Prognostic Significance of TWIST1, CD24, CD44, and ALDH1 Transcript Quantification in EpCAM-Positive Circulating Tumor Cells from Early Stage Breast Cancer Patients




Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Lines
2.2. Patients
2.3. Isolation of EpCAM+ CTCs
2.4. RNA Extraction-cDNA Synthesis
2.5. RT-qPCR
2.6. Statistical Analysis
3. Results
3.1. Analytical Validation of the Quadraplex RT-qPCR Assay for CD24, CD44, ALDH1, HPRT
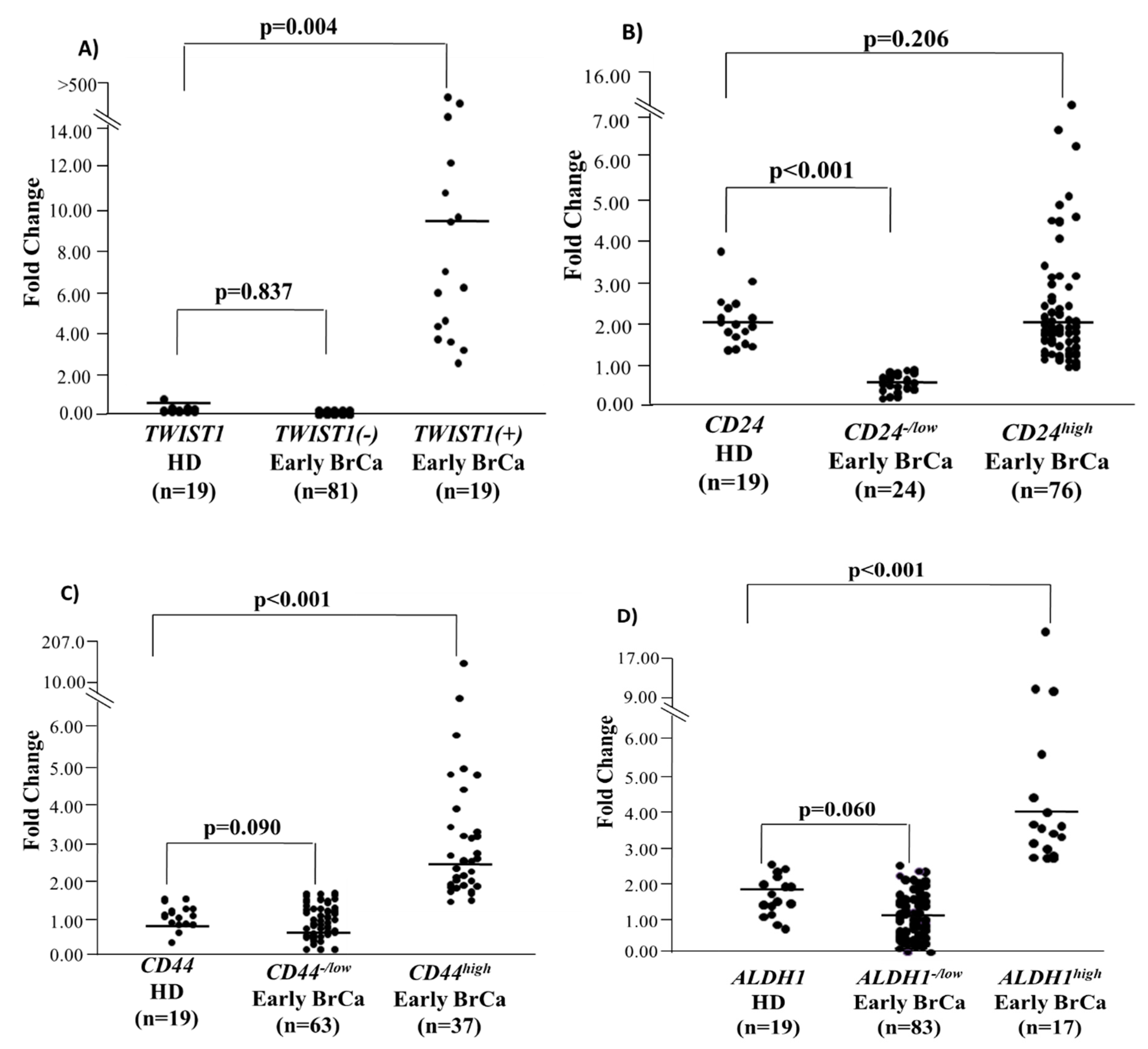
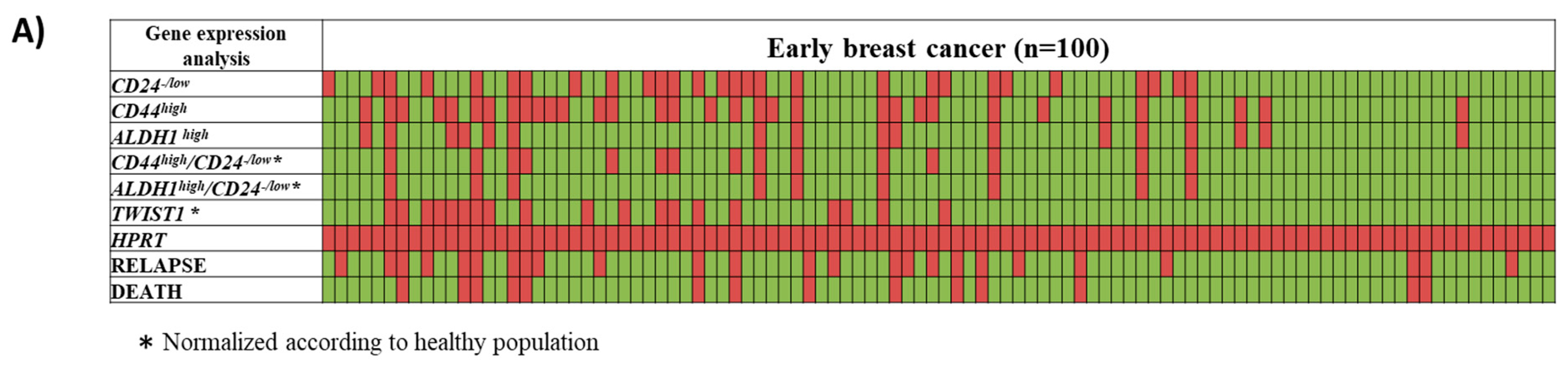
3.2. Quantification of CD24, CD44, ALDH1, and TWIST1 mRNA in the EpCAM(+) Fraction in Early Stage BrCa Patients and (HD)
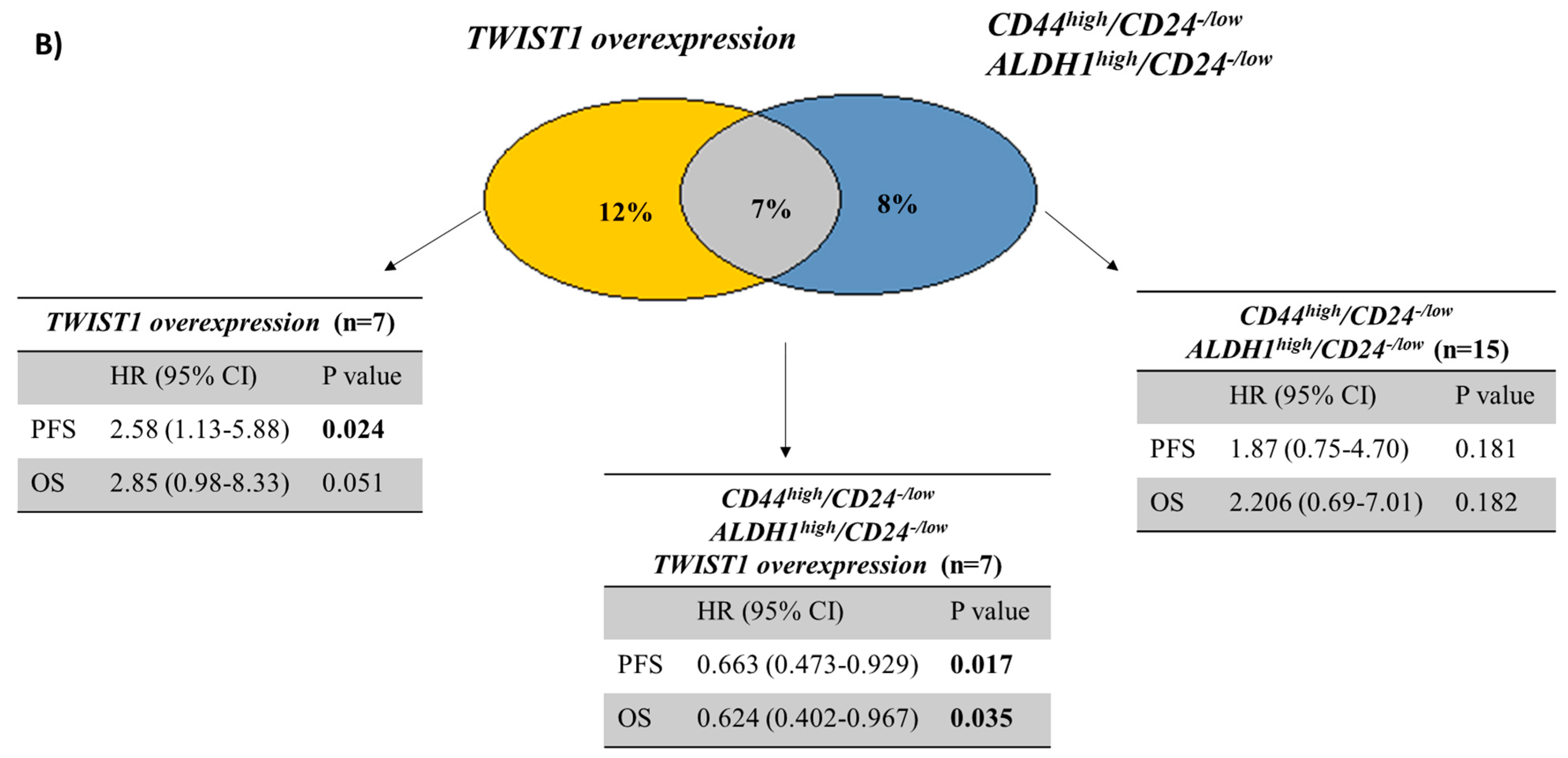
3.3. Evaluation of Prognostic Significance
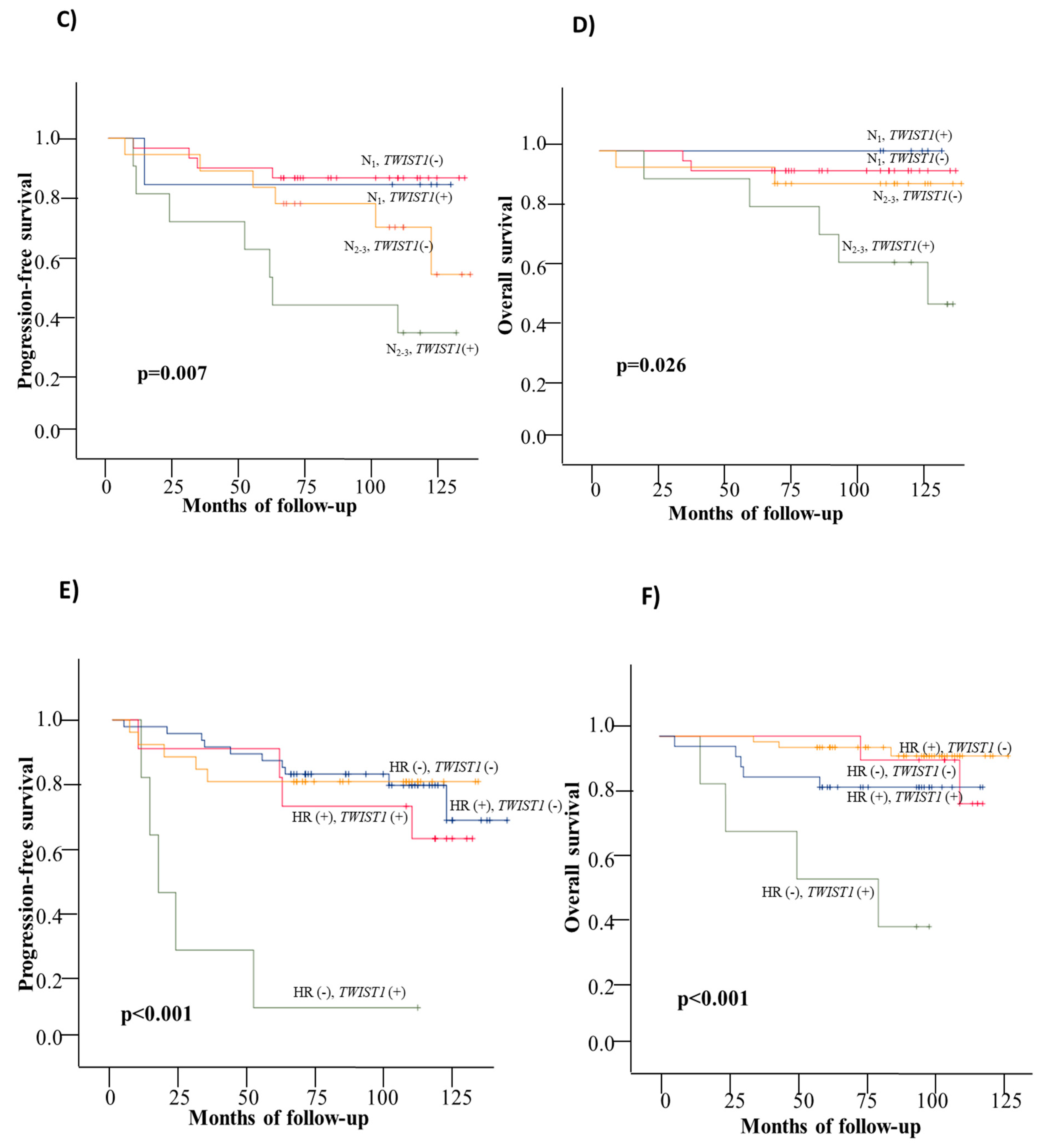
3.3.1. Disease Free Interval
3.3.2. Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| EMT | epithelial–mesenchymal transition |
| MET | mesenchymal-epithelial transition |
| MICs | metastasis-initiating cells |
| SC | Stem Cell |
| HR | Hormone Receptor |
| BCSC | breast cancer stem cells |
| CSCs | Cancer stem cells |
| CTCs | Circulating tumor cells |
| ER | estrogen receptor |
| PR | progesterone receptor |
| HER2 | human epidermal growth factor receptor 2 |
| ALDH1 | aldehyde dehydrogenase 1 |
| HD | Healthy Donors |
| RT-qPCR | Quantitative Reverse Transcription Polymerase Chain Reaction |
| PBMCs | peripheral blood mononuclear cells |
| PBS | phosphate-buffered saline |
| LN | lymph nodes |
References
- Lianidou, E.S. Gene expression profiling and DNA methylation analyses of CTCs. Mol. Oncol. 2016, 10, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Bardelli, A.; Pantel, K. Liquid Biopsies, What We Do Not Know (Yet). Cancer Cell 2017, 31, 172–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boral, D.; Vishnoi, M.; Liu, H.N.; Yin, W.; Sprouse, M.L.; Scamardo, A.; Hong, D.S.; Tan, T.Z.; Thiery, J.P.; Chang, J.C.; et al. Molecular characterization of breast cancer CTCs associated with brain metastasis. Nat. Commun. 2017, 8, 196. [Google Scholar] [CrossRef] [PubMed]
- Jakabova, A.; Bielcikova, Z.; Pospisilova, E.; Matkowski, R.; Szynglarewicz, B.; Staszek-Szewczyk, U.; Zemanova, M.; Petruzelka, L.; Eliasova, P.; Kolostova, K.; et al. Molecular characterization and heterogeneity of circulating tumor cells in breast cancer. Breast Cancer Res. Treat. 2017, 166, 695–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansoori, M.; Madjd, Z.; Janani, L.; Rasti, A. Circulating cancer stem cell markers in breast carcinomas: A systematic review protocol. Syst. Rev. 2017, 6, 262. [Google Scholar] [CrossRef] [PubMed]
- Reya, T.; Morrison, S.J.; Clarke, M.F.; Weissman, I.L. Stem cells, cancer, and cancer stem cells. Nature 2001, 414, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Luo, M.; Clouthier, S.G.; Deol, Y.; Liu, S.; Nagrath, S.; Azizi, E.; Wicha, M.S. Breast cancer stem cells: Current advances and clinical implications. Methods Mol. Biol. 2015, 1293, 1–49. [Google Scholar]
- Al-Hajj, M.; Wicha, M.S.; Benito-Hernandez, A.; Morrison, S.J.; Clarke, M.F. Prospective identification of tumorigenic breast cancer cells. Proc. Natl. Acad. Sci. USA 2003, 100, 3983–3988. [Google Scholar] [CrossRef] [Green Version]
- Ginestier, C.; Hur, M.H.; Charafe-Jauffret, E.; Monville, F.; Dutcher, J.; Brown, M.; Jacquemier, J.; Viens, P.; Kleer, C.G.; Liu, S.; et al. ALDH1 is a marker of normal and malignant human mammary stem cells and a predictor of poor clinical outcome. Cell Stem Cell 2007, 1, 555–567. [Google Scholar] [CrossRef]
- Balic, M.; Lin, H.; Young, L.; Hawes, D.; Giuliano, A.; McNamara, G.; Datar, R.H.; Cote, R.J. Most early disseminated cancer cells detected in bone marrow of breast cancer patients have a putative breast cancer stem cell phenotype. Clin. Cancer Res. 2006, 12, 5615–5621. [Google Scholar] [CrossRef]
- Theodoropoulos, P.A.; Polioudaki, H.; Agelaki, S.; Kallergi, G.; Saridaki, Z.; Mavroudis, D.; Georgoulias, V. Circulating tumor cells with a putative stem cell phenotype in peripheral blood of patients with breast cancer. Cancer Lett. 2010, 288, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Bredemeier, M.; Edimiris, P.; Tewes, M.; Mach, P.; Aktas, B.; Schellbach, D.; Wagner, J.; Kimmig, R.; Kasimir-Bauer, S. Establishment of a multimarker qPCR panel for the molecular characterization of circulating tumor cells in blood samples of metastatic breast cancer patients during the course of palliative treatment. Oncotarget 2016, 7, 41677–41690. [Google Scholar] [CrossRef] [PubMed]
- Baccelli, I.; Schneeweiss, A.; Riethdorf, S.; Stenzinger, A.; Schillert, A.; Vogel, V.; Klein, C.; Saini, M.; Bäuerle, T.; Wallwiener, M.; et al. Identification of a population of blood circulating tumor cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat. Biotechnol. 2013, 31, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Schölch, S.; García, S.A.; Iwata, N.; Niemietz, T.; Betzler, A.M.; Nanduri, L.K.; Bork, U.; Kahlert, C.; Thepkaysone, M.-L.; Swiersy, A.; et al. Circulating tumor cells exhibit stem cell characteristics in an orthotopic mouse model of colorectal cancer. Oncotarget 2016, 7, 27232–27242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Li, Y.; Xu, J.; Zhang, A.; Wang, X.; Tang, R.; Zhang, X.; Yin, H.; Liu, M.; Wang, D.D.; et al. Quantified postsurgical small cell size CTCs and EpCAM+ circulating tumor stem cells with cytogenetic abnormalities in hepatocellular carcinoma patients determine cancer relapse. Cancer Lett. 2018, 412, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Cong, Y.; Wang, D.; Sun, Y.; Deng, L.; Liu, Y.; Martin-Trevino, R.; Shang, L.; McDermott, S.P.; Landis, M.D.; et al. Breast cancer stem cells transition between epithelial and mesenchymal states reflective of their normal counterparts. Stem Cell Rep. 2014, 2, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Aktas, B.; Tewes, M.; Fehm, T.; Hauch, S.; Kimmig, R.; Kasimir-Bauer, S. Stem cell and epithelial-mesenchymal transition markers are frequently overexpressed in circulating tumor cells of metastatic breast cancer patients. Breast Cancer Res. 2009, 11, R46. [Google Scholar] [CrossRef]
- Giordano, A.; Gao, H.; Anfossi, S.; Cohen, E.; Mego, M.; Lee, B.-N.; Tin, S.; De Laurentiis, M.; Parker, C.A.; Alvarez, R.H.; et al. Epithelial-mesenchymal transition and stem cell markers in patients with HER2-positive metastatic breast cancer. Mol. Cancer 2012, 11, 2526–2534. [Google Scholar] [CrossRef]
- Mego, M.; Gao, H.; Lee, B.-N.; Cohen, E.N.; Tin, S.; Giordano, A.; Wu, Q.; Liu, P.; Nieto, Y.; Champlin, R.E.; et al. Prognostic Value of EMT-Circulating Tumor Cells in Metastatic Breast Cancer Patients Undergoing High-Dose Chemotherapy with Autologous Hematopoietic Stem Cell Transplantation. J. Cancer 2012, 3, 369–380. [Google Scholar] [CrossRef]
- Zhang, L.; Ridgway, L.D.; Wetzel, M.D.; Ngo, J.; Yin, W.; Kumar, D.; Goodman, J.C.; Groves, M.D.; Marchetti, D. The identification and characterization of breast cancer CTCs competent for brain metastasis. Sci. Transl. Med. 2013, 5, 180ra48. [Google Scholar] [CrossRef]
- Papadaki, M.A.; Kallergi, G.; Zafeiriou, Z.; Manouras, L.; Theodoropoulos, P.A.; Mavroudis, D.; Georgoulias, V.; Agelaki, S. Co-expression of putative stemness and epithelial-to-mesenchymal transition markers on single circulating tumour cells from patients with early and metastatic breast cancer. BMC Cancer 2014, 14, 651. [Google Scholar] [CrossRef] [PubMed]
- Ning, Y.; Zhang, W.; Hanna, D.L.; Yang, D.; Okazaki, S.; Berger, M.D.; Miyamoto, Y.; Suenaga, M.; Schirripa, M.; El-Khoueiry, A.; et al. Clinical relevance of EMT and stem-like gene expression in circulating tumor cells of metastatic colorectal cancer patients. Pharm. J. 2018, 18, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, M.A.; Stoupis, G.; Theodoropoulos, P.A.; Mavroudis, D.; Georgoulias, V.; Agelaki, S. Circulating Tumor Cells with Stemness and Epithelial-to-Mesenchymal Transition Features Are Chemoresistant and Predictive of Poor Outcome in Metastatic Breast Cancer. Mol. Cancer 2019, 18, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Stathopoulou, A.; Vlachonikolis, I.; Mavroudis, D.; Perraki, M.; Kouroussis, C.; Apostolaki, S.; Malamos, N.; Kakolyris, S.; Kotsakis, A.; Xenidis, N.; et al. Molecular Detection of Cytokeratin-19–Positive Cells in the Peripheral Blood of Patients With Operable Breast Cancer: Evaluation of Their Prognostic Significance. J. Clin. Oncol. 2002, 20, 3404–3412. [Google Scholar] [CrossRef] [PubMed]
- Xenidis, N.; Markos, V.; Apostolaki, S.; Perraki, M.; Pallis, A.; Sfakiotaki, G.; Papadatos-Pastos, D.; Kalmanti, L.; Kafousi, M.; Stathopoulos, E.; et al. Clinical relevance of circulating CK-19 mRNA-positive cells detected during the adjuvant tamoxifen treatment in patients with early breast cancer. Ann. Oncol. 2007, 18, 1623–1631. [Google Scholar] [CrossRef] [PubMed]
- Xenidis, N.; Ignatiadis, M.; Apostolaki, S.; Perraki, M.; Kalbakis, K.; Agelaki, S.; Stathopoulos, E.N.; Chlouverakis, G.; Lianidou, E.; Kakolyris, S.; et al. Cytokeratin-19 mRNA-Positive Circulating Tumor Cells After Adjuvant Chemotherapy in Patients With Early Breast Cancer. J. Clin. Oncol. 2009, 27, 2177–2184. [Google Scholar] [CrossRef]
- Xenidis, N.; Perraki, M.; Apostolaki, S.; Agelaki, S.; Kalbakis, K.; Vardakis, N.; Kalykaki, A.; Xyrafas, A.; Kakolyris, S.; Mavroudis, D.; et al. Differential effect of adjuvant taxane-based and taxane-free chemotherapy regimens on the CK-19 mRNA-positive circulating tumour cells in patients with early breast cancer. Br. J. Cancer 2013, 108, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Bidard, F.-C.; Michiels, S.; Riethdorf, S.; Mueller, V.; Esserman, L.J.; Lucci, A.; Naume, B.; Horiguchi, J.; Gisbert-Criado, R.; Sleijfer, S.; et al. Circulating Tumor Cells in Breast Cancer Patients Treated by Neoadjuvant Chemotherapy: A Meta-analysis. JNCI J. Natl. Cancer Inst. 2018, 110, 560–567. [Google Scholar] [CrossRef]
- Lucci, A.; Hall, C.S.; Lodhi, A.K.; Bhattacharyya, A.; Anderson, A.E.; Xiao, L.; Bedrosian, I.; Kuerer, H.M.; Krishnamurthy, S. Circulating tumour cells in non-metastatic breast cancer: A prospective study. Lancet Oncol. 2012, 13, 688–695. [Google Scholar] [CrossRef]
- Georgoulias, V.; Bozionelou, V.; Agelaki, S.; Perraki, M.; Apostolaki, S.; Kallergi, G.; Kalbakis, K.; Xyrafas, A.; Mavroudis, D. Trastuzumab decreases the incidence of clinical relapses in patients with early breast cancer presenting chemotherapy-resistant CK-19mRNA-positive circulating tumor cells: Results of a randomized phase II study. Ann. Oncol. 2012, 23, 1744–1750. [Google Scholar] [CrossRef]
- Ignatiadis, M.; Litière, S.; Rothe, F.; Riethdorf, S.; Proudhon, C.; Fehm, T.; Aalders, K.; Forstbauer, H.; Fasching, P.A.; Brain, E.; et al. Trastuzumab versus observation for HER2 nonamplified early breast cancer with circulating tumor cells (EORTC 90091-10093, BIG 1-12, Treat CTC): A randomized phase II trial. Ann. Oncol. 2018, 29, 1777–1783. [Google Scholar] [CrossRef] [PubMed]
- Schneble, E.J.; Graham, L.J.; Shupe, M.P.; Flynt, F.L.; Banks, K.P.; Kirkpatrick, A.D.; Nissan, A.; Henry, L.; Stojadinovic, A.; Shumway, N.M.; et al. Current approaches and challenges in early detection of breast cancer recurrence. J. Cancer 2014, 5, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Strati, A.; Markou, A.; Parisi, C.; Politaki, E.; Mavroudis, D.; Georgoulias, V.; Lianidou, E. Gene expression profile of circulating tumor cells in breast cancer by RT-qPCR. BMC Cancer 2011, 11, 422. [Google Scholar] [CrossRef] [PubMed]
- Mavroudis, D.; Saloustros, E.; Boukovinas, I.; Papakotoulas, P.; Kakolyris, S.; Ziras, N.; Christophylakis, C.; Kentepozidis, N.; Fountzilas, G.; Rigas, G.; et al. Sequential vs concurrent epirubicin and docetaxel as adjuvant chemotherapy for high-risk, node-negative, early breast cancer: An interim analysis of a randomised phase III study from the Hellenic Oncology Research Group. Br. J. Cancer 2017, 117, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Wittwer, C.T.; Herrmann, M.G.; Gundry, C.N.; Elenitoba-Johnson, K.S.J. Real-Time Multiplex PCR Assays. Methods 2001, 25, 430–442. [Google Scholar] [CrossRef]
- Stathopoulou, A.; Ntoulia, M.; Perraki, M.; Apostolaki, S.; Mavroudis, D.; Malamos, N.; Georgoulias, V.; Lianidou, E.S. A highly specific real-time RT-PCR method for the quantitative determination of CK-19 mRNA positive cells in peripheral blood of patients with operable breast cancer. Int. J. Cancer 2006, 119, 1654–1659. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of Relative Gene Expression Data Using Real-Time Quantitative PCR and the 2−ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Ignatiadis, M.; Xenidis, N.; Perraki, M.; Apostolaki, S.; Politaki, E.; Kafousi, M.; Stathopoulos, E.N.; Stathopoulou, A.; Lianidou, E.; Chlouverakis, G.; et al. Different prognostic value of cytokeratin-19 mRNA positive circulating tumor cells according to estrogen receptor and HER2 status in early-stage breast cancer. J. Clin. Oncol. 2007, 25, 5194–5202. [Google Scholar] [CrossRef]
- Aktas, B.; Müller, V.; Tewes, M.; Zeitz, J.; Kasimir-Bauer, S.; Loehberg, C.R.; Rack, B.; Schneeweiss, A.; Fehm, T. Comparison of estrogen and progesterone receptor status of circulating tumor cells and the primary tumor in metastatic breast cancer patients. Gynecol. Oncol. 2011, 122, 356–360. [Google Scholar] [CrossRef]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef]
- Trapp, E.; Janni, W.; Schindlbeck, C.; Jückstock, J.; Andergassen, U.; de Gregorio, A.; Alunni-Fabbroni, M.; Tzschaschel, M.; Polasik, A.; Koch, J.G.; et al. Presence of Circulating Tumor Cells in High-Risk Early Breast Cancer During Follow-Up and Prognosis. Jnci J. Natl. Cancer Inst. 2019, 111, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Mirza, S.; Jain, N.; Rawal, R. Evidence for circulating cancer stem-like cells and epithelial-mesenchymal transition phenotype in the pleurospheres derived from lung adenocarcinoma using liquid biopsy. Tumour Biol. 2017, 39, 1010428317695915. [Google Scholar] [CrossRef] [PubMed]
- Emprou, C.; Le Van Quyen, P.; Jégu, J.; Prim, N.; Weingertner, N.; Guérin, E.; Pencreach, E.; Legrain, M.; Voegeli, A.-C.; Leduc, C.; et al. SNAI2 and TWIST1 in lymph node progression in early stages of NSCLC patients. Cancer Med. 2018, 7, 3278–3291. [Google Scholar] [CrossRef] [PubMed]
- Markiewicz, A.; Wełnicka-Jaśkiewicz, M.; Seroczyńska, B.; Skokowski, J.; Majewska, H.; Szade, J.; Żaczek, A.J. Epithelial-mesenchymal transition markers in lymph node metastases and primary breast tumors - relation to dissemination and proliferation. Am. J. Transl. Res. 2014, 6, 793–808. [Google Scholar] [PubMed]
- Voutsadakis, I.A. Epithelial-Mesenchymal Transition (EMT) and Regulation of EMT Factors by Steroid Nuclear Receptors in Breast Cancer: A Review and in Silico Investigation. J. Clin. Med. 2016, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Vesuna, F.; Lisok, A.; Kimble, B.; Domek, J.; Kato, Y.; van der Groep, P.; Artemov, D.; Kowalski, J.; Carraway, H.; van Diest, P.; et al. Twist contributes to hormone resistance in breast cancer by downregulating estrogen receptor-α. Oncogene 2012, 31, 3223–3234. [Google Scholar] [CrossRef]
- Sarrió, D.; Rodriguez-Pinilla, S.M.; Hardisson, D.; Cano, A.; Moreno-Bueno, G.; Palacios, J. Epithelial-mesenchymal transition in breast cancer relates to the basal-like phenotype. Cancer Res. 2008, 68, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Lee, H.J.; Jang, M.H.; Gwak, J.M.; Lee, K.S.; Kim, E.J.; Kim, H.J.; Lee, H.E.; Park, S.Y. Epithelial-mesenchymal transition increases during the progression of in situ to invasive basal-like breast cancer. Hum. Pathol. 2013, 44, 2581–2589. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CD44high/CD24−/low | p a | ALDH1high/CD24−/low | p a | |||
|---|---|---|---|---|---|---|
| TWIST1 | Positive | Negative | 0.008 | Positive | Negative | 0.366 |
| Positive | 7 (46.7%) | 12(14.1%) | 3 (33.3) | 16(17.6%) | ||
| Negative | 8 (53.3%) | 73(85.9%) | 6 (66.7%) | 75 (82.4%) | ||
| Concordance | 80/100 (80%) | 78/100 (78%) | ||||
| Gene Expression in CTCs | DFI | OS | ||||||
|---|---|---|---|---|---|---|---|---|
| Gene | Mean Survival | 95% CI (months) | Range (months) | p | Mean Survival | 95% CI (Months) | Range (Months) | p |
| TWIST1+ | 83.6 | 61.9–105.3 | 9–125 | 0.019 | 106.4 | 90.3–122.3 | 16–127 | 0.046 |
| TWIST1− | 115 | 106.3–125.2 | 4–137 | 127.2 | 120.7–133.7 | 6–137 | ||
| Stem cell profile positive (SC+) | 86.7 | 66.7–106.8 | 16–118 | 0.174 | 107.3 | 89.8–124.8 | 26–127 | 0.171 |
| Stem cell profile negative (SC−) | 113.2 | 103.5–122.8 | 4–137 | 125.2 | 118.3–132.1 | 6–137 | ||
| TWIST1+/SC+ | 68.9 | 39.4–98.31 | 16–112 | 0.087 | 96.2 | 67.4–125.1 | 26–127 | 0.118 |
| TWIST1+/SC− | 88.8 | 61.2–116.4 | 9–125 | 111.1 | 93.3–128 | 16–125 | ||
| TWIST1−/SC+ | 100.1 | 78.6–121.7 | 41–118 | 109.1 | 92.8–125.3 | 47–118 | ||
| TWIST1−/SC− | 115.8 | 105.8–126 | 4–137 | 127.3 | 120.4–134.2 | 6–137 | ||
| TWIST1+/LN+ | 82.6 | 59.3–105.9 | 9–125 | 0.05 | 108.8 | 93–124.6 | 16–127 | 0.194 |
| TWIST1+/LN− | 88.7 | 30.5–146.8 | 16–125 | 92 | 39.1–144.8 | 26–125 | ||
| TWIST1−/LN+ | 110.3 | 99.2–121.4 | 6–130 | 121.3 | 113–129.6 | 6–130 | ||
| TWIST1−/LN− | 123.3 | 110.6–135.9 | 4–137 | 128.9 | 120.2–137.7 | 37–137 | ||
| TWIST1+/N2–3 | 68.6 | 40.5–96.7 | 9–125 | 0.007 | 98.3 | 75.5–121.2 | 16–127 | 0.026 |
| TWIST1+/N1 | 104.5 | 71.8–137.5 | 13–123 | 112 | 94–125 | 101–118 | ||
| TWIST1−/N2-3 | 103.1 | 84.1–121.9 | 6–130 | 118.8 | 103.4–134.1 | 6–130 | ||
| TWIST1−/N1 | 114.4 | 101.7–126.9 | 9–128 | 121.1 | 111.9–130.3 | 30–128 | ||
| TWIST1+/HR+ | 102.3 | 81.2–123.4 | 9–125 | <0.001 | 121.6 | 113.9–129.3 | 79–127 | <0.001 |
| TWIST1+/HR− | 36 | 8.9–63 | 10–106 | 65.7 | 36.7–94.6 | 76–106 | ||
| TWIST1−/HR+ | 117.9 | 107.1–128.7 | 4–137 | 131.9 | 126.2–137.5 | 37–137 | ||
| TWIST1−/HR− | 107.7 | 92.3–123.1 | 6–127 | 110.2 | 96.5–123.84 | 6–127 | ||
| Covariates | Covariate Value | DFI | OS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Cox Regression Analysis | Multivariate Cox Regression Analysis | Univariate Cox Regression Analysis | Multivariate Cox Regression Analysis | ||||||||||
| HR a | 95% CI b | p | HR a | 95% CI b | p | HRa | 95% CIb | p | HR a | 95% CI b | p | ||
| Age | ≥50 vs <50 | 0.787 | 0.357–1.734 | 0.552 | 0.432 | 0.169–1.103 | 0.079 | 0.718 | 0.249–2.070 | 0.539 | 0.593 | 0.169–2.080 | 0.414 |
| ER | Yes vs No | 0.647 | 0.286–1.463 | 0.295 | 4.391 | 1.040–18.549 | 0.044 | 0.238 | 0.079–0.721 | 0.011 | 0.623 | 0.092–4.215 | 0.628 |
| PR | Yes vs No | 0.492 | 0.217–1.114 | 0.089 | 0.087 | 0.021–0.362 | 0.001 | 0.196 | 0.054–0.707 | 0.013 | 0.098 | 0.011–0.851 | 0.035 |
| HER2 | Yes vs No | 0.500 | 0.197–1.269 | 0.145 | 0.626 | 0.232–1.693 | 0.357 | 0.381 | 0.106–1.366 | 0.139 | 0.247 | 0.060–1.023 | 0.054 |
| Lymph nodes | N0 vs N1 vs N2–3 | 2.207 | 1.261–3.861 | 0.006 | 2.433 | 1.272–4.654 | 0.007 | 1.659 | 0.817–3.371 | 0.162 | 1.351 | 0.637–2.862 | 0.433 |
| Size | ≥2cm vs <2cm | 3.060 | 1.049–8.922 | 0.041 | 4.926 | 1.225–19.811 | 0.025 | 7.244 | 0.947–55.432 | 0.056 | 17.450 | 1.464–208.1 | 0.024 |
| Grade | I/II vs III | 1.366 | 0.570–3.273 | 0.485 | 0.753 | 0.228–2.483 | 0.641 | 1.953 | 0.544–7.008 | 0.305 | 0.286 | 0.040–2.028 | 0.211 |
| TWIST1 | Yes vs No | 2.582 | 1.135–5.875 | 0.024 | 1.382 | 0.490–3.899 | 0.540 | 2.851 | 0.975–8.33 | 0.051 | 1.481 | 0.382–5.743 | 0.570 |
| HR and TWIST1 status | HR+TWIST1+ | 0.486 | 0.302–0.784 | 0.003 | 0.597 | 0.360–0.991 | 0.046 c | 0.576 | 0.313–1.062 | 0.077 | 0.666 | 0.345–1.284 | 0.225c |
| HR+TWIST1- | |||||||||||||
| HR-TWIST1+ | |||||||||||||
| HR-TWIST1- | |||||||||||||
| LN and TWIST1 status | N0-1TWIST1+ | 0.540 | 0.383–0.762 | <0.001 | 0.542 | 0.371–0.792 | 0.002 d | 0.559 | 0.357–0.875 | 0.011 | 0.604 | 0.373–0.976 | 0.040 d |
| N0-1TWIST1- | |||||||||||||
| N2-3TWIST1+ | |||||||||||||
| N2-3TWIST1- | |||||||||||||
| Stem cell profile | Yes vs No | 1.873 | 0.746–4.703 | 0.181 | 1.755 | 0.526–5.855 | 0.360 | 2.206 | 0.690–7.050 | 0.182 | 3.689 | 0.806–16.884 | 0.093 |
| Stem cell profile/TWIST1+ | Yes vs No | 0.663 | 0.473–0.929 | 0.017 | 0.776 | 0.521–1.146 | 0.202e | 0.624 | 0.402–0.967 | 0.035 | 0.634 | 0.378–1.065 | 0.085e |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strati, A.; Nikolaou, M.; Georgoulias, V.; Lianidou, E.S. Prognostic Significance of TWIST1, CD24, CD44, and ALDH1 Transcript Quantification in EpCAM-Positive Circulating Tumor Cells from Early Stage Breast Cancer Patients. Cells 2019, 8, 652. https://doi.org/10.3390/cells8070652
Strati A, Nikolaou M, Georgoulias V, Lianidou ES. Prognostic Significance of TWIST1, CD24, CD44, and ALDH1 Transcript Quantification in EpCAM-Positive Circulating Tumor Cells from Early Stage Breast Cancer Patients. Cells. 2019; 8(7):652. https://doi.org/10.3390/cells8070652
Chicago/Turabian StyleStrati, Areti, Michail Nikolaou, Vassilis Georgoulias, and Evi S. Lianidou. 2019. "Prognostic Significance of TWIST1, CD24, CD44, and ALDH1 Transcript Quantification in EpCAM-Positive Circulating Tumor Cells from Early Stage Breast Cancer Patients" Cells 8, no. 7: 652. https://doi.org/10.3390/cells8070652
APA StyleStrati, A., Nikolaou, M., Georgoulias, V., & Lianidou, E. S. (2019). Prognostic Significance of TWIST1, CD24, CD44, and ALDH1 Transcript Quantification in EpCAM-Positive Circulating Tumor Cells from Early Stage Breast Cancer Patients. Cells, 8(7), 652. https://doi.org/10.3390/cells8070652