil, J., Barta, A., Kállay, K. M., Lang, P., Lucchini, G., Pol, R., Schulz, A., Sykora, K. -W., Teichert von Luettichau, I., Herter-Sprie, G., Ashab Uddin, M., Jenkin, P., ... Bader, P. (2019). Children and Adults with Refractory Acute Graft-versus-Host Disease Respond to Treatment with the Mesenchymal Stromal Cell Preparation “MSC-FFM”—Outcome Report of 92 Patients. Cells, 8(12), 1577. https://doi.org/10.3390/cells8121577