
Old and New Systemic Immune-Inflammation Indexes Are Associated with Overall Survival of Glioblastoma Patients Treated with Radio-Chemotherapy

 ,
,  , , , ,
, , , ,  ,
,  ,
,  ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Patients and Systemic Inflammation Indexes
- PLR = P/L
- PW/L = P × W/L
- SII = N × P/L
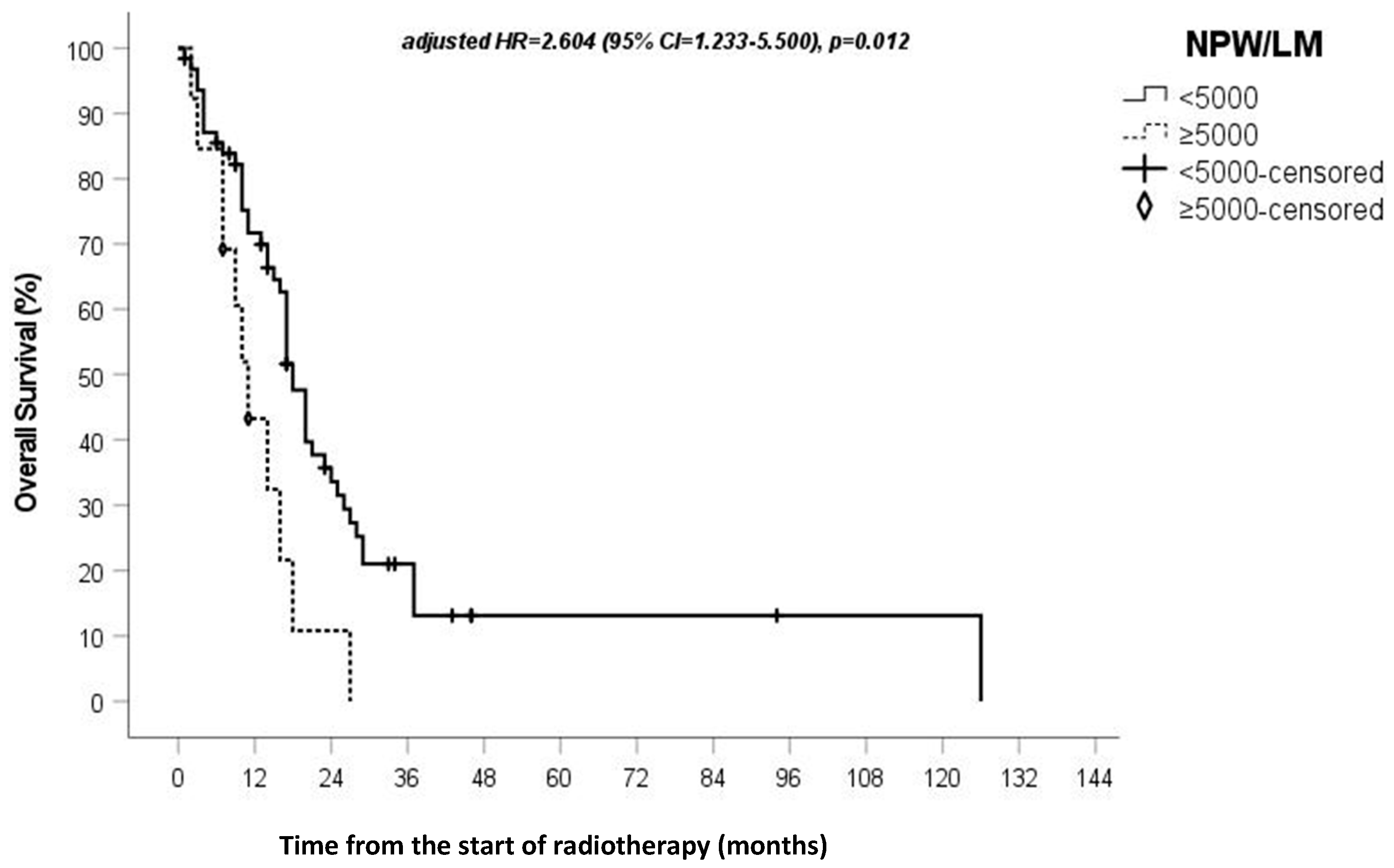
- NPW/L = N × P × W/L
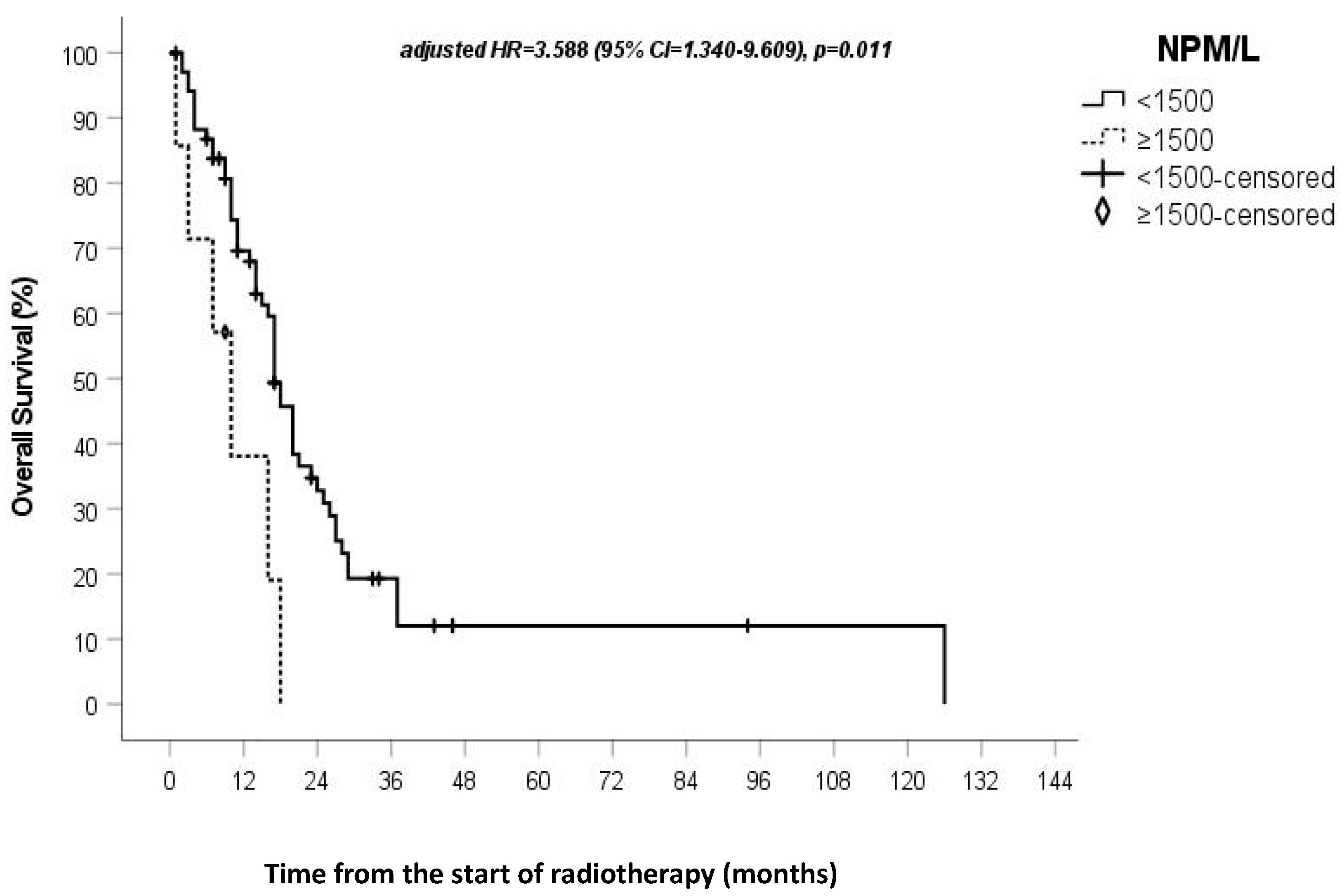
- NPM/L = N × P × M/L
- NPMW/L = N × P × M × W/L
- NPM/LW = N × P × M/(L × W)
- NP/LM = N × P/(L × M)
- NP/(L + M) = N × P/(L + M)
- NPW/LM = N × P × W/(L × M)
- NP/WLM = N × P/(W × (L + M))
- NPW/(L + M) = N × P × W/(L + M)
4. Statistical Analysis
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stupp, R.; Mason, W.P.; Van Den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef]
- Wen, P.Y.; Weller, M.; Lee, E.Q.; Alexander, B.M.; Barnholtz-Sloan, J.S.; Barthel, F.P.; Batchelor, T.T.; Bindra, R.S.; Chang, S.M.; Chiocca, E.A.; et al. Glioblastoma in adults: A Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) consensus review on current management and future directions. Neuro-Oncology 2020, 22, 1073–1113. [Google Scholar] [CrossRef] [PubMed]
- Piccirillo, S.G.M.; Alonso, M.M.; Pasqualetti, F. Basic and Translational Advances in Glioblastoma. BioMed Res. Int. 2018, 2018, 1820345. [Google Scholar] [CrossRef] [PubMed]
- Pasqualetti, F.; Orlandi, P.; Simeon, V.; Cantarella, M.; Giuliani, D.; Di Desidero, T.; Gonnelli, A.; Delishaj, D.; Lombardi, G.; Sechi, A.; et al. Melanocortin Receptor-4 Gene Polymorphisms in Glioblastoma Patients Treated with Concomitant Radio-Chemotherapy. Mol. Neurobiol. 2017, 55, 1396–1404. [Google Scholar] [CrossRef]
- Wesseling, P.; Capper, D.W.H.O. WHO 2016 Classification of gliomas. Neuropathol. Appl. Neurobiol. 2018, 44, 139–150. [Google Scholar] [CrossRef]
- Fanelli, G.; Grassini, D.; Ortenzi, V.; Pasqualetti, F.; Montemurro, N.; Perrini, P.; Naccarato, A.; Scatena, C. Decipher the Glioblastoma Microenvironment: The First Milestone for New Groundbreaking Therapeutic Strategies. Genes 2021, 12, 445. [Google Scholar] [CrossRef]
- Montemurro, N.; Fanelli, G.N.; Scatena, C.; Ortenzi, V.; Pasqualetti, F.; Mazzanti, C.M.; Morganti, R.; Paiar, F.; Naccarato, A.G.; Perrini, P. Surgical outcome and molecular pattern characterization of recurrent glioblastoma multiforme: A single-center retrospective series. Clin. Neurol. Neurosurg. 2021, 207, 106735. [Google Scholar] [CrossRef]
- Yan, Q.; Ertao, Z.; Zhimei, Z.; Weigang, D.; Jianjun, P.; Jianhui, C.; Chuangqi, C. Systemic immune-inflammation index (SII): A More Promising Inflammation-Based Prognostic Marker for Patients with synchronic colorectal peritoneal carcinomatosis. J. Cancer 2020, 11, 5264–5272. [Google Scholar] [CrossRef]
- Wang, D.; Kang, K.; Lin, Q.; Hai, J. Prognostic Significance of Preoperative Systemic Cellular Inflammatory Markers in Gliomas: A Systematic Review and Meta-Analysis. Clin. Transl. Sci. 2019, 13, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Hiam-Galvez, K.J.; Allen, B.M.; Spitzer, M.H. Systemic immunity in cancer. Nat. Cancer 2021, 21, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Liu, Y.; Li, Q.; Li, Z.; Hou, H.; Wu, A. Pre-treatment neutrophil-to-lymphocyte ratio is associated with neutrophil and T-cell infiltration and predicts clinical outcome in patients with glioblastoma. BMC Cancer 2015, 15, 617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clavreul, A.; Lemée, J.-M.; Soulard, G.; Rousseau, A.; Menei, P. A Simple Preoperative Blood Count to Stratify Prognosis in Isocitrate Dehydrogenase-Wildtype Glioblastoma Patients Treated with Radiotherapy plus Concomitant and Adjuvant Temozolomide. Cancers 2021, 13, 5778. [Google Scholar] [CrossRef]
- Topkan, E.; Besen, A.A.; Ozdemir, Y.; Küçük, A.; Mertsoylu, H.; Pehlivan, B.; Selek, U. Prognostic Value of Pretreatment Systemic Immune-Inflammation Index in Glioblastoma Multiforme Patients Undergoing Postneurosurgical Radiotherapy Plus Concurrent and Adjuvant Temozolomide. Mediat. Inflamm. 2020, 2020, 4392189. [Google Scholar] [CrossRef]
- Wang, Q.; Tan, X.; Deng, G.; Fu, S.; Li, J.; Li, Z. Dynamic changes in the systemic immune-inflammation index predict the prognosis of EGFR-mutant lung adenocarcinoma patients receiving brain metastasis radiotherapy. BMC Pulm. Med. 2022, 22, 75. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Z.; Jin, F.; Guo, D.; Chen, Q.; Liu, Z.; Ji, S.; Gao, G. The Value of the Systemic Immune-Inflammation Index in Predicting Survival Outcomes in Patients with Brain Metastases of Non-Small-Cell Lung Cancer Treated with Stereotactic Radiotherapy. Mediat. Inflamm. 2021, 2021, 2910892. [Google Scholar] [CrossRef] [PubMed]
- Perrini, P.; Gambacciani, C.; Weiss, A.; Pasqualetti, F.; Delishaj, D.; Paiar, F.; Morganti, R.; Vannozzi, R.; Lutzemberger, L. Survival outcomes following repeat surgery for recurrent glioblastoma: A single-center retrospective analysis. J. Neuro-Oncol. 2016, 131, 585–591. [Google Scholar] [CrossRef]
- Pasqualetti, F.; Gonnelli, A.; Molinari, A.; Cantarella, M.; Montrone, S.; Cristaudo, A.; Baldaccini, D.; Mattioni, R.; Delishaj, D.; Mazzotti, V.; et al. Different Timing to Use Bevacizumab in Patients with Recurrent Glioblastoma: Early Versus Delayed Administration. Anticancer Res. 2018, 38, 5877–5881. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; DeGroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.J.; Afshar-Kharghan, V.; Schafer, A.I. Paraneoplastic thrombocytosis: The secrets of tumor self-promotion. Blood 2014, 124, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Karpatkin, S.; Pearlstein, E. Role of Platelets in Tumor Cell Metastases. Ann. Intern. Med. 1981, 95, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Nolte, I.; Przibylla, H.; Bostel, T.; Groden, C.; Brockmann, M.A. Tumor–platelet interactions: Glioblastoma growth is accompanied by increasing platelet counts. Clin. Neurol. Neurosurg. 2008, 110, 339–342. [Google Scholar] [CrossRef]
- Yu, D.; Liu, B.; Zhang, L.; Du, K. Platelet count predicts prognosis in operable non-small cell lung cancer. Exp. Ther. Med. 2013, 5, 1351–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.S.; Suh, K.W.; Oh, S.Y. Preoperative thrombocytosis predicts prognosis in stage II colorectal cancer patients. Ann. Surg. Treat. Res. 2016, 90, 322–327. [Google Scholar] [CrossRef] [Green Version]
- Marini, A.; Dobran, M.; Aiudi, D.; Pesaresi, A.; di Somma, L.G.M.; Iacoangeli, M. Pre-operative hematological markers as predictive factors for overall survival and progression free survival in glioblastomas. Clin. Neurol. Neurosurg. 2020, 197, 106162. [Google Scholar] [CrossRef]
- Uribe-Querol, E.; Rosales, C. Neutrophils in Cancer: Two Sides of the Same Coin. J. Immunol. Res. 2015, 2015, 983698. [Google Scholar] [CrossRef] [Green Version]
- Powell, D.R.; Huttenlocher, A. Neutrophils in the Tumor Microenvironment. Trends Immunol. 2015, 37, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Liang, J.; Piao, Y.; Holmes, L.; Fuller, G.; Henry, V.; Tiao, N.; De Groot, J.F. Neutrophils Promote the Malignant Glioma Phenotype through S100A4. Clin. Cancer Res. 2013, 20, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Rahbar, A.; Cederarv, M.; Wolmer-Solberg, N.; Tammik, C.; Stragliotto, G.; Peredo, I.; Fornara, O.; Xu, X.; Dzabic, M.; Taher, C.; et al. Enhanced neutrophil activity is associated with shorter time to tumor progression in glioblastoma patients. OncoImmunology 2015, 5, e1075693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Mittal, S.; McGee, K.; Alfaro-Munoz, K.D.; Majd, N.; Balasubramaniyan, V.; de Groot, J.F. Role of Neutrophils and Myeloid-Derived Suppressor Cells in Glioma Progression and Treatment Resistance. Int. J. Mol. Sci. 2020, 21, 1954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolás-Ávila, J.Á.; Adrover, J.M.; Hidalgo, A. Neutrophils in Homeostasis, Immunity, and Cancer. Immunity 2017, 46, 15–28. [Google Scholar] [CrossRef] [Green Version]
- Sippel, T.R.; White, J.; Nag, K.; Tsvankin, V.; Klaassen, M.; Kleinschmidt-DeMasters, B.; Waziri, A. Neutrophil Degranulation and Immunosuppression in Patients with GBM: Restoration of Cellular Immune Function by Targeting Arginase I. Clin. Cancer Res. 2011, 17, 6992–7002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Song, H.-W.; Cai, H.-Q.; Kong, L.-W.; Yao, K.; Jiang, T.; Li, S.; Yan, C.-X. Preoperative inflammation markers and IDH mutation status predict glioblastoma patient survival. Oncotarget 2017, 8, 50117–50123. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Feature | Number |
|---|---|
| Gender M/F | 43/34 |
| Median age (years) | 64 (range 26–84) |
| Second surgery | 20 (24.3%) |
| Median KPS | 80 |
| Extent of Surgery: Gross Tumor Removal: 31 (40.2%) Partial Tumor Removal: 46 (59.8%) | |
| MGMT meth. | 23/34 (67.6%) |
| Blood cells | Mean Value |
| White blood cells | 9.26 (3.55) |
| Red blood cells | 4.70 (0.50) |
| Hemoglobin | 13.9 (1.6) |
| Platelets | 246 (87) |
| Neutrophils | 6.75 (3.29) |
| Lymphocytes | 1.96 (1.39) |
| Monocytes | 0.608 (0.393) |
| Eosinophils | 0.073 (0.082) |
| Basophils | 0.016 (0.013) |
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| Factor | HR (95% CI) | p-Value | RC | HR (95% CI) | p-Value |
| PLR (0) ≤ 250 (1) > 250 | 2.402 (1.242–4.644) | 0.009 | 0.477 | ||
| PLRW (0) < 2500 (1) ≥ 2500 | 2.175 (0.965–4.903) | 0.061 | 0.363 | ||
| SII (0) < 1200 (1) ≥ 1200 | 1.848 (1.056–3.234) | 0.032 | 0.924 | ||
| NPW/L (0) < 7500 (1) ≥ 7500 | 1.773 (1.045–3.007) | 0.034 | 0.894 | ||
| NPM/L (0) < 1500 (1) ≥ 1500 | 2.983 (1.243–7.161) | 0.014 | 1.278 | 3.588 (1.340–9.609) | 0.011 |
| NPMW/L (0) < 8000 (1) ≥ 8000 | 3.271 (1.269–8.435) | 0.014 | 0.538 | ||
| NPM/LW (0) < 90 (1) ≥ 90 | 2.404 (1.148–5.033) | 0.020 | 0.941 | ||
| NP/LM (0) < 5000 (1) ≥ 5000 | 2.283 (1.179–4.420) | 0.014 | 0.748 | ||
| NP/(L + M) (0) < 1300 (1) ≥ 1300 | 2.263 (1.147–4.463) | 0.018 | 0.736 | ||
| NPW/LM (0) < 5000 (1) ≥ 5000 | 2.411 (1.218–4.771) | 0.012 | 0.957 | 2.604 (1.233–5.500) | 0.012 |
| NP/LMW (0) < 1000 (1) ≥ 1000 | 2.147 (1.036–4.450) | 0.040 | 0.996 | ||
| NPW/(L + M) (0) < 2500 (1) ≥ 2500 | 1.852 (0.930–3.689) | 0.080 | 0.860 | ||
| Surgery (0) GTR (1) STR | 2.235 (1.214–4.117) | 0.010 | 0.703 | 2.020 (1.081–3.775) | 0.028 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasqualetti, F.; Giampietro, C.; Montemurro, N.; Giannini, N.; Gadducci, G.; Orlandi, P.; Natali, E.; Chiarugi, P.; Gonnelli, A.; Cantarella, M.; et al. Old and New Systemic Immune-Inflammation Indexes Are Associated with Overall Survival of Glioblastoma Patients Treated with Radio-Chemotherapy. Genes 2022, 13, 1054. https://doi.org/10.3390/genes13061054
Pasqualetti F, Giampietro C, Montemurro N, Giannini N, Gadducci G, Orlandi P, Natali E, Chiarugi P, Gonnelli A, Cantarella M, et al. Old and New Systemic Immune-Inflammation Indexes Are Associated with Overall Survival of Glioblastoma Patients Treated with Radio-Chemotherapy. Genes. 2022; 13(6):1054. https://doi.org/10.3390/genes13061054
Chicago/Turabian StylePasqualetti, Francesco, Celeste Giampietro, Nicola Montemurro, Noemi Giannini, Giovanni Gadducci, Paola Orlandi, Eleonora Natali, Paolo Chiarugi, Alessandra Gonnelli, Martina Cantarella, and et al. 2022. "Old and New Systemic Immune-Inflammation Indexes Are Associated with Overall Survival of Glioblastoma Patients Treated with Radio-Chemotherapy" Genes 13, no. 6: 1054. https://doi.org/10.3390/genes13061054
APA StylePasqualetti, F., Giampietro, C., Montemurro, N., Giannini, N., Gadducci, G., Orlandi, P., Natali, E., Chiarugi, P., Gonnelli, A., Cantarella, M., Scatena, C., Fanelli, G. N., Naccarato, A. G., Perrini, P., Liberti, G., Morganti, R., Franzini, M., Paolicchi, A., Pellegrini, G., ... Paiar, F. (2022). Old and New Systemic Immune-Inflammation Indexes Are Associated with Overall Survival of Glioblastoma Patients Treated with Radio-Chemotherapy. Genes, 13(6), 1054. https://doi.org/10.3390/genes13061054