
Accurate Parameter Estimation for Master–Slave Operation of a Surgical Robot



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Motion Analysis of Surgical Manipulator
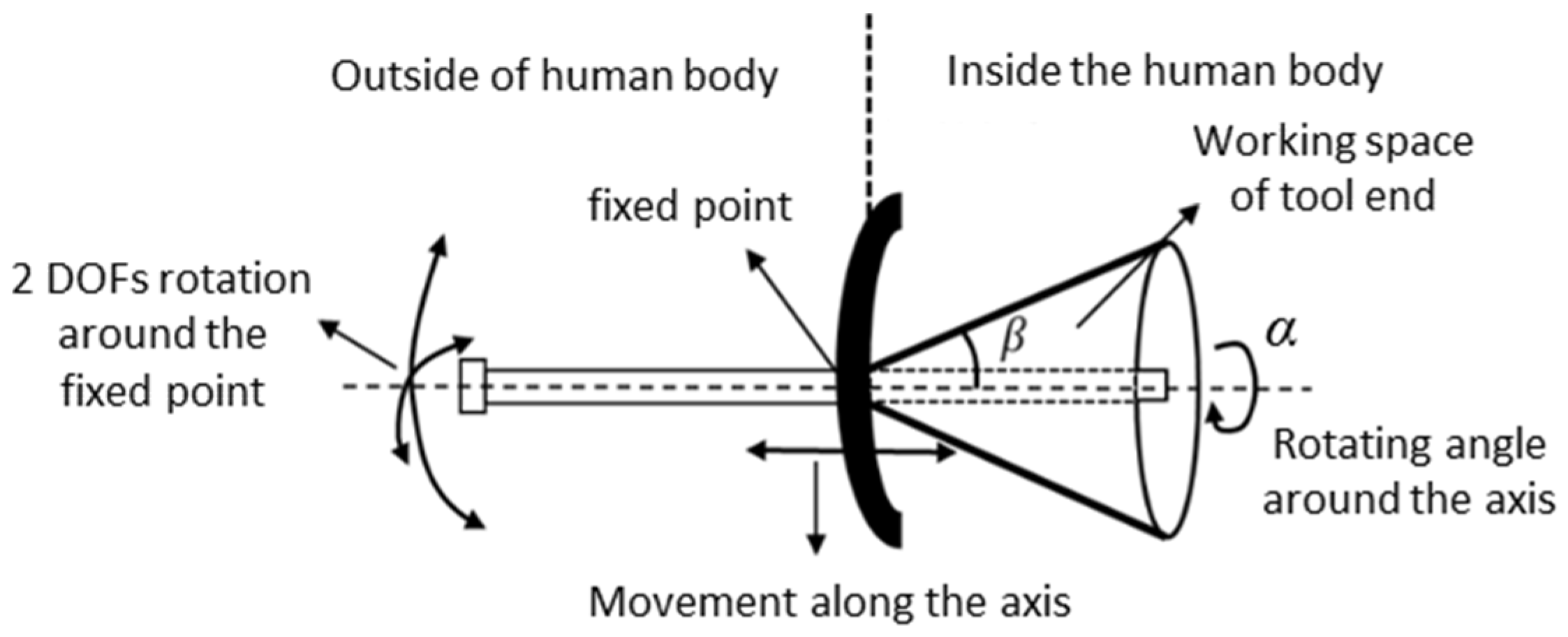
2.1. Movement of the Surgical Manipulator
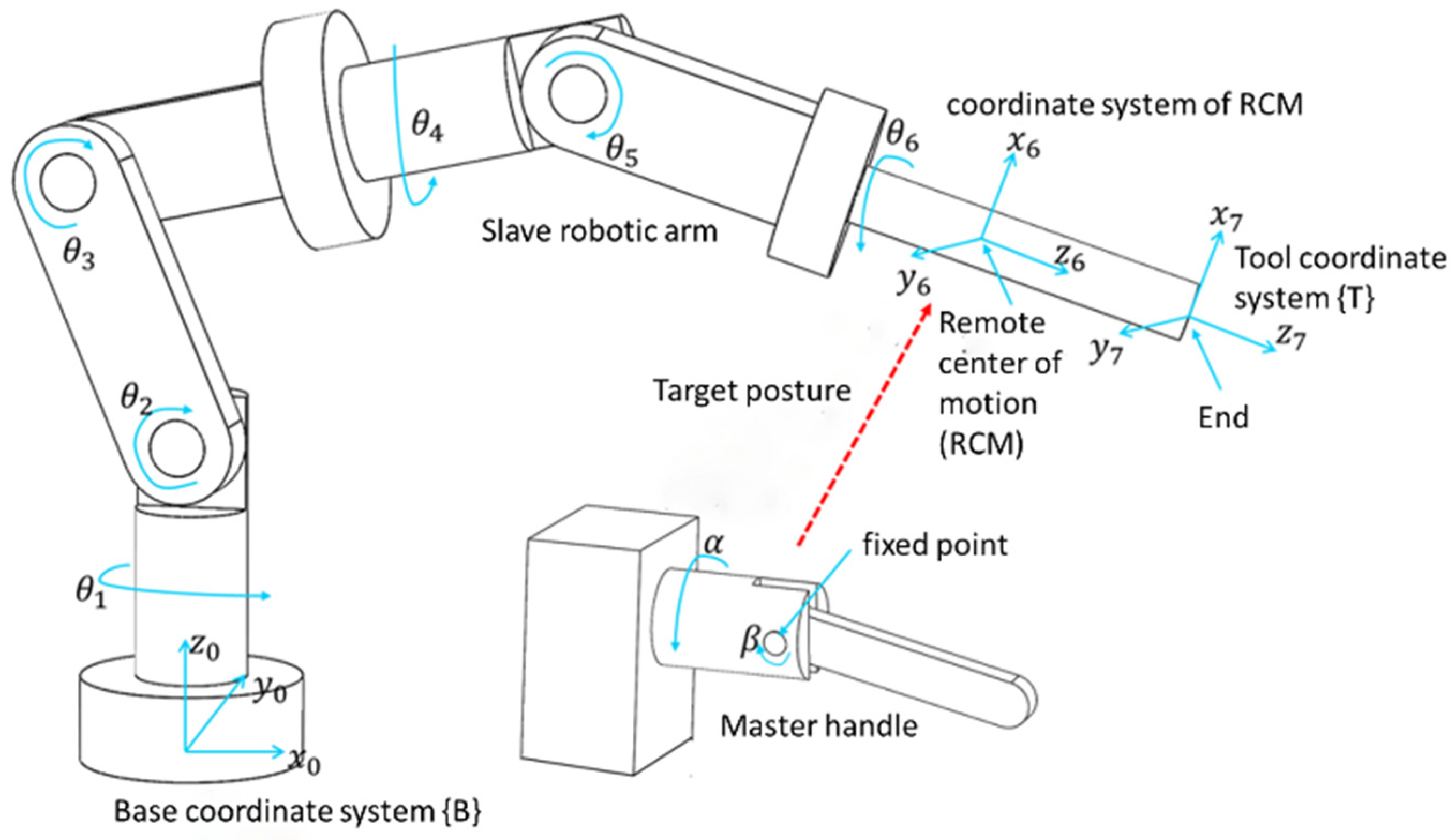
2.2. Modeling of End Effector Posture
3. Parameter Estimation by Simulation
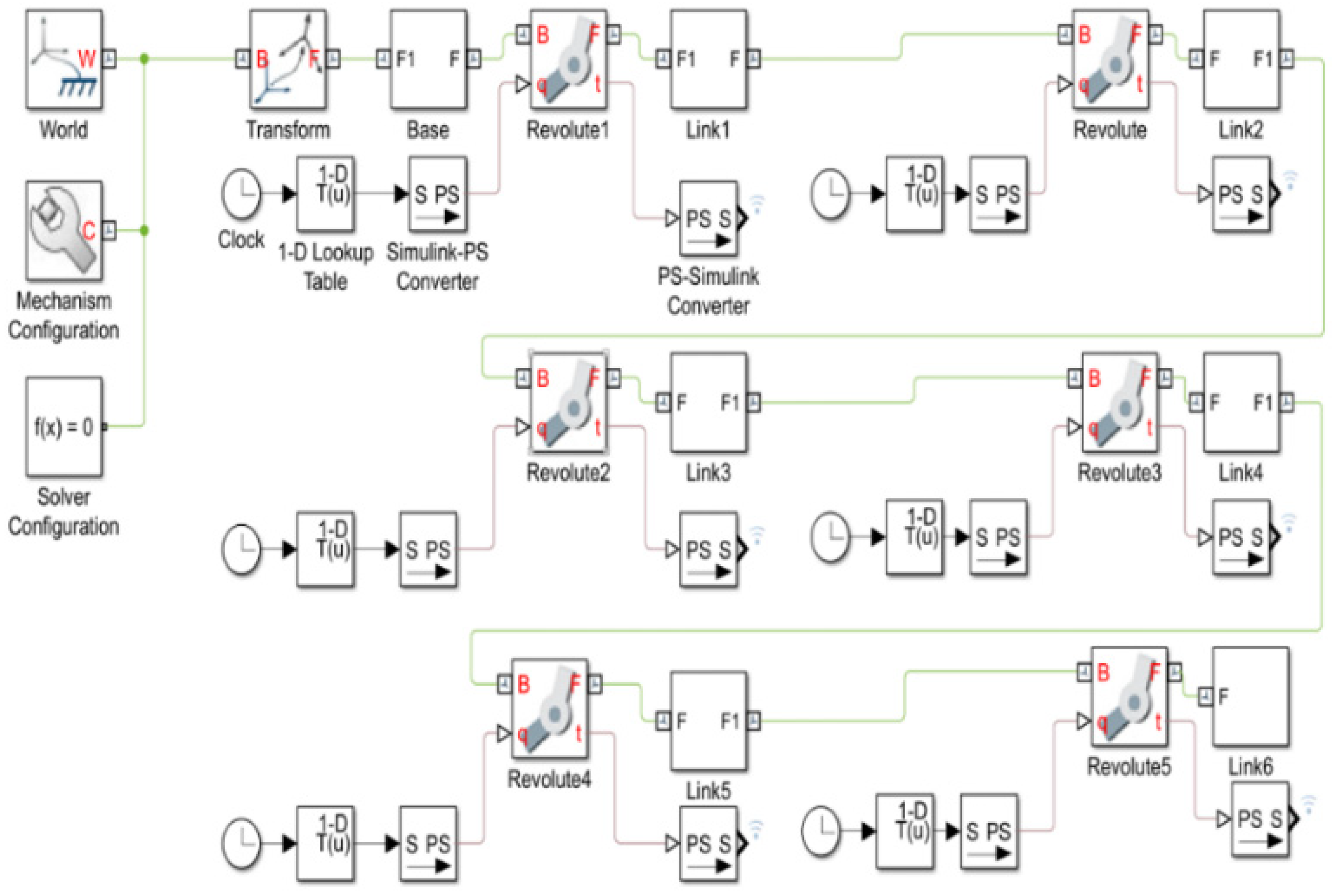
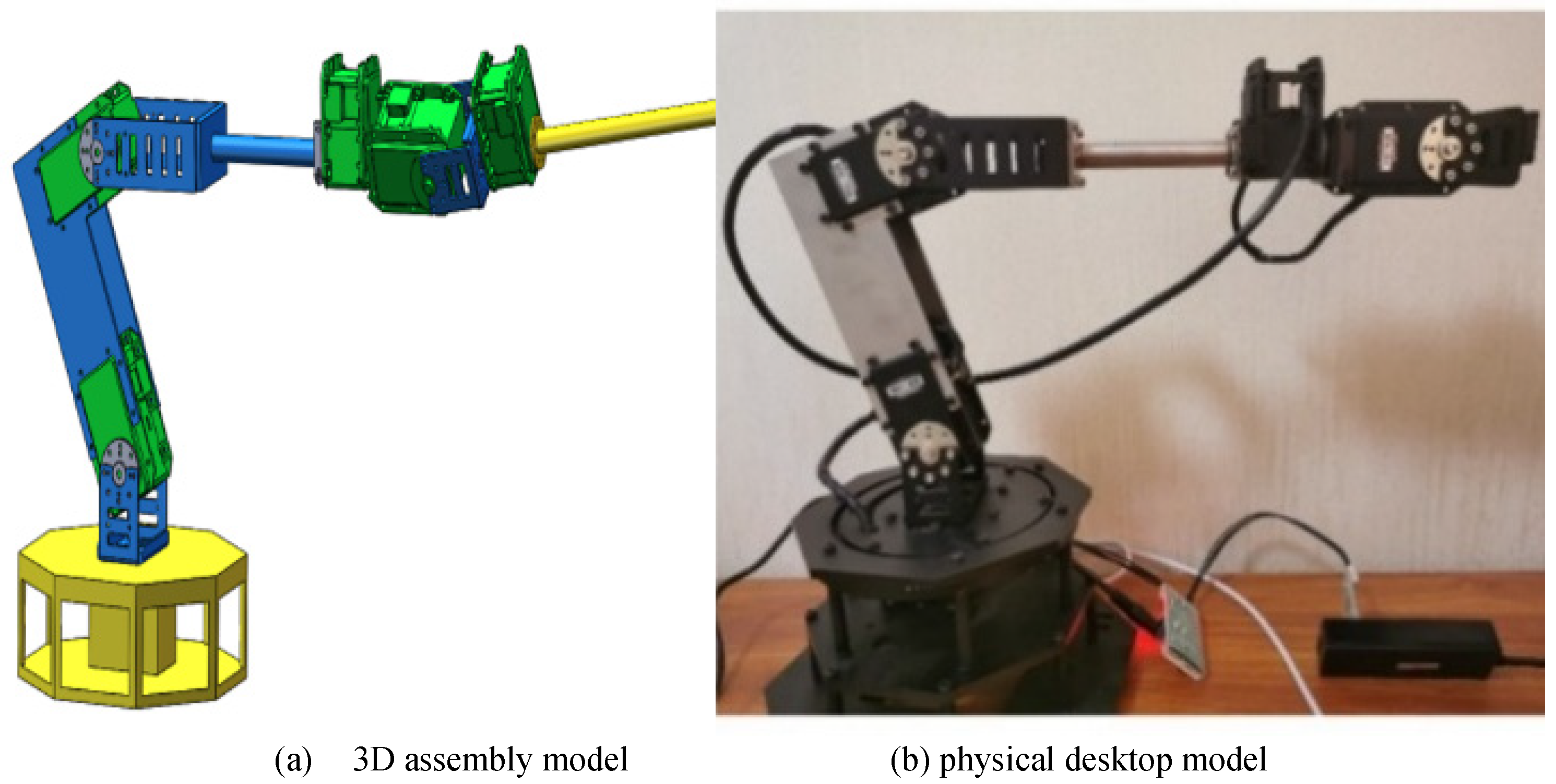
3.1. Simulation Model Creation
3.2. Trajectory Planning
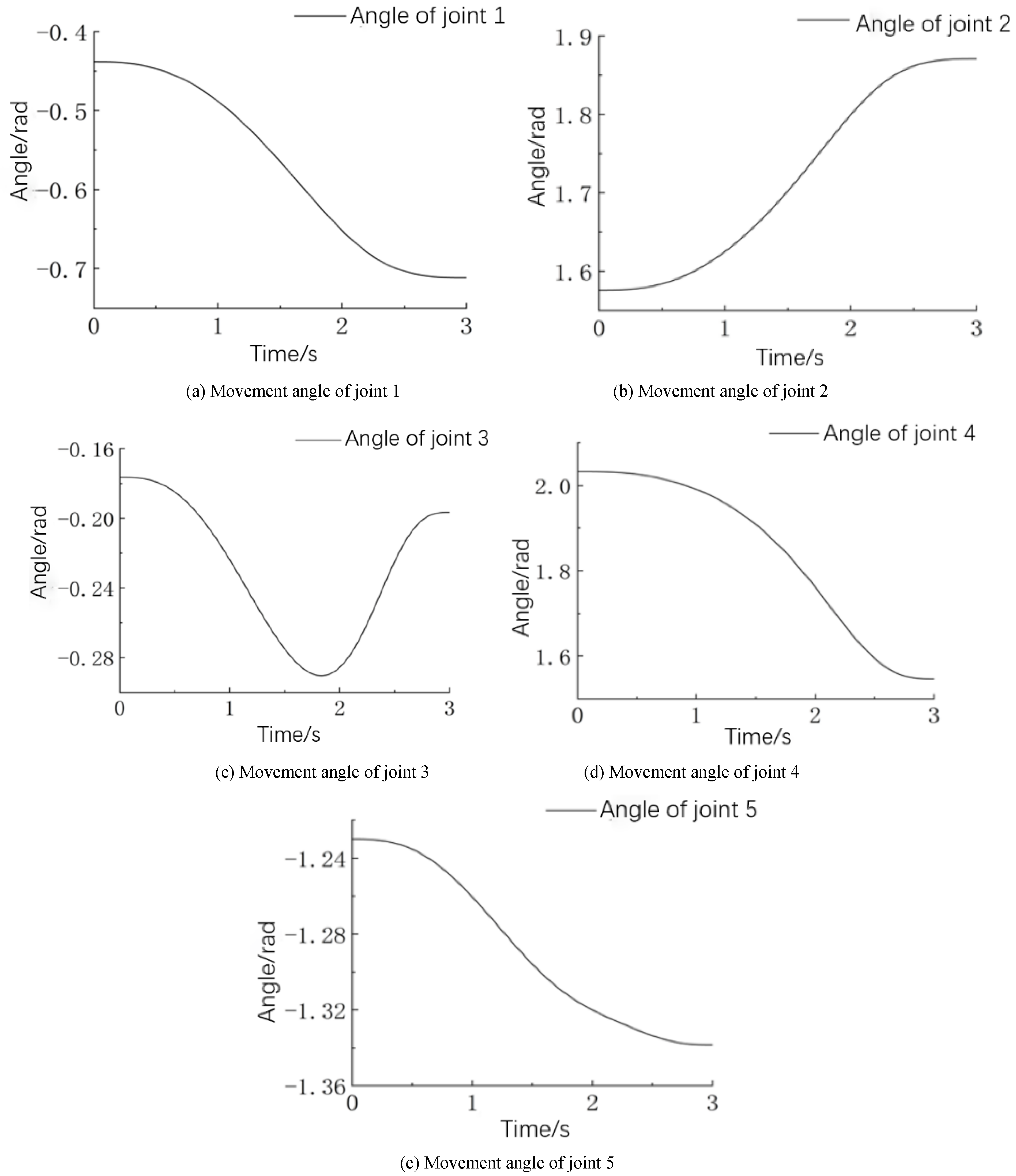
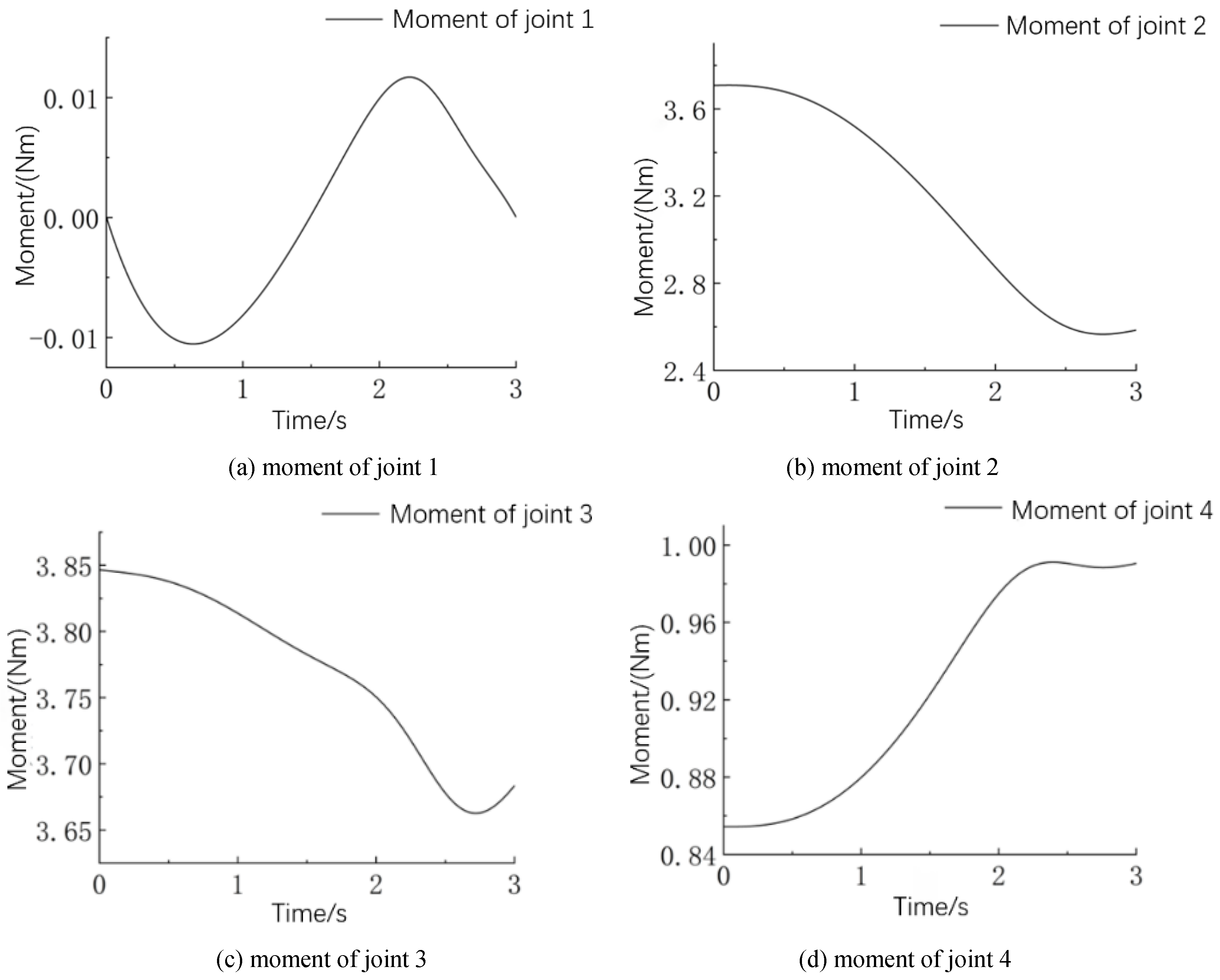
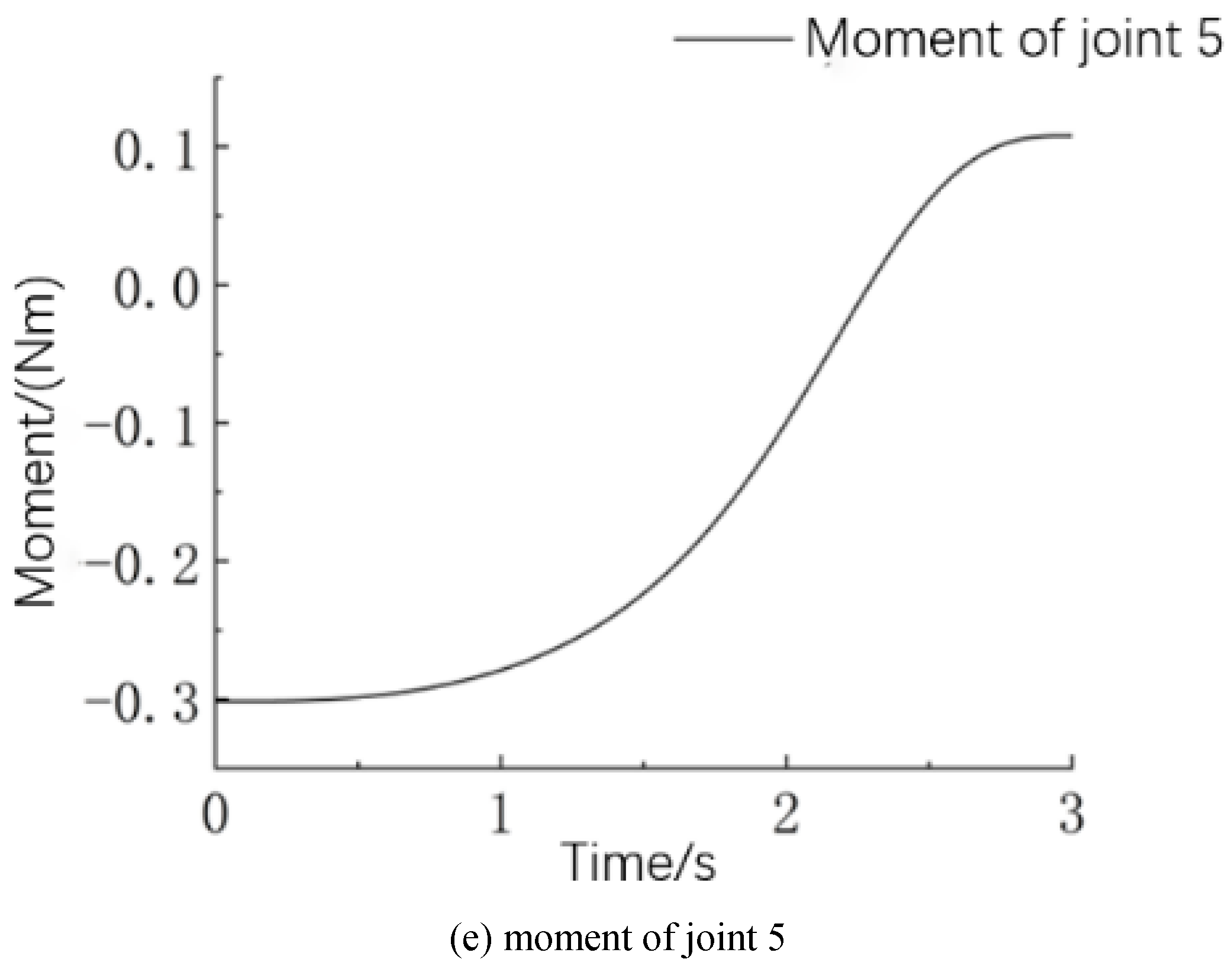
3.3. Joint Dynamics Simulation
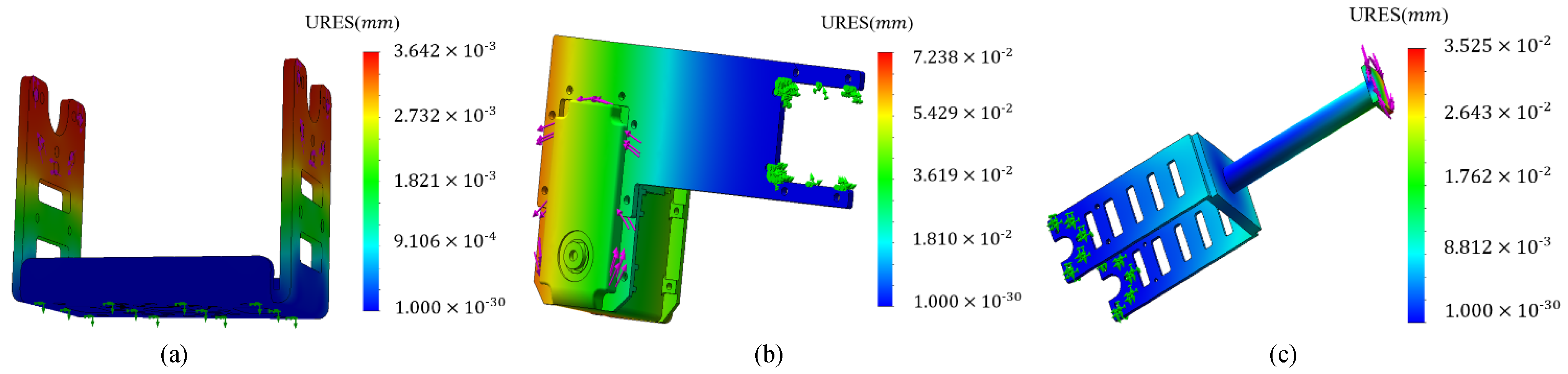
3.4. Structure Design of Surgical Slave Robotic Arm
4. Master–Slave Control Experiment
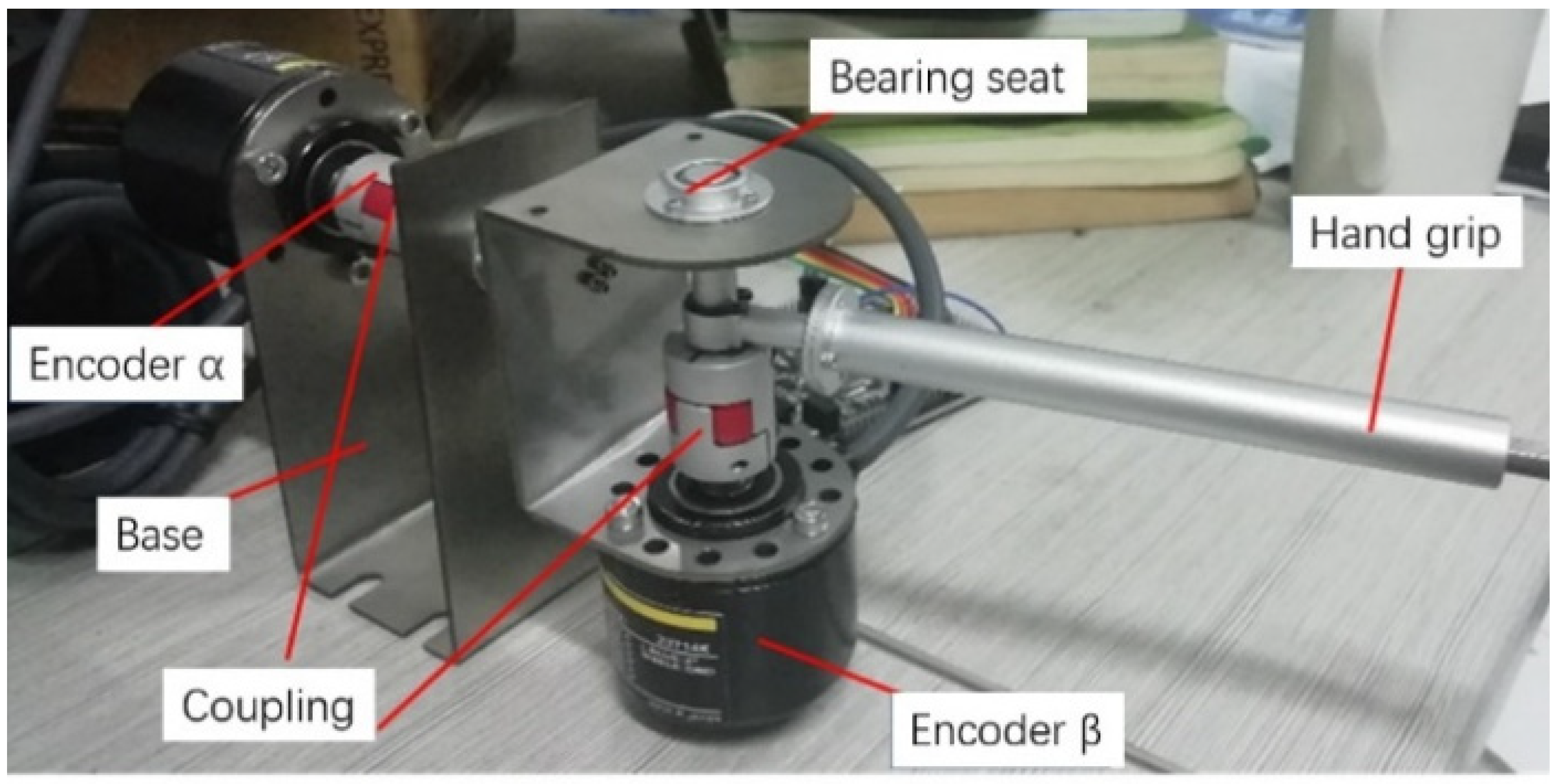
4.1. Master Mechanism Design
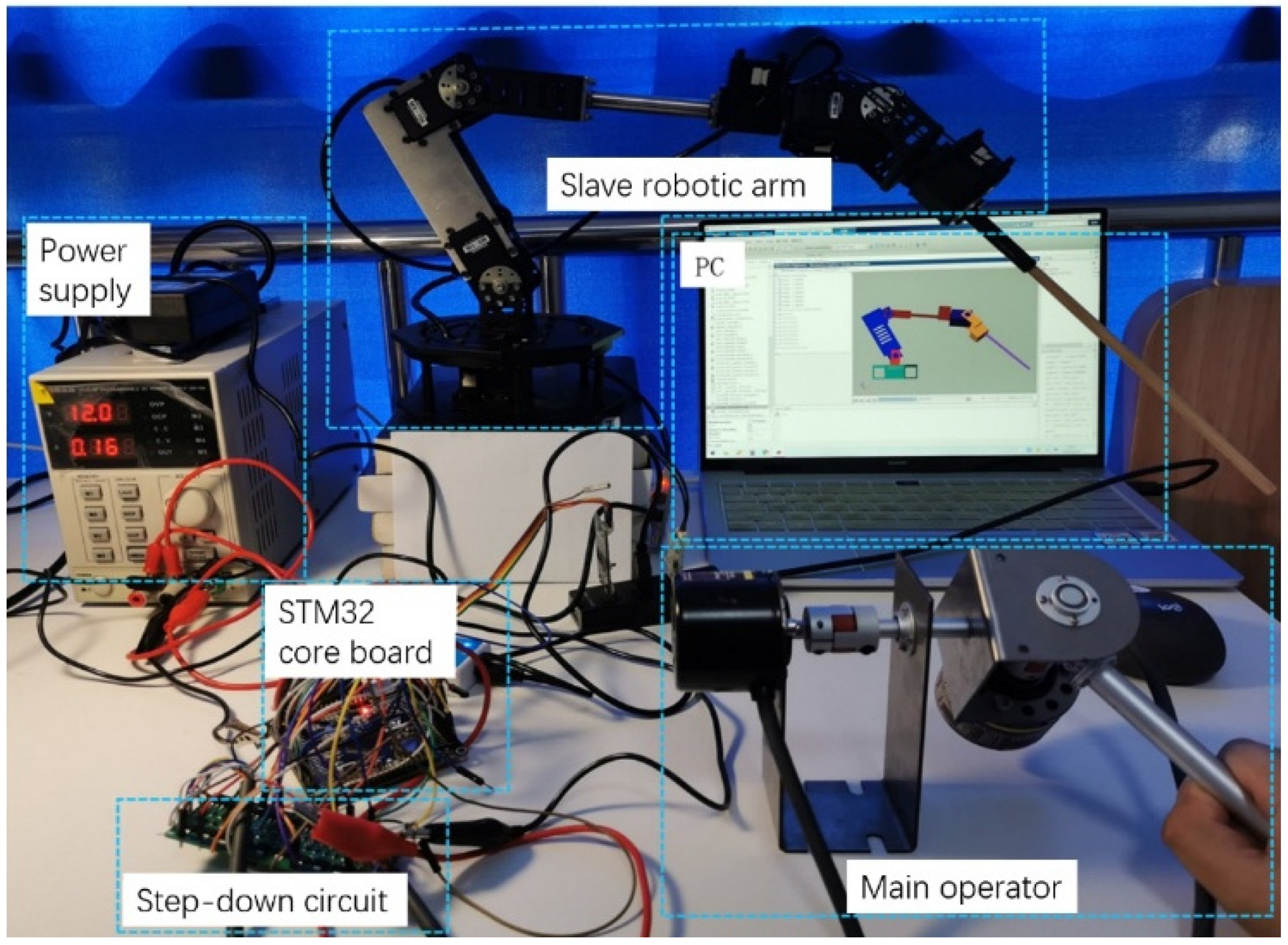
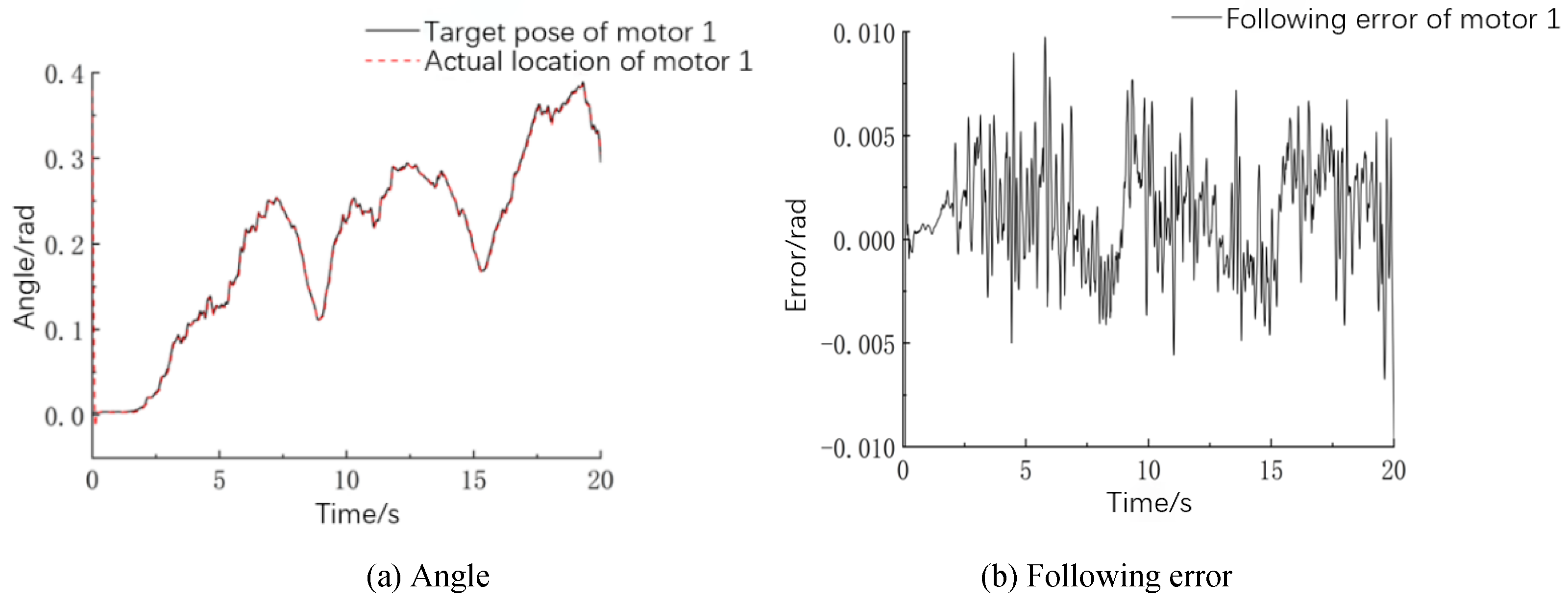
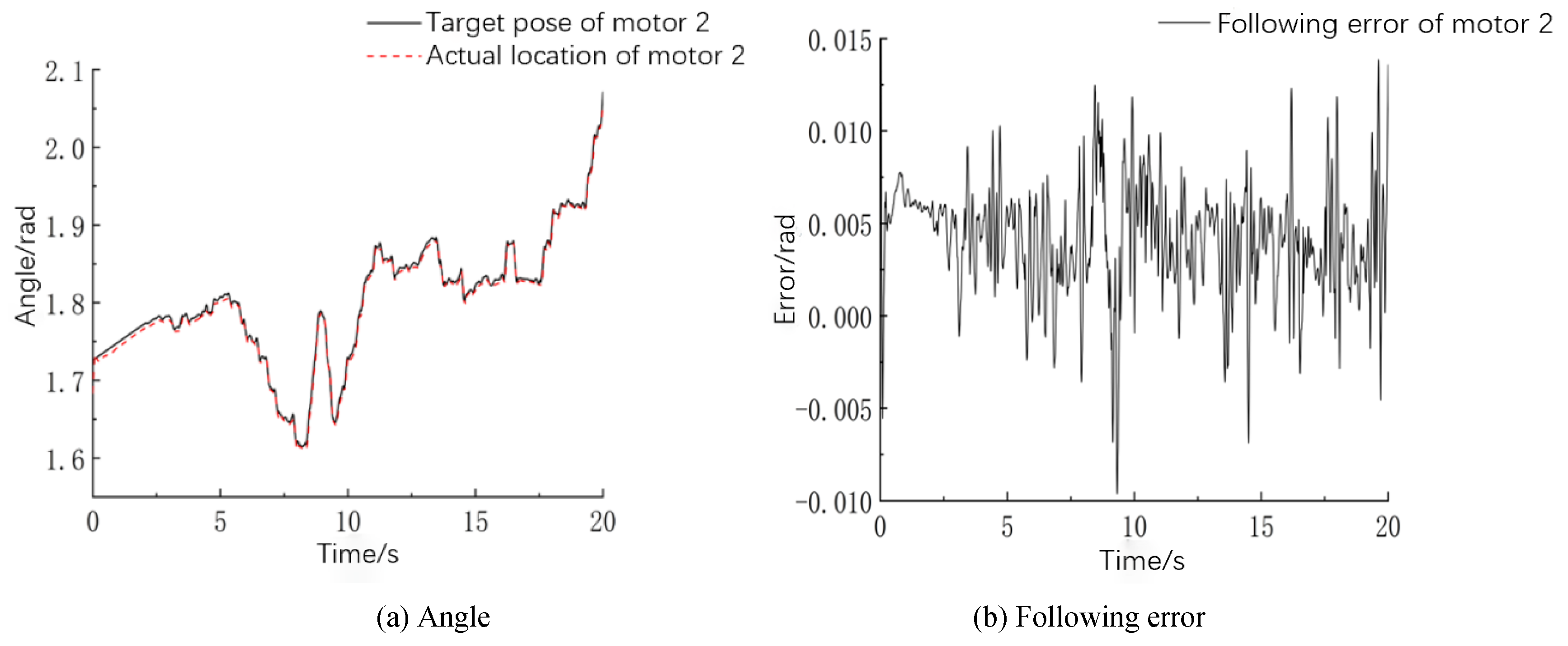
4.2. Experiment and Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Carlos, E.D.; Roemi, F.; Manuel, A. State of the art in robots used in minimally invasive surgeries. Natural Orifice Transluminal Surgery (NOTES) as a particular case. Ind. Robot 2015, 42, 508–532. [Google Scholar]
- Lum, M.J.H.; Rosen, J.; Sinanan, M.N.; Hannaford, B. Optimization of a spherical mechanism for a minimally invasive surgical robot: Theoretical and experimental approaches. IEEE Trans. Biomed. Eng. 2006, 53, 1440–1445. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Wang, T. Progress of Da Vinci robot in surgical operation of gastric cancer. J. Clin. Surg. 2020, 28, 991–994. [Google Scholar]
- Locke, R.C.O.; Patel, R.V. Optimal remote center-of-motion location for robotics-assisted minimally-invasive surgery. In Proceedings of the 2007 IEEE International Conference on Robotics and Automation, Rome, Italy, 10–14 April 2007; pp. 1900–1905. [Google Scholar]
- Hagn, U.; Nickl, M.; Stephan, J. The DLR MIRO: A versatile lightweight robot for surgical applications. Ind. Robot 2008, 35, 324–336. [Google Scholar] [CrossRef] [Green Version]
- Allett, S.G.; Rossitto, C.; Cianci, S. The Sen-hance™ surgical robotic system (‘Senhance’) for total hysterectomy in obese patients: A pilot study. J. Robot. Surg. 2017, 12, 229–234. [Google Scholar] [CrossRef]
- Aksungur, S.; Aydin, M.; Yakut, O. Real-time PID control of a novel RCM mechanism designed and manufactured for use in laparoscopic surgery. Ind. Robot 2019, 47, 153–166. [Google Scholar] [CrossRef]
- Kuo, C.H.; Dai, J.S.; Dasgupta, P. Kinematic design considerations for minimally invasive surgical robots: An overview. Int. J. Med. Robot. Comput. Assist. Surg. 2012, 8, 127–145. [Google Scholar] [CrossRef]
- Liu, S.T.; Harewood, L.; Chen, B.; Chen, C. A skeletal prototype of surgical arm based on dual-triangular mechanism. Mech. Robot. 2016, 8, 041015. [Google Scholar] [CrossRef]
- Guo, L.J.; Shi, H.; Mei, X.S. Implementation of fixed point of minimally invasive surgical robot: A survey. J. Adv. Manuf. Sci. Technol. 2021, 1, 2020003. [Google Scholar]
- Xue, R.F.; Du, Z.J.; Yan, Z.Y.; Ren, B.Y. An estimation method of grasping force for laparoscope surgical robot based on the model of a cable-pulley system. Mech. Mach. Theory 2019, 134, 440–454. [Google Scholar] [CrossRef]
- Jin, S.; Lee, S.K.; Lee, J.; Han, S. Kinematic model and real-time path generator for a wire-driven surgical robot arm with articulated joint structure. Appl. Sci. 2019, 9, 4114. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Wang, H.; Quan, L. Smooth point-to-point trajectory planning for industrial robots with kinematical constraints based on high-order polynomial curve. Mech. Mach. Theory 2019, 139, 284–293. [Google Scholar] [CrossRef]
- Zhao, B.L.; Nelson, C.A. Estimating tool–tissue forces using a 3 degree-of-freedom robotic surgical tool. J. Mech. Robot. 2016, 8, 051015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, P.; Neptune, R.R.; Deshpande, A.D. A simulation framework for virtual prototyping of robotic exoskeletons. Biomech. Eng. 2016, 138, 061004. [Google Scholar] [CrossRef] [PubMed]
- Kurc, K.; Szybicki, D.; Burghardt, A.; Muszyńska, M. The application of virtual prototyping methods to determine the dynamic parameters of mobile robot. Open Eng. 2016, 6, 55–63. [Google Scholar] [CrossRef]
- Yue, L.; Cao, Y.; Wang, S. Proportional coefficient analysis of master-slave robot system in workspace. Mech. Sci. Technol. 2007, 26, 803–807. [Google Scholar]
- Li, K.; Ji, S.; Niu, G.; Ai, Y.; Pan, B.; Fu, Y. Master-slave control and evaluation of force sensing for robot-assisted minimally invasive surgery. Ind. Robot Int. J. Robot. Res. Appl. 2020, 47, 903–914. [Google Scholar] [CrossRef]
- Guo, S.; Wang, Y.; Xiao, N. Study on real-time force feedback for a master–slave interventional surgical robotic system. Biomed. Microdevices 2018, 20, 37. [Google Scholar] [CrossRef]
- He, C.Y.; Huang, L.; Yang, Y. Research and realization of a master-slave robotic system for retinal vascular bypass surgery. Chin. J. Mech. Eng. 2018, 31, 78. [Google Scholar] [CrossRef]
- Yu, H.; Wang, H.; Chang, J.; Niu, J.; Wang, F.; Yan, Y.; Tian, H.; Fang, J.; Lu, H. A novel vascular intervention surgical robot based on force feedback and flexible clamping. Appl. Sci. 2021, 11, 611. [Google Scholar] [CrossRef]
- Du, Z.J.; Liang, Y.L.; Yan, Z.Y.; Sun, L.N.; Chen, W. Human-robot interaction control of a haptic master manipulator used in laparoscopic minimally invasive surgical robot system. Mech. Mach. Theory 2020, 156, 104132. [Google Scholar] [CrossRef]
- Li, J.; Shi, H.; Yang, L. Inverse kinematics analysis, size optimization and error analysis of urology surgical manipulator. In Proceedings of the IEEE Biomedical Engineering International Conference, Chiang Mai, Thailand, 21–24 November 2018. [Google Scholar]
- Niccolini, M.; Petroni, G.; Menciassi, A. Real-time control architecture of a novel single-port laparoscopy bimanual robot (SPRINT). In Proceedings of the IEEE International Conference on Robotics and Automation, Saint Paul, MN, USA, 14–18 May 2012; pp. 3395–3400. [Google Scholar]
- David, S.D.; Kwartowitz, M. Toward image-guided robotic surgery determining intrinsic accuracy of the da Vinci robot. Int. J. Comput. Assist. Radiol. Surg. 2006, 1, 157–165. [Google Scholar]




















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, H.; Liu, Q.; Mei, X. Accurate Parameter Estimation for Master–Slave Operation of a Surgical Robot. Machines 2021, 9, 213. https://doi.org/10.3390/machines9100213
Shi H, Liu Q, Mei X. Accurate Parameter Estimation for Master–Slave Operation of a Surgical Robot. Machines. 2021; 9(10):213. https://doi.org/10.3390/machines9100213
Chicago/Turabian StyleShi, Hu, Qingxin Liu, and Xuesong Mei. 2021. "Accurate Parameter Estimation for Master–Slave Operation of a Surgical Robot" Machines 9, no. 10: 213. https://doi.org/10.3390/machines9100213
APA StyleShi, H., Liu, Q., & Mei, X. (2021). Accurate Parameter Estimation for Master–Slave Operation of a Surgical Robot. Machines, 9(10), 213. https://doi.org/10.3390/machines9100213