Functional, Metabolic and Morphologic Results of Ex Vivo Donor Lung Perfusion with a Perfluorocarbon-Based Oxygen Carrier Nanoemulsion in a Large Animal Transplantation Model

 ,
,  , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Groups
- (1)
- EVLP Only Groups
- (i)
- PFCOC: Lungs were retrieved and stored for 24 h at 4 °C. PFCOC emulsion was added to the EVLP circuit (n = 7). EVLP time was 6 h.
- (ii)
- Control: Lungs were retrieved and stored for 24 h at 4 °C. EVLP was performed without PFCOC (n = 6). EVLP time was 6 h.
- (2)
- Transplantation Groups
- (i)
- Control: Lungs were retrieved and stored for 24 h at 4 °C. EVLP was performed without PFCOC. The left lung was transplanted after 6 h of EVLP. Observation of the transplanted lung was 4 h (n = 5).
- (ii)
- PFCOC: Lungs were retrieved and stored for 24 h at 4 °C. PFCOC emulsion was added to the EVLP. The left lung was transplanted after 6 h of EVLP. Observation of the transplanted lung was 4 h (n = 4).
- (iii)
- Immediate Transplantation (Im-Tx): Following 4 h of cold ischemic storage, the left lung was transplanted. Observation of the transplanted lung was 4 h (n = 3).
2.2. Lung Retrieval, EVLP, and Lung Transplantation Procedures
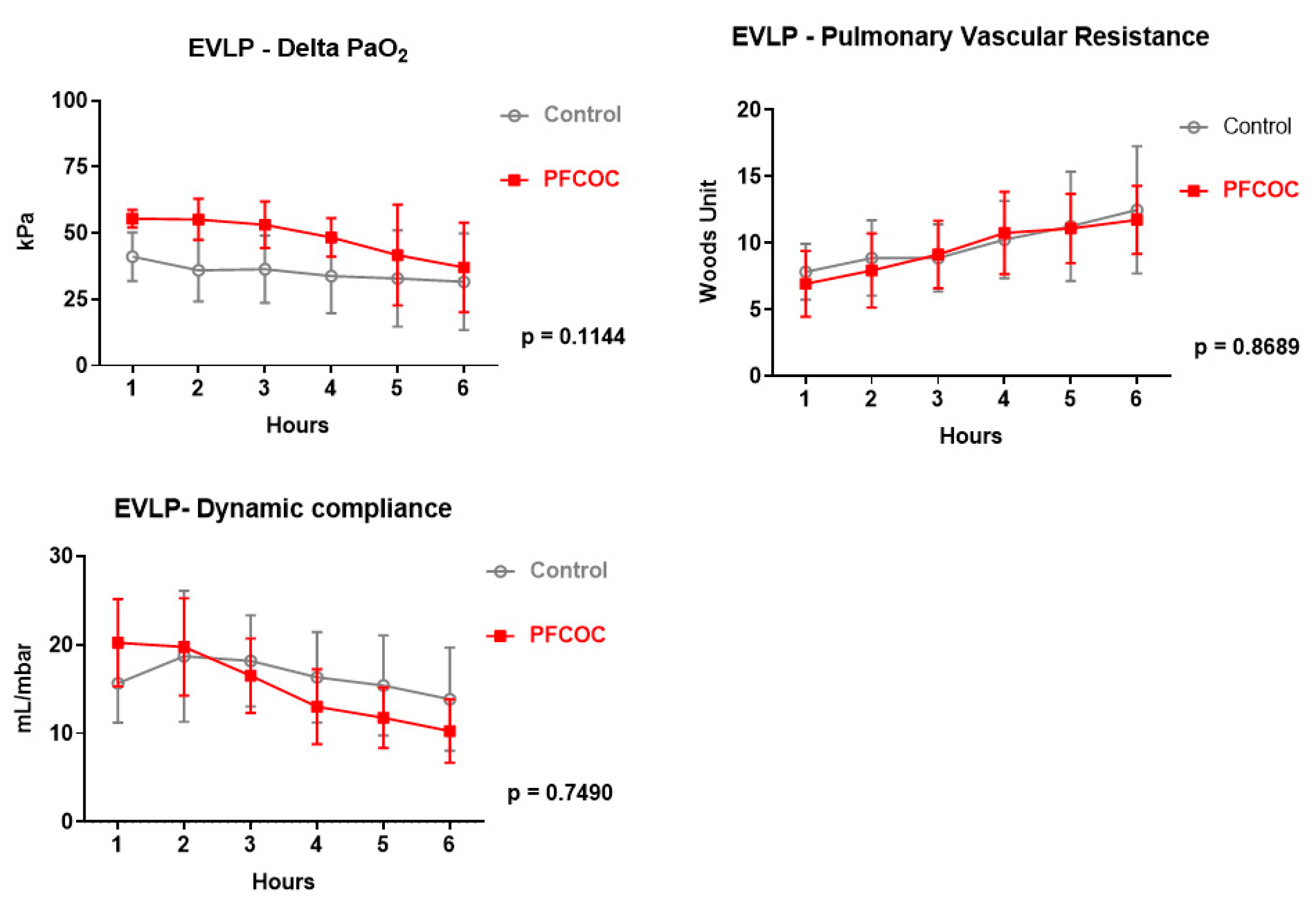
2.3. Physiological Assessment During EVLP and after Transplantation
2.4. Perfusate, Plasma, Bronchoalveolar Lavage (BAL), and Tissue Collection and Analyses
2.5. Assessment of the Inflammatory Response
2.6. Myeloperoxidase Activity Measurement
2.7. Estimate of Tissue ATP Content
2.8. Flavin Mononucleotide Measurement
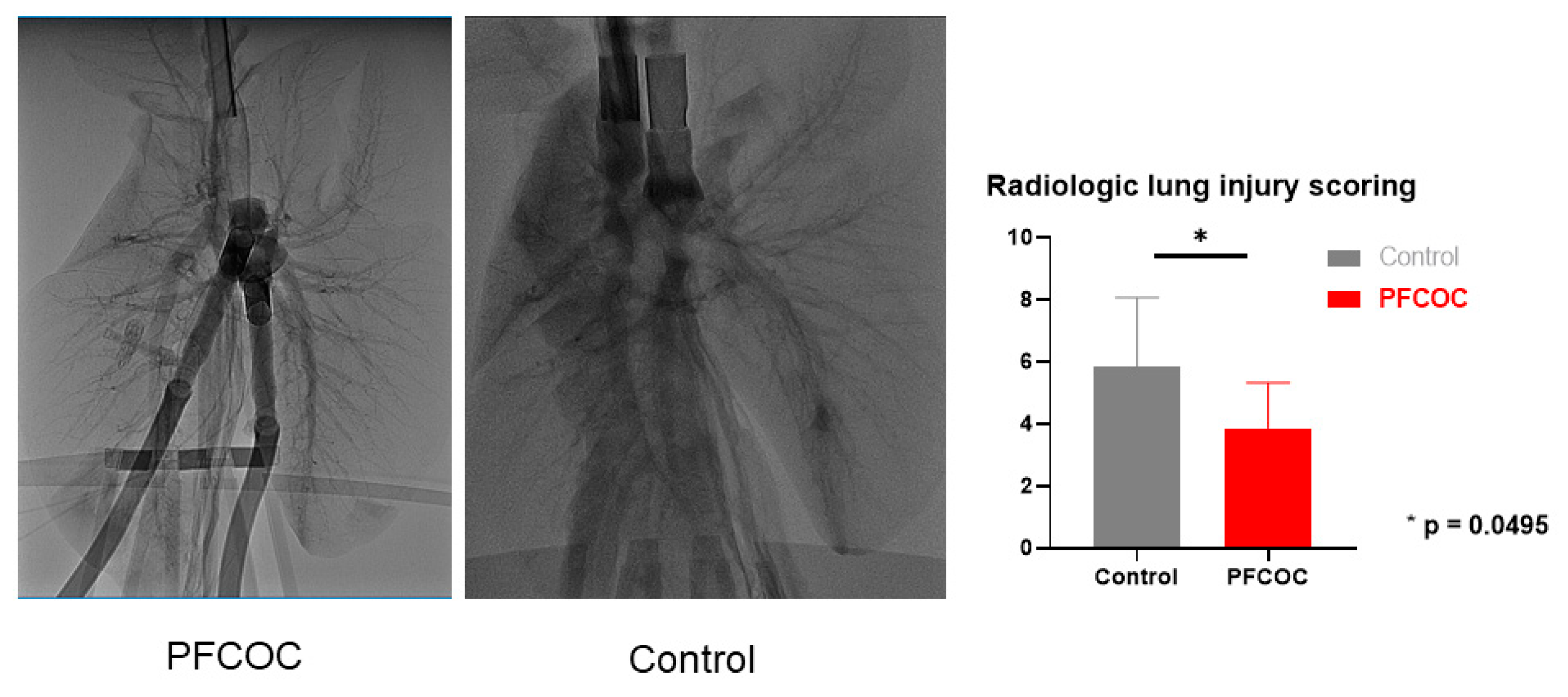
2.9. Radiologic Assessment of the Lungs
2.10. Histological Assessment of the Lungs
2.11. Transmission Electron Microscopy (TEM)
2.12. Preparation of PFCOC Emulsion
2.13. Timing and Dosage of PFCOC
3. Statistical Analysis
4. Results
4.1. EVLP Only Groups
Donor Characteristics
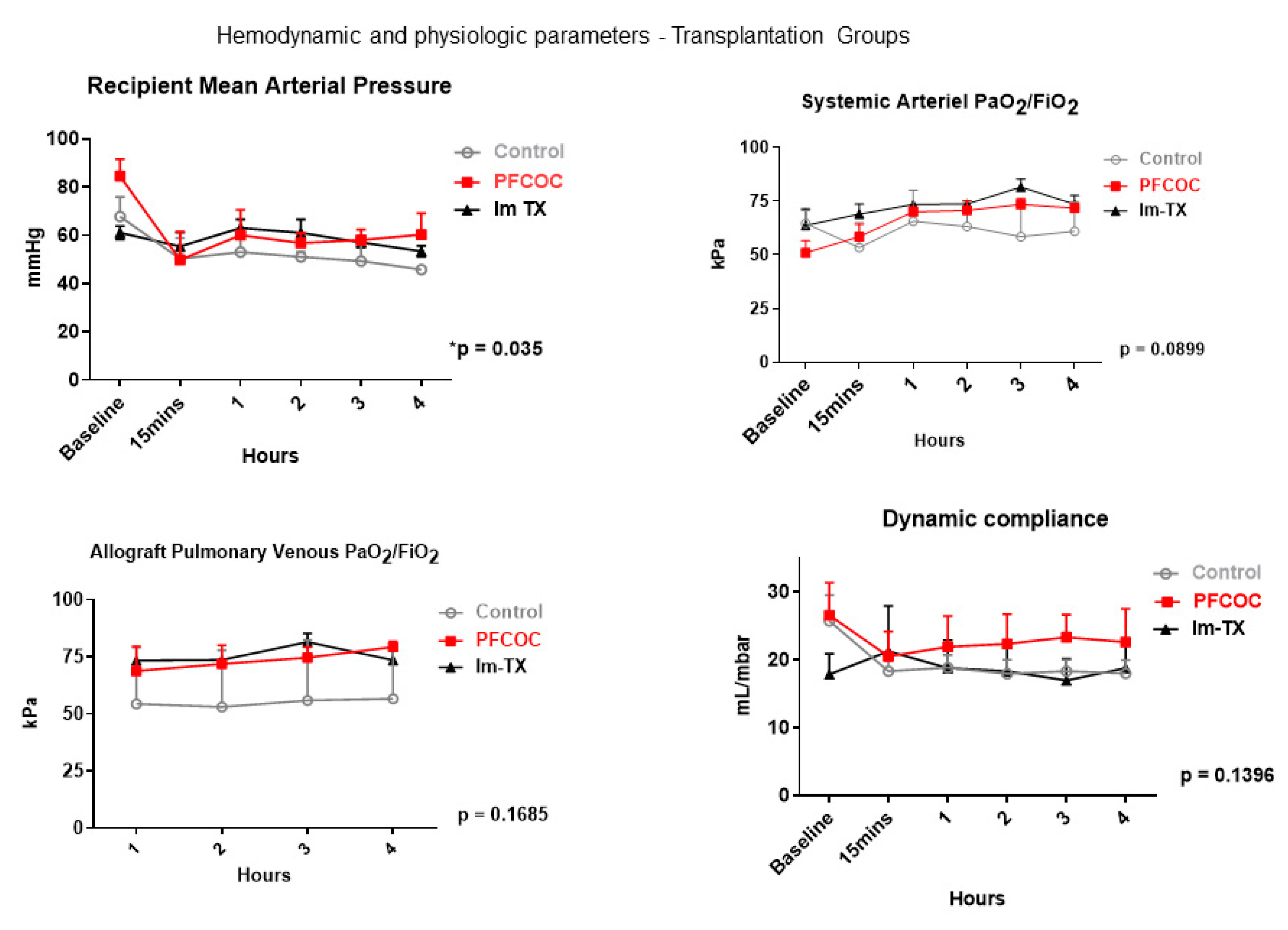
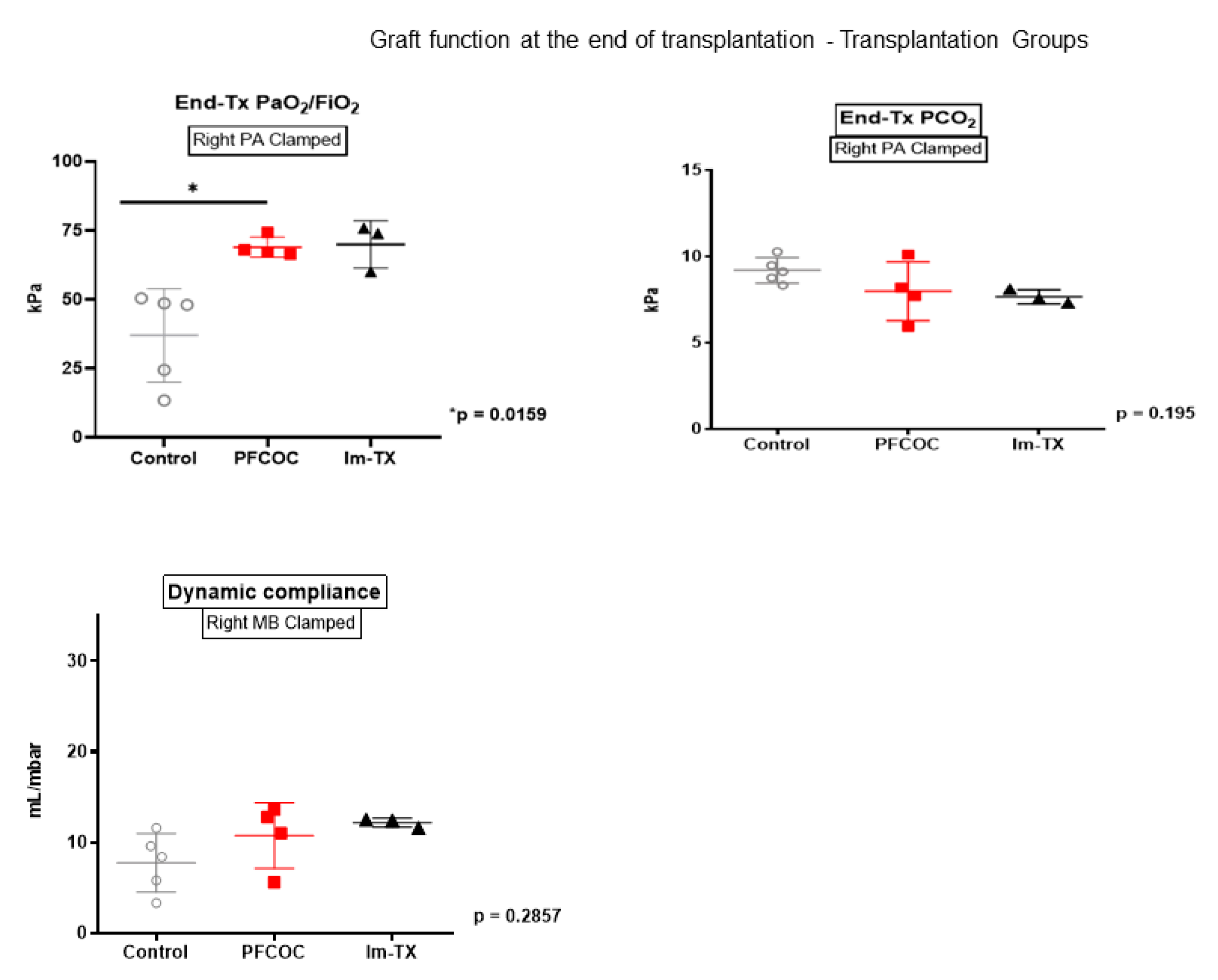
4.2. Results for Transplantation Groups
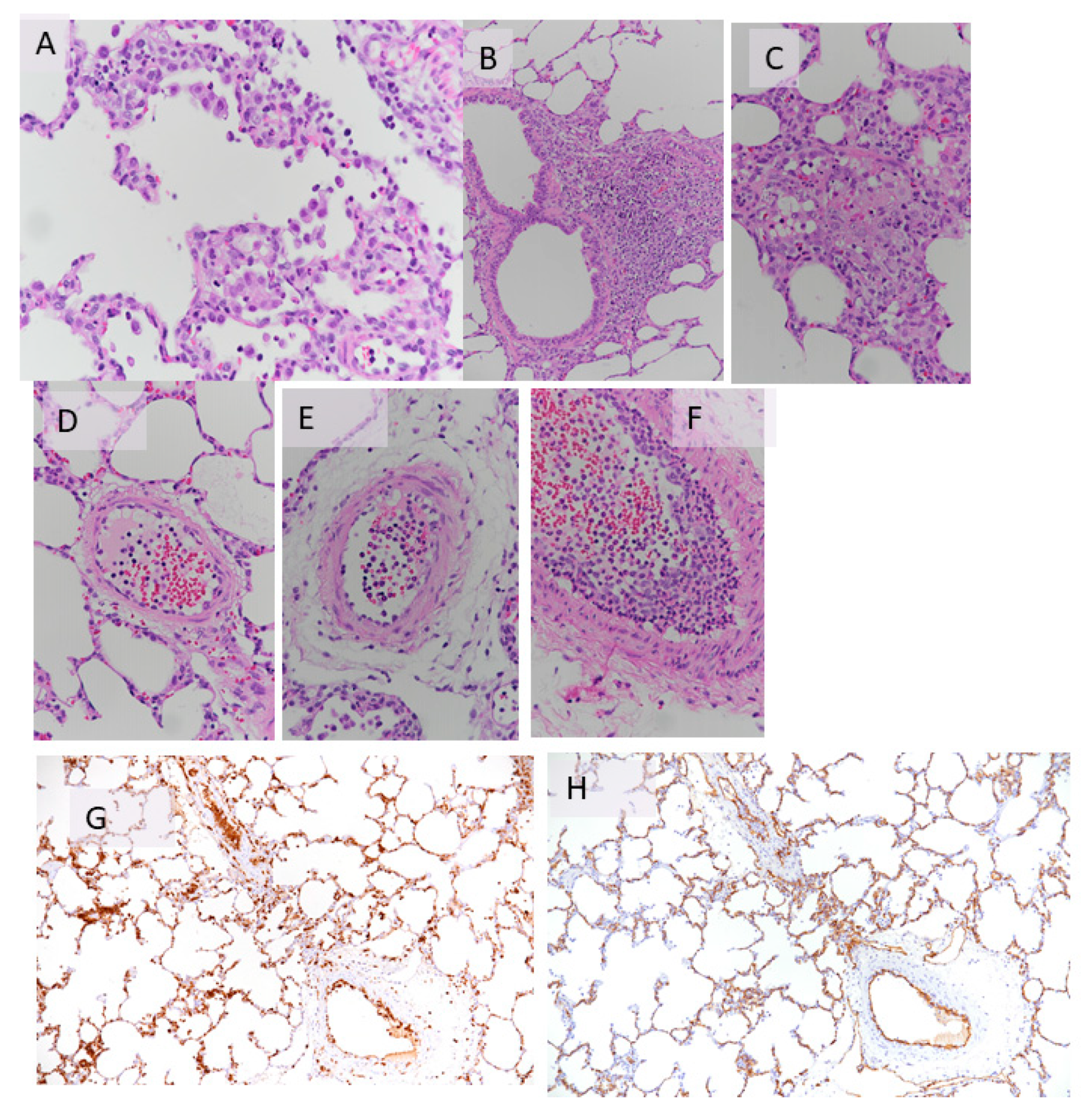
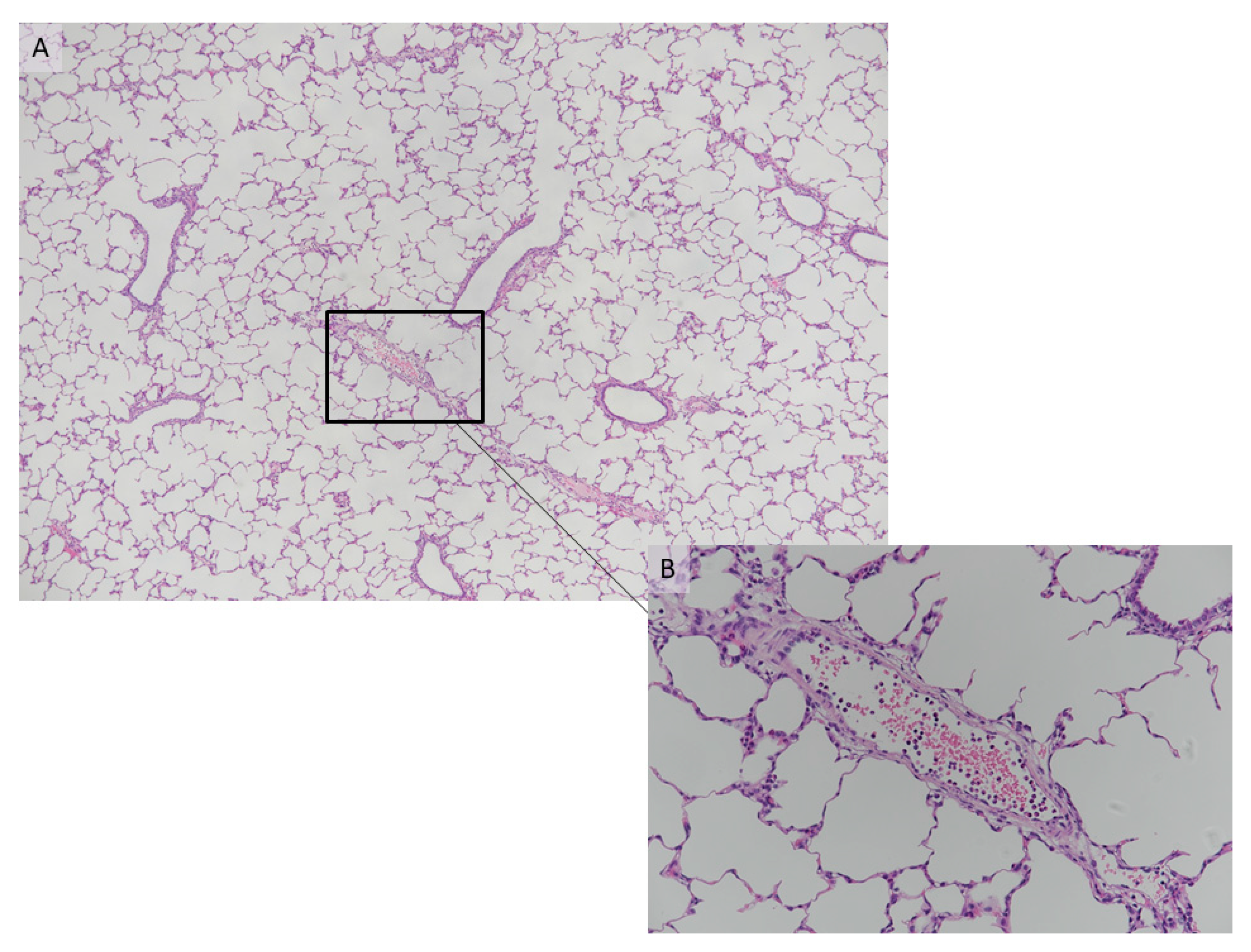
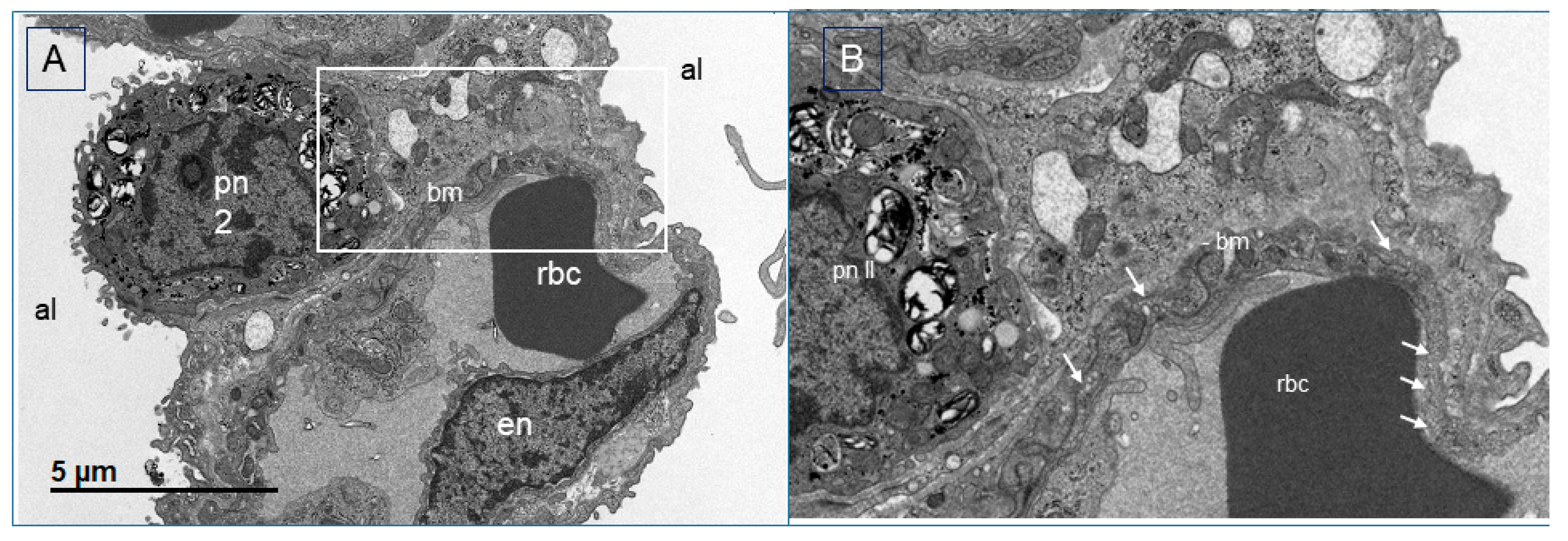
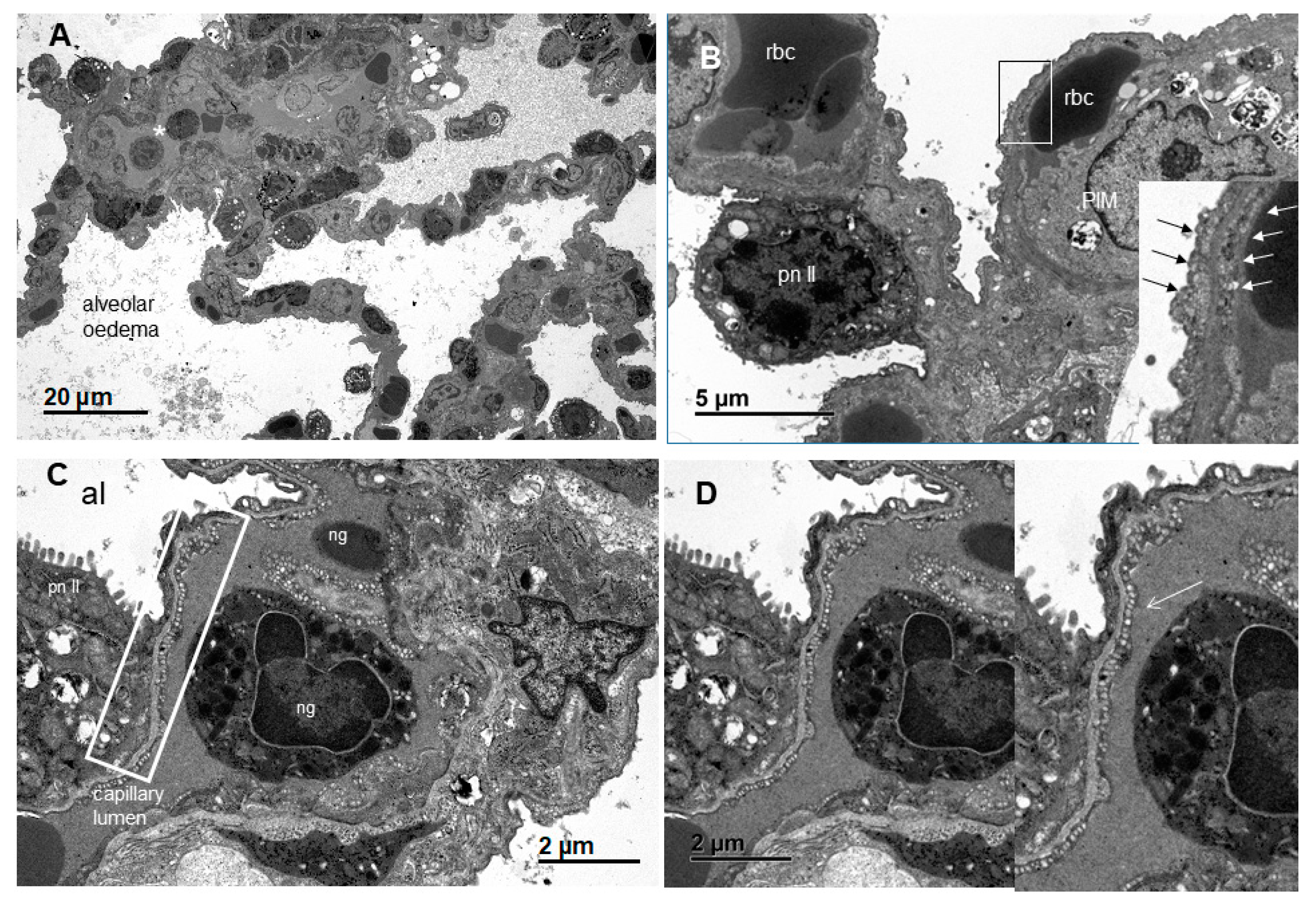
4.3. Histology of the Transplantation Groups
5. Discussion and Conclusions
- ▪
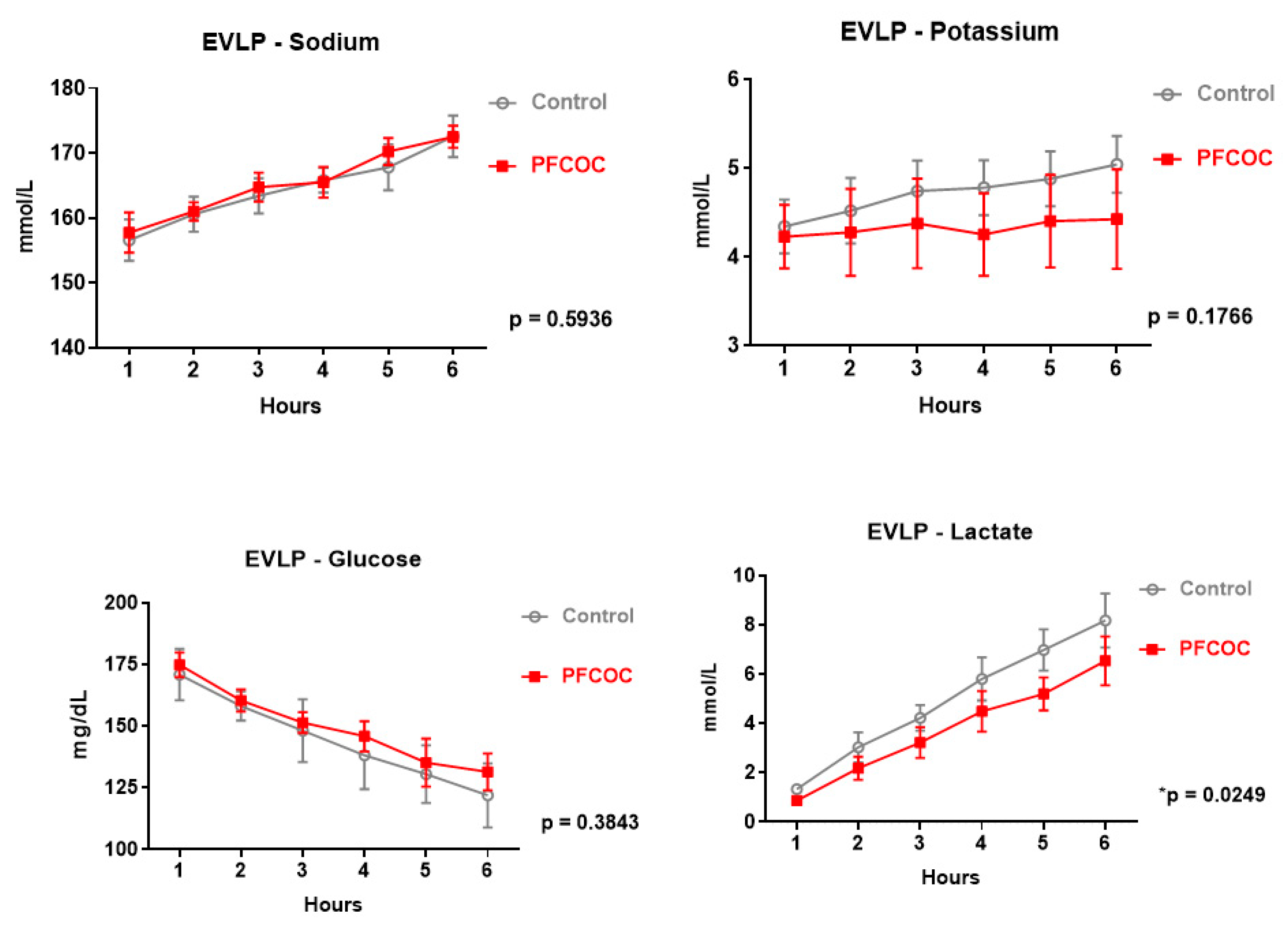
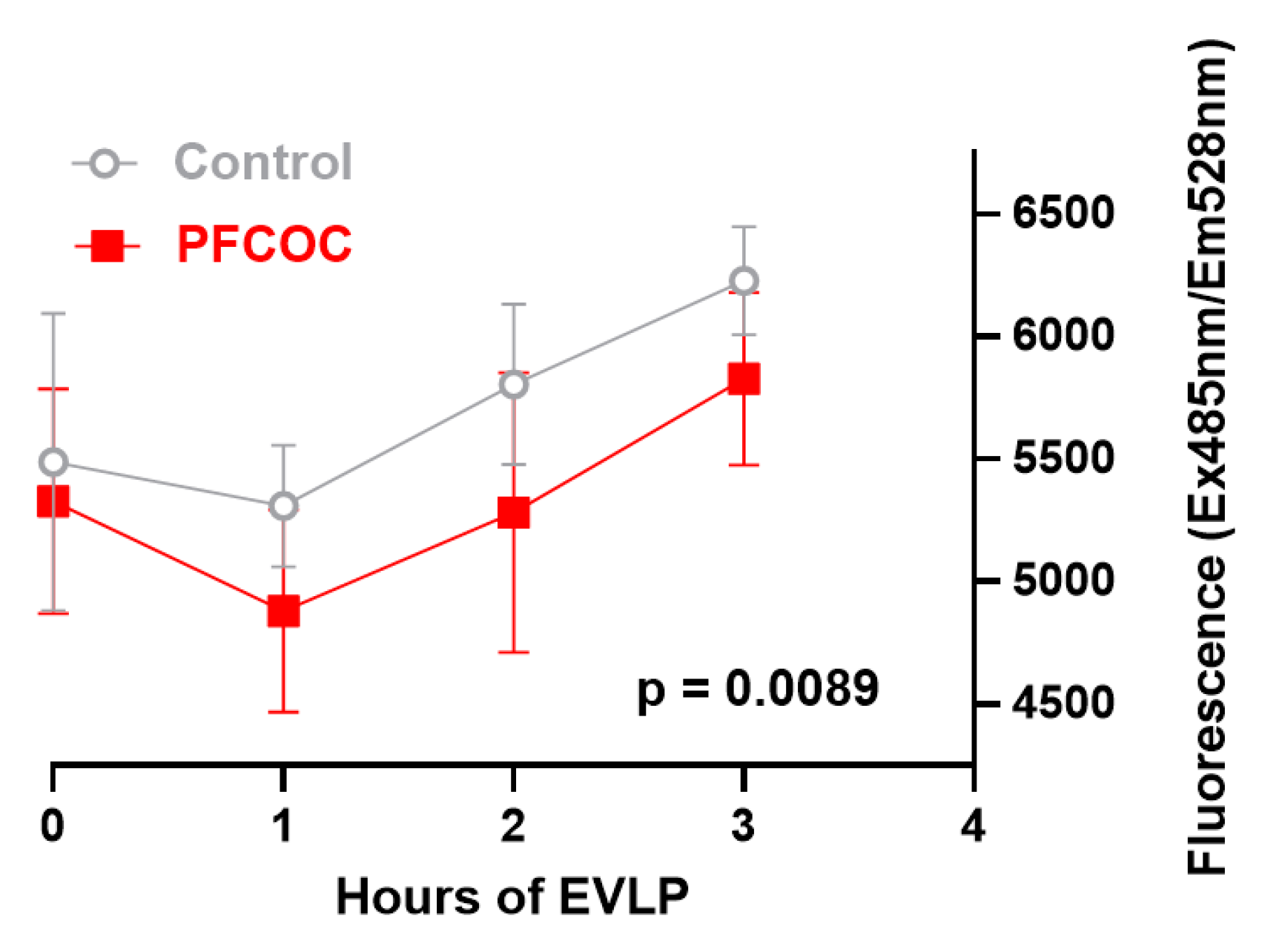
- In this experimental study, we tested the protective effect of PFCOC emulsion given during EVLP. We observed that metabolic markers of donor quality such as lactate production, glucose consumption and preservation of mitochondrial function were better in the PFCOC group. Following transplantation, the PFCOC group demonstrated better graft function and TEM showed better tissue preservation and cellular viability.
- ▪
- As the number of available organs is less than the number of the patients on the waiting list, the transplant community continues to search for alternatives to increase the number of available lung donors. These include extended criteria donors, DCD or utilizing EVLP for assessment of questionable lungs prior to implantation. A successful transplantation begins with the optimal preservation of the organ. In lung transplantation, the current standard is the infusion of cold organ preservation solution followed by cold static storage. In cold static storage, the metabolism is decreased, however, energy consumption continues and the hypoxic state activates anaerobic pathways, which results in cell death [51].
- ▪
- Perfluorocarbons (PFCs) are a class of chemicals that are essentially composed of carbon and fluorine atoms [36,38,39,52]. The fluorine atoms contribute to their high chemical and thermal stability [52]. Two essential features of the PFC are their unique gas-dissolving capacity and their exceptional chemical and biological “inertness” [52]. Their gas-dissolving capacity is a consequence of the weakness of the intermolecular forces that prevail in liquid fluorocarbons, which facilitate the formation of “holes” that can accommodate gas molecules within the liquid. On the other hand, their inertness reflects the strength of the intramolecular chemical bonds [36,38,39,52].
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Weill, D. Access to Lung Transplantation. The Long and Short of It. Am. J. Respir. Crit. Care Med. 2016, 193, 605–606. [Google Scholar] [CrossRef] [PubMed]
- Valapour, M.; Skeans, M.A.; Heubner, B.M.; Smith, J.M.; Hertz, M.I.; Edwards, L.B.; Cherikh, W.S.; Callahan, E.R.; Snyder, J.J.; Israni, A.K.; et al. OPTN/SRTR 2013 Annual Data Report: Lung. Arab. Archaeol. Epigr. 2015, 15, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yusen, R.D.; Shearon, T.H.; Qian, Y.; Kotloff, R.; Barr, M.L.; Sweet, S.; Dyke, D.B.; Murray, S. Lung Transplantation in the United States, 1999–2008. Arab. Archaeol. Epigr. 2010, 10, 1047–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charles, E.J.; Huerter, M.E.; Wagner, C.E.; Sharma, A.K.; Zhao, Y.; Stoler, M.H.; Mehaffey, J.H.; Isbell, J.M.; Lau, C.L.; Tribble, C.G.; et al. Donation after Circulatory Death Lungs Transplantable Up to Six Hours after Ex Vivo Lung Perfusion. Ann. Thorac. Surg. 2016, 102, 1845–1853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Raemdonck, D.E.; Rega, F.R.; Neyrinck, A.P.; Jannis, N.; Verleden, G.M.; Lerut, T.E. Non-heart-beating donors. Semin. Thorac. Cardiovasc. Surg. 2004, 16, 309–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierre, A.F.; Sekine, Y.; Hutcheon, M.A.; Waddell, T.K.; Keshavjee, S. Marginal donor lungs: A reassessment. J. Thorac. Cardiovasc. Surg. 2002, 123, 421–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artemiou, O.; Bîrsan, T.; Taghavi, S.; Eichler, I.; Wisser, W.; Wolner, E.; Klepetko, W. Bilateral lobar transplantation with the split lung technique. J. Thorac. Cardiovasc. Surg. 1999, 118, 369–370. [Google Scholar] [CrossRef] [Green Version]
- Cohen, M.R.G.; Starnes, M.V.A. Living Donor Lung Transplantation. World J. Surg. 2001, 25, 244–250. [Google Scholar] [CrossRef]
- Van Raemdonck, D.; Keshavjee, S.; Levvey, B.; Cherikh, W.S.; Snell, G.; Erasmus, M.; Simon, A.; Glanville, A.R.; Clark, S.; D’Ovidio, F.; et al. Donation after circulatory death in lung transplantation—Five-year follow-up from ISHLT Registry. J. Heart Lung Transplant. 2019, 38, 1235–1245. [Google Scholar] [CrossRef]
- Inci, I. Donors after cardiocirculatory death and lung transplantation. J. Thorac. Dis. 2017, 9, 2660–2669. [Google Scholar] [CrossRef] [Green Version]
- Cypel, M.; Yeung, J.C.; Liu, M.; Anraku, M.; Chen-Yoshikawa, T.F.; Karolak, W.; Sato, M.; Laratta, J.; Azad, S.; Madonik, M.; et al. Normothermic Ex Vivo Lung Perfusion in Clinical Lung Transplantation. New Engl. J. Med. 2011, 364, 1431–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Raemdonck, D.; Neyrinck, A.; Cypel, M.; Keshavjee, S. Ex-vivo lung perfusion. Transpl. Int. 2015, 28, 643–656. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, D.; Watanabe, Y.; Ohsumi, A.; Pipkin, M.; Chen, M.; Mordant, P.; Kanou, T.; Saito, T.; Lam, R.; Coutinho, R.; et al. Mesenchymal stromal cell therapy during ex vivo lung perfusion ameliorates ischemia-reperfusion injury in lung transplantation. J. Heart Lung Transplant. 2019, 38, 1214–1223. [Google Scholar] [CrossRef] [PubMed]
- Galasso, M.; Feld, J.J.; Watanabe, Y.; Pipkin, M.; Summers, C.; Ali, A.; Qaqish, R.; Chen, M.; Ribeiro, R.V.P.; Ramadan, K.; et al. Inactivating hepatitis C virus in donor lungs using light therapies during normothermic ex vivo lung perfusion. Nat. Commun. 2019, 10, 1–12. [Google Scholar] [CrossRef]
- Machuca, T.N.; Cypel, M.; Bonato, R.; Yeung, J.C.; Chun, Y.-M.; Juvet, S.; Guan, Z.; Hwang, D.M.; Chen, M.; Saito, T.; et al. Safety and Efficacy of Ex Vivo Donor Lung Adenoviral IL-10 Gene Therapy in a Large Animal Lung Transplant Survival Model. Hum. Gene Ther. 2017, 28, 757–765. [Google Scholar] [CrossRef]
- Carrel, A.; Lindbergh, C.A. The cultivation of whole thyroid glands. Comptes Rendus Hebd. Seances Acad. Sci. 1935, 201, 14–16. [Google Scholar]
- Steen, S.; Liao, Q.; Wierup, P.N.; Bolys, R.; Pierre, L.; Sjöberg, T. Transplantation of lungs from non–heart-beating donors after functional assessment ex vivo. Ann. Thorac. Surg. 2003, 76, 244–252. [Google Scholar] [CrossRef]
- Steen, S.; Sjöberg, T.; Pierre, L.; Liao, Q.; Eriksson, L.; Algotsson, L. Transplantation of lungs from a non-heart-beating donor. Lancet 2001, 357, 825–829. [Google Scholar] [CrossRef]
- Rega, F.R.; Wuyts, W.A.; Vanaudenaerde, B.M.; Jannis, N.C.; Neyrinck, A.P.; Verleden, G.M.; Lerut, T.E.; Van Raemdonck, D.E. Nebulized N-Acetyl Cysteine Protects the Pulmonary Graft Inside the Non–Heart-Beating Donor. J. Heart Lung Transplant. 2005, 24, 1369–1377. [Google Scholar] [CrossRef]
- Rega, F.R.; Jannis, N.C.; Verleden, G.M.; Flameng, W.J.; Lerut, T.E.; Van Raemdonck, D.E. Should we ventilate or cool the pulmonary graft inside the non–heart-beating donor? J. Heart Lung Transplant. 2003, 22, 1226–1233. [Google Scholar] [CrossRef]
- Rega, F.R.; Jannis, N.C.; Verleden, G.M.; Lerut, T.E.; Van Raemdonck, D.E.M. Long-term Preservation with Interim Evaluation of Lungs from a Non-Heart-Beating Donor after a Warm Ischemic Interval of 90 Minutes. Ann. Surg. 2003, 238, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Rega, F.R.; Vanaudenaerde, B.M.; Wuyts, W.A.; Jannis, N.C.; Verleden, G.M.; Lerut, T.E.; Van Raemdonck, D.E. IL-1β in bronchial lavage fluid is a non-invasive marker that predicts the viability of the pulmonary graft from the non-heart-beating donor. J. Heart Lung Transplant. 2005, 24, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Rega, F.R.; Neyrinck, A.P.; Verleden, G.M.; Lerut, T.E.; Van Raemdonck, D.E.M. How long can we preserve the pulmonary graft inside the nonheart-beating donor? Ann. Thorac. Surg. 2004, 77, 438–444. [Google Scholar] [CrossRef] [Green Version]
- Cypel, M.; Rubacha, M.; Yeung, J.; Hirayama, S.; Torbicki, K.; Madonik, M.; Fischer, S.; Hwang, D.; Pierre, A.; Waddell, T.K.; et al. NormothermicEx VivoPerfusion Prevents Lung Injury Compared to Extended Cold Preservation for Transplantation. Arab. Archaeol. Epigr. 2009, 9, 2262–2269. [Google Scholar] [CrossRef]
- Cypel, M.; Yeung, J.C.; Hirayama, S.; Rubacha, M.; Fischer, S.; Anraku, M.; Sato, M.; Harwood, S.; Pierre, A.; Waddell, T.K.; et al. Technique for Prolonged Normothermic Ex Vivo Lung Perfusion. J. Heart Lung Transplant. 2008, 27, 1319–1325. [Google Scholar] [CrossRef]
- Cypel, M.; Liu, M.; Rubacha, M.; Yeung, J.C.; Hirayama, S.; Anraku, M.; Sato, M.; Medin, J.; Davidson, B.L.; De Perrot, M.; et al. Functional Repair of Human Donor Lungs by IL-10 Gene Therapy. Sci. Transl. Med. 2009, 1, 4ra9. [Google Scholar] [CrossRef]
- Yeung, J.C.; Cypel, M.; Machuca, T.N.; Koike, T.; Cook, D.J.; Bonato, R.; Chen, M.; Sato, M.; Waddell, T.K.; Liu, M.; et al. Physiologic assessment of the ex vivo donor lung for transplantation. J. Heart Lung Transplant. 2012, 31, 1120–1126. [Google Scholar] [CrossRef]
- Inci, I.; Zhai, W.; Arni, S.; Inci, D.; Hillinger, S.; Lardinois, D.; Vogt, P.; Weder, W. Fibrinolytic Treatment Improves the Quality of Lungs Retrieved From Non-Heart-Beating Donors. J. Heart Lung Transplant. 2007, 26, 1054–1060. [Google Scholar] [CrossRef]
- Inci, I.; Zhai, W.; Arni, S.; Inci, D.; Hillinger, S.; Leskosek, B.; Weder, W. 145: Impact of Topical Cooling Solution and Prediction of Pulmonary Graft Viability from Non-Heart-Beating Donors. J. Heart Lung Transplant. 2008, 27, S112. [Google Scholar] [CrossRef]
- Inci, I.; Ampollini, L.; Arni, S.; Jungraithmayr, W.; Inci, D.; Hillinger, S.; Leskosek, B.; Vogt, P.; Weder, W. Ex Vivo Reconditioning of Marginal Donor Lungs Injured by Acid Aspiration. J. Heart Lung Transplant. 2008, 27, 1229–1236. [Google Scholar] [CrossRef]
- Inci, I.; Arni, S.; Acevedo, C.; Jungraithmayr, W.; Inci, D.; Vogt, P.; Weder, W. Surfactant alterations following donation after cardiac death donor lungs. Transpl. Int. 2010, 24, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Iskender, I.; Arni, S.; Hillinger, S.; Cosgun, T.; Yu, K.; Jungraithmayr, W.; Cesarovic, N.; Weder, W.; Inci, I. Ex vivo treatment with inhaled N-acetylcysteine in porcine lung transplantation. J. Surg. Res. 2017, 218, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Iskender, I.; Cosgun, T.; Arni, S.; Trinkwitz, M.; Fehlings, S.; Yamada, Y.; Cesarovic, N.; Yu, K.; Frauenfelder, T.; Jungraithmayr, W.; et al. Cytokine filtration modulates pulmonary metabolism and edema formation during ex vivo lung perfusion. J. Heart Lung Transplant. 2018, 37, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Inci, I.; Hillinger, S.; Arni, S.; Kaplan, T.; Inci, D.; Weder, W. Reconditioning of an injured lung graft with intrabronchial surfactant instillation in an ex vivo lung perfusion system followed by transplantation. J. Surg. Res. 2013, 184, 1143–1149. [Google Scholar] [CrossRef]
- Cosgun, T.; Iskender, I.; Yamada, Y.; Arni, S.; Lipiski, M.; Van Tilburg, K.; Weder, W.; Inci, I. Ex vivo administration of trimetazidine improves post-transplant lung function in pig model †. Eur. J. Cardio-Thoracic Surg. 2017, 52, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Riess, J.G. Oxygen carriers (“blood substitutes”)—Raison d’etre, chemistry, and some physiology. Chem. Rev. 2001, 101, 2797–2920. [Google Scholar] [CrossRef]
- Cabrales, P.; Intaglietta, M. Blood substitutes: Evolution from noncarrying to oxygen- and gas-carrying fluids. Asaio J. 2013, 59, 337–354. [Google Scholar] [CrossRef] [Green Version]
- Riess, J.G.; Krafft, M.P. Fluorocarbon emulsions as in vivo oxygen delivery systems: Background and chemistry A2. In Blood Substitutes; Winslow, R.M., Ed.; Academic Press: Oxford, UK, 2006; pp. 259–275. [Google Scholar]
- Krafft, M.P.; Riess, J.G. Perfluorocarbons: Life sciences and biomedical usesDedicated to the memory of Professor Guy Ourisson, a true RENAISSANCE man. J. Polym. Sci. Part A Polym. Chem. 2007, 45, 1185–1198. [Google Scholar] [CrossRef]
- Chu, S.-J.; Huang, K.-L.; Wu, S.-Y.; Ko, F.-C.; Wu, G.-C.; Li, R.-Y.; Li, M.-H. Systemic Administration of FC-77 Dampens Ischemia–Reperfusion-Induced Acute Lung Injury in Rats. Inflammation 2013, 36, 1383–1392. [Google Scholar] [CrossRef]
- Chang, H.; Kuo, F.-C.; Lai, Y.-S.; Chou, T.-C. Inhibition of inflammatory responses by FC-77, a perfluorochemical, in lipopolysaccharide-treated RAW 264.7 macrophages. Intensiv. Care Med. 2005, 31, 977–984. [Google Scholar] [CrossRef]
- Kawamae, K.; Pristine, G.; Chiumello, D.; Tremblay, L.N.; Slutsky, A.S. Partial liquid ventilation decreases serum tumor necrosis factor-α concentrations in a rat acid aspiration lung injury model. Crit. Care Med. 2000, 28, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Nakata, S.; Yasui, K.; Nakamura, T.; Kubota, N.; Baba, A. Perfluorocarbon Suppresses Lipopolysaccharide- and α-Toxin-Induced Interleukin-8 Release from Alveolar Epithelial Cells. Neonatology 2006, 91, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.M.; Steinhorn, D.M.; Thusu, K.; Fuhrman, B.P.; Dandona, P. A liquid perfluorochemical decreases the in vitro production of reactive oxygen species by alveolar macrophages. Crit. Care Med. 1995, 23, 1533–1539. [Google Scholar] [CrossRef] [PubMed]
- Krafft, M.P. Overcoming inactivation of the lung surfactant by serum proteins: A potential role for fluorocarbons? Soft Matter 2015, 11, 5982–5994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Thompson, E.; Bates, L.; Pither, T.L.; Hosgood, S.A.; Nicholson, M.L.; Watson, C.J.; Wilson, C.; Fisher, A.J.; Ali, S.; et al. Flavin Mononucleotide as a Biomarker of Organ Quality-A Pilot Study. Transpl. Direct 2020, 6, e600. [Google Scholar]
- Riess, J.G.; Cornélus, C.; Follana, R.; Krafft, M.P.; Mahé, A.M.; Postelf, M.; Zarif, L. Novel Fluorocarbon-Based Injectable Oxygen-Carrying Formulations with Long-Term Room-Temperature Storage Stability. Biol. Mammary Gland 1994, 345, 227–234. [Google Scholar] [CrossRef]
- Riess, J.G.; Krafft, M.P. Advanced Fluorocarbon-Based Systems for Oxygen and Drug Delivery, and Diagnosis. Artif. Cells Blood Substit. Biotechnol. 1997, 25, 43–52. [Google Scholar] [CrossRef]
- Riess, J.G.; Krafft, M.P. Fluorocarbons and Fluorosurfactants for In Vivo Oxygen Transport (Blood Substitutes), Imaging, and Drug Delivery. MRS Bull. 1999, 24, 42–48. [Google Scholar] [CrossRef]
- Krafft, M.P.; Riess, J.G. ChemInform Abstract: Chemistry, Physical Chemistry, and Uses of Molecular Fluorocarbon-Hydrocarbon Diblocks, Triblocks, and Related Compounds—Unique “Apolar” Components for Self-Assembled Colloid and Interface Engineering. ChemInform 2009, 40, 1714–1792. [Google Scholar] [CrossRef]
- Battula, N.R.; Andreoni, K.A. Oxygenated Preservation Solutions for Organ Preservation. Transplantation 2019, 103, 233–234. [Google Scholar] [CrossRef]
- Centis, V. Enhancing oxygen solubility using hemoglobin- and perfluorocarbon-based carriers. Front. Biosci. 2009, 14, 665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krafft, M.P.; Riess, J.G.; Weers, J.G. The Design and Engineering of Oxygen-Delivering Fluorocarbon Emulsions; Informa UK Limited: London, UK, 2019; pp. 235–334. [Google Scholar]
- Riess, J.G.; Postel, M. Stability and Stabilization of Fluorocarbon Emulsions Destined for Injection. Biomater. Artif. Cells Immobil. Biotechnol. 1992, 20, 819–830. [Google Scholar] [CrossRef] [PubMed]
- Riess, J.G.; Krafft, M.P. Fluorinated materials for in vivo oxygen transport (blood substitutes), diagnosis and drug delivery. Biomaterials 1998, 19, 1529–1539. [Google Scholar] [CrossRef]
- Weers, J.G. A physicochemical evaluation of perfluorochemicals for oxygen transport applications. J. Fluor. Chem. 1993, 64, 73–93. [Google Scholar] [CrossRef]
- Clark, L.C.; Gollan, F. Survival of Mammals Breathing Organic Liquids Equilibrated with Oxygen at Atmospheric Pressure. Science 1966, 152, 1755–1756. [Google Scholar] [CrossRef]
- Riess, J.G.; Le Blanc, M. Solubility and transport phenomena in perfluorochemicals relevant to blood substitution and other biomedical applications. Pure Appl. Chem. 1982, 54, 2383–2406. [Google Scholar] [CrossRef]
- Castro, C.I.; Triana, J.C.B. Perfluorocarbon-Based Oxygen Carriers: Review of Products and Trials. Artif. Organs 2010, 34, 622–634. [Google Scholar] [CrossRef]
- Yang, Z.-J.; Price, C.D.; Bosco, G.; Tucci, M.; El-Badri, N.S.; Mangar, D.; Camporesi, E.M. The Effect of Isovolemic Hemodilution with Oxycyte®, a Perfluorocarbon Emulsion, on Cerebral Blood Flow in Rats. PLoS ONE 2008, 3, e2010. [Google Scholar] [CrossRef]
- Chang, H.; Li, M.-H.; Chen, C.-W.; Yan, H.-C.; Huang, K.-L.; Chu, S.-J. Intravascular FC-77 attenuates phorbol myristate acetate-induced acute lung injury in isolated rat lungs. Crit. Care Med. 2008, 36, 1222–1229. [Google Scholar] [CrossRef]
- Schroeder, J.L.; Highsmith, J.M.; Young, H.F.; Mathern, B.E. Reduction of hypoxia by perfluorocarbon emulsion in a traumatic spinal cord injury model. J. Neurosurg. Spine 2008, 9, 213–220. [Google Scholar] [CrossRef]
- Mullah, S.H.; Saha, B.K.; AbuTarboush, R.; Walker, P.B.; Haque, A.; Arnaud, F.G.; Hazzard, B.; Auker, C.R.; McCarron, R.M.; Scultetus, A.H.; et al. Perfluorocarbon NVX-108 increased cerebral oxygen tension after traumatic brain injury in rats. Brain Res. 2016, 1634, 132–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leach, C.L.; Greenspan, J.S.; Rubenstein, S.D.; Shaffer, T.H.; Wolfson, M.R.; Jackson, J.C.; Delemos, R.A.; Fuhrman, B.P. Partial Liquid Ventilation with Perflubron in Premature Infants with Severe Respiratory Distress Syndrome. N. Engl. J. Med. 1996, 335, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Woods, S.D.; Skinner, R.D.; Brown, A.T.; Lowery, J.D.; Roberson, P.K.; Culp, W.C. Dodecafluoropentane Emulsion Decreases Cerebral Infarcts in a Rabbit Embolic Stroke Model. Circulation 2011, 124, A9303. [Google Scholar]
- Culp, W.C.; Woods, S.D.; Skinner, R.D.; Brown, A.T.; Lowery, J.D.; Johnson, J.L.H.; Unger, E.C.; Hennings, L.J.; Borrelli, M.J.; Roberson, P.K. Dodecafluoropentane Emulsion Decreases Infarct Volume in a Rabbit Ischemic Stroke Model. J. Vasc. Interv. Radiol. 2012, 23, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Habler, O.; Kleen, M.; Hutter, J.; Podtschaske, A.; Tiede, M.; Kemming, G.; Welte, M.; Corso, C.; Batra, S.; Keipert, P.; et al. Hemodilution and intravenous perflubron emulsion as an alternative to blood transfusion: Effects on tissue oxygenation during profound hemodilution in anesthetized dogs. Transfusion 1998, 38, 145–155. [Google Scholar] [CrossRef]
- Holman, W.L.; Spruell, R.D.; Ferguson, E.R.; Clymer, J.J.; Vicente, W.V.; Murrah, C.; Pacifico, A.D. Tissue oxygenation with graded dissolved oxygen delivery during cardiopulmonary bypass. J. Thorac. Cardiovasc. Surg. 1995, 110, 774–785. [Google Scholar] [CrossRef] [Green Version]
- Spahn, D.R.; van Brempt, R.; Theilmeier, G.; Reibold, J.P.; Welte, M.; Heinzerling, H.; Birck, K.M.; Keipert, P.E.; Messmer, K.; Heinzerling, H.; et al. Perflubron emulsion delays blood transfusions in orthopedic surgery. Anesthesiology 1999, 91, 1195–1208. [Google Scholar] [CrossRef]
- Kuzmiak-Glancy, S.; Covian, R.; Femnou, A.N.; Glancy, B.; Jaimes, R.; Wengrowski, A.M.; Garrott, K.; French, S.A.; Balaban, R.S.; Kay, M.W. Cardiac performance is limited by oxygen delivery to the mitochondria in the crystalloid-perfused working heart. Am. J. Physiol. Circ. Physiol. 2018, 314, H704–H715. [Google Scholar] [CrossRef]
- Deuchar, G.A.; Van Kralingen, J.C.; Work, L.M.; Santosh, C.; Muir, K.W.; McCabe, C.; Macrae, I.M. Preclinical Validation of the Therapeutic Potential of Glasgow Oxygen Level Dependent (GOLD) Technology: A Theranostic for Acute Stroke. Transl. Stroke Res. 2018, 10, 583–595. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, J.; Ying, M.; Spiekermann, K.; Holay, M.; Zhang, Y.; Chen, F.; Gong, H.; Lee, J.H.; Gao, W.; Fang, R.H.; et al. Biomimetic Nanoemulsions for Oxygen Delivery In Vivo. Adv. Mater. 2018, 30, e1804693. [Google Scholar] [CrossRef]
- Hou, S.; Ding, H.; Lv, Q.; Yin, X.; Song, J.; Landén, N.X.; Fan, H. Therapeutic Effect of Intravenous Infusion of Perfluorocarbon Emulsion on LPS-Induced Acute Lung Injury in Rats. PLoS ONE 2014, 9, e87826. [Google Scholar] [CrossRef] [PubMed]
- Okumura, S.; Uemura, T.; Zhao, X.; Masano, Y.; Tsuruyama, T.; Fujimoto, Y.; Iida, T.; Yagi, S.; Bezinover, D.; Spiess, B.; et al. Liver graft preservation using perfluorocarbon improves the outcomes of simulated donation after cardiac death liver transplantation in rats. Liver Transplant. 2017, 23, 1171–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spahn, D.R.; Waschke, K.F.; Standl, T.; Motsch, J.; Van Huynegem, L.; Welte, M.; Gombotz, H.; Coriat, P.; Verkh, L.; Faithfull, S.; et al. Use of perflubron emulsion to decrease allogeneic blood transfusion in high-blood-loss non-cardiac surgery—Results of a European phase 3 study. Anesthesiology 2002, 97, 1338–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paxian, M.; Rensing, H.; Geckeis, K.; Bauer, I.; Kubulus, D.; Spahn, D.R.; Bauer, M. Perflubron emulsion in prolonged hemorrbagic shock—Influence on hepatocellular energy metabolism and oxygen-dependent gene expression. Anesthesiology 2003, 98, 1391–1399. [Google Scholar] [CrossRef] [PubMed]
- Paxian, M.; Keller, S.A.; Huynh, T.; Clemens, M.G. Perflubron Emulsion Improves Hepatic Microvascular Integrity and Mitochondrial Redox State after Hemorrhagic Shock. Shock 2003, 20, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Schubert, A. Current Artificial Oxygen Carriers and Their Potential Role in the Management of Hemorrhage. Int. Trauma Care 2008, 18, 86–93. [Google Scholar]
- Flaim, S.F. Pharmacokinetics and Side Effects of Perfluorocarbon-Based Blood Substitutes. Artif. Cells Blood Substit. Biotechnol. 1994, 22, 1043–1054. [Google Scholar] [CrossRef]
- Smith, D.J.; Lane, T.A. Effect of a high concentration perfluorocarbon emulsion on platelet function. Biomater. Artif. Cells Immobil. Biotechnol. 1992, 20, 1045–1049. [Google Scholar]
- Gale, S.C.; Gorman, G.D.; Copeland, J.G.; McDonagh, P.F. Perflubron Emulsion Prevents PMN Activation and Improves Myocardial Functional Recovery after Cold Ischemia and Reperfusion. J. Surg. Res. 2007, 138, 135–140. [Google Scholar] [CrossRef]
- AbuTarboush, R.; Saha, B.K.; Mullah, S.H.; Arnaud, F.; Haque, A.; Aligbe, C.; Pappas, G.; Auker, C.R.; McCarron, R.M.; Moon-Massat, P.; et al. Cerebral Microvascular and Systemic Effects Following Intravenous Administration of the Perfluorocarbon Emulsion Perftoran. J. Funct. Biomater. 2016, 7, 29. [Google Scholar] [CrossRef]
- Dominguez, M.S.; Maillard, E.; Krafft, M.P.; Sigrist, S.; Belcourt, A. Prevention of adhesion and promotion of pseudoislets formation from a beta-cell line by fluorocarbon emulsions. Chembiochem 2006, 7, 1160–1163. [Google Scholar] [CrossRef] [PubMed]
- Kruse, J.A.; Carlson, R.W. Lactate metabolism. Crit. Care Clin. 1987, 3, 725–746. [Google Scholar] [CrossRef]
- Roman, M.A.; Nair, S.; Tsui, S.; Dunning, J.; Parmar, J.S. Ex Vivo Lung Perfusion. Transplantation 2013, 96, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Valenza, F.; Rosso, L.; Pizzocri, M.; Salice, V.; Umbrello, M.; Conte, G.; Stanzi, A.; Colombo, J.; Gatti, S.; Santambrogio, L.; et al. The Consumption of Glucose during Ex Vivo Lung Perfusion Correlates with Lung Edema. Transplant. Proc. 2011, 43, 993–996. [Google Scholar] [CrossRef] [PubMed]
- Koike, T.; Yeung, J.; Cypel, M.; Rubacha, M.; Matsuda, Y.; Liu, M.; Waddell, T.K.; Keshavjee, S. 283: Lactate Production during Acellular Normothermic Ex Vivo Pig and Human Lung Perfusion. J. Heart Lung Transplant. 2010, 29, S96. [Google Scholar] [CrossRef]
- Koike, T.; Yeung, J.C.; Cypel, M.; Rubacha, M.; Matsuda, Y.; Sato, M.; Waddell, T.K.; Liu, M.; Keshavjee, S. Kinetics of lactate metabolism during acellular normothermic ex vivo lung perfusion. J. Heart Lung Transplant. 2011, 30, 1312–1319. [Google Scholar] [CrossRef]
- Hirst, J. Mitochondrial complex I. Annu. Rev. Biochem. 2013, 82, 551–575. [Google Scholar] [CrossRef]
- Stepanova, A.; Sosunov, S.; Niatsetskaya, Z.; Konrad, C.; Starkov, A.A.; Manfredi, G.; Wittig, I.; Ten, V.; Galkin, A.; Sosunov, S. Redox-Dependent Loss of Flavin by Mitochondrial Complex I in Brain Ischemia/Reperfusion Injury. Antioxid. Redox Signal. 2019, 31, 608–622. [Google Scholar] [CrossRef]
- Muller, X.; Schlegel, A.; Kron, P.; Eshmuminov, D.; Würdinger, M.; Meierhofer, D.; Clavien, P.-A.; Dutkowski, P. Novel Real-time Prediction of Liver Graft Function During Hypothermic Oxygenated Machine Perfusion Before Liver Transplantation. Ann. Surg. 2019, 270, 783–790. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cytokine | Control | PFCOC | p Value |
|---|---|---|---|
| TNFα | 335.1 ± 335.2 | 161.6 ± 76.9 | 0.6667 |
| IL1-α | 68 ± 46.8 | 28 ± 20.9 | 0.2857 |
| IL1-β | 982 ± 777.1 | 599.6 ± 345.1 | 0.5556 |
| IL1-Ra | 944.7 ± 384.3 | 703 ± 461.3 | 0.7302 |
| IL-2 | 1224.9 ± 922.7 | 1439 ± 466.4 | 0.7302 |
| IL-4 | 6108.8 ± 5479.9 | 6657.6 ± 2611 | 0.9999 |
| IL-6 | 3612.3 ± 1786.4 | 3680.2 ± 910.4 | 0.9999 |
| IL-8 | 33901.1 ± 10995.8 | 38632.6 ± 15126 | 0.7302 |
| IL-10 | 871.4 ± 796.4 | 935.6 ± 376.8 | 0.5556 |
| IL-12 | 438.6 ± 130.9 | 346.4 ± 72.8 | 0.2857 |
| IL-18 | 10845.1 ± 3782.1 | 10142.8 ± 4613 | 0.7302 |
| Control | PFCOC | p Value | |
|---|---|---|---|
| IFNγ | 1605.3 ± 264.4 | 1602.6 ± 509.7 | 0.9048 |
| TNFα | 72.4 ± 53.1 | 23.8 ± 9.9 | 0.44 |
| IL1-β | 355.8 ± 244 | 261.9 ± 136 | 0.7302 |
| IL1-Ra | 12.1 ± 20.8 | 8.7 ± 10.9 | 0.9762 |
| IL-4 | 12.1 ± 20.8 | 221.5 ± 284.4 | 0.9048 |
| IL-6 | 331.3 ± 55 | 334.2 ± 143 | 0.7302 |
| IL-8 | 477.2 ± 892 | 3.3 ± 3.9 | 0.0159 |
| IL-10 | 226.5 ± 283.2 | 160.3 ± 137.1 | 0.7302 |
| IL-12 | 1116.3 ± 116.5 | 916.3 ± 105.9 | 0.0317 |
| IL-18 | 524 ± 498.9 | 572 ± 317.1 | 0.7302 |
| Control | PFCOC | p Value | |
|---|---|---|---|
| IL1-α | 20.6 ± 10 | 9.1 ± 16.6 | 0.1111 |
| IL1-β | 583.5 ± 563.1 | 104.8 ± 91.2 | 0.0653 |
| IL1-Ra | 3057 ± 2896 | 439.4 ± 289.8 | 0.1111 |
| IL-2 | 29.7 ± 26.7 | 529.6 ± 779.4 | 0.0635 |
| IL-4 | 73.5 ± 92.9 | 2269 ± 1909 | 0.7302 |
| IL-6 | 601.5 ± 123 | 931.2 ± 194.7 | 0.0317 |
| IL-8 | 3064 ± 2160 | 3118 ± 3526 | 0.5556 |
| IL-10 | 24 ± 25.3 | 248.6 ± 419.8 | 0.5556 |
| IL-12 | 159.1 ± 107.1 | 102.6 ± 83.2 | 0.7302 |
| IL-18 | 272.2 ± 96 | 2282 ± 2687 | 0.1905 |
| Group | NL in Vessels | NL Emigration | NL in Alveoli | Total Score | Average Score |
|---|---|---|---|---|---|
| CONT | 1 | 1 | 1 | 3 | |
| CONT | 1.5 | 1 | 1 | 3.5 | |
| CONT | 2 | 2 | 3 | 7 | 5.2 |
| CONT | 1 | 1 | 1.5 | 3.5 | |
| CONT | 3 | 3 | 3 | 9 | |
| PFCOC | 1 | 1 | 0.5 | 2.5 | |
| PFCOC | 2 | 1.5 | 0 | 3.5 | 2.8 |
| PFCOC | 1 | 1.5 | 0 | 2.5 | |
| PFCOC | 1.5 | 1.5 | 0 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inci, I.; Arni, S.; Iskender, I.; Citak, N.; Rodriguez, J.M.; Weisskopf, M.; Opitz, I.; Weder, W.; Frauenfelder, T.; Krafft, M.P.; et al. Functional, Metabolic and Morphologic Results of Ex Vivo Donor Lung Perfusion with a Perfluorocarbon-Based Oxygen Carrier Nanoemulsion in a Large Animal Transplantation Model. Cells 2020, 9, 2501. https://doi.org/10.3390/cells9112501
Inci I, Arni S, Iskender I, Citak N, Rodriguez JM, Weisskopf M, Opitz I, Weder W, Frauenfelder T, Krafft MP, et al. Functional, Metabolic and Morphologic Results of Ex Vivo Donor Lung Perfusion with a Perfluorocarbon-Based Oxygen Carrier Nanoemulsion in a Large Animal Transplantation Model. Cells. 2020; 9(11):2501. https://doi.org/10.3390/cells9112501
Chicago/Turabian StyleInci, Ilhan, Stephan Arni, Ilker Iskender, Necati Citak, Josep Monné Rodriguez, Miriam Weisskopf, Isabelle Opitz, Walter Weder, Thomas Frauenfelder, Marie Pierre Krafft, and et al. 2020. "Functional, Metabolic and Morphologic Results of Ex Vivo Donor Lung Perfusion with a Perfluorocarbon-Based Oxygen Carrier Nanoemulsion in a Large Animal Transplantation Model" Cells 9, no. 11: 2501. https://doi.org/10.3390/cells9112501
APA StyleInci, I., Arni, S., Iskender, I., Citak, N., Rodriguez, J. M., Weisskopf, M., Opitz, I., Weder, W., Frauenfelder, T., Krafft, M. P., & Spahn, D. R. (2020). Functional, Metabolic and Morphologic Results of Ex Vivo Donor Lung Perfusion with a Perfluorocarbon-Based Oxygen Carrier Nanoemulsion in a Large Animal Transplantation Model. Cells, 9(11), 2501. https://doi.org/10.3390/cells9112501