
Association Study of SLC6A4 (5-HTTLPR) Polymorphism and Its Promoter Methylation with Rehabilitation Outcome in Patients with Subacute Stroke

 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Rehabilitation Treatment and Outcome
2.3. DNA Extraction
2.4. SLC6A4 (5-HTTLPR) Genotyping
2.5. DNA Bisulphite Conversion and SLC6A4 Methylation Analysis
2.6. Statistical Analysis
3. Results
3.1. Samples

{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD), or Count (%) |
|---|---|
| Age | 68.7 (14.3) |
| Sex | 27 men (54.0%) 23 women (46.0%) |
| Time since stroke (days) | 89.7 (31.1) |
| Type of stroke | 37 ischemic (74.0%) 13 hemorrhagic (26.0%) |
| Hemiparesis side | 20 right (40.0%) 30 left (60.0%) |
| Spatial Neglect | 10 (20.0%) |
| Language impairment | 9 (18.0%) |
| SSRI | 26 (52.0%) |
| Modified Barthel Index | 38.5 (17.7) |
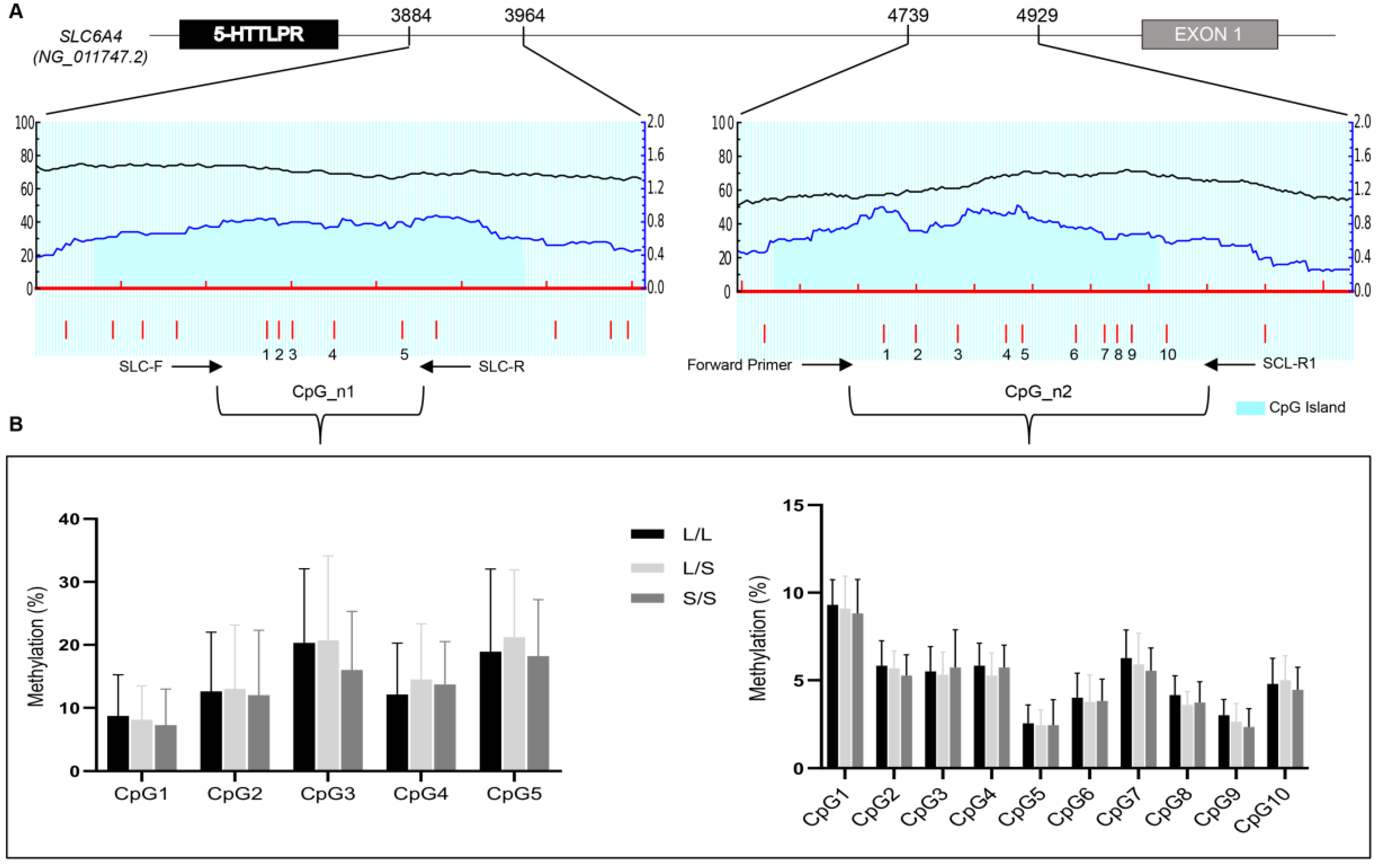
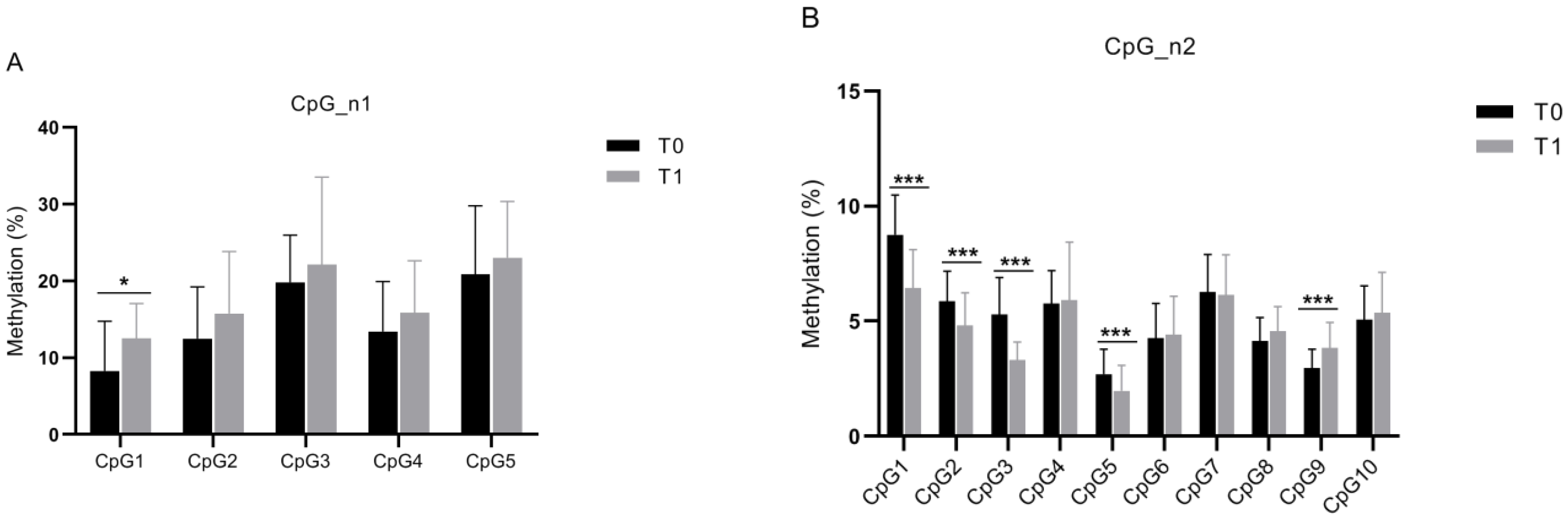
3.2. 5-HTTLPR Genotype and Methylation Analysis

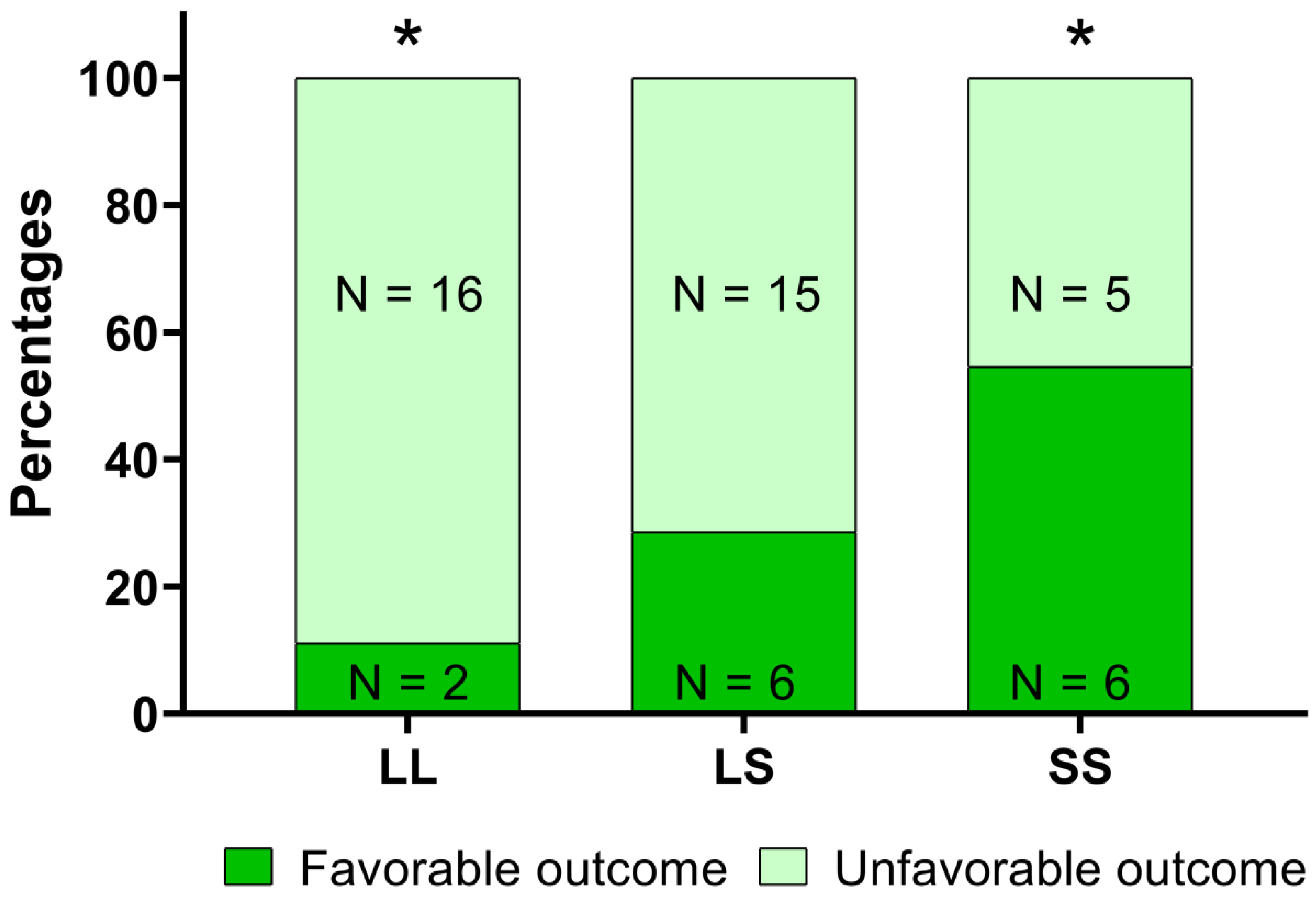
3.3. Correlation of 5-HTTLPR Genotype/Methylation Analysis and Rehabilitation Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Executive summary: Heart disease and stroke statistics-2016 update: A Report from the American Heart Association. Circulation 2016, 133, 447–454. [Google Scholar] [CrossRef]
- Prabhakaran, S.; Zarahn, E.; Riley, C.; Speizer, A.; Chong, J.Y.; Lazar, R.M.; Marshall, R.S.; Krakauer, J.W. Inter-individual variability in the capacity for motor recovery after ischemic stroke. Neurorehabil. Neural Repair 2008, 22, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Kollen, B. Predicting improvement in the upper paretic limb after stroke: A longitudinal prospective study. Restor. Neurol. Neurosci. 2007, 25, 453–460. [Google Scholar] [PubMed]
- Stinear, C.M.; Barber, P.A.; Petoe, M.; Anwar, S.; Byblow, W.D. The PREP algorithm predicts potential for upper limb recovery after stroke. Brain 2012, 135, 2527–2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stinear, C.M.; Barber, P.A.; Smale, P.R.; Coxon, J.P.; Fleming, M.K.; Byblow, W.D. Functional potential in chronic stroke patients depends on corticospinal tract integrity. Brain 2007, 130, 170–180. [Google Scholar] [CrossRef]
- Vogt, G.; Laage, R.; Shuaib, A.; Schneider, A. Initial lesion volume is an independent predictor of clinical stroke outcome at day 90: An analysis of the Virtual International Stroke Trials Archive (VISTA) database. Stroke 2012, 43, 1266–1272. [Google Scholar] [CrossRef] [Green Version]
- Cheng, B.; Forkert, N.D.; Zavaglia, M.; Hilgetag, C.C.; Golsari, A.; Siemonsen, S.; Fiehler, J.; Pedraza, S.; Puig, J.; Cho, T.H.; et al. Influence of stroke infarct location on functional outcome measured by the modified rankin scale. Stroke 2014, 45, 1695–1702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinlan, E.B.; Dodakian, L.; See, J.; McKenzie, A.; Le, V.; Wojnowicz, M.; Shahbaba, B.; Cramer, S.C. Neural function, injury, and stroke subtype predict treatment gains after stroke. Ann. Neurol. 2015, 77, 132–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyd, L.A.; Hayward, K.S.; Ward, N.S.; Stinear, C.M.; Rosso, C.; Fisher, R.J.; Carter, A.R.; Leff, A.P.; Copland, D.A.; Carey, L.M.; et al. Biomarkers of Stroke Recovery: Consensus-Based Core Recommendations from the Stroke Recovery and Rehabilitation Roundtable*. Neurorehabil. Neural Repair 2017, 31, 864–876. [Google Scholar] [CrossRef]
- Pearson-Fuhrhop, K.M.; Cramer, S.C. Genetic influences on neural plasticity. PubMed 2010, 2 (Suppl. 2), S227–S240. [Google Scholar] [CrossRef]
- Luddington, N.S.; Mandadapu, A.; Husk, M.; El-Mallakh, R.S. Clinical implications of genetic variation in the serotonin transporter promoter region: A review. Prim. Care Companion J. Clin. Psychiatry 2009, 11, 93–102. [Google Scholar] [CrossRef]
- Santoro, M.; Siotto, M.; Germanotta, M.; Bray, E.; Mastrorosa, A.; Galli, C.; Papadopoulou, D.; Aprile, I. Bdnf rs6265 polymorphism and its methylation in patients with stroke undergoing rehabilitation. Int. J. Mol. Sci. 2020, 21, 8438. [Google Scholar] [CrossRef]
- Booij, L.; Richard, T.; Szyf, M.; Benkelfat, C. Genetic and early environmental influences on the serotonin system: Consequences for brain development and risk for psychopathology. J. Psychiatry Neurosci. 2015, 40, 5–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesch, K.P.; Balling, U.; Gross, J.; Strauss, K.; Wolozin, B.L.; Murphy, D.L.; Riederer, P. Organization of the human serotonin transporter gene. J. Neural Transm. 1994, 95, 157–162. [Google Scholar] [CrossRef]
- Heils, A.; Teufel, A.; Petri, S.; Seemann, M.; Bengel, D.; Balling, U.; Riederer, P.; Lesch, K.P. Functional promoter and polyadenylation site mapping of the human serotonin (5-HT) transporter gene. J. Neural Transm. 1995, 102, 247–254. [Google Scholar] [CrossRef]
- Nakatani, D.; Sato, H.; Sakata, Y.; Shiotani, I.; Kinjo, K.; Mizuno, H.; Shimizu, M.; Ito, H.; Koretsune, Y.; Hirayama, A.; et al. Influence of serotonin transporter gene polymorphism on depressive symptoms and new cardiac events after acute myocardial infarction. Am. Heart J. 2005, 150, 652–658. [Google Scholar] [CrossRef]
- Lesch, K.P.; Mössner, R. Genetically driven variation in serotonin uptake: Is there a link to affective spectrum, neurodevelopmental, and neurodegenerative disorders? Biol. Psychiatry 1998, 44, 179–192. [Google Scholar] [CrossRef]
- Bleich, S.; Bönsch, D.; Rauh, J.; Bayerlein, K.; Fiszer, R.; Frieling, H.; Hillemacher, T. Association of the long allele of the 5-HTTLPR polymorphism with compulsive craving in alcohol dependence. Alcohol Alcohol. 2007, 42, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Gerra, G.; Garofano, L.; Santoro, G.; Bosari, S.; Pellegrini, C.; Zaimovic, A.; Moi, G.; Bussandri, M.; Moi, A.; Brambilla, F.; et al. Association between Low-Activity Serotonin Transporter Genotype and Heroin Dependence: Behavioral and Personality Correlates. Am. J. Med. Genet. 2004, 126, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Caspi, A.; Sugden, K.; Moffitt, T.E.; Taylor, A.; Craig, I.W.; Harrington, H.L.; McClay, J.; Mill, J.; Martin, J.; Braithwaite, A.; et al. Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science 2003, 301, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Stewart, R.; Bae, K.Y.; Kim, S.W.; Kang, H.J.; Shin, I.S.; Kim, J.T.; Park, M.S.; Kim, M.K.; Park, S.W.; et al. Serotonergic and BDNF genes and risk of depression after stroke. J. Affect. Disord. 2012, 136, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Kohen, R.; Cain, K.C.; Mitchell, P.H.; Becker, K.; Buzaitis, A.; Millard, S.P.; Navaja, G.P.; Teri, L.; Tirschwell, D.; Veith, R. Association of serotonin transporter gene polymorphisms with poststroke depression. Arch. Gen. Psychiatry 2008, 65, 1296–1302. [Google Scholar] [CrossRef] [Green Version]
- Choi-Kwon, S.; Han, K.; Choi, S.; Suh, M.; Kim, Y.J.; Song, H.; Cho, K.H.; Nah, H.W.; Kwon, S.U.; Kang, D.W.; et al. Poststroke depression and emotional incontinence: Factors related to acute and subacute stages. Neurology 2012, 78, 1130–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Szyf, M.; Benkelfat, C.; Provençal, N.; Turecki, G.; Caramaschi, D.; Côté, S.M.; Vitaro, F.; Tremblay, R.E.; Booij, L. Peripheral SLC6A4 DNA methylation is associated with in vivo measures of human brain serotonin synthesis and childhood physical aggression. PLoS ONE 2012, 7, e39501. [Google Scholar] [CrossRef] [Green Version]
- Ismaylova, E.; Di Sante, J.; Szyf, M.; Nemoda, Z.; Yu, W.J.; Pomares, F.B.; Turecki, G.; Gobbi, G.; Vitaro, F.; Tremblay, R.E.; et al. Serotonin transporter gene promoter methylation in peripheral cells in healthy adults: Neural correlates and tissue specificity. Eur. Neuropsychopharmacol. 2017, 27, 1032–1041. [Google Scholar] [CrossRef]
- Philibert, R.A.; Sandhu, H.; Hollenbeck, N.; Gunter, T.; Adams, W.; Madan, A. Rapid publication: The relationship of 5HTT (SLC6A4) methylation and genotype on mRNA expression and liability to major depression and alcohol dependence in subjects from the Iowa adoption studies. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2008, 147, 543–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.T.J.M.; Stewart, R.; Kang, H.J.; Kim, S.W.; Shin, I.S.; Kim, H.R.; Shin, M.G.; Kim, J.T.J.M.; Park, M.S.; Cho, K.H.; et al. A longitudinal study of SLC6A4 DNA promoter methylation and poststroke depression. J. Psychiatr. Res. 2013, 47, 1222–1227. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.G.; Jorge, R.E. Post-stroke depression: A review. Am. J. Psychiatry 2016, 173, 221–231. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Leys, D.; Esquenazi, A. The interaction between neuropsychological and motor deficits in patients after stroke. Neurology 2013, 80, S27–S34. [Google Scholar] [CrossRef]
- Van Ijzendoorn, M.H.; Caspers, K.; Bakermans-Kranenburg, M.J.; Beach, S.R.H.; Philibert, R. Methylation matters: Interaction between methylation density and serotonin transporter genotype predicts unresolved loss or trauma. Biol. Psychiatry 2010, 68, 405–407. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Steer, R.A.; Carbin, M.G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Li, L.C.; Dahiya, R. MethPrimer: Designing primers for methylation PCRs. Bioinformatics 2002, 18, 1427–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uyttenboogaart, M.; Stewart, R.E.; Vroomen, P.C.A.J.; De Keyser, J.; Luijckx, G.J. Optimizing cutoff scores for the Barthel Index and the modified Rankin Scale for defining outcome in acute stroke trials. Stroke 2005, 36, 1984–1987. [Google Scholar] [CrossRef] [Green Version]
- Lindgren, A. Stroke Genetics: A Review and Update. J. Stroke 2014, 16, 114. [Google Scholar] [CrossRef]
- Philibert, R.; Madan, A.; Andersen, A.; Cadoret, R.; Packer, H.; Sandhu, H. Serotonin transporter mRNA levels are associated with the methylation of an upstream CpG island. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2007, 144, 101–105. [Google Scholar] [CrossRef]
- Anguelova, M.; Benkelfat, C.; Turecki, G. A systematic review of association studies investigating genes coding for serotonin receptors and the serotonin transporter: I. Affective disorders. Mol. Psychiatry 2003, 8, 574–591. [Google Scholar] [CrossRef] [Green Version]
- Kobiella, A.; Reimold, M.; Ulshöfer, D.E.; Ikonomidou, V.N.; Vollmert, C.; Vollstädt-Klein, S.; Rietschel, M.; Reischl, G.; Heinz, A.; Smolka, M.N. How the serotonin transporter 5-HTTLPR polymorphism influences amygdala function: The roles of in vivo serotonin transporter expression and amygdala structure. Transl. Psychiatry 2011, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahar, I.; Bambico, F.R.; Mechawar, N.; Nobrega, J.N. Stress, serotonin, and hippocampal neurogenesis in relation to depression and antidepressant effects. Neurosci. Biobehav. Rev. 2014, 38, 173–192. [Google Scholar] [CrossRef]
- Gould, E. Serotonin and hippocampal neurogenesis. Neuropsychopharmacology 1999, 21, 46S–51S. [Google Scholar] [CrossRef]
- Tang, M.; He, T.; Sun, X.; Meng, Q.Y.; Diao, Y.; Lei, J.Y.; He, X.J.; Chen, L.; Sang, X.B.; Zhao, S. Subregion-specific decreases in hippocampal serotonin transporter protein expression and function associated with endophenotypes of depression. Hippocampus 2014, 24, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Frodl, T.; Carballedo, A.; Hughes, M.M.; Saleh, K.; Fagan, A.; Skokauskas, N.; McLoughlin, D.M.; Meaney, J.; O’Keane, V.; Connor, T.J. Reduced expression of glucocorticoid-inducible genes GILZ and SGK-1: High IL-6 levels are associated with reduced hippocampal volumes in major depressive disorder. Transl. Psychiatry 2012, 2, e88. [Google Scholar] [CrossRef] [Green Version]
- Fassbender, K.; Schmidt, R.; Mößner, R.; Daffertshofer, M.; Hennerici, M. Pattern of activation of the hypothalamic-pituitary-adrenal axis in acute stroke: Relation to acute confusional state, extent of brain damage, and clinical outcome. Stroke 1994, 25, 1105–1108. [Google Scholar] [CrossRef] [Green Version]
- Olsson, T.; Marklund, N.; Gustafson, Y.; Nasman, B. Abnormalities at different levels of the hypothalamic-pituitary-adrenocortical axis early after stroke. Stroke 1992, 23, 1573–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neidert, S.; Katan, M.; Schuetz, P.; Fluri, F.; Ernst, A.; Bingisser, R.; Kappos, L.; Engelter, S.T.; Steck, A.; Müller, B.; et al. Anterior pituitary axis hormones and outcome in acute ischaemic stroke. J. Intern. Med. 2011, 269, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Iurescia, S.; Seripa, D.; Rinaldi, M. Role of the 5-HTTLPR and SNP Promoter Polymorphisms on Serotonin Transporter Gene Expression: A Closer Look at Genetic Architecture and In Vitro Functional Studies of Common and Uncommon Allelic Variants. Mol. Neurobiol. 2016, 53, 5510–5526. [Google Scholar] [CrossRef]
- Hu, X.Z.; Lipsky, R.H.; Zhu, G.; Akhtar, L.A.; Taubman, J.; Greenberg, B.D.; Xu, K.; Arnold, P.D.; Richter, M.A.; Kennedy, J.L.; et al. Serotonin transporter promoter gain-of-function genotypes are linked to obsessive-compulsive disorder. Am. J. Hum. Genet. 2006, 78, 815–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendland, J.R.; Moya, P.R.; Kruse, M.R.; Ren-Patterson, R.F.; Jensen, C.L.; Timpano, K.R.; Murphy, D.L. A novel, putative gain-of-function haplotype at SLC6A4 associates with obsessive-compulsive disorder. Hum. Mol. Genet. 2008, 17, 717–723. [Google Scholar] [CrossRef] [Green Version]


| CpG_n1 Sites | Patients with Unfavorable Outcome Mean (SD) | Patients with Favorable Outcome Mean (SD) | p |
|---|---|---|---|
| CpG1 (T0) | 8.5 (6.4) | 7.6 (4.1) | 0.974 |
| CpG2 (T0) | 13.7 (10.7) | 10.5 (6.7) | 0.509 |
| CpG3 (T0) | 21.6 (13.0) | 15.4 (7.5) | 0.124 |
| CpG4 (T0) | 14.5 (8.9) | 11.1 (5.6) | 0.346 |
| CpG5 (T0) | 21.5 (12.5) | 16.1 (4.9) | 0.243 |
| CpG1 (T1) | 9.9 (4.2) | 12.9 (5.1) | 0.049 |
| CpG2 (T1) | 15.7 (6.8) | 15.9 (7.4) | 0.751 |
| CpG3 (T1) | 21.5 (11.0) | 24.3 (13.2) | 0.537 |
| CpG4 (T1) | 15.3 (6.7) | 18.0 (7.0) | 0.320 |
| CpG5 (T1) | 22.1 (7.1) | 26.3 (7.6) | 0.168 |
| Δ CpG1 | 1.4 (8.6) | 5.4 (5.7) | 0.339 |
| Δ CpG2 | 2.6 (11.3) | 5.6 (11.3) | 0.641 |
| Δ CpG3 | 0.6 (17.8) | 8.3 (12.2) | 0.236 |
| Δ CpG4 | 0.7 (9.6) | 8.6 (6.1) | 0.024 |
| Δ CpG5 | −0.5 (13.0) | 11.4 (7.5) | 0.009 |
| CpG_n2 Sites | Patients with Unfavorable Outcome Mean (SD) | Patients with Favorable Outcome Mean (SD) | p |
|---|---|---|---|
| CpG1 (T0) | 9.2 (1.7) | 9.0 (1.8) | 0.598 |
| CpG2 (T0) | 5.8 (1.3) | 5.3 (1.0) | 0.101 |
| CpG3 (T0) | 5.5 (1.5) | 5.4 (1.6) | 0.851 |
| CpG5 (T0) | 2.4 (1.0) | 2.4 (1.3) | 0.441 |
| CpG9 (T0) | 2.8 (.9) | 2.3 (1.1) | 0.097 |
| CpG1 (T1) | 6.9 (1.6) | 5.0 (1.2) | 0.004 |
| CpG2 (T1) | 4.9 (1.0) | 3.6 (0.7) | 0.004 |
| CpG3 (T1) | 3.4 (0.8) | 2.9 (0.6) | 0.135 |
| CpG5 (T1) | 1.9 (1.3) | 0.8 (0.7) | 0.027 |
| CpG9 (T1) | 3.8 (1.1) | 4.1 (1.2) | 0.320 |
| Δ CpG1 | −2.1 (2.0) | −3.0 (1.8) | 0.193 |
| Δ CpG2 | −1.1 (1.4) | −1.9 (1.1) | 0.070 |
| Δ CpG3 | −2.0 (1.9) | −1.9 (1.5) | 0.867 |
| Δ CpG5 | −0.9 (1.5) | −2.1 (1.2) | 0.107 |
| Δ CpG9 | 0.7 (1.1) | 1.5 (1.2) | 0.070 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santoro, M.; Siotto, M.; Germanotta, M.; Mastrorosa, A.; Papadopoulou, D.; Aprile, I. Association Study of SLC6A4 (5-HTTLPR) Polymorphism and Its Promoter Methylation with Rehabilitation Outcome in Patients with Subacute Stroke. Genes 2021, 12, 579. https://doi.org/10.3390/genes12040579
Santoro M, Siotto M, Germanotta M, Mastrorosa A, Papadopoulou D, Aprile I. Association Study of SLC6A4 (5-HTTLPR) Polymorphism and Its Promoter Methylation with Rehabilitation Outcome in Patients with Subacute Stroke. Genes. 2021; 12(4):579. https://doi.org/10.3390/genes12040579
Chicago/Turabian StyleSantoro, Massimo, Mariacristina Siotto, Marco Germanotta, Alessia Mastrorosa, Dionysia Papadopoulou, and Irene Aprile. 2021. "Association Study of SLC6A4 (5-HTTLPR) Polymorphism and Its Promoter Methylation with Rehabilitation Outcome in Patients with Subacute Stroke" Genes 12, no. 4: 579. https://doi.org/10.3390/genes12040579
APA StyleSantoro, M., Siotto, M., Germanotta, M., Mastrorosa, A., Papadopoulou, D., & Aprile, I. (2021). Association Study of SLC6A4 (5-HTTLPR) Polymorphism and Its Promoter Methylation with Rehabilitation Outcome in Patients with Subacute Stroke. Genes, 12(4), 579. https://doi.org/10.3390/genes12040579