
Reduced Plasma Ascorbate and Increased Proportion of Dehydroascorbic Acid Levels in Patients Undergoing Hemodialysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. Collection of Blood and Urine Samples
2.3. Determination of Ascorbate and DHA Levels
2.4. Study Items
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients with CKD Stage G3–G5 and Those Undergoing Hemodialysis
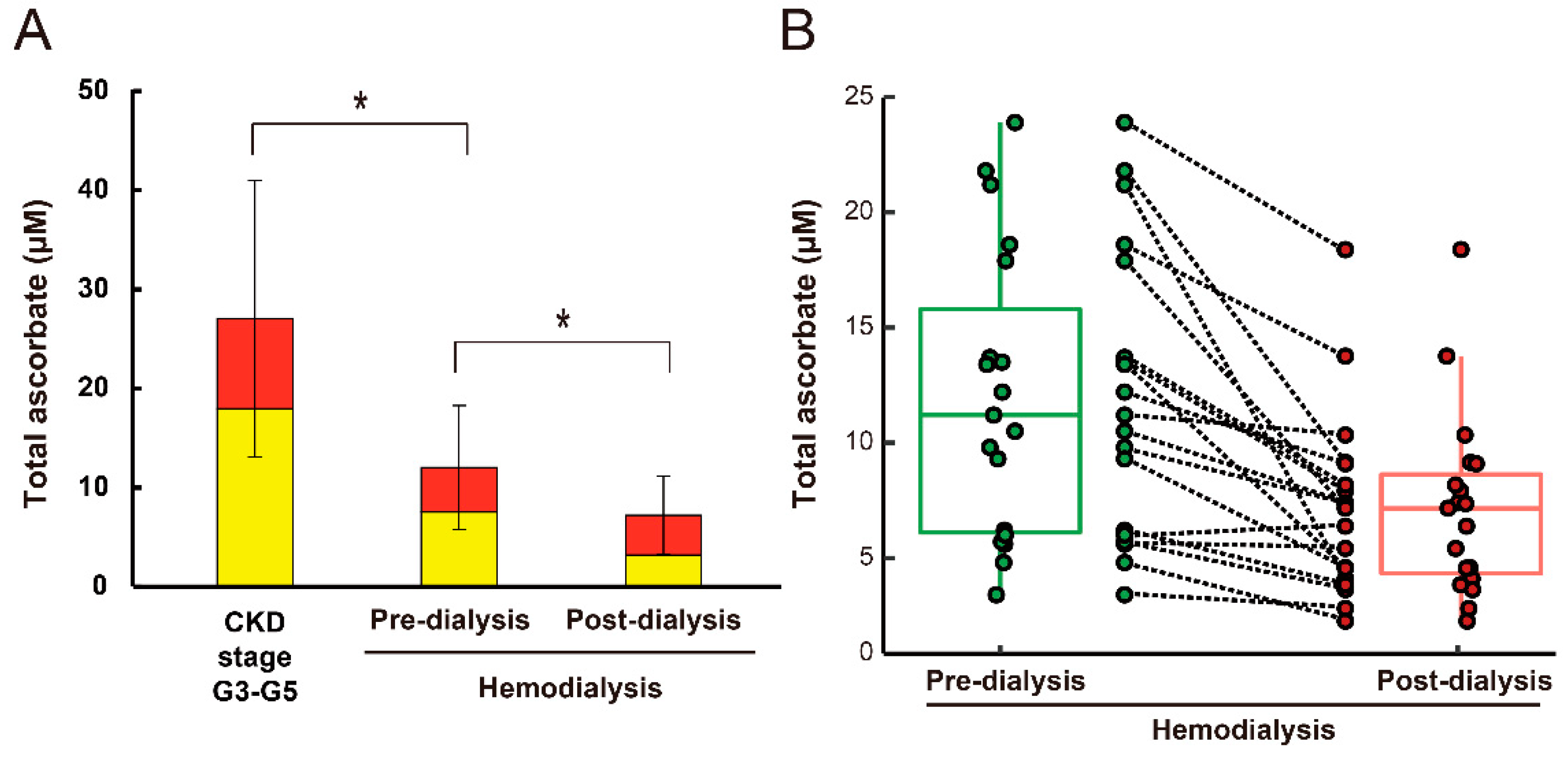
3.2. Plasma Ascorbate and DHA Levels in CKD Stage G3–G5 and Hemodialysis Patients
3.3. Pre- and Post-Dialysis Plasma Ascorbate and DHA Levels in Hemodialysis Patients
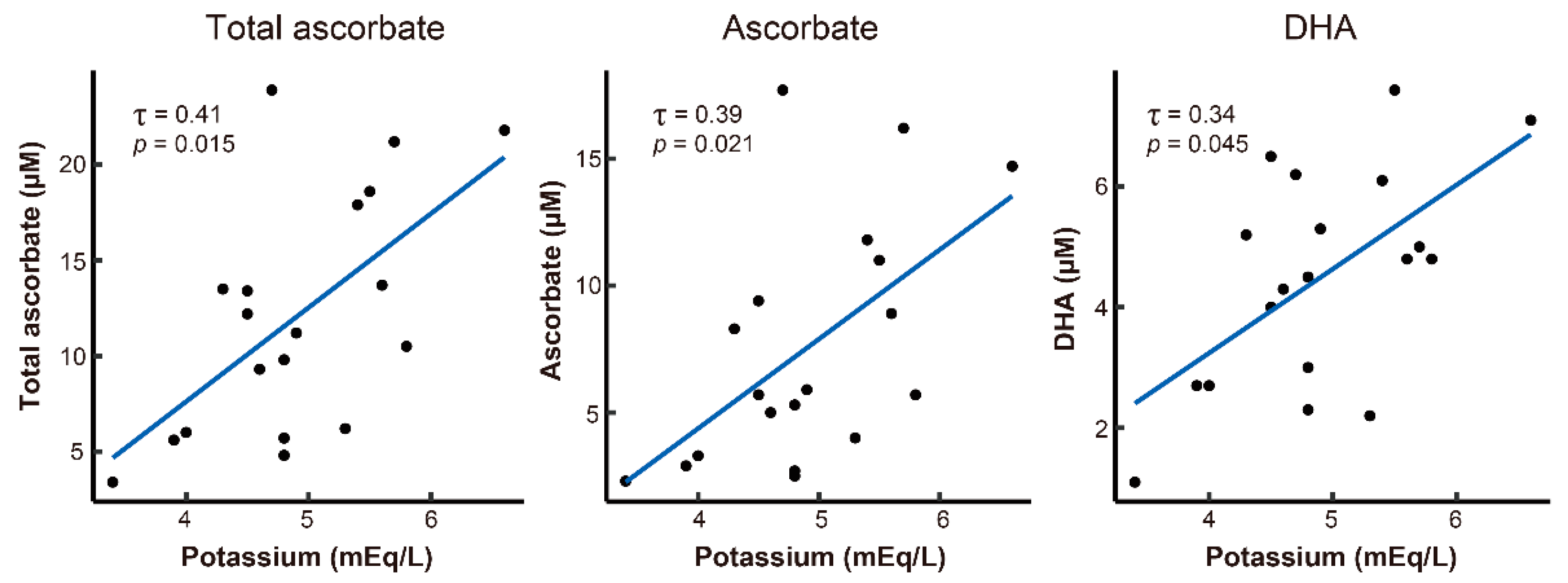
3.4. Relationships between Clinical Characteristics and Plasma Ascorbate and DHA Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| CKD stage G3–G5 (N = 27) | Total ascorbate | 27.1 ± 13.9 | |
| Ascorbate | 18.0 ± 12.8 | ||
| DHA | 9.1 ± 13.6 | ||
| Hemodialysis (N = 19) | Pre-dialysis | Total ascorbate | 12.0 ± 6.2 |
| Ascorbate | 7.5 ± 4.8 | ||
| DHA | 4.5 ± 1.8 | ||
| Post-dialysis | Total ascorbate | 7.2 ± 3.9 | |
| Ascorbate | 3.2 ± 2.8 | ||
| DHA | 4.0 ± 1.5 |
Appendix B

References
- Linster, C.L.; Van Schaftingen, E. Vitamin C: Biosynthesis, recycling and degradation in mammals. FEBS J. 2007, 274, 1–22. [Google Scholar] [CrossRef]
- Winterbourn, C.C. Reconciling the chemistry and biology of reactive oxygen species. Nat. Chem. Biol. 2008, 4, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Sasaki, T.; Sato, Y.; Amano, A.; Aizawa, S.; Iwama, M.; Handa, S.; Shimada, N.; Fukuda, M.; Akita, M.; et al. Vitamin C depletion increases superoxide generation in brains of SMP30/GNL knockout mice. Biochem. Biophys. Res. Commun. 2008, 377, 291–296. [Google Scholar] [CrossRef]
- Lane, D.J.; Lawen, A. Ascorbate and plasma membrane electron transport--enzymes vs efflux. Free Radic. Biol. Med. 2009, 47, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Mandl, J.; Szarka, A.; Banhegyi, G. Vitamin C: Update on physiology and pharmacology. Br. J. Pharmacol. 2009, 157, 1097–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amano, A.; Tsunoda, M.; Aigaki, T.; Maruyama, N.; Ishigami, A. Effect of ascorbic acid deficiency on catecholamine synthesis in adrenal glands of SMP30/GNL knockout mice. Eur. J. Nutr. 2014, 53, 177–185. [Google Scholar] [CrossRef]
- Furusawa, H.; Sato, Y.; Tanaka, Y.; Inai, Y.; Amano, A.; Iwama, M.; Kondo, Y.; Handa, S.; Murata, A.; Nishikimi, M.; et al. Vitamin C is not essential for carnitine biosynthesis in vivo: Verification in vitamin C-depleted senescence marker protein-30/gluconolactonase knockout mice. Biol. Pharm. Bull. 2008, 31, 1673–1679. [Google Scholar] [CrossRef] [Green Version]
- Sato, Y.; Uchiki, T.; Iwama, M.; Kishimoto, Y.; Takahashi, R.; Ishigami, A. Determination of dehydroascorbic acid in mouse tissues and plasma by using tris(2-carboxyethyl)phosphine hydrochloride as reductant in metaphosphoric acid/ethylenediaminetetraacetic acid solution. Biol. Pharm. Bull. 2010, 33, 364–369. [Google Scholar] [CrossRef] [Green Version]
- Kondo, Y.; Inai, Y.; Sato, Y.; Handa, S.; Kubo, S.; Shimokado, K.; Goto, S.; Nishikimi, M.; Maruyama, N.; Ishigami, A. Senescence marker protein 30 functions as gluconolactonase in L-ascorbic acid biosynthesis, and its knockout mice are prone to scurvy. Proc. Natl. Acad. Sci. USA 2006, 103, 5723–5728. [Google Scholar] [CrossRef] [Green Version]
- Nishikimi, M.; Koshizaka, T.; Ozawa, T.; Yagi, K. Occurrence in humans and guinea pigs of the gene related to their missing enzyme L-gulono-gamma-lactone oxidase. Arch. Biochem. Biophys. 1988, 267, 842–846. [Google Scholar] [CrossRef]
- Panchal, S.; Schneider, C.; Malhotra, K. Scurvy in a hemodialysis patient. Rare or ignored? Hemodial. Int. 2018, 22, S83–S87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimata, N.; Tsuchiya, K.; Akiba, T.; Nitta, K. Differences in the Characteristics of Dialysis Patients in Japan Compared with Those in Other Countries. Blood Purif. 2015, 40, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.F.; Eisenstein, A.B. Ascorbic acid depletion during hemodialysis. JAMA 1972, 220, 1697–1699. [Google Scholar] [CrossRef] [PubMed]
- Ponka, A.; Kuhlback, B. Serum ascorbic acid in patients undergoing chronic hemodialysis. Acta Med. Scand. 1983, 213, 305–307. [Google Scholar] [CrossRef] [PubMed]
- DeBari, V.A.; Frank, O.; Baker, H.; Needle, M.A. Water soluble vitamins in granulocytes, erythrocytes, and plasma obtained from chronic hemodialysis patients. Am. J. Clin. Nutr. 1984, 39, 410–415. [Google Scholar] [CrossRef] [Green Version]
- Papastephanidis, C.; Agroyannis, B.; Tzanatos-Exarchou, H.; Orthopoulos, B.; Koutsicos, D.; Frangos-Plemenos, M.; Kallitsis, M.; Yatzidis, H. Re-evaluation of ascorbic acid deficiency in hemodialysed patients. Int. J. Artif. Organs. 1987, 10, 163–165. [Google Scholar] [CrossRef]
- Wang, S.; Eide, T.C.; Sogn, E.M.; Berg, K.J.; Sund, R.B. Plasma ascorbic acid in patients undergoing chronic haemodialysis. Eur. J. Clin. Pharmacol. 1999, 55, 527–532. [Google Scholar] [CrossRef]
- Morena, M.; Cristol, J.P.; Bosc, J.Y.; Tetta, C.; Forret, G.; Leger, C.L.; Delcourt, C.; Papoz, L.; Descomps, B.; Canaud, B. Convective and diffusive losses of vitamin C during haemodiafiltration session: A contributive factor to oxidative stress in haemodialysis patients. Nephrol. Dial. Transplant. 2002, 17, 422–427. [Google Scholar] [CrossRef] [Green Version]
- Loughrey, C.M.; Young, I.S.; Lightbody, J.H.; McMaster, D.; McNamee, P.T.; Trimble, E.R. Oxidative stress in haemodialysis. QJM 1994, 87, 679–683. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- National Kidney, F. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Kodama, Y.; Kishimoto, Y.; Muramatsu, Y.; Tatebe, J.; Yamamoto, Y.; Hirota, N.; Itoigawa, Y.; Atsuta, R.; Koike, K.; Sato, T.; et al. Antioxidant nutrients in plasma of Japanese patients with chronic obstructive pulmonary disease, asthma-COPD overlap syndrome and bronchial asthma. Clin. Respir. J. 2017, 11, 915–924. [Google Scholar] [CrossRef] [PubMed]
- Clase, C.M.; Ki, V.; Holden, R.M. Water-soluble vitamins in people with low glomerular filtration rate or on dialysis: A review. Semin. Dial. 2013, 26, 546–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleicher, R.L.; Carroll, M.D.; Ford, E.S.; Lacher, D.A. Serum vitamin C and the prevalence of vitamin C deficiency in the United States: 2003-2004 National Health and Nutrition Examination Survey (NHANES). Am. J. Clin. Nutr. 2009, 90, 1252–1263. [Google Scholar] [CrossRef]
- Young, J.I.; Züchner, S.; Wang, G. Regulation of the Epigenome by Vitamin C. Annu. Rev. Nutr. 2015, 35, 545–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marik, P.E.; Liggett, A. Adding an orange to the banana bag: Vitamin C deficiency is common in alcohol use disorders. Crit. Care 2019, 23, 165. [Google Scholar] [CrossRef] [Green Version]
- Honore, P.M.; Spapen, H.D.; Marik, P.; Boer, W.; Oudemans-van Straaten, H. Dosing vitamin C in critically ill patients with special attention to renal replacement therapy: A narrative review. Ann. Intensive Care 2020, 10, 23. [Google Scholar] [CrossRef] [Green Version]
- Raimann, J.G.; Abbas, S.R.; Liu, L.; Larive, B.; Beck, G.; Kotanko, P.; Levin, N.W.; Handelman, G.; Trial, F.H.N. The effect of increased frequency of hemodialysis on vitamin C concentrations: An ancillary study of the randomized Frequent Hemodialysis Network (FHN) daily trial. BMC Nephrol. 2019, 20, 179. [Google Scholar] [CrossRef] [Green Version]
- Deicher, R.; Ziai, F.; Bieglmayer, C.; Schillinger, M.; Horl, W.H. Low total vitamin C plasma level is a risk factor for cardiovascular morbidity and mortality in hemodialysis patients. J. Am. Soc. Nephrol. 2005, 16, 1811–1818. [Google Scholar] [CrossRef]
- Elder, T.D.; Wyngaarden, J.B. The biosynthesis and turnover of oxalate in normal and hyperoxaluric subjects. J. Clin. Investig. 1960, 39, 1337–1344. [Google Scholar] [CrossRef] [Green Version]
- Morgan, S.H.; Purkiss, P.; Watts, R.W.; Mansell, M.A. Oxalate dynamics in chronic renal failure. Comparison with normal subjects and patients with primary hyperoxaluria. Nephron 1987, 46, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Machida, N.; Ogawa, T.; Oda, M.; Hokama, S.; Chinen, Y.; Uchida, A.; Morozumi, M.; Sugaya, K.; Motoyoshi, Y.; et al. Calcium oxalate saturation in dialysis patients with and without primary hyperoxaluria. Urol. Res. 2006, 34, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Rolton, H.A.; McConnell, K.M.; Modi, K.S.; Macdougall, A.I. The effect of vitamin C intake on plasma oxalate in patients on regular haemodialysis. Nephrol. Dial. Transplant. 1991, 6, 440–443. [Google Scholar] [CrossRef]
- Canavese, C.; Petrarulo, M.; Massarenti, P.; Berutti, S.; Fenoglio, R.; Pauletto, D.; Lanfranco, G.; Bergamo, D.; Sandri, L.; Marangella, M. Long-term, low-dose, intravenous vitamin C leads to plasma calcium oxalate supersaturation in hemodialysis patients. Am. J. Kidney Dis. 2005, 45, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Prier, M.; Carr, A.C.; Baillie, N. No Reported Renal Stones with Intravenous Vitamin C Administration: A Prospective Case Series Study. Antioxidants 2018, 7, 68. [Google Scholar] [CrossRef] [Green Version]
- Fujii, T.; Luethi, N.; Young, P.J.; Frei, D.R.; Eastwood, G.M.; French, C.J.; Deane, A.M.; Shehabi, Y.; Hajjar, L.A.; Oliveira, G.; et al. Effect of Vitamin C, Hydrocortisone, and Thiamine vs Hydrocortisone Alone on Time Alive and Free of Vasopressor Support Among Patients With Septic Shock: The VITAMINS Randomized Clinical Trial. JAMA 2020, 323, 423–431. [Google Scholar] [CrossRef]
- Tentori, F.; Blayney, M.J.; Albert, J.M.; Gillespie, B.W.; Kerr, P.G.; Bommer, J.; Young, E.W.; Akizawa, T.; Akiba, T.; Pisoni, R.L.; et al. Mortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2008, 52, 519–530. [Google Scholar] [CrossRef]
- Block, G.A.; Klassen, P.S.; Lazarus, J.M.; Ofsthun, N.; Lowrie, E.G.; Chertow, G.M. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J. Am. Soc. Nephrol. 2004, 15, 2208–2218. [Google Scholar] [CrossRef] [Green Version]
- Taniguchi, M.; Fukagawa, M.; Fujii, N.; Hamano, T.; Shoji, T.; Yokoyama, K.; Nakai, S.; Shigematsu, T.; Iseki, K.; Tsubakihara, Y.; et al. Serum phosphate and calcium should be primarily and consistently controlled in prevalent hemodialysis patients. Ther. Apher. Dial. 2013, 17, 221–228. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Kuwae, N.; Regidor, D.L.; Kovesdy, C.P.; Kilpatrick, R.D.; Shinaberger, C.S.; McAllister, C.J.; Budoff, M.J.; Salusky, I.B.; Kopple, J.D. Survival predictability of time-varying indicators of bone disease in maintenance hemodialysis patients. Kidney Int. 2006, 70, 771–780. [Google Scholar] [CrossRef] [Green Version]
- Floege, J.; Kim, J.; Ireland, E.; Chazot, C.; Drueke, T.; de Francisco, A.; Kronenberg, F.; Marcelli, D.; Passlick-Deetjen, J.; Schernthaner, G.; et al. Serum iPTH, calcium and phosphate, and the risk of mortality in a European haemodialysis population. Nephrol. Dial. Transplant. 2011, 26, 1948–1955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshikawa, M.; Takase, O.; Tsujimura, T.; Sano, E.; Hayashi, M.; Takato, T.; Hishikawa, K. Long-term effects of low calcium dialysates on the serum calcium levels during maintenance hemodialysis treatments: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 5310. [Google Scholar] [CrossRef] [Green Version]
- Ke, G.; Huang, J.; Zhu, Y.; Yang, J.; Zhang, Y.; Chen, L.; Hu, J.; Tao, S.; Hu, Y.; Yang, D.; et al. Effect of Ascorbic Acid on Mineral and Bone Disorders in Hemodialysis Patients: A Systematic Review and Meta-Analysis. Kidney Blood Press Res. 2018, 43, 1459–1471. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.L.; Chertow, G.M.; Jin, C.; Kutner, N.G. Significance of frailty among dialysis patients. J. Am. Soc. Nephrol. 2007, 18, 2960–2967. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Characteristic | CKD Stage G3-G5 (N = 27) | Hemodialysis (N = 19) |
|---|---|---|
| Age (years) | 83.9 ± 6.8 | 78.9 ± 10.9 |
| Sex (male/female) | 10/17 | 9/10 |
| White blood cell (×10³/μL) | M: 6.7 ± 1.8 | M: 6.5 ± 1.3 |
| F: 7.0 ± 1.7 | F: 7.1 ± 3.5 | |
| Hemoglobin (g/dL) | M: 12.1 ± 1.2 | M: 11.3 ± 0.6 |
| F: 11.8 ± 1.2 | F: 11.2 ± 0.8 | |
| Hematocrit (%) | M: 36.5 ± 3.9 | M: 34.3 ± 2.3 |
| F: 36.2 ± 3.0 | F: 35.1 ± 2.5 | |
| Platelet (×10⁴/μL) | M: 20.5 ± 6.3 | M: 23.8 ± 6.8 |
| F: 22.1 ± 5.8 * | F: 16.0 ± 6.0 | |
| Total protein (g/dL) | 6.9 ± 0.5 * | 6.3 ± 0.5 |
| Albumin (g/dL) | 3.6 ± 0.3 * | 3.1 ± 0.5 |
| C-reactive protein (mg/dL) | 0.4 ± 0.7 | 0.8 ± 2.4 |
| AST (IU/L) | 21.2 ± 5.1 * | 24.7 ± 36.4 |
| Blood urea nitrogen (mg/dL) | 32.9 ± 14.6 * | 62.7 ± 13.3 |
| Creatinine (mg/dL) | M: 2.0 ± 0.9 * | M: 10.4 ± 1.8 |
| F: 2.1 ± 1.0 * | F: 7.4 ± 1.3 | |
| Uric acid (mg/dL) | M: 6.0 ± 1.1 | M: 5.9 ± 1.5 |
| F: 6.3 ± 1.7 | F: 5.9 ± 1.6 | |
| Sodium (mEq/L) | 140.4 ± 3.5 * | 137.7 ± 3.6 |
| Potassium (mEq/L) | 4.4 ± 0.6 | 4.9 ± 0.8 |
| Calcium (mg/dL) | 9.1 ± 0.6 * | 8.5 ± 0.5 |
| Phosphorus (mg/dL) | 3.8 ± 0.7 * | 5.1 ± 1.3 |
| Triglyceride (mg/dL) | 150.9 ± 71.8 * | 108.7 ± 32.8 |
| Total cholesterol (mg/dL) | 200.9 ± 47.8 * | 152.8 ± 38.0 |
| LDL cholesterol (mg/dL) | 109.5 ± 34.7 * | 81.2 ± 26.7 |
| Iron (μg/dL) | M: 66.2 ± 13.8 | M: 62.8 ± 44.7 |
| F: 76.6 ± 28.1 * | F: 47.5 ± 16.8 | |
| TIBC (μg/dL) | M: 234.6 ± 16.3 | M: 251.7 ± 38.4 |
| F: 253.6 ± 35.5 | F: 230.9 ± 48.9 | |
| Ferritin (ng/dL) | M: 159.6 ± 86.2 | M:105.9 ± 83.5 |
| F: 177.2 ± 250.1 | F: 117.3 ± 79.4 | |
| β2-microglobulin (mg/L) | 5.1 ± 2.1 * | 27.0 ± 7.4 |
| Prealbumin (mg/dL) | 23.2 ± 5.6 | 24.1 ± 5.2 |
| HbA1c (%) | 6.1 ± 0.7 | 5.8 ± 0.7 |
| Total Ascorbate | Ascorbate | DHA | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | τ | p-Value | q-Value | τ | p-Value | q-Value | τ | p-Value | q-Value |
| Age | 0.31 | 0.063 | 0.588 | 0.33 | 0.049 * | 0.457 | 0.14 | 0.419 | 0.692 |
| Dry weight | 0.05 | 0.783 | 0.914 | 0.01 | 0.944 | 0.944 | −0.02 | 0.916 | 0.916 |
| White blood cell | −0.05 | 0.783 | 0.914 | −0.05 | 0.779 | 0.922 | −0.14 | 0.420 | 0.692 |
| Hemoglobin | 0.07 | 0.699 | 0.914 | 0.11 | 0.527 | 0.918 | −0.22 | 0.193 | 0.600 |
| Hematocrit | 0.09 | 0.599 | 0.914 | 0.17 | 0.326 | 0.803 | −0.21 | 0.220 | 0.611 |
| Platelet | −0.20 | 0.238 | 0.680 | −0.23 | 0.161 | 0.751 | −0.28 | 0.100 | 0.400 |
| Total Protein | 0.08 | 0.647 | 0.914 | 0.02 | 0.888 | 0.922 | 0.10 | 0.548 | 0.797 |
| Albumin | 0.16 | 0.350 | 0.817 | 0.12 | 0.495 | 0.918 | 0.36 | 0.044 * | 0.302 |
| C-reactive protein | −0.19 | 0.261 | 0.680 | −0.17 | 0.308 | 0.803 | −0.29 | 0.092 | 0.400 |
| AST | −0.19 | 0.260 | 0.680 | −0.25 | 0.149 | 0.751 | −0.06 | 0.725 | 0.872 |
| Blood urea nitrogen | 0.01 | 0.944 | 0.945 | 0.04 | 0.806 | 0.922 | 0.05 | 0.779 | 0.872 |
| Creatinine | −0.09 | 0.629 | 0.914 | −0.09 | 0.575 | 0.918 | −0.10 | 0.552 | 0.797 |
| Uric acid | −0.10 | 0.551 | 0.914 | −0.12 | 0.483 | 0.918 | −0.03 | 0.861 | 0.916 |
| Sodium | 0.13 | 0.458 | 0.914 | 0.12 | 0.480 | 0.918 | 0.20 | 0.243 | 0.611 |
| Potassium | 0.41 | 0.015 * | 0.420 | 0.39 | 0.021 * | 0.420 | 0.34 | 0.045 * | 0.302 |
| Calcium | −0.01 | 0.944 | 0.945 | −0.04 | 0.805 | 0.922 | −0.02 | 0.888 | 0.916 |
| Phosphorus | -0.05 | 0.752 | 0.914 | −0.08 | 0.623 | 0.918 | −0.08 | 0.648 | 0.825 |
| Triglyceride | 0.19 | 0.263 | 0.680 | 0.16 | 0.344 | 0.803 | 0.19 | 0.262 | 0.611 |
| Total cholesterol | 0.19 | 0.248 | 0.680 | 0.18 | 0.293 | 0.803 | 0.33 | 0.054 | 0.302 |
| LDL cholesterol | 0.08 | 0.624 | 0.914 | 0.09 | 0.599 | 0.918 | 0.15 | 0.362 | 0.676 |
| Iron | 0.23 | 0.172 | 0.680 | 0.20 | 0.233 | 0.803 | 0.34 | 0.046 * | 0.302 |
| TIBC | −0.19 | 0.267 | 0.680 | −0.19 | 0.263 | 0.803 | −0.17 | 0.310 | 0.620 |
| Ferritin | 0.27 | 0.107 | 0.680 | 0.26 | 0.115 | 0.751 | 0.26 | 0.123 | 0.431 |
| β2-microglobulin | −0.02 | 0.889 | 0.945 | −0.03 | 0.861 | 0.922 | −0.18 | 0.293 | 0.620 |
| Prealbumin | −0.06 | 0.776 | 0.914 | −0.07 | 0.711 | 0.922 | 0.10 | 0.592 | 0.797 |
| HbA1c | −0.07 | 0.699 | 0.914 | −0.07 | 0.673 | 0.922 | −0.09 | 0.598 | 0.797 |
| Parathyroid hormone | 0.02 | 0.945 | 0.945 | 0.02 | 0.889 | 0.922 | −0.05 | 0.753 | 0.872 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doshida, Y.; Itabashi, M.; Takei, T.; Takino, Y.; Sato, A.; Yumura, W.; Maruyama, N.; Ishigami, A. Reduced Plasma Ascorbate and Increased Proportion of Dehydroascorbic Acid Levels in Patients Undergoing Hemodialysis. Life 2021, 11, 1023. https://doi.org/10.3390/life11101023
Doshida Y, Itabashi M, Takei T, Takino Y, Sato A, Yumura W, Maruyama N, Ishigami A. Reduced Plasma Ascorbate and Increased Proportion of Dehydroascorbic Acid Levels in Patients Undergoing Hemodialysis. Life. 2021; 11(10):1023. https://doi.org/10.3390/life11101023
Chicago/Turabian StyleDoshida, Yuta, Mitsuyo Itabashi, Takashi Takei, Yuka Takino, Ayami Sato, Wako Yumura, Naoki Maruyama, and Akihito Ishigami. 2021. "Reduced Plasma Ascorbate and Increased Proportion of Dehydroascorbic Acid Levels in Patients Undergoing Hemodialysis" Life 11, no. 10: 1023. https://doi.org/10.3390/life11101023
APA StyleDoshida, Y., Itabashi, M., Takei, T., Takino, Y., Sato, A., Yumura, W., Maruyama, N., & Ishigami, A. (2021). Reduced Plasma Ascorbate and Increased Proportion of Dehydroascorbic Acid Levels in Patients Undergoing Hemodialysis. Life, 11(10), 1023. https://doi.org/10.3390/life11101023