Three-Dimensional Finite Element Analysis of Maxillary Sinus Floor Augmentation with Optimal Positioning of a Bone Graft Block

 ,
,
Abstract
:1. Introduction
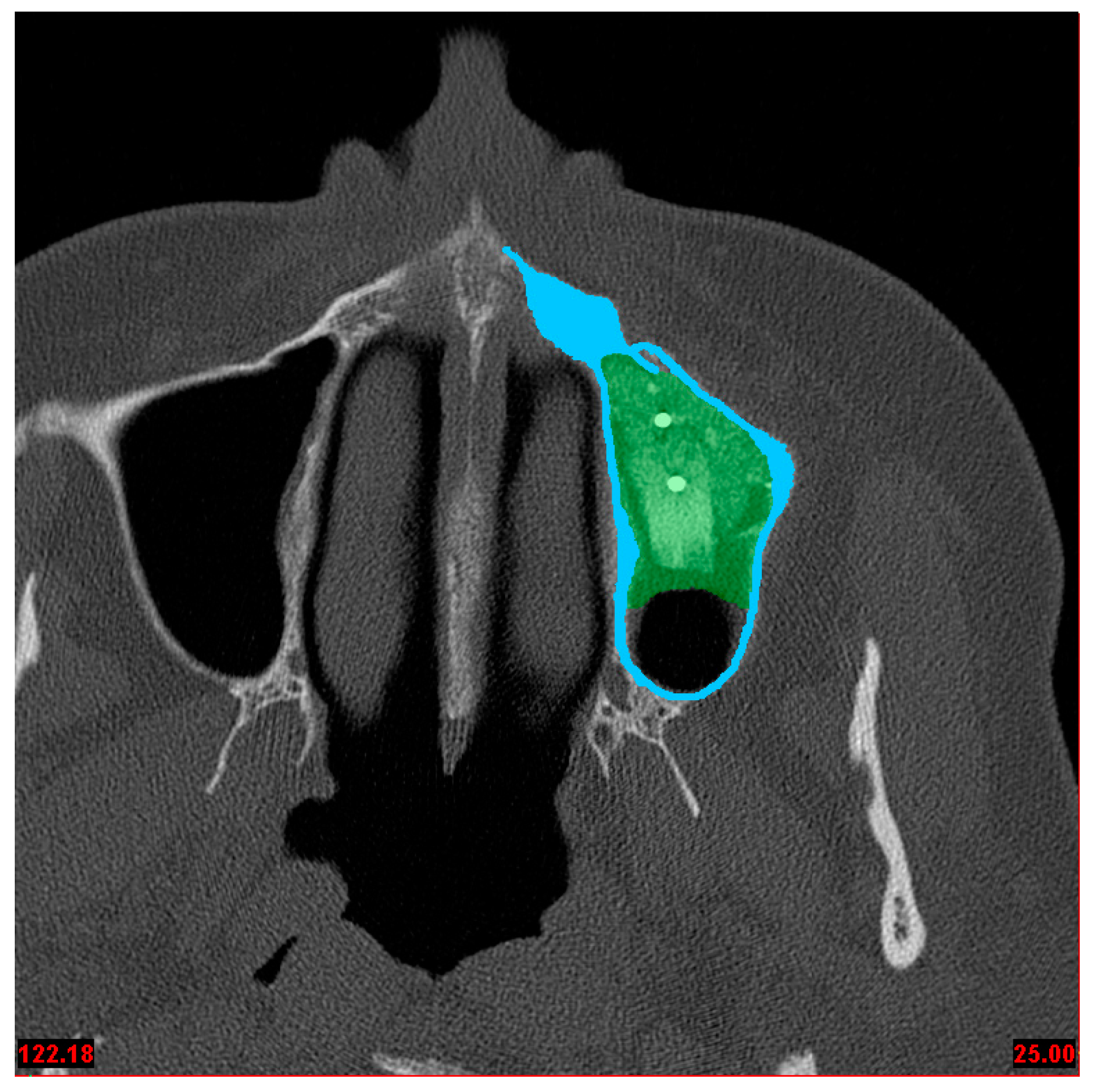
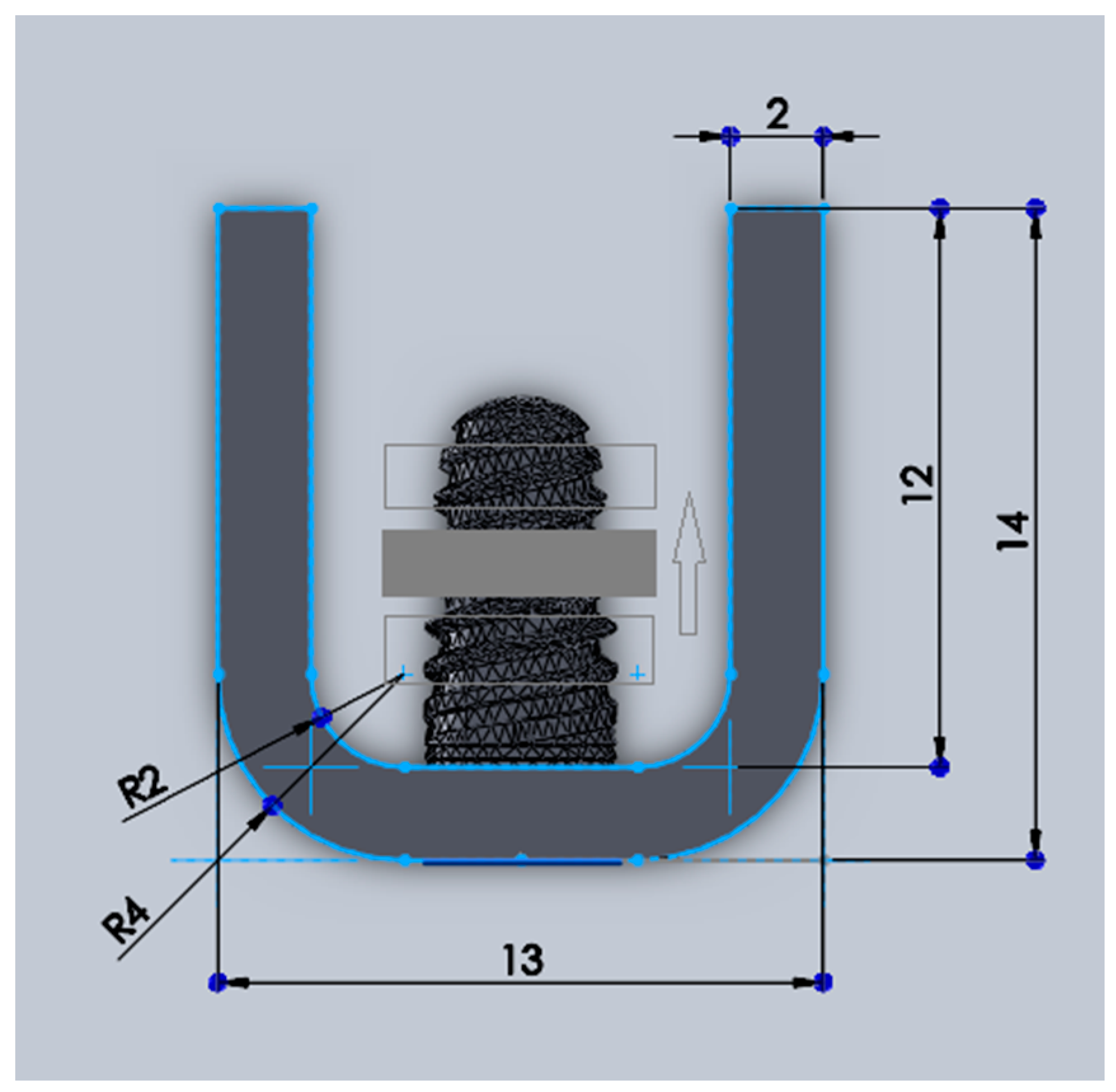
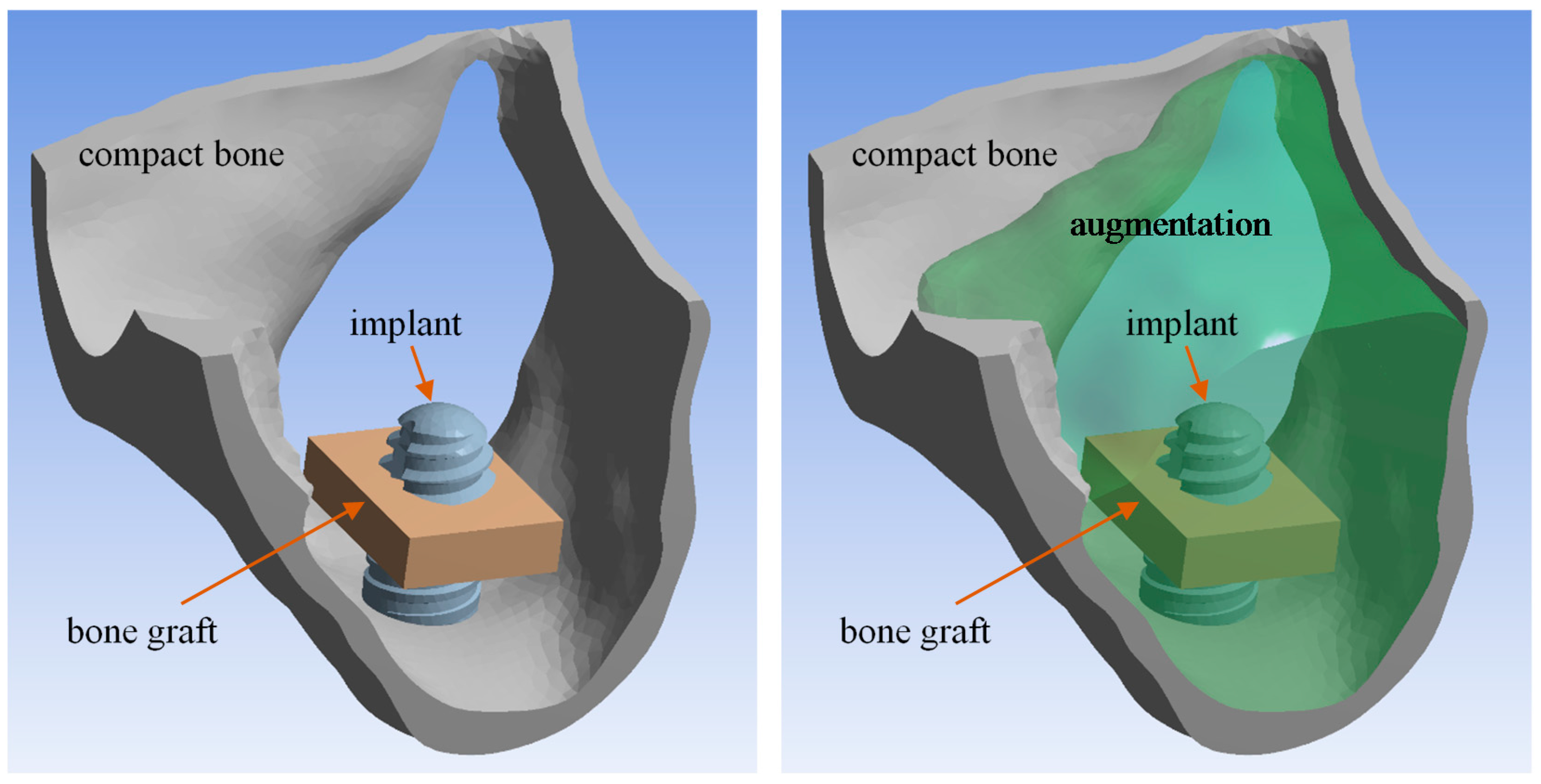
2. Material and Methods
3. Contact Definition
- -
- Fz = 96 N in the z-axis representing masticatory force,
- -
- Py = 36 N in the y-axis presumed from protrusion, and
- -
- Lx = 13 N in the x-axis from laterotrusion.
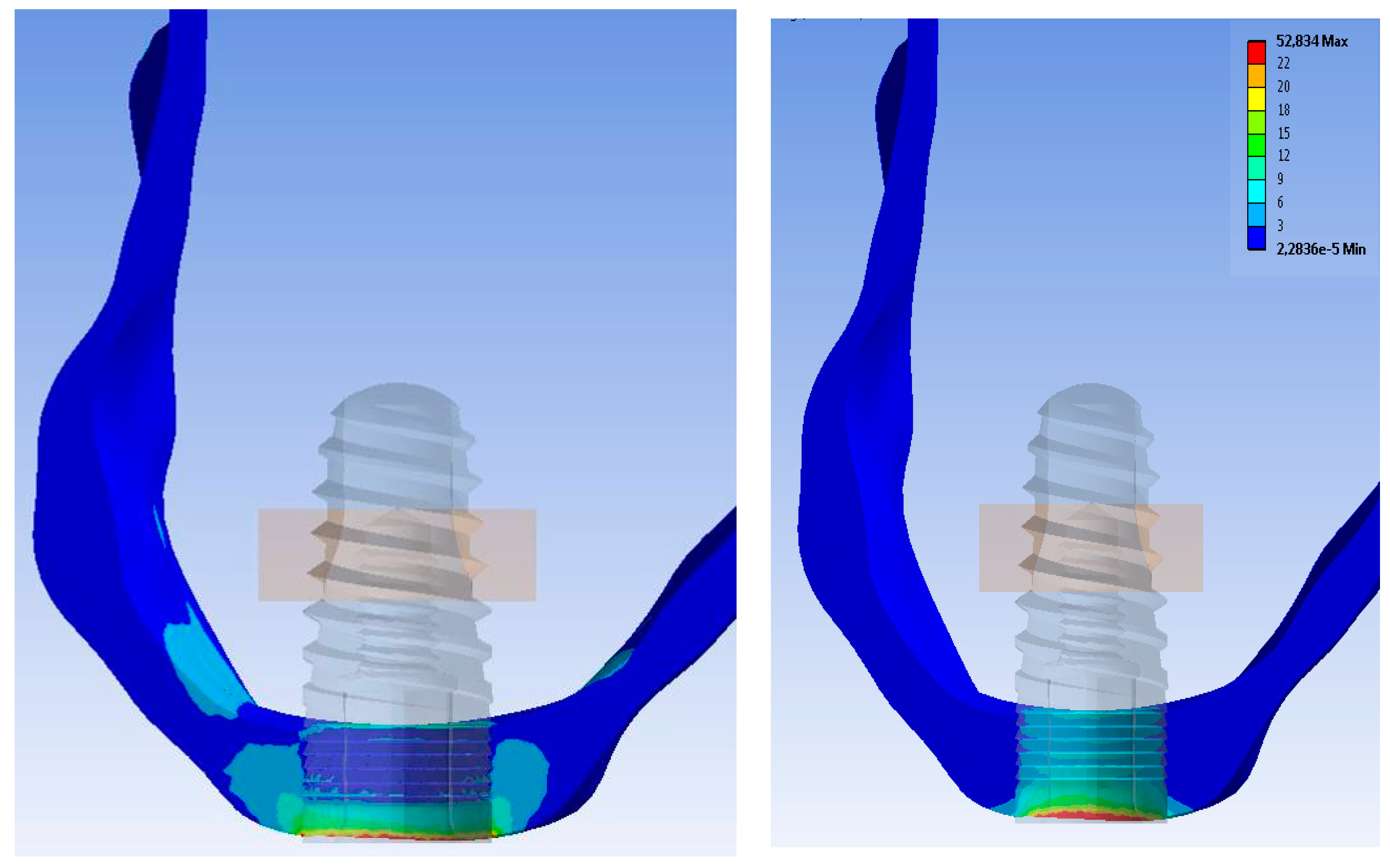
4. Results
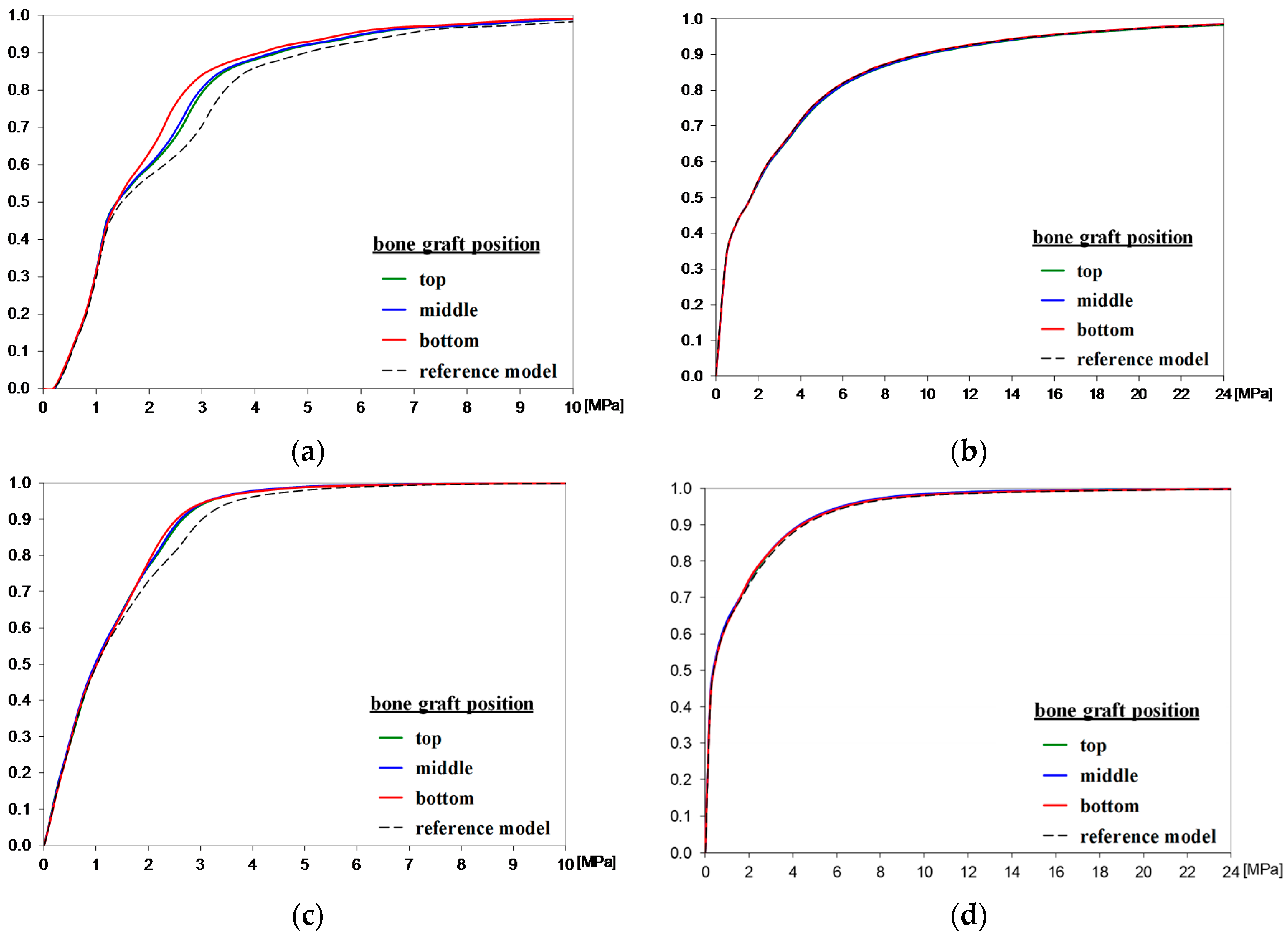
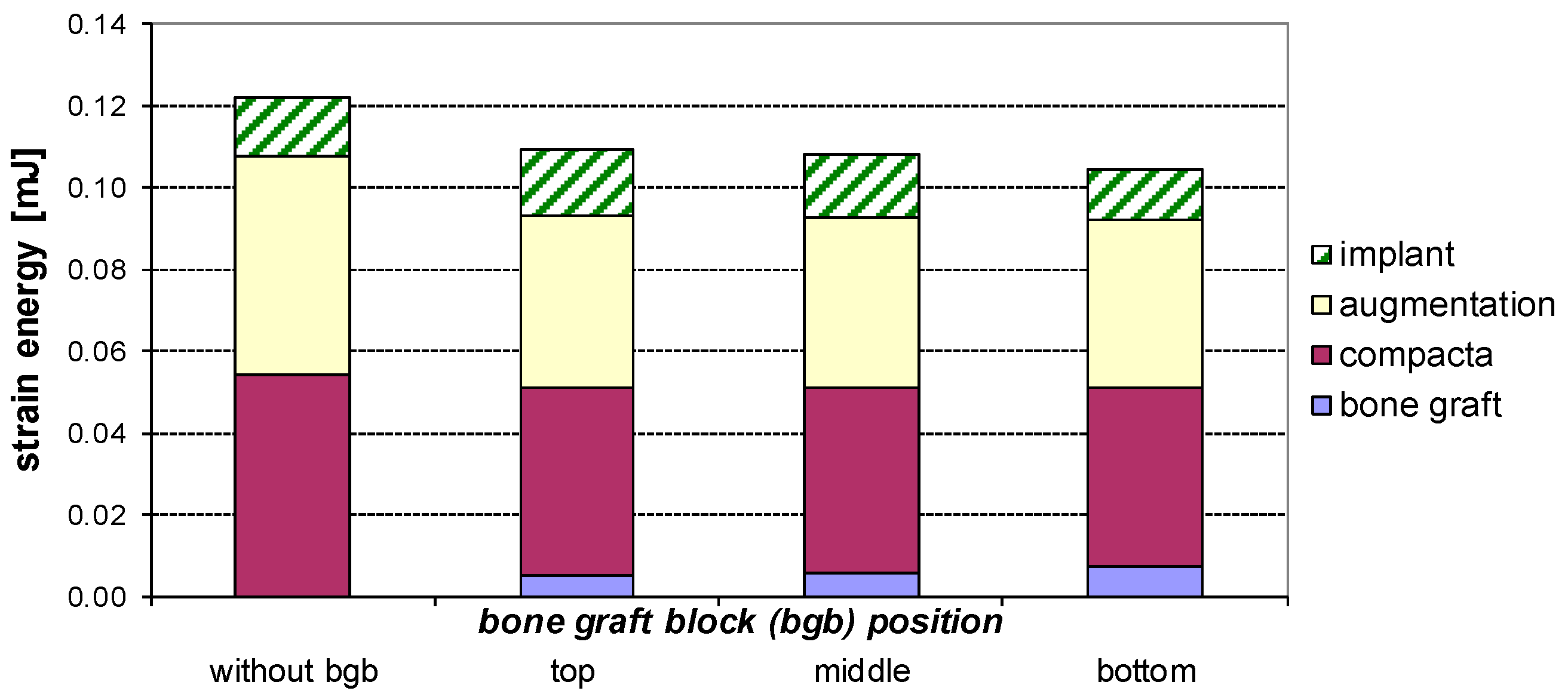
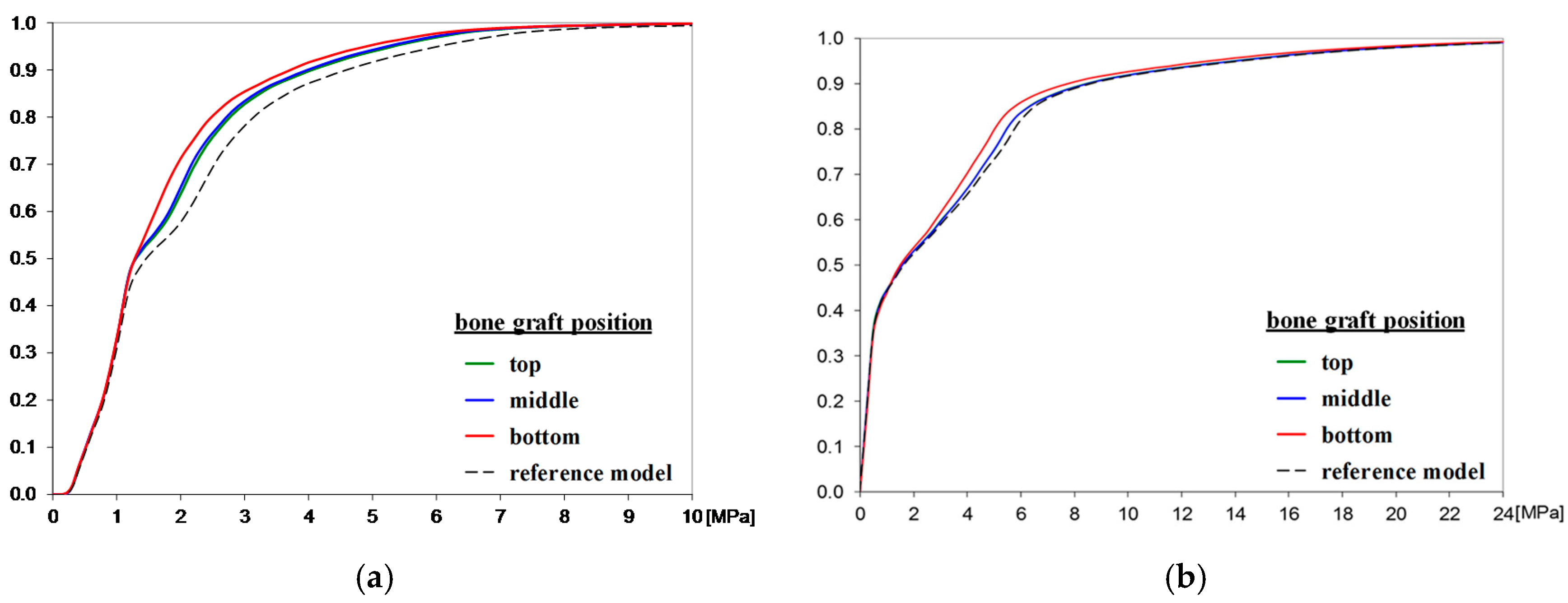
4.1. Bone Graft Position
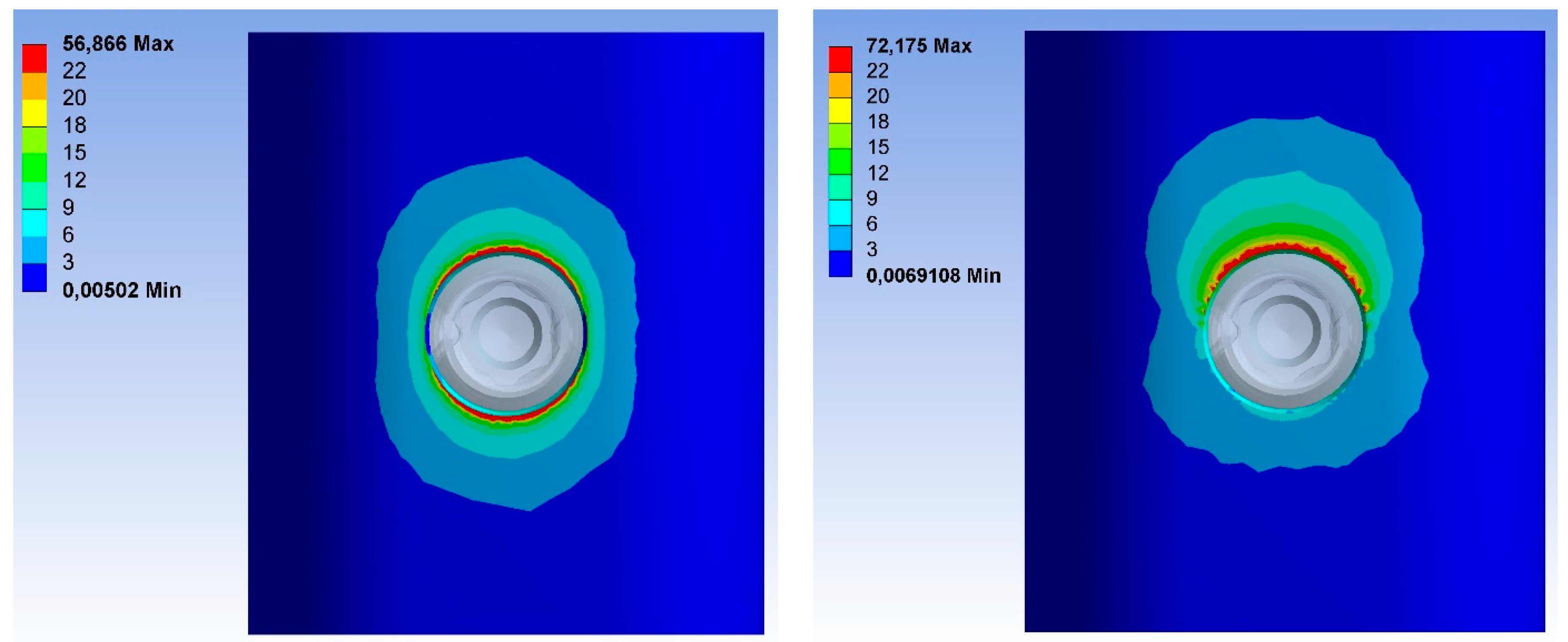
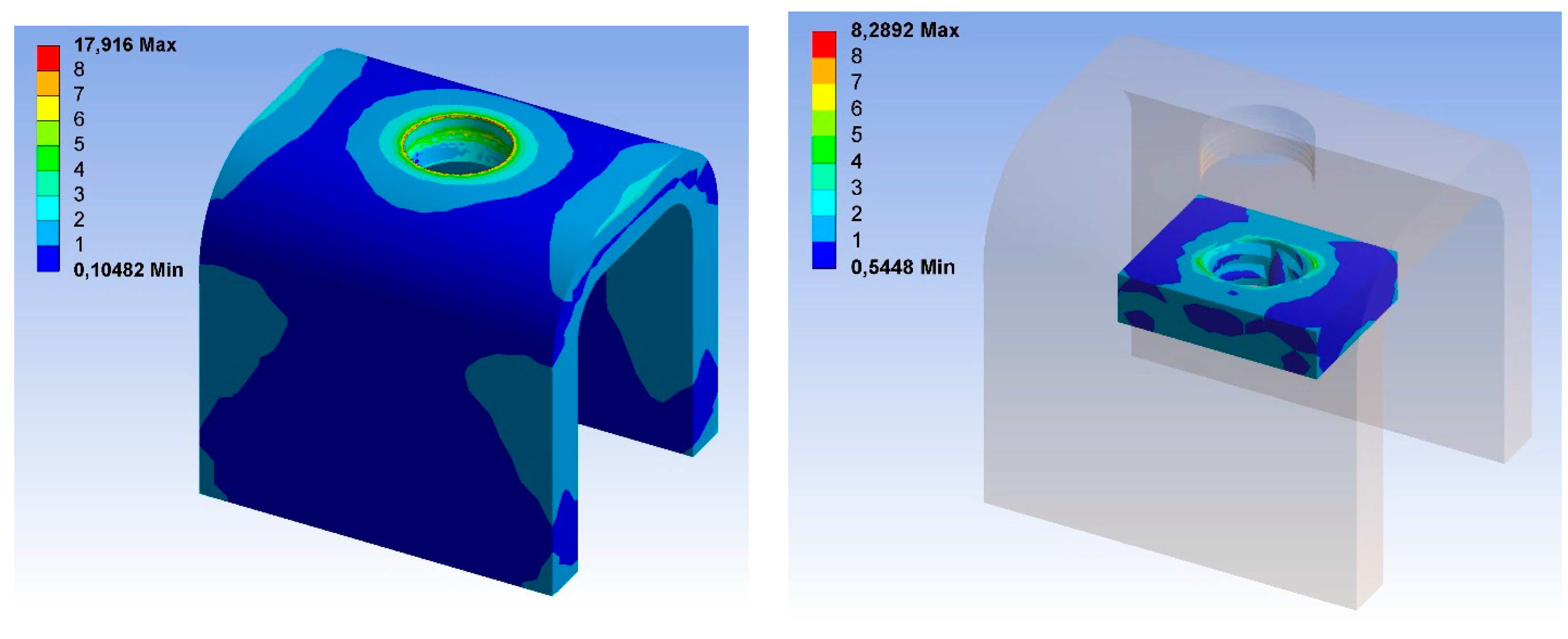
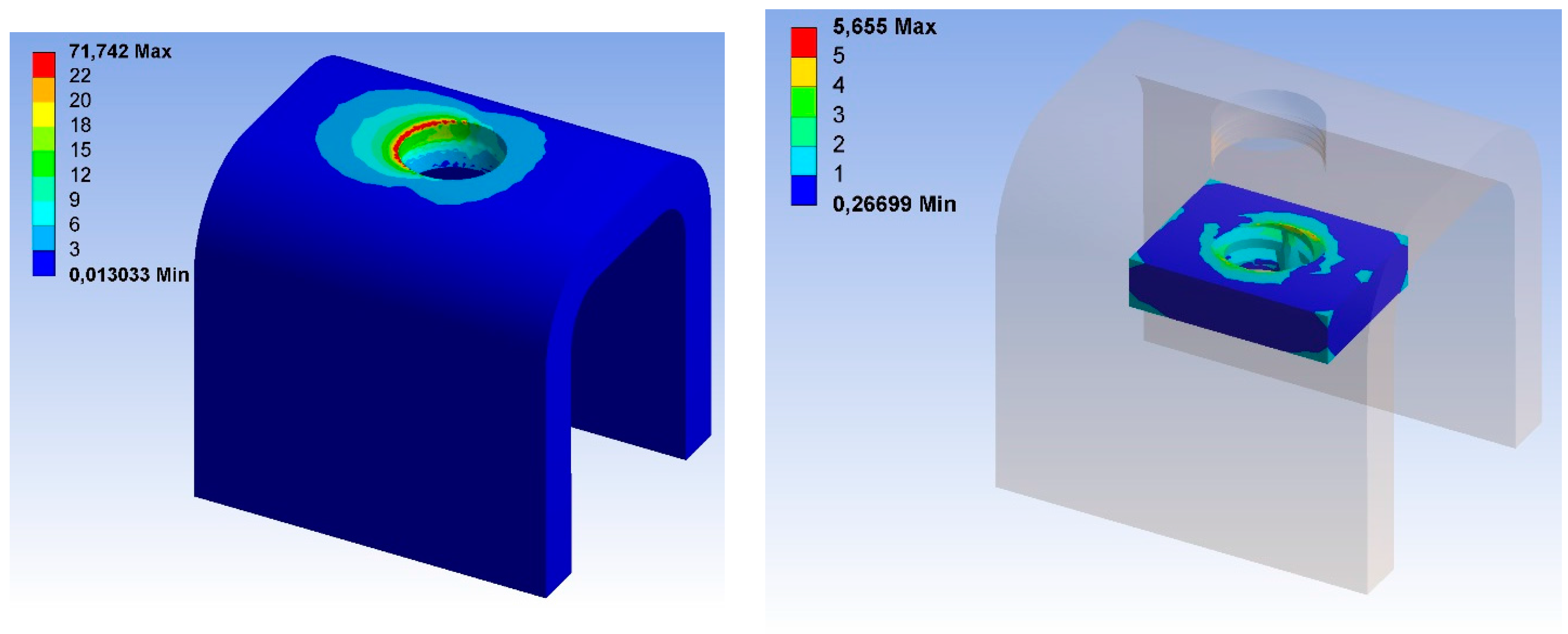
4.2. Consideration of the Friction Coefficient in Contact between the Implant and Compact Bone
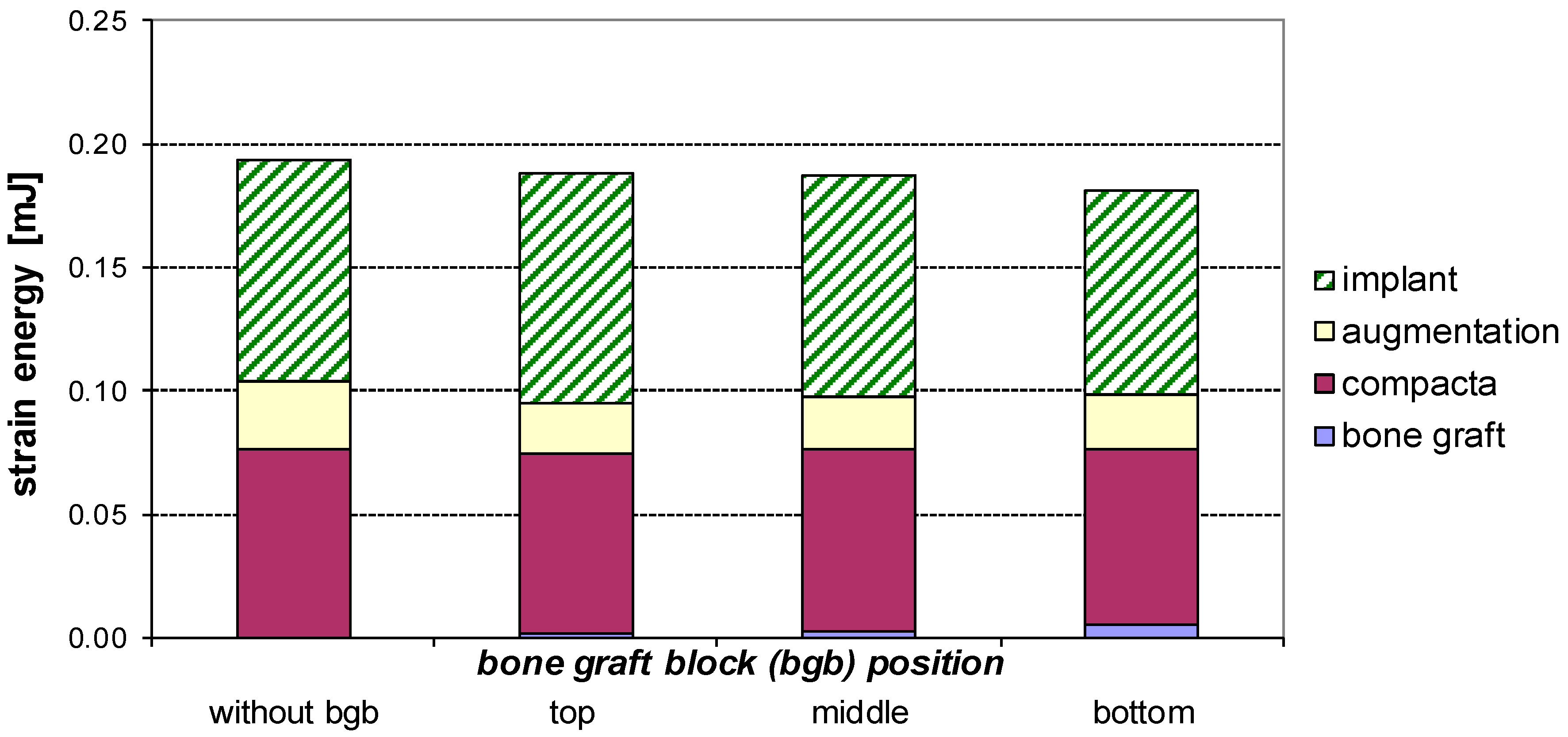
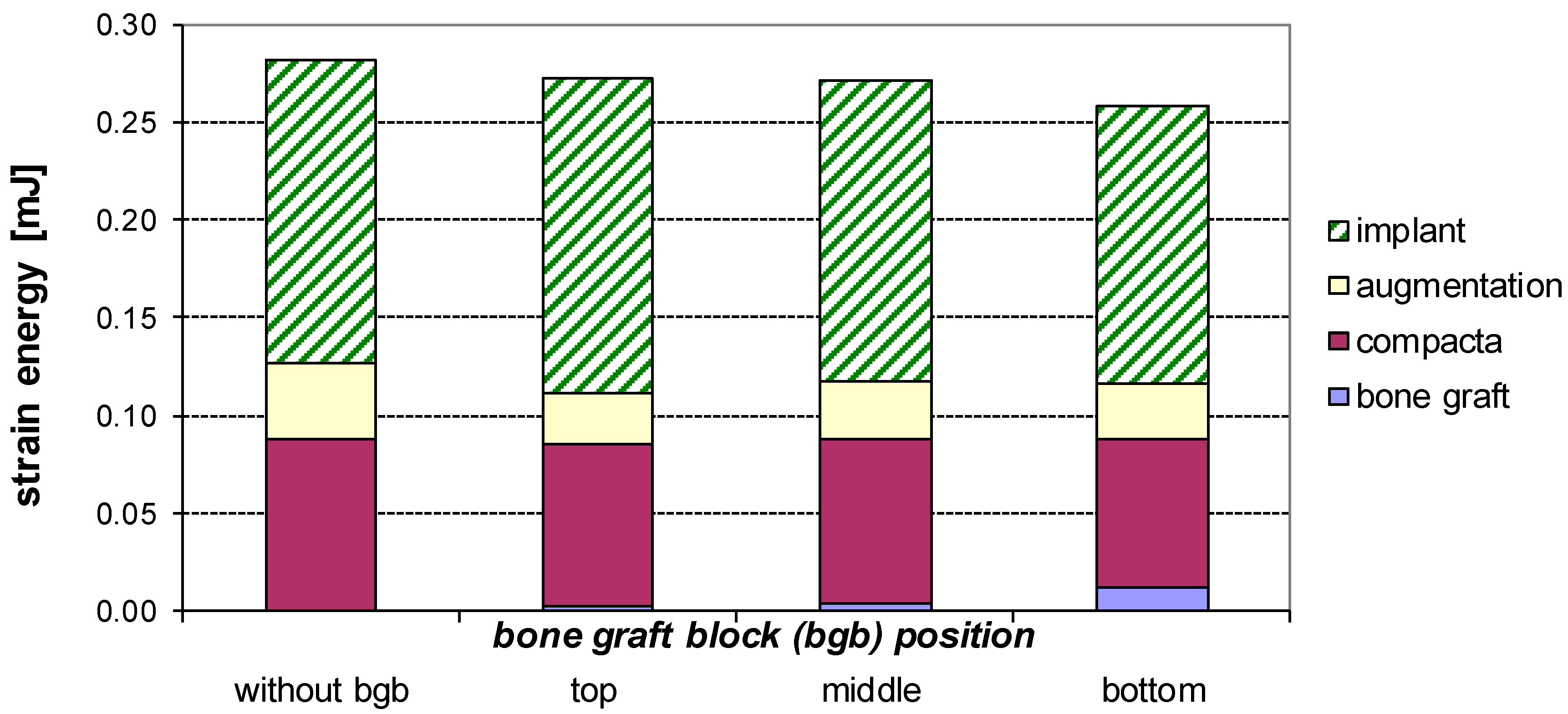
4.3. Strain Energy in the M1f Model
4.4. Additional Information
5. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Poelert, S.; Valstar, E.; Weinans, H.; Zadpoor, A.A. Patient-specific finite element modeling of bones. Proc. Inst. Mech. Eng. H 2013, 227, 464–478. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, R.; Seitz, S.; Vargas, L. The use of virtual models to estimate the amount of grafting material: A case study. Int. J. Oral Maxillofac. Implants 2015, 30, e43–e44. [Google Scholar] [CrossRef] [PubMed]
- Boyne, P.J.; James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J. Oral Surg. 1980, 38, 613–616. [Google Scholar] [PubMed]
- Guerrero, J.S.; Al-Jandan, B.A. Lateral wall sinus floor elevation for implant placement: Revisiting fundamentals and the surgical technique. J. Calif. Dent. Assoc. 2013, 41, 185–195. [Google Scholar] [PubMed]
- Schuller-Götzburg, P.; Entacher, K.; Petutschnigg, A.; Pomwenger, W.; Watzinger, F. Sinus lift with cortical bone graft block: A patient-specific 3D-finite element study. Int. J. Oral Maxillofac. Implants 2012, 27, 359–368. [Google Scholar] [PubMed]
- Yan, X.; Zhang, X.; Chi, W.; Ai, H.; Wu, L. Comparing the influence of crestal cortical bone and sinus floor cortical bone in posterior maxilla bi-cortical dental implantation: A three-dimensional finite element analysis. Acta Odontol. Scand. 2015, 73, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Khoury, F. Augmentation of the sinus floor with mandibular bone block and simultaneous implantation: A 6-year clinical investigation. Int. J. Oral Maxillofac. Implants 1999, 14, 557–564. [Google Scholar] [PubMed]
- Joda, T.; Bragger, U.; Gallucci, G. Systematic literature review of digital three-dimensional superimposition techniques to create virtual dental patients. Int. J. Oral Maxillofac. Implants 2015, 30, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.L.; Chang, S.H.; Chang, W.J.; Kuo, Y.C. Factorial analysis of variables influencing mechanical characteristics of a single tooth implant placed in the maxilla using finite element analysis and the statistics-based taguchi method. Eur. J. Oral Sci. 2007, 115, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Duyck, J.; Van Oosterwyck, D.J.; De Cooman, H.; Puers, M.; Vander Sloten, R.; Naert, I. Three-dimensional force measurements on oral implants: A methodological study. J. Oral Rehabilit. 2000, 27, 744–753. [Google Scholar] [CrossRef]
- Tepper, G.; Haas, R.; Zechner, W.; Krach, W.; Watzek, G. Three-dimensional finite element analysis of implant stability in the atrophic posterior maxilla: A mathematical study of the sinus floor augmentation. Clin. Oral Implants Res. 2002, 13, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.A.; Bishop, N.E.; Götzen, N.; Sprecher, C.; Honl, M.; Morlock, M.M. Artificial composite as a model of human trabecular bone: The implant-bone interface. J. Biomech. 2007, 40, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Fanuscu, M.I.; Vu, H.V.; Poncelet, B. Implant biomechanics in grafted sinus: A finite element analysis. J. Oral Implantol. 2004, 30, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Mericske-Stern, R.; Venetz, E.; Fahrlander, F.; Burgin, W. In vivo force measurements on maxillary implants supporting a fixed prosthesis or an overdenture: A pilot study. J. Prosthet. Dent. 2000, 84, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J. Das Gesetz der Transformation der Knochen—1892; Reprint; Pro Business: Berlin, Germany, 2010. [Google Scholar]
- Frost, H.M. From Wolff’s law to the Utah paradigm: Insights about bone physiology and its clinical applications. Anat. Rec. 2001, 262, 398–419. [Google Scholar] [CrossRef] [PubMed]
- Jensen, O.T.; Shulman, L.B.; Block, M.S.; Iacono, V.J. Report of the Sinus Consensus Conference of 1996. Int. J. Oral Maxillofac. Implants 1998, 13, 11–45. [Google Scholar] [PubMed]
- Pesqueria, A.; Goiato, M.; Gennari-Filho, H.; Monteiro, D.; Dos Santos, D.; Haddad, M.; Pellizzer, E. The use of stress analysis methods to evaluate the biomechanics of oral rehabilitation with implants. J. Oral Implantol. 2012, 40, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Himmlová, L.; Dostálová, T.; Kácovsky, A.; Konvicková, S. Influence of implant length and diameter on stress distribution: A finite element analysis. J. Prosthet. Dent. 2004, 91, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Koca, O.L.; Eskitascioglu, G.; Usumez, A. Three-dimensional finite-element analysis of functional stresses in different bone locations produced by implants placed in the maxillary posterior region of the sinus floor. J. Prosthet. Dent. 2005, 93, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Okumura, N.; Stegaroiu, R.; Kitamura, E.; Kurokawa, K.; Nomura, S. Influence of maxillary cortical bone thickness, implant design and implant diameter on stress around implants: A three-dimensional finite element analysis. J. Prosthodont. Res. 2010, 54, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Van Staden, R.C.; Guan, H.; Loo, Y.C. Application of the finite element method in dental implant research. Comput. Methods Biomech. Biomed. Eng. 2006, 9, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Yang, X.; Zhang, D.; Zhou, H.; Shao, J.; Ding, Y.; Kong, L. Analysis of the biomechanical feasibility of a wide implant in moderately atrophic maxillary sinus region with finite element method. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.; Wang, Q.; Dechow, P.C. Material properties of the dentate maxilla. Anat. Rec. A Discov. Mol. Cell. Evolut. Biol. 2006, 288, 962–972. [Google Scholar] [CrossRef] [PubMed]
- Garcia, D.; Zysset, P.K.; Charlebois, M.; Curnier, A. A three-dimensional elastic plastic damage constitutive law for bone tissue. Biomech. Model. Mechanobiol. 2009, 8, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Mullender, M.G.; Huiskes, R. Proposal for the regulatory mechanism of Wolff’s law. J. Orthop. Res. 1995, 13, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, S.; Shanbhag, V.; Stavropoulos, A. Volume changes of maxillary sinus augmentations over time: A systematic review. Int. J. Oral Maxillofac. Implants 2014, 29, 881–892. [Google Scholar] [CrossRef] [PubMed]
- Schuller-Götzburg, P.; Krenkel, C.; Reiter, T.J.; Plenk, H. 2D-finite element analyses and histomorphology of lag screws with and without a biconcave washer. J. Biomech. 1999, 32, 511–520. [Google Scholar] [CrossRef]
- Ding, X.; Zhu, X.H.; Liao, S.H.; Zhang, X.H.; Chen, H. Implant-bone interface stress distribution in immediately loaded implants of different diameters: A three-dimensional finite element analysis. J. Prosthodont. 2009, 18, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Goiato, M.C.; Bannwart, L.C.; Pesqueria, A.A.; Santos, D.M.; Haddad, M.F.; Santos, M.R.; Castilho, P.U. Immediate loading of overdentures: Systematic review. Oral Maxillofac. Surg. 2014, 18, 259–264. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bone Graft Position (Main Question) | |||||
|---|---|---|---|---|---|
| Model (Sub-Question 1) | on the Top (t) | in the Center (c) | Below (b) | Reference Model (r) | Additional Information |
| M1 | M1_t | M1_c | M1_b | M1_r | Compact bone 2 mm (osseointegrated phase) |
| M1f_t | M1f_c | M1f_b | M1f_r | Compact bone 2 mm with friction contact (healing phase) | |
| M2 | M2_t | M2_c | M2_b | M2_r | Model from CT data (osseointegrated phase) |
| M1_r | M1_t | M1_c | M1_b | ||
|---|---|---|---|---|---|
| Bone graft | 0.005 | 0.006 | 0.007 | mJ | |
| Compact bone | 0.054 | 0.046 | 0.045 | 0.044 | mJ |
| Augmentation | 0.053 | 0.042 | 0.042 | 0.041 | mJ |
| Implant | 0.014 | 0.016 | 0.015 | 0.012 | mJ |
| M1_r | M1_t | M1_c | M1_b | ||
|---|---|---|---|---|---|
| Bone graft | 0.001 | 0.002 | 0.006 | mJ | |
| Compact bone | 0.077 | 0.073 | 0.074 | 0.070 | mJ |
| Augmentation | 0.027 | 0.020 | 0.021 | 0.023 | mJ |
| Implant | 0.090 | 0.094 | 0.090 | 0.083 | mJ |
| M1f_c Model | σv,max Load Fz | σv,max Load Py | σv,max Load Lx |
|---|---|---|---|
| Compact bone | 11.66 (17.92 *) | 35.03 (71.74 *) | 13.79 (25.14 *) |
| Bone graft | 7.18 (8.29 *) | 4.80 (5.66 *) | 1.53 * (1.79 *) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schuller-Götzburg, P.; Forte, T.; Pomwenger, W.; Petutschnigg, A.; Watzinger, F.; Entacher, K. Three-Dimensional Finite Element Analysis of Maxillary Sinus Floor Augmentation with Optimal Positioning of a Bone Graft Block. Symmetry 2018, 10, 33. https://doi.org/10.3390/sym10020033
Schuller-Götzburg P, Forte T, Pomwenger W, Petutschnigg A, Watzinger F, Entacher K. Three-Dimensional Finite Element Analysis of Maxillary Sinus Floor Augmentation with Optimal Positioning of a Bone Graft Block. Symmetry. 2018; 10(2):33. https://doi.org/10.3390/sym10020033
Chicago/Turabian StyleSchuller-Götzburg, Peter, Thomas Forte, Werner Pomwenger, Alexander Petutschnigg, Franz Watzinger, and Karl Entacher. 2018. "Three-Dimensional Finite Element Analysis of Maxillary Sinus Floor Augmentation with Optimal Positioning of a Bone Graft Block" Symmetry 10, no. 2: 33. https://doi.org/10.3390/sym10020033
APA StyleSchuller-Götzburg, P., Forte, T., Pomwenger, W., Petutschnigg, A., Watzinger, F., & Entacher, K. (2018). Three-Dimensional Finite Element Analysis of Maxillary Sinus Floor Augmentation with Optimal Positioning of a Bone Graft Block. Symmetry, 10(2), 33. https://doi.org/10.3390/sym10020033