
Rectal Cancer in a Patient with Bartter Syndrome: A Case Report

Abstract
:1. Introduction
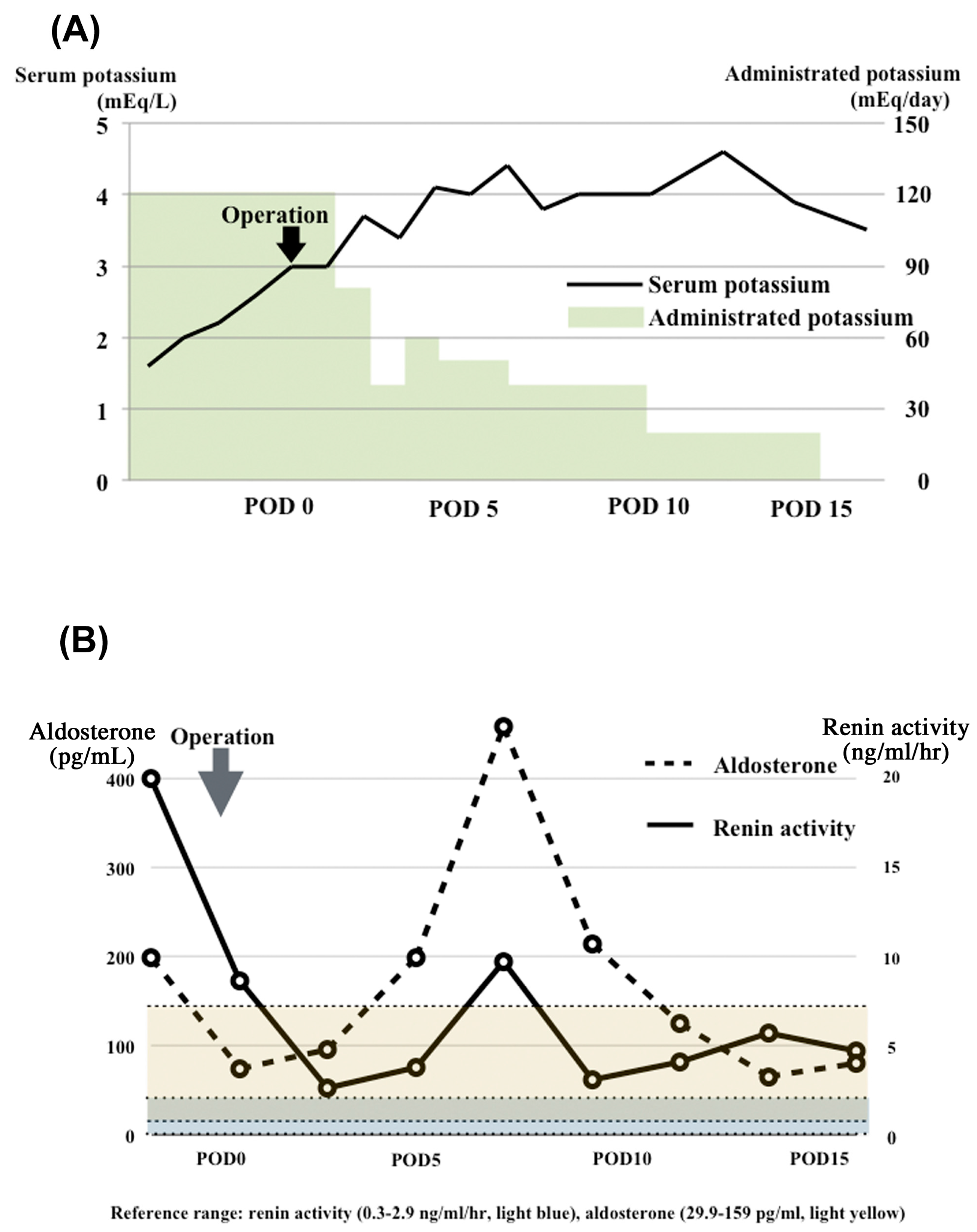
2. Case Report
3. Methods
3.1. Genetic Analyses Using a Next-Generation Sequencer
3.2. Immunohistochemical Study of PGE2
4. Results
4.1. Identification of Gene Mutations
4.2. Increased PGE2 Levels in the Tumor
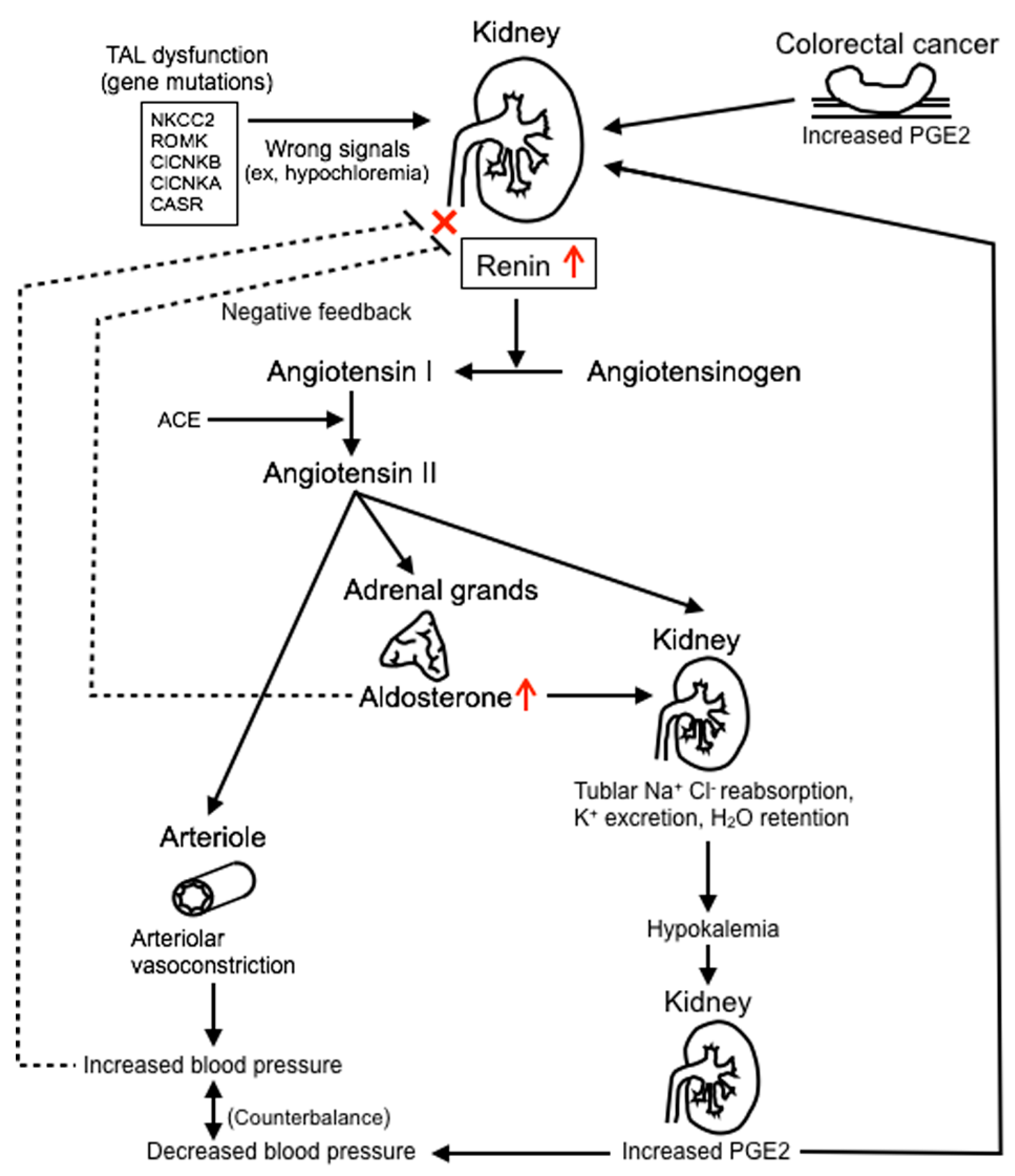
5. Discussion
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bartter, F.C.; Pronove, P.; Gill, J.R., Jr.; Maccardle, R.C. Hyperplasia of the juxtaglomerular complex with hyperaldosteronism and hypokalemic alkalosis. A new syndrome. Am. J. Med. 1962, 33, 811–828. [Google Scholar] [CrossRef]
- Rodriguez-Soriano, J. Bartter and related syndromes: The puzzle is almost solved. Pediatr. Nephrol. 1998, 12, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Proesmans, W. Bartter syndrome and its neonatal variant. Eur. J. Pediatr. 1997, 156, 669–679. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.B.; Karet, F.E.; Rodriguez-Soriano, J.; Hamdan, J.H.; DiPietro, A.; Trachtman, H.; Sanjad, S.A.; Lifton, R.P. Genetic heterogeneity of Bartter's syndrome revealed by mutations in the k+ channel, ROMK. Nat. Genet. 1996, 14, 152–156. [Google Scholar]
- Simon, D.B.; Bindra, R.S.; Mansfield, T.A.; Nelson-Williams, C.; Mendonca, E.; Stone, R.; Schurman, S.; Nayir, A.; Alpay, H.; Bakkaloglu, A.; et al. Mutations in the chloride channel gene, CLCNKB, cause Bartter's syndrome type III. Nat. Genet. 1997, 17, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Birkenhager, R.; Otto, E.; Schurmann, M.J.; Vollmer, M.; Ruf, E.M.; Maier-Lutz, I.; Beekmann, F.; Fekete, A.; Omran, H.; Feldmann, D.; et al. Mutation of BSND causes Bartter syndrome with sensorineural deafness and kidney failure. Nat. Genet. 2001, 29, 310–314. [Google Scholar] [CrossRef] [PubMed]
- Schlingmann, K.P.; Konrad, M.; Jeck, N.; Waldegger, P.; Reinalter, S.C.; Holder, M.; Seyberth, H.W.; Waldegger, S. Salt wasting and deafness resulting from mutations in two chloride channels. N. Engl. J. Med. 2004, 350, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Poussou, R.; Huang, C.; Hulin, P.; Houillier, P.; Jeunemaitre, X.; Paillard, M.; Planelles, G.; Dechaux, M.; Miller, R.T.; Antignac, C. Functional characterization of a calcium-sensing receptor mutation in severe autosomal dominant hypocalcemia with a Bartter-like syndrome. J. Am. Soc. Nephrol. 2002, 13, 2259–2266. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.B.; Nelson-Williams, C.; Bia, M.J.; Ellison, D.; Karet, F.E.; Molina, A.M.; Vaara, I.; Iwata, F.; Cushner, H.M.; Koolen, M.; et al. Gitelman’s variant of Bartter's syndrome, inherited hypokalaemic alkalosis, is caused by mutations in the thiazide-sensitive Na-Cl cotransporter. Nat. Genet. 1996, 12, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Konrad, M.; Vollmer, M.; Lemmink, H.H.; van den Heuvel, L.P.; Jeck, N.; Vargas-Poussou, R.; Lakings, A.; Ruf, R.; Deschenes, G.; Antignac, C.; et al. Mutations in the chloride channel gene CLCNKB as a cause of classic Bartter syndrome. J. Am. Soc. Nephrol. 2000, 11, 1449–1459. [Google Scholar] [PubMed]
- Choi, M.; Scholl, U.I.; Ji, W.; Liu, T.; Tikhonova, I.R.; Zumbo, P.; Nayir, A.; Bakkaloglu, A.; Ozen, S.; Sanjad, S.; et al. Genetic diagnosis by whole exome capture and massively parallel DNA sequencing. Proc. Natl. Acad. Sci. USA 2009, 106, 19096–19101. [Google Scholar] [CrossRef] [PubMed]
- Ishimori, S.; Kaito, H.; Matsunoshita, N.; Otsubo, H.; Hashimoto, F.; Ninchoji, T.; Nozu, K.; Morisada, N.; Iijima, K. SLC26A3 gene analysis in patients with Bartter and Gitelman syndromes and the clinical characteristics of patients with unidentified mutations. Kobe J. Med. Sci. 2013, 59, E36–E43. [Google Scholar] [PubMed]
- Simon, D.B.; Karet, F.E.; Hamdan, J.M.; DiPietro, A.; Sanjad, S.A.; Lifton, R.P. Bartter's syndrome, hypokalaemic alkalosis with hypercalciuria, is caused by mutations in the Na-K-2Cl cotransporter NKCC2. Nat. Genet. 1996, 13, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Dubois, R.N. Prostaglandins and cancer. Gut 2006, 55, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Tougeron, D.; Sha, D.; Manthravadi, S.; Sinicrope, F.A. Aspirin and colorectal cancer: Back to the future. Clin. Cancer Res. 2014, 20, 1087–1094. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Itabashi, M.; Shimada, Y.; Tanaka, S.; Ito, Y.; Ajioka, Y.; Hamaguchi, T.; Hyodo, I.; Igarashi, M.; Ishida, H.; et al. Japanese society for cancer of the colon and rectum (JSCCR) guidelines 2010 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 2012, 17, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Seyberth, H.W. An improved terminology and classification of Bartter-like syndromes. Nat. Clin. Pract. Nephrol. 2008, 4, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Urbanova, M.; Reiterova, J.; Stekrova, J.; Lnenicka, P.; Rysava, R. DNA analysis of renal electrolyte transporter genes among patients suffering from Bartter and Gitelman syndromes: Summary of mutation screening. Folia Biol. 2011, 57, 65–73. [Google Scholar]
- Zelikovic, I.; Szargel, R.; Hawash, A.; Labay, V.; Hatib, I.; Cohen, N.; Nakhoul, F. A novel mutation in the chloride channel gene, CLCNKB, as a cause of Gitelman and Bartter syndromes. Kidney Int. 2003, 63, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Udelsman, R.; Norton, J.A.; Jelenich, S.E.; Goldstein, D.S.; Linehan, W.M.; Loriaux, D.L.; Chrousos, G.P. Responses of the hypothalamic-pituitary-adrenal and renin-angiotensin axes and the sympathetic system during controlled surgical and anesthetic stress. J. Clin. Endocrinol. Metab. 1987, 64, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Rigas, B.; Goldman, I.S.; Levine, L. Altered eicosanoid levels in human colon cancer. J. Lab. Clin. Med. 1993, 122, 518–523. [Google Scholar] [PubMed]
- Young, A.L.; Chalmers, C.R.; Hawcroft, G.; Perry, S.L.; Treanor, D.; Toogood, G.J.; Jones, P.F.; Hull, M.A. Regional differences in prostaglandin e(2) metabolism in human colorectal cancer liver metastases. BMC Cancer 2013, 13, 92. [Google Scholar] [CrossRef] [PubMed]
- Narisawa, T.; Kusaka, H.; Yamazaki, Y.; Takahashi, M.; Koyama, H.; Koyama, K.; Fukaura, Y.; Wakizaka, A. Relationship between blood plasma prostaglandin e2 and liver and lung metastases in colorectal cancer. Dis. Colon Rectum 1990, 33, 840–845. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Transcript | Function | Codon | Exon | Coding |
|---|---|---|---|---|---|
| CLCNKB | NM_000085.4 | synonymous | TCG | 4 | c.324A>G |
| CLCNKB | NM_000085.4|NM_001165945.2 | synonymous | GGC | 5 | c.492G>C| |
| CLCNKB | NM_000085.4|NM_001165945.2 | missense | GTG | 2 | c.860C>T|c.353C>T |
| CLCNKB | NM_000085.4|NM_001165945.2 | synonymous | TGC | 3 | c.876T>C|c.369T>C |
| CLCNKB | NM_000085.4|NM_001165945.2 | missense | ACG | 9 | c.1685T>C|c.1178T>C |
| CLCNKB | NM_000085.4|NM_001165945.2 | missense | GAG | 9 | c.1732A>G|c.1225A>G |
| CLCNKB | NM_000085.4|NM_001165945.2 | synonymous | TTG | 9 | c.1741C>T|c.1234C>T |
| CASR | NM_001178065.1 | synonymous | CCC | 7 | c.2274G>C |
| CASR | NM_001178065.1 | missense | CAG | 7 | c.3061G>C |
| SLC12A1 | NM_001184832.1 | synonymous | CAT | 2 | c.405C>T |
| SLC12A1 | NM_001184832.1 | synonymous | TAC | 13 | c.1614T>C |
| SLC12A1 | NM_001184832.1 | missense | GCA | 23 | c.2873T>C |
| SLC26A3 | NM_000111.2 | synonymous | CTC | 17 | c.1953T>C |
| SLC26A3 | NM_000111.2 | synonymous | GCA | 11 | c.1299G>A |
| SLC12A3 | NM_000339.2 | missense | GGC | 6 | c.791C>G |
| SLC12A3 | NM_000339.2 | synonymous | GCA | 11 | c.1392C>A |
| SLC12A3 | NM_000339.2 | synonymous | GCT | 17 | c.2142C>T |
| SLC12A3 | NM_000339.2 | synonymous | GGT | 22 | c.2625C>T |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujino, S.; Miyoshi, N.; Ohue, M.; Mukai, M.; Kukita, Y.; Hata, T.; Matsuda, C.; Mizushima, T.; Doki, Y.; Mori, M. Rectal Cancer in a Patient with Bartter Syndrome: A Case Report. Genes 2017, 8, 139. https://doi.org/10.3390/genes8050139
Fujino S, Miyoshi N, Ohue M, Mukai M, Kukita Y, Hata T, Matsuda C, Mizushima T, Doki Y, Mori M. Rectal Cancer in a Patient with Bartter Syndrome: A Case Report. Genes. 2017; 8(5):139. https://doi.org/10.3390/genes8050139
Chicago/Turabian StyleFujino, Shiki, Norikatsu Miyoshi, Masayuki Ohue, Mikio Mukai, Yoji Kukita, Taishi Hata, Chu Matsuda, Tsunekazu Mizushima, Yuichiro Doki, and Masaki Mori. 2017. "Rectal Cancer in a Patient with Bartter Syndrome: A Case Report" Genes 8, no. 5: 139. https://doi.org/10.3390/genes8050139
APA StyleFujino, S., Miyoshi, N., Ohue, M., Mukai, M., Kukita, Y., Hata, T., Matsuda, C., Mizushima, T., Doki, Y., & Mori, M. (2017). Rectal Cancer in a Patient with Bartter Syndrome: A Case Report. Genes, 8(5), 139. https://doi.org/10.3390/genes8050139