
RANTES 59029A/G Polymorphisms Associated with Diabetic Compilations in Korean Patients with Type 2 Diabetes for over 15 Years


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Evaluation of Diabetic Complications
2.3. Genotyping of RANTES 59029A/G
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Diabetic Complications Relative to Patient BMI
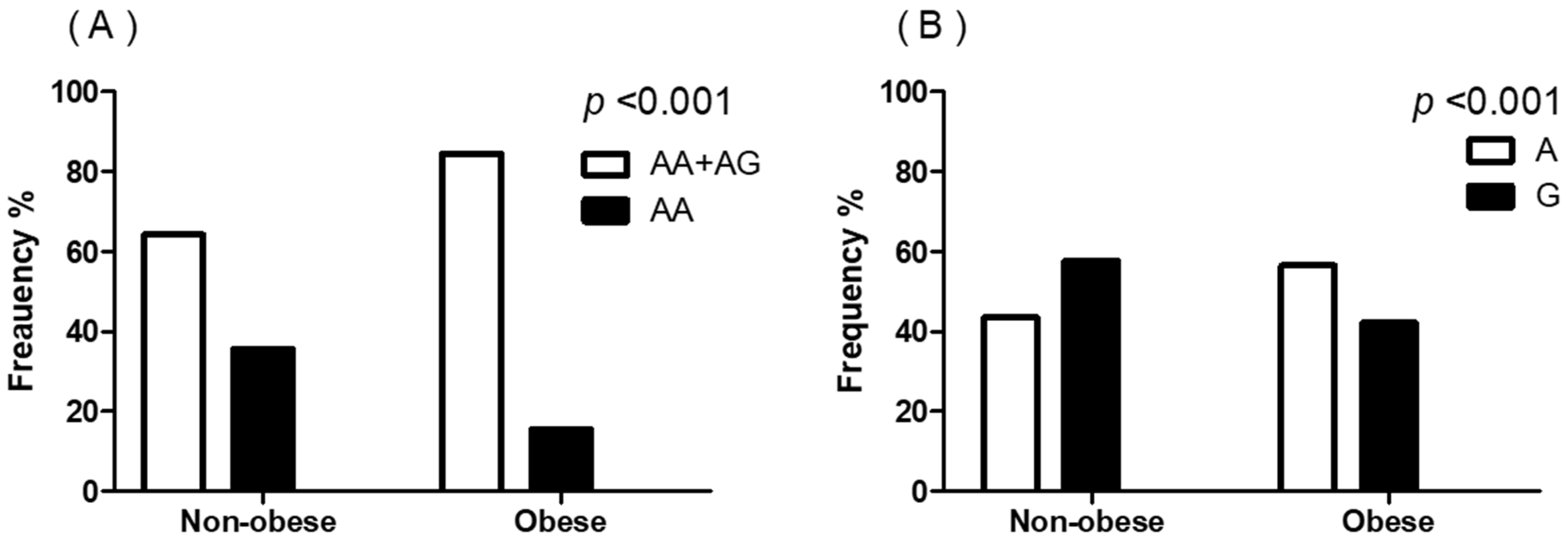
3.3. RANTES Genotype Relative to Patient BMI
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.H.; Ku, H.; Park, K.S. Prevalence and socioeconomic burden of diabetes mellitus in South Korean adults: A population-based study using administrative data. BMC Public Health 2021, 21, 548. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Jung, C.H.; Son, J.W.; Kang, S.; Kim, W.J.; Kim, H.S.; Kim, H.S.; Seo, M.; Shin, H.J.; Lee, S.S.; Jeong, S.J.; et al. Diabetes Fact Sheets in Korea, 2020: An Appraisal of Current Status. Diabetes Metab. J. 2021, 45, 1–10. [Google Scholar] [CrossRef]
- Barsh, G.S.; Farooqi, I.S.; O’Rahilly, S. Genetics of body-weight regulation. Nature 2000, 404, 644–651. [Google Scholar] [CrossRef]
- Yang, L.; Wu, L.; Fan, Y.; Ma, J. Vitamin D receptor gene polymorphisms in association with diabetic nephropathy: A systematic review and meta-analysis. BMC Med. Genet. 2017, 18, 95. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Ping, Y.; Wang, Y.; Zhang, Y. The roles of endothelial nitric oxide synthase gene polymorphisms in diabetes mellitus and its associated vascular complications: A systematic review and meta-analysis. Endocrine 2018, 62, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Niu, F.; Liu, D.; Sun, J.; Zhang, X.; Zhang, J.; Guo, S. Associations of TCF7L2 gene polymorphisms with the risk of diabetic nephropathy: A case-control study. Medicine 2018, 97, e8388. [Google Scholar] [CrossRef]
- Montesanto, A.; Bonfigli, A.R.; Crocco, P.; Garagnani, P.; De Luca, M.; Boemi, M.; Marasco, E.; Pirazzini, C.; Giuliani, C.; Franceschi, C.; et al. Genes associated with Type 2 Diabetes and vascular complications. Aging 2018, 10, 178–196. [Google Scholar] [CrossRef] [Green Version]
- Ferrante, A.W., Jr. Obesity-induced inflammation: A metabolic dialogue in the language of inflammation. J. Intern. Med. 2007, 262, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Neels, J.G.; Olefsky, J.M. Inflamed fat: What starts the fire? J. Clin. Investig. 2006, 116, 33–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appay, V.; Rowland-Jones, S.L. RANTES: A versatile and controversial chemokine. Trends Immunol. 2001, 22, 83–87. [Google Scholar] [CrossRef]
- Wu, H.; Ghosh, S.; Perrard, X.D.; Feng, L.; Garcia, G.E.; Perrard, J.L.; Sweeney, J.F.; Peterson, L.E.; Chan, L.; Smith, C.W.; et al. T-cell accumulation and regulated on activation, normal T cell expressed and secreted upregulation in adipose tissue in obesity. Circulation 2007, 115, 1029–1038. [Google Scholar] [CrossRef] [Green Version]
- Herder, C.; Illig, T.; Baumert, J.; Muller, M.; Klopp, N.; Khuseyinova, N.; Meisinger, C.; Poschen, U.; Martin, S.; Koenig, W.; et al. RANTES/CCL5 gene polymorphisms, serum concentrations, and incident type 2 diabetes: Results from the MONICA/KORA Augsburg case-cohort study, 1984–2002. Eur. J. Endocrinol. 2008, 158, R1. [Google Scholar] [CrossRef] [PubMed]
- Ueba, T.; Nomura, S.; Inami, N.; Yokoi, T.; Inoue, T. Elevated RANTES level is associated with metabolic syndrome and correlated with activated platelets associated markers in healthy younger men. Clin. Appl. Thromb. Hemost. 2014, 20, 813–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ting, K.H.; Ueng, K.C.; Chiang, W.L.; Chou, Y.E.; Yang, S.F.; Wang, P.H. Relationship of Genetic Polymorphisms of the Chemokine, CCL5, and Its Receptor, CCR5, with Coronary Artery Disease in Taiwan. Evid. Based Complement. Altern. Med. 2015, 2015, 851683. [Google Scholar] [CrossRef] [Green Version]
- Mokubo, A.; Tanaka, Y.; Nakajima, K.; Watada, H.; Hirose, T.; Kawasumi, M.; Sakai, K.; Kanazawa, A.; Maeda, S.; Hosokawa, K.; et al. Chemotactic cytokine receptor 5 (CCR5) gene promoter polymorphism (59029A/G) is associated with diabetic nephropathy in Japanese patients with type 2 diabetes: A 10-year longitudinal study. Diabetes Res. Clin. Pract. 2006, 73, 89–94. [Google Scholar] [CrossRef]
- Pan, W.H.; Yeh, W.T. How to define obesity? Evidence-based multiple action points for public awareness, screening, and treatment: An extension of Asian-Pacific recommendations. Asia Pac. J. Clin. Nutr. 2008, 17, 370–374. [Google Scholar] [PubMed]
- Baggiolini, M. Chemokines and leukocyte traffic. Nature 1998, 392, 565–568. [Google Scholar] [CrossRef]
- Mause, S.F.; von Hundelshausen, P.; Zernecke, A.; Koenen, R.R.; Weber, C. Platelet microparticles: A transcellular delivery system for RANTES promoting monocyte recruitment on endothelium. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1512–1518. [Google Scholar] [CrossRef] [Green Version]
- Tang, C.H.; Hsu, C.J.; Fong, Y.C. The CCL5/CCR5 axis promotes interleukin-6 production in human synovial fibroblasts. Arthritis Rheum. 2010, 62, 3615–3624. [Google Scholar] [CrossRef]
- Schwabe, R.F.; Bataller, R.; Brenner, D.A. Human hepatic stellate cells express CCR5 and RANTES to induce proliferation and migration. Am. J. Physiol. Gastrointest. Liver Physiol. 2003, 285, G949–G958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.G.; Huang, J.; Zhang, J.; Li, X.B.; He, C.; Xiao, Y.L.; Tian, C.; Wan, H.; Zhao, Y.L.; Tsewang, Y.G.; et al. RANTES gene polymorphisms and asthma risk: A meta-analysis. Arch. Med. Res. 2010, 41, 50–58. [Google Scholar] [CrossRef]
- Madani, R.; Karastergiou, K.; Ogston, N.C.; Miheisi, N.; Bhome, R.; Haloob, N.; Tan, G.D.; Karpe, F.; Malone-Lee, J.; Hashemi, M.; et al. RANTES release by human adipose tissue in vivo and evidence for depot-specific differences. Am. J. Physiol. Endocrinol. Metab. 2009, 296, E1262–E1268. [Google Scholar] [CrossRef]
- Borel, J.C.; Roux-Lombard, P.; Tamisier, R.; Arnaud, C.; Monneret, D.; Arnol, N.; Baguet, J.P.; Levy, P.; Pepin, J.L. Endothelial dysfunction and specific inflammation in obesity hypoventilation syndrome. PLoS ONE 2009, 4, e6733. [Google Scholar] [CrossRef] [Green Version]
- Baturcam, E.; Abubaker, J.; Tiss, A.; Abu-Farha, M.; Khadir, A.; Al-Ghimlas, F.; Al-Khairi, I.; Cherian, P.; Elkum, N.; Hammad, M.; et al. Physical exercise reduces the expression of RANTES and its CCR5 receptor in the adipose tissue of obese humans. Mediat. Inflamm. 2014, 2014, 627150. [Google Scholar] [CrossRef] [PubMed]
- Xue, W.; Fan, Z.; Li, L.; Lu, J.; Zhai, Y.; Zhao, J. The chemokine system and its role in obesity. J. Cell. Physiol. 2019, 234, 3336–3346. [Google Scholar] [CrossRef] [PubMed]
- Keshavarzi, F.; Golsheh, S. IRS1-rs10498210 G/A and CCR5-59029 A/G polymorphisms in patients with type 2 diabetes in Kurdistan. Mol. Genet. Genom. Med. 2019, 7, e631. [Google Scholar] [CrossRef]
- Kochetova, O.V.; Avzaletdinova, D.S.; Morugova, T.V.; Mustafina, O.E. Chemokine gene polymorphisms association with increased risk of type 2 diabetes mellitus in Tatar ethnic group, Russia. Mol. Biol. Rep. 2019, 46, 887–896. [Google Scholar] [CrossRef]
- Simeoni, E.; Winkelmann, B.R.; Hoffmann, M.M.; Fleury, S.; Ruiz, J.; Kappenberger, L.; Marz, W.; Vassalli, G. Association of RANTES G-403A gene polymorphism with increased risk of coronary arteriosclerosis. Eur. Heart J. 2004, 25, 1438–1446. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Jia, Y.J.; Li, X.L.; Xu, R.X.; Zhu, C.G.; Guo, Y.L.; Wu, N.Q.; Li, J.J. RANTES gene G-403A polymorphism and coronary artery disease: A meta analysis of observational studies. PLoS ONE 2012, 7, e47211. [Google Scholar] [CrossRef]
- Nakajima, K.; Tanaka, Y.; Nomiyama, T.; Ogihara, T.; Ikeda, F.; Kanno, R.; Iwashita, N.; Sakai, K.; Watada, H.; Onuma, T.; et al. RANTES promoter genotype is associated with diabetic nephropathy in type 2 diabetic subjects. Diabetes Care 2003, 26, 892–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Non-Obese (n = 168) | Obese (n = 103) | p-Value | |
|---|---|---|---|
| Age (years) | 59.2 ± 10.6 | 62.1 ± 9.3 | 0.025 |
| Sex (F/M) | 74/94 | 66/37 | 0.001 |
| Duration of DM (years) | 24.4 ± 5.0 | 25.4 ± 6.1 | 0.163 |
| BMI (kg/m2) | 22.2 ± 2.3 | 26.7 ± 1.8 | 0.001 |
| SBP (mmHg) | 138.9 ± 16.6 | 137.8 ± 15.1 | 0.611 |
| DBP (mmHg) | 85.8 ± 10.8 | 86.0 ± 9.6 | 0.882 |
| FPG (mg/dl) | 146.2 ± 55.5 | 137.0 ± 45.5 | 0.215 |
| PP2 (mg/dl) | 248.3 ± 96.7 | 225.1 ± 89.2 | 0.093 |
| HbA1c (%) | 7.8 ± 1.6 | 7.7 ± 1.7 | 0.744 |
| C-peptide (ng/mL) | 4.20 ± 1.78 | 3.04 ± 1.83 | 0.618 |
| Total cholesterol (mg/dL) | 179.4 ± 46.0 | 189.9 ± 55.5 | 0.145 |
| Triglycerides (mg/dL) | 153.9 ± 81.5 | 191.2 ± 99.1 | 0.056 |
| HDL-cholesterol (mg/dL) | 44.7 ± 10.9 | 44.7 ± 12.0 | 0.996 |
| LDL-cholesterol (mg/dL) | 103.8 ± 32.6 | 108.7 ± 43.7 | 0.384 |
| AST (IU/L) | 38.2 ± 10.4 | 39.1 ± 15.4 | 0.901 |
| ALT (IU/L) | 39.2 ± 11.4 | 38.2 ± 11.4 | 0.801 |
| BUN (mg/dL) | 25.4 ± 21.3 | 26.3 ± 19.9 | 0.302 |
| Creatinine (mg/dL) | 2.32 ± 2.85 | 2.41 ± 2.68 | 0.803 |
| Complications, N (%) | Non-Obese (n = 168) | Obese (n = 103) | p-Value |
|---|---|---|---|
| Microvascular complications | 121 (72.0) | 86 (83.5) | 0.039 |
| Retinopathy | 94 (75.6) | 70 (79.6) | 0.207 |
| Nephropathy | 45 (50.3) | 58 (56.3) | 0.320 |
| Macrovascular complications | 65 (38.7) | 41 (39.8) | 0.898 |
| Coronary artery disease | 48 (58.6) | 33 (32.1) | 0.682 |
| Cerebrovascular disease | 27 (16.7) | 16 (15.5) | 0.988 |
| Variables, N (%) | Non-Obese (n = 168) | Obese (n = 103) | p-Value |
|---|---|---|---|
| Genotype | 0.001 | ||
| AA + AG | 108 (64.3) | 87 (84.5) | |
| GG | 60 (35.7) | 16 (15.5) | |
| Allele | 0.001 | ||
| A | 146 (43.5) | 119 (57.8) | |
| G | 190 (56.5) | 87 (42.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.-H.; Ku, E.-J.; Oh, T.-K.; Jeon, H.-J. RANTES 59029A/G Polymorphisms Associated with Diabetic Compilations in Korean Patients with Type 2 Diabetes for over 15 Years. Genes 2021, 12, 1445. https://doi.org/10.3390/genes12091445
Lee D-H, Ku E-J, Oh T-K, Jeon H-J. RANTES 59029A/G Polymorphisms Associated with Diabetic Compilations in Korean Patients with Type 2 Diabetes for over 15 Years. Genes. 2021; 12(9):1445. https://doi.org/10.3390/genes12091445
Chicago/Turabian StyleLee, Dong-Hwa, Eu-Jeong Ku, Tae-Keun Oh, and Hyun-Jeong Jeon. 2021. "RANTES 59029A/G Polymorphisms Associated with Diabetic Compilations in Korean Patients with Type 2 Diabetes for over 15 Years" Genes 12, no. 9: 1445. https://doi.org/10.3390/genes12091445
APA StyleLee, D. -H., Ku, E. -J., Oh, T. -K., & Jeon, H. -J. (2021). RANTES 59029A/G Polymorphisms Associated with Diabetic Compilations in Korean Patients with Type 2 Diabetes for over 15 Years. Genes, 12(9), 1445. https://doi.org/10.3390/genes12091445