
A Systematic Review of Systematic Reviews on the Epidemiology, Evaluation, and Treatment of Plantar Fasciitis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Systematic Review Regisrtation
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Data Extraction
2.6. Methodological Quality Evaluation
3. Results
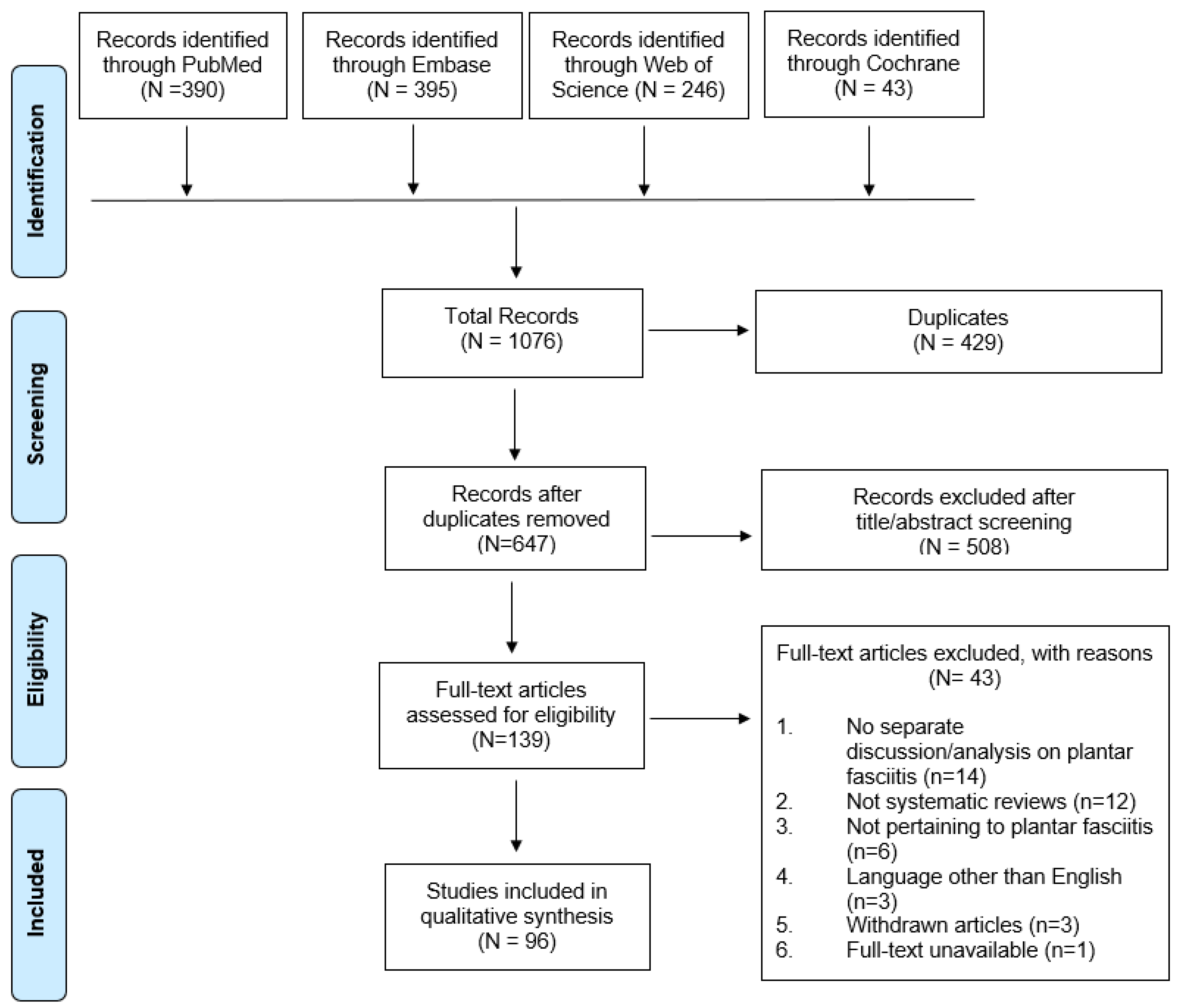
3.1. Eligible Studies
3.2. Methodological Quality Evaluation
3.3. Epidemiology
3.3.1. Prevalence/Incidence
3.3.2. Risk Factors
- Body mass index (BMI): The association between BMI and plantar fasciitis has been examined in multiple reviews. Butterworth et al. examined the association between body mass index (BMI) and musculoskeletal foot disorders and included 12 studies (nine matched case-control and three cross-sectional) on plantar fasciitis [20]. The authors found that while BMI was not associated with plantar fasciitis in the athletic population, there was evidence to support such an association in the non-athletic population [20]. Likewise, Franceschi et al. reported a strong association between increased body weight and plantar fasciitis based on four observational studies [21]. These results have been supported by other reviews that specifically investigated risk factors of plantar fasciitis, especially in non-athletic population [22,23,24].
- Weightbearing activities: Waclawski et al. specifically focused on adult workers and explored the association between weight-bearing activities (such as walking or standing) and plantar fasciitis [25]. The authors identified four studies and found that there was low-quality evidence to support an association between weight-bearing tasks and plantar fasciitis.
- Muscle function and size: Osborne et al. investigated muscle function and muscle size differences between those with and without plantar fasciitis [26]. Seven studies were included in this review, and the strength of muscle groups including hallux plantar flexion, lesser toe plantar flexion, ankle dorsiflexion, ankle inversion, and ankle eversion were lower in patients with plantar fasciitis. Foot muscle volume was also smaller in people with plantar fasciitis. However, there was no significant difference in calf muscle endurance between people with and without plantar fasciitis. The authors cautioned that these results are from studies with GRADE ratings suggesting strength of evidence rated as very low, and they concluded the role of muscle strength warrants further investigation.
- Kinematics: Mousavi et al. focused on distance runners with aims to identify kinematic risk factors for lower limb tendinopathy [27]. The authors included two studies that compared kinematic data of runners suffering from plantar fasciitis with healthy runners and found no significant difference between the two groups. However, another review concluded that decreased ankle dorsiflexion and decreased first metatarsophalangeal joint extension were weakly associated with plantar fasciitis [22]. The most recent review by Hamstra-Wright et al. investigated 16 studies focusing on physically active individuals and identified that increased plantarflexion range of motion was a risk factor [24]. Other biomechanical aspects such as ground reaction forces did not have sufficient studies to draw conclusions.
- Others: A review published in 2006 included 16 articles and found that the presence of a calcaneal spur were consistently associated with plantar fasciitis, and weaker associations for increased age, and prolonged standing [22]. These findings were echoed by van Leeuwen et al. who identified 51 articles, evaluated a total of 104 variables, and conducted a meta-analysis for 12 variables [23]. These authors found that patients with plantar fasciitis were more likely to have increased plantar fascia thickness, hypoechogenicity, and subcalcaneal spurs primarily identified on ultrasound and X-ray.
3.4. Diagnosis
3.5. Treatments
3.5.1. Corticosteroid
3.5.2. Platelet-Rich Plasma (PRP)
3.5.3. PRP vs. Corticosteroid
3.5.4. Extracorporeal Shockwave Therapy (ESWT)
3.5.5. Mechanical Treatments
- Insoles: Six reviews investigated the effects of insoles in the treatment of plantar fasciitis with mixed findings. Lee et al. performed a meta-analysis of 6 RCTs and cohort studies evaluating the effect of insole interventions in patients with a clinical diagnosis of plantar fasciitis. The authors found significant improvements in both pain and function in patients using insole orthotic devices in short (less than 6 weeks), medium (6–12 weeks), and long terms (more than 12 weeks) [72]. Two systematic analyses similarly reported favorable findings for insole use [73,74]. In contrast, four studies reported limited or no benefits from insoles compared to other interventions [75,76,77,78]. Hawke et al. conducted a meta-analysis of 5 RCTs and found significant improvements in function, but not pain, for custom versus sham orthotics after 12 weeks. They also concluded that custom orthotics were less effective in improving pain and function than treatments consisting of manipulation, mobilizations, and stretching at 2 weeks but there were no differences after 2 weeks between the groups [75]. Whittaker et al. conducted a similar systematic review with meta-analyses of 19 RCTs and found significant differences in pain relief when comparing sham versus true orthotics; conversely, potential benefits were observed in sham condition in the medium term (6–12 weeks), with differences not meeting minimally clinically significant values when back-transformed to the pain subscale of the Foot Health Status Questionnaire [76]. Rasenburg et al. reported similar findings and concluded that insoles were not superior for improving pain, function, or self-reported recovery compared to other conservative interventions across 20 RCTs [77]. Healy et al. also suggested that the lack of high-quality studies precluded any conclusions about orthotic interventions’ effectiveness and cost-effectiveness in treating plantar fasciitis [78].
- Four studies specifically investigated the effects of custom versus prefabricated insole orthotics [73,75,76,77]. Three of four found minor or no improvements in pain and function for prefabricated versus custom orthoses, custom versus sham orthoses, and prefabricated versus sham orthoses. Three studies also examined the effects of orthotics versus night splints [75,76,77]. All three reported no differences in pain reduction, although Hawke et al. found a significant improvement with combined use versus individual use of either device.
- Taping: Two systematic reviews explored the use of taping as an intervention for patients with plantar fasciitis [79,80]. Podolsky et al. reported Low Dye taping was the most commonly used technique across eight different studies followed by calcaneal taping. While taping may be a beneficial technique in improving pain in the short term (less than 1 week), authors could not draw conclusions for longer term outcomes as the longest follow-up was only one week among the included studies [79]. Van de Water et al. reported similar findings, with limited evidence favoring Low Dye and calcaneal taping versus sham interventions for improving pain, but not function, after 1 week [80]. The authors also noted that a combined intervention of taping and stretching may be superior to stretching alone. Both studies could not perform quantitative synthesis due to the heterogeneity of methods in their included studies.
- Mixed treatment: Schuitema et al. conducted a systematic review of 43 studies to investigate the effects of various commonly used mechanical interventions in the treatment of plantar fasciitis, including foot orthotics, taping, ankle foot orthoses, night splints, and specialized shoes [74]. The authors suggested that mechanical treatments overall may be beneficial in symptom reduction. However, the authors added that methodological limitations of included studies prevented them from making any comparisons between them regarding relative effectiveness and frequent use of non-mechanical co-interventions also confounds interpretation of role of each intervention.
3.5.6. Needling Therapies
- Acupuncture: Two systematic reviews investigated the use of acupuncture in the treatment of plantar fasciitis [81,82]. Both concluded that acupuncture therapies were associated with symptom reduction over outcome measures obtained 1–6 months although each cited significant heterogeneity of methods amongst their included studies as a major limitation.
- Dry needling: Two studies investigated the use of dry needling in the treatment of plantar fasciitis [83,84]. Cotchett et al. conducted a systematic review of three quasi-experimental studies and found limited evidence favoring the use of dry needling and poor quality of included studies [83]. He et al. conducted a meta-analysis of 7 RCTs published seven years after Cotchett et al., and compared trigger point dry needling or acupuncture to other interventions [84]. The authors concluded that myofascial trigger point needling was associated with significantly greater reductions in pain in at 1, 6, and 12 months. However, they reported substantial heterogeneity of methods, poor quality, and small sample sizes inherent in their included studies.
3.5.7. Low-Level Laser Therapy (LLLT)
3.5.8. Exercise Therapy
- Strengthening exercise: Only one study examined the effects of strengthening interventions on plantar fasciitis [87]. Huffer et al., who conducted a systematic review of seven studies, classified strengthening interventions into three distinct categories—minimalist running shoe intrinsic foot muscle (IFM) strengthening, IFM foot exercises, and plantar aponeurosis loading. While the authors found that these minimalist running shoes and toe flexion against resistance may improve intrinsic foot musculature in asymptomatic populations, high-load plantar fascia resistance training has not been shown to change plantar fascia thickness. Therefore, reviews determined no definitive conclusions regarding the benefits of strengthening interventions in patients with plantar fasciitis could be made.
- Stretching: Three studies investigated the effects of stretching in the treatment of plantar fasciitis [88,89,90]. Sweeting et al. conducted a systematic review of six studies comparing stretching with other conservative treatments or without intervention/natural history [88]. Patients who received stretching interventions seemed to improve over time in both pain and function, especially in the first two weeks to four months. However, the reviewers concluded that there were no significant differences between stretching and other interventions. They also noted that their study was limited by the large degree of heterogeneity in techniques, dosages, and comparison groups between individual studies, which made it difficult to comment on the relative effectiveness of different stretching regimens. Woitzik et al. conducted a systematic review of six RCTs investigating the effects of exercise on clinical outcomes in various soft tissue injuries of the lower extremities [90]. Of these, two studies that focused on plantar heel pain provided preliminary evidence supporting the use of static plantar fascia stretching in improving pain and function, but no support for static calf stretching. These findings were largely consistent with report by Siriphorn et al. who conducted a systematic review with meta-analysis of eight RCTs and found that there was moderate quality evidence in favor of plantar fascia-specific stretching (PFSS) over the Achilles tendon or calf stretching (CS) reducing pain in the short term (less than 3 months [89].
3.5.9. Manual Therapy
3.5.10. Prolotherapy
3.5.11. Iontophoresis
3.5.12. Endoscopic Plantar Fasciotomy
3.6. Comparative Evaluation of Multiple Treatments
3.7. Psychosocial Variables
4. Discussion
Future Research Direction
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Author/Year | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Item 12 | Item 13 | Item 14 | Item 15 | Item 16 | Overall Assessment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Agyekum 2015 | Yes | No | No | No | No | No | No | No | No | No | N/A | N/A | No | No | N/A | No | Critically low |
| Al-Abbad 2020 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Low |
| Al-Boloushi 2019 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | N/A | N/A | No | Yes | N/A | Yes | Critically low |
| Alkhatib 2020 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Critically low |
| Andia 2015 | Yes | No | Yes | No | No | No | No | Partial Yes | No | No | N/A | N/A | No | Yes | N/A | Yes | Critically low |
| Aqil 2013 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Partial Yes | No | Yes | No | No | Yes | No | Yes | Critically low |
| Assad 2016 | Yes | No | No | Partial Yes | No | No | No | Partial Yes | No | No | N/A | N/A | No | No | N/A | Yes | Critically low |
| Atkins 1999 | Yes | No | Yes | Partial Yes | No | Yes | No | Partial Yes | Partial Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Critically low |
| Babatunde 2019 | Yes | Yes | No | Partial Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| Brantingham 2012 | Yes | No | Yes | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | N/A | N/A | Yes | No | N/A | Yes | Critically low |
| Butterworth 2012 | Yes | No | Yes | Partial Yes | Yes | Yes | Yes | Partial yes | Partial Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Low |
| Chang 2012 | Yes | No | Yes | Partial Yes | Yes | Yes | No | Parial Yes | Partial Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Chen 2018 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Partial Yes | No | Yes | No | No | No | No | Yes | Critically low |
| Chen 2019 | Yes | No | Yes | Partial Yes | Yes | No | No | Partial Yes | Partial Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Critically low |
| Chiew 2016 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Partial Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Critically low |
| Clar 2014 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | Yes | N/A | N/A | Yes | Yes | N/A | Yes | Critically low |
| Clark 2012 | Yes | Yes | No | Partial Yes | No | No | No | Partial Yes | Partial Yes | Yes | N/A | N/A | Yes | Yes | N/A | Yes | Low |
| Clijsen 2012 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | N/A | Yes | Critically low |
| Cotchett 2010 | Yes | No | Yes | Partial Yes | Yes | Yes | Yes | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Low |
| David 2017 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Dizon 2013 | Yes | No | Yes | Partial Yes | No | No | No | Partial Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | Critically low |
| Dos Santos 2019 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Drake 2018 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Low |
| Franceschi 2014 (PRP) | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | No | No | N/A | N/A | No | Yes | N/A | Yes | Critically low |
| Franceschi 2015 | Yes | No | Yes | Partial Yes | Yes | Yes | No | Partial Yes | No | No | N/A | N/A | No | Yes | N/A | Yes | Critically low |
| Franchini 2018 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | No | Yes | Critically low |
| Fraser 2018 | Yes | Yes | No | Partial Yes | No | No | No | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Critically low |
| Fusini 2017 | Yes | No | No | Partial Yes | Yes | No | No | Partial Yes | No | No | N/A | N/A | No | No | N/A | No | Critically low |
| Hamstra-Wright 2021 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | No | Yes | Yes | No | No | Yes | No | Yes | Critically low |
| Hawke 2008 | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| He 2017 | Yes | No | No | Partial Yes | Yes | No | Yes | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Healy 2018 | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | High |
| Hohmann 2020 | Yes | No | No | Partial Yes | Yes | No | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Critically low |
| Hsiao 2015 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Partial Yes | No | Yes | No | No | Yes | Yes | Yes | Critically low |
| Huang 2020 | Yes | Yes | No | Partial Yes | Yes | No | No | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Huffer 2017 | Yes | Yes | No | Partial Yes | No | No | No | Partial Yes | Partial Yes | No | N/A | N/A | No | Yes | N/A | Yes | Critically low |
| Hurley 2020 | Yes | No | No | Partial Yes | Yes | Yes | No | Patial Yes | Yes | No | Yes | No | Yes | Yes | No | Yes | Critically low |
| Irving 2006 | Yes | No | Yes | Partial Yes | Yes | No | No | Partial Yes | Partial Yes | No | N/A | N/A | No | Yes | N/A | No | Critically low |
| Lee 2009 | Yes | No | No | Partial Yes | Yes | No | No | Partial Yes | Yes | No | No | No | Yes | Yes | No | Yes | Critically low |
| Li 2013 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Partial Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Li 2014 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Critically low |
| Li 2015 | Yes | No | No | Partial Yes | No | Yes | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Critically low |
| S Li 2018 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Critically low |
| X Li 2018 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| H Li 2018 | Yes | No | No | Partial Yes | Yes | No | No | Yes | No | No | Yes | No | No | Yes | Yes | Yes | Critically low |
| Li 2019 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Ling 2018 | Yes | No | No | Partial Yes | No | Yes | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Critically low |
| Lou 2017 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Malahias 2020 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | No | No | N/A | N/A | No | Yes | N/A | Yes | Critically low |
| Mao 2019 | Yes | No | No | Partial Yes | Yes | No | No | Partial Yes | No | No | No | No | No | Yes | No | Yes | Critically low |
| McMillan 2009 | Yes | Yes | No | Partial Yes | No | Yes | Yes | Partial Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Moderate |
| Mendes 2020 | Yes | Yes | No | Partial Yes | Yes | No | No | Partial Yes | Yes | No | N/A | N/A | No | No | N/A | Yes | Critically low |
| Mischke 2017 | Yes | No | No | Partial Yes | Yes | No | No | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Critically low |
| Mohammed 2020 | Yes | Yes | No | Partial Yes | No | Yes | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Low |
| Mohseni-Bandpei 2014 | Yes | No | No | Partial Yes | Yes | No | No | Partial Yes | Partial Yes | No | N/A | N/A | No | No | N/A | No | Critically low |
| Mousavi 2019 | Yes | No | No | Partial Yes | Yes | No | No | Partial Yes | Yes | No | Yes | No | No | No | No | Yes | Critically low |
| Ogden 2002 | Yes | No | No | No | No | No | No | No | No | No | No | No | No | No | No | No | Critically low |
| Osborne 2019 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | No | Yes | Critically low |
| Petragila 2017 | Yes | No | No | Partial Yes | No | Yes | No | Partial Yes | No | No | N/A | N/A | No | No | N/A | No | Critically low |
| Philips 2017 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Critically low |
| Piper 2016 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | N/A | N/A | No | No | N/A | Yes | Critically low |
| Podolsky 2015 | Yes | No | No | Partial Yes | No | No | No | Partial Yes | Yes | No | N/A | N/A | No | Yes | N/A | Yes | Critically low |
| Radwan 2016 | Yes | No | No | Partial Yes | Yes | No | No | Partial Yes | Yes | Yes | N/A | N/A | No | Yes | N/A | No | Critically low |
| Rasenberg 2018 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Roerdink 2017 | Yes | No | No | Partial Yes | Yes | Yes | No | Yes | No | No | N/A | N/A | Yes | Yes | N/A | Yes | Critically low |
| Salvioli 2017 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | No | Yes | Critically low |
| Sanderson 2015 | Yes | No | No | Partial Yes | No | No | Yes | Partial Yes | Partial Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Low |
| Schuitema 2020 | Yes | No | No | Partial Yes | Yes | No | No | Partial Yes | Yes | Yes | N/A | N/A | Yes | Yes | N/A | Yes | Critically low |
| Sheth 2012 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Partial Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Critically low |
| Singh 2017 | Yes | Yes | No | Partial Yes | No | Yes | No | Partial Yes | Partial Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Siriphorn 2020 | Yes | Yes | No | Partial Yes | No | No | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Low |
| Speed 2013 | Yes | No | Yes | Partial Yes | No | No | No | Partial Yes | No | No | N/A | N/A | No | Yes | N/A | Yes | Critically low |
| Sun 2017 | Yes | No | No | Partial Yes | No | Yes | Yes | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Sun 2020 | Yes | No | Yes | Partial Yes | Yes | Yes | No | No | Yes | No | Yes | No | Yes | No | No | Yes | Critically low |
| Sutton 2016 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Low |
| Sweeting 2011 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Critically low |
| Thiagarajah 2017 | Yes | No | No | Partial Yes | No | No | No | Partial Yes | Yes | No | N/A | N/A | No | Yes | N/A | No | Critically low |
| Thomson 2005 | Yes | No | No | Partial Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Tseng 2020 | Yes | Yes | Yes | Partial Yes | Yes | No | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
| Tsikopoulos 2016 (AWB) | Yes | Yes | No | Partial Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Low |
| Tsikopoulos 2016 (NMA)) | Yes | Yes | No | Partial Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Uden 2011 | Yes | No | Yes | Partial Yes | Yes | Yes | Yes | Partial Yes | Yes | No | N/A | N/A | Yes | No | N/A | Yes | Low |
| Van de Water 2010 | Yes | No | No | Partial Yes | Yes | Yes | Yes | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Low |
| Van Leeuwen 2016 | Yes | Partial Yes | Yes | Partial Yes | Yes | Yes | No | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Low |
| Vannini 2014 | Yes | No | No | No | No | No | No | Partial Yes | No | No | N/A | N/A | No | Yes | N/A | Yes | Critically low |
| Waclawski 2015 | Yes | Partial Yes | No | Partial Yes | Yes | No | Partial Yes | Partial Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Moderate |
| Wang 2019 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | No | Yes | Critically low |
| Wang 2019 (Laser) | Yes | No | No | Partial Yes | No | Yes | No | Partial Yes | Yes | No | Yes | No | No | No | Yes | Yes | Critically low |
| Whittaker 2017 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Critically low |
| Whittaker 2019 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Woitzik 2015 | Yes | Yes | No | Partial Yes | Yes | Yes | No | Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | Low |
| Xiong 2019 | Yes | No | No | Partial Yes | Yes | Yes | No | Partial Yes | Yes | No | Yes | No | No | Yes | No | Yes | Critically low |
| Yang 2017 | Yes | No | No | Partial Yes | No | Yes | No | Partial Yes | Yes | No | Yes | No | No | Yes | No | Yes | Critically low |
| Yin 2014 | Yes | No | No | Partial Yes | No | Yes | No | Partial Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Critically low |
| Yu 2016 | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | No | N/A | N/A | Yes | Yes | N/A | Yes | High |
| Yu 2020 (PRP) | Yes | No | No | Partial Yes | No | No | No | Partial Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | Critically low |
References
- López-López, D.; Pérez-Ríos, M.; Ruano-Ravina, A.; Losa-Iglesias, M.E.; Becerro-de-Bengoa-Vallejo, R.; Romero-Morales, C.; Calvo-Lobo, C.; Navarro-Flores, E. Impact of quality of life related to foot problems: A case-control study. Sci. Rep. 2021, 11, 14515. [Google Scholar] [CrossRef]
- Dunn, J.E.; Link, C.L.; Felson, D.T.; Crincoli, M.G.; Keysor, J.J.; McKinlay, J.B. Prevalence of foot and ankle conditions in a multiethnic community sample of older adults. Am. J. Epidemiol. 2004, 159, 491–498. [Google Scholar] [CrossRef]
- Hill, C.L.; Gill, T.K.; Menz, H.B.; Taylor, A.W. Prevalence and correlates of foot pain in a population-based study: The North West Adelaide health study. J. Foot Ankle Res. 2008, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Riddle, D.L.; Schappert, S.M. Volume of ambulatory care visits and patterns of care for patients diagnosed with plantar fasciitis: A national study of medical doctors. Foot Ankle Int. 2004, 25, 303–310. [Google Scholar] [CrossRef]
- Sobhani, S.; Dekker, R.; Postema, K.; Dijkstra, P.U. Epidemiology of ankle and foot overuse injuries in sports: A systematic review. Scand. J. Med. Sci. Sports 2013, 23, 669–686. [Google Scholar] [CrossRef]
- Lopes, A.D.; Hespanhol Júnior, L.C.; Yeung, S.S.; Costa, L.O. What are the main running-related musculoskeletal injuries? A Systematic Review. Sports Med. 2012, 42, 891–905. [Google Scholar] [CrossRef]
- Wearing, S.C.; Smeathers, J.E.; Urry, S.R.; Hennig, E.M.; Hills, A.P. The pathomechanics of plantar fasciitis. Sports Med. 2006, 36, 585–611. [Google Scholar] [CrossRef]
- Ostermann, S.; Olesen, J.L.; Holden, S.; Riel, H. Stretching and relaxing the plantar fascia may change plantar fascia thickness but not pressure pain thresholds: A cross-sectional study of patients with plantar fasciopathy. BMC Musculoskelet. Disord. 2020, 21, 804. [Google Scholar] [CrossRef]
- Melo, S.N.S.; Ezekwesili, A.; Yurdi, N.A.; Murrell, W.D.; Maffulli, N. Gold-Induced Cytokine (GOLDIC(®)) Injection Therapy in Patient with Plantar Fasciosis: A Case Report. Indian J. Orthop. 2020, 54, 348–351. [Google Scholar] [CrossRef]
- Babatunde, O.O.; Legha, A.; Littlewood, C.; Chesterton, L.S.; Thomas, M.J.; Menz, H.B.; van der Windt, D.; Roddy, E. Comparative effectiveness of treatment options for plantar heel pain: A systematic review with network meta-analysis. Br. J. Sports Med. 2019, 53, 182–194. [Google Scholar] [CrossRef] [Green Version]
- David, J.A.; Sankarapandian, V.; Christopher, P.R.; Chatterjee, A.; Macaden, A.S. Injected corticosteroids for treating plantar heel pain in adults. Cochrane Database Syst. Rev. 2017, 6, Cd009348. [Google Scholar] [CrossRef]
- Schepsis, A.A.; Leach, R.E.; Gorzyca, J. Plantar fasciitis. Etiology, treatment, surgical results, and review of the literature. Clin. Orthop. Relat. Res. 1991, 266, 185–196. [Google Scholar]
- Klein, S.E.; Dale, A.M.; Hayes, M.H.; Johnson, J.E.; McCormick, J.J.; Racette, B.A. Clinical presentation and self-reported patterns of pain and function in patients with plantar heel pain. Foot Ankle Int. 2012, 33, 693–698. [Google Scholar] [CrossRef] [Green Version]
- Yi, T.I.; Lee, G.E.; Seo, I.S.; Huh, W.S.; Yoon, T.H.; Kim, B.R. Clinical characteristics of the causes of plantar heel pain. Ann. Rehabil. Med. 2011, 35, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Karhade, A.V.; Kwon, J.Y. Trends in Foot and Ankle Studies Published in High-Impact General Medical Journals: A Systematic Review. J. Foot Ankle Surg. 2019, 58, 540–544. [Google Scholar] [CrossRef]
- Smith, V.; Devane, D.; Begley, C.M.; Clarke, M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Agyekum, E.K.; Ma, K. Heel pain: A systematic review. Chin. J. Traumatol. 2015, 18, 164–169. [Google Scholar] [CrossRef]
- Butterworth, P.A.; Landorf, K.B.; Smith, S.E.; Menz, H.B. The association between body mass index and musculoskeletal foot disorders: A systematic review. Obes. Rev. 2012, 13, 630–642. [Google Scholar] [CrossRef]
- Franceschi, F.; Papalia, R.; Paciotti, M.; Franceschetti, E.; Di Martino, A.; Maffulli, N.; Denaro, V. Obesity as a risk factor for tendinopathy: A systematic review. Int. J. Endocrinol. 2014, 2014, 670262. [Google Scholar] [CrossRef]
- Irving, D.B.; Cook, J.L.; Menz, H.B. Factors associated with chronic plantar heel pain: A systematic review. J. Sci. Med. Sport 2006, 9, 11–22. [Google Scholar] [CrossRef]
- van Leeuwen, K.D.; Rogers, J.; Winzenberg, T.; van Middelkoop, M. Higher body mass index is associated with plantar fasciopathy/‘plantar fasciitis’: Systematic review and meta-analysis of various clinical and imaging risk factors. Br. J. Sports Med. 2016, 50, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Hamstra-Wright, K.L.; Huxel Bliven, K.C.; Bay, R.C.; Aydemir, B. Risk Factors for Plantar Fasciitis in Physically Active Individuals: A Systematic Review and Meta-Analysis. Sports Health 2021, 13, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Waclawski, E.R.; Beach, J.; Milne, A.; Yacyshyn, E.; Dryden, D.M. Systematic review: Plantar fasciitis and prolonged weight bearing. Occup. Med. 2015, 65, 97–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osborne, J.W.A.; Menz, H.B.; Whittaker, G.A.; Landorf, K.B. Muscle Function and Muscle Size Differences in People with and without Plantar Heel Pain: A Systematic Review. J. Orthop. Sports Phys. Ther. 2019, 49, 925–933. [Google Scholar] [CrossRef]
- Mousavi, S.H.; Hijmans, J.M.; Rajabi, R.; Diercks, R.; Zwerver, J.; van der Worp, H. Kinematic risk factors for lower limb tendinopathy in distance runners: A systematic review and meta-analysis. Gait Posture 2019, 69, 13–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMillan, A.M.; Landorf, K.B.; Barrett, J.T.; Menz, H.B.; Bird, A.R. Diagnostic imaging for chronic plantar heel pain: A systematic review and meta-analysis. J. Foot Ankle Res. 2009, 2, 32. [Google Scholar] [CrossRef] [Green Version]
- Mohseni-Bandpei, M.A.; Nakhaee, M.; Mousavi, M.E.; Shakourirad, A.; Safari, M.R.; Vahab Kashani, R. Application of ultrasound in the assessment of plantar fascia in patients with plantar fasciitis: A systematic review. Ultrasound Med. Biol. 2014, 40, 1737–1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radwan, A.; Wyland, M.; Applequist, L.; Bolowsky, E.; Klingensmith, H.; Virag, I. Ultrasonography, an effective tool in diagnosing plantar fasciitis: A systematic review of diagnostic trials. Int. J. Sports Phys. Ther. 2016, 11, 663–671. [Google Scholar]
- Fusini, F.; Langella, F.; Busilacchi, A.; Tudisco, C.; Gigante, A.; Massé, A.; Bisicchia, S. Real-time sonoelastography: Principles and clinical applications in tendon disorders. A systematic review. Muscles Ligaments Tendons J. 2017, 7, 467–477. [Google Scholar] [CrossRef]
- Petraglia, F.; Ramazzina, I.; Costantino, C. Plantar fasciitis in athletes: Diagnostic and treatment strategies. a systematic review. Muscles Ligaments Tendons J. 2017, 7, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Yu, A.; Qi, B.; Zhao, Y.; Wang, W.; Li, P.; Ding, J. Corticosteroid versus placebo injection for plantar fasciitis: A meta-analysis of randomized controlled trials. Exp. Ther. Med. 2015, 9, 2263–2268. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.-M.; Lee, M.; Lin, C.-H.; Chang, C.-H.; Lin, C.-H. Comparative efficacy of corticosteroid injection and non-invasive treatments for plantar fasciitis: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 4033. [Google Scholar]
- Whittaker, G.A.; Munteanu, S.E.; Menz, H.B.; Bonanno, D.R.; Gerrard, J.M.; Landorf, K.B. Corticosteroid injection for plantar heel pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Xia, C.; Yu, A.; Qi, B. Ultrasound- versus palpation-guided injection of corticosteroid for plantar fasciitis: A meta-analysis. PLoS ONE 2014, 9, e92671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vannini, F.; Di Matteo, B.; Filardo, G.; Kon, E.; Marcacci, M.; Giannini, S. Platelet-rich plasma for foot and ankle pathologies: A systematic review. Foot Ankle Surg. 2014, 20, 2–9. [Google Scholar] [CrossRef]
- Franceschi, F.; Papalia, R.; Franceschetti, E.; Paciotti, M.; Maffulli, N.; Denaro, V. Platelet-rich plasma injections for chronic plantar fasciopathy: A systematic review. Br. Med. Bull. 2014, 112, 83–95. [Google Scholar] [CrossRef] [Green Version]
- Chiew, S.K.; Ramasamy, T.S.; Amini, F. Effectiveness and relevant factors of platelet-rich plasma treatment in managing plantar fasciitis: A systematic review. J. Res. Med. Sci. 2016, 21, 38. [Google Scholar] [CrossRef]
- Ling, Y.; Wang, S. Effects of platelet-rich plasma in the treatment of plantar fasciitis: A meta-analysis of randomized controlled trials. Medicine 2018, 97, E12110. [Google Scholar] [CrossRef]
- Yu, T.; Xia, J.; Li, B.; Zhou, H.; Yang, Y.; Yu, G. Outcomes of platelet-rich plasma for plantar fasciopathy: A best-evidence synthesis. J. Orthop. Surg. Res. 2020, 15, 432. [Google Scholar] [CrossRef]
- Sheth, U.; Simunovic, N.; Klein, G.; Fu, F.; Einhorn, T.A.; Schemitsch, E.; Ayeni, O.R.; Bhandari, M. Efficacy of autologous platelet-rich plasma use for orthopaedic indications: A meta-analysis. J. Bone Joint Surg. Am. 2012, 94, 298–307. [Google Scholar] [CrossRef]
- Franchini, M.; Cruciani, M.; Mengoli, C.; Marano, G.; Pupella, S.; Veropalumbo, E.; Masiello, F.; Pati, I.; Vaglio, S.; Liumbruno, G.M. Efficacy of platelet-rich plasma as conservative treatment in orthopaedics: A systematic review and meta-analysis. Blood Transfus. 2018, 16, 502–513. [Google Scholar] [CrossRef] [PubMed]
- Andia, I.; Maffulli, N. Muscle and tendon injuries: The role of biological interventions to promote and assist healing and recovery. Arthroscopy 2015, 31, 999–1015. [Google Scholar] [CrossRef] [PubMed]
- Tsikopoulos, K.; Tsikopoulos, A.; Natsis, K. Autologous whole blood or corticosteroid injections for the treatment of epicondylopathy and plantar fasciopathy? a systematic review and meta-analysis of randomized controlled trials. Phys. Ther. Sport 2016, 22, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Madanipour, S.; Bhamra, J.S.; Gill, I. A systematic review and meta-analysis of platelet-rich plasma versus corticosteroid injections for plantar fasciopathy. Int. Orthop. 2017, 41, 1169–1181. [Google Scholar] [CrossRef]
- Yang, W.Y.; Han, Y.H.; Cao, X.W.; Pan, J.K.; Zeng, L.F.; Lin, J.T.; Liu, J. Platelet-rich plasma as a treatment for plantar fasciitis: A meta-analysis of randomized controlled trials. Medicine 2017, 96, e8475. [Google Scholar] [CrossRef]
- Chen, Y.J.; Wu, Y.C.; Tu, Y.K.; Cheng, J.W.; Tsai, W.C.; Yu, T.Y. Autologous Blood-Derived Products Compared with Corticosteroids for Treatment of Plantar Fasciopathy: A Systematic Review and Meta-Analysis. Am. J. Phys. Med. Rehabil. 2019, 98, 343–352. [Google Scholar] [CrossRef]
- Huang, K.; Giddins, G.; Wu, L.D. Platelet-Rich Plasma Versus Corticosteroid Injections in the Management of Elbow Epicondylitis and Plantar Fasciitis: An Updated Systematic Review and Meta-Analysis. Am. J. Sports Med. 2020, 48, 2572–2585. [Google Scholar] [CrossRef]
- Mohammed, W.; Farah, S.; Nassiri, M.; McKenna, J. Therapeutic efficacy of platelet-rich plasma injection compared to corticosteroid injection in plantar fasciitis: A systematic review and meta-analysis. J. Orthop. 2020, 22, 124–134. [Google Scholar] [CrossRef]
- Hohmann, E.; Tetsworth, K.; Glatt, V. Platelet-Rich Plasma Versus Corticosteroids for the Treatment of Plantar Fasciitis: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2021, 49, 1381–1393. [Google Scholar] [CrossRef]
- Alkhatib, N.; Salameh, M.; Ahmed, A.F.; Alkaramany, E.; Ahmed, G.; Mekhaimar, M.M.; Alsaei, J. Platelet-Rich Plasma Versus Corticosteroids in the Treatment of Chronic Plantar Fasciitis: A Systematic Review and Meta-analysis of Prospective Comparative Studies. J. Foot Ankle Surg. 2020, 59, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Hurley, E.T.; Shimozono, Y.; Hannon, C.P.; Smyth, N.A.; Murawski, C.D.; Kennedy, J.G. Platelet-Rich Plasma Versus Corticosteroids for Plantar Fasciitis: A Systematic Review of Randomized Controlled Trials. Orthop. J. Sports Med. 2020, 8, 2325967120915704. [Google Scholar] [CrossRef] [PubMed]
- Tseng, W.C.; Uy, J.; Chiu, Y.H.; Chen, W.S.; Vora, A. The Comparative Effectiveness of Autologous Blood-derived Products Versus Steroid Injections in Plantar Fasciitis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. PMR 2021, 13, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Speed, C. A systematic review of shockwave therapies in soft tissue conditions: Focusing on the evidence. Br. J. Sports Med. 2014, 48, 1538–1542. [Google Scholar] [CrossRef]
- Sun, J.; Gao, F.; Wang, Y.; Sun, W.; Jiang, B.; Li, Z. Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: A meta-analysis of RCTs. Medicine 2017, 96, e6621. [Google Scholar] [CrossRef]
- Al-Abbad, H.; Allen, S.; Morris, S.; Reznik, J.; Biros, E.; Paulik, B.; Wright, A. The effects of shockwave therapy on musculoskeletal conditions based on changes in imaging: A systematic review and meta-analysis with meta-regression. BMC Musculoskelet. Disord. 2020, 21, 275. [Google Scholar] [CrossRef]
- Ogden, J.A.; Alvarez, R.G.; Marlow, M. Shockwave therapy for chronic proximal plantar fasciitis: A meta-analysis. Foot Ankle Int. 2002, 23, 301–308. [Google Scholar] [CrossRef]
- Thomson, C.E.; Crawford, F.; Murray, G.D. The effectiveness of extra corporeal shock wave therapy for plantar heel pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2005, 6, 19. [Google Scholar] [CrossRef] [Green Version]
- Aqil, A.; Siddiqui, M.R.; Solan, M.; Redfern, D.J.; Gulati, V.; Cobb, J.P. Extracorporeal shock wave therapy is effective in treating chronic plantar fasciitis: A meta-analysis of RCTs. Clin. Orthop. Relat. Res. 2013, 471, 3645–3652. [Google Scholar] [CrossRef] [Green Version]
- Lou, J.; Wang, S.; Liu, S.; Xing, G. Effectiveness of Extracorporeal Shock Wave Therapy without Local Anesthesia in Patients with Recalcitrant Plantar Fasciitis: A Meta-Analysis of Randomized Controlled Trials. Am. J. Phys. Med. Rehabil. 2017, 96, 529–534. [Google Scholar] [CrossRef]
- Sun, K.; Zhou, H.; Jiang, W. Extracorporeal shock wave therapy versus other therapeutic methods for chronic plantar fasciitis. Foot Ankle Surg. 2020, 26, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Jin, T.; Shao, Z. Meta-analysis of high-energy extracorporeal shock wave therapy in recalcitrant plantar fasciitis. Swiss Med. Wkly. 2013, 143, w13825. [Google Scholar] [CrossRef]
- Yin, M.C.; Ye, J.; Yao, M.; Cui, X.J.; Xia, Y.; Shen, Q.X.; Tong, Z.Y.; Wu, X.Q.; Ma, J.M.; Mo, W. Is extracorporeal shock wave therapy clinical efficacy for relief of chronic, recalcitrant plantar fasciitis? a systematic review and meta-analysis of randomized placebo or active-treatment controlled trials. Arch. Phys. Med. Rehabil. 2014, 95, 1585–1593. [Google Scholar] [CrossRef] [PubMed]
- Dizon, J.N.; Gonzalez-Suarez, C.; Zamora, M.T.; Gambito, E.D. Effectiveness of extracorporeal shock wave therapy in chronic plantar fasciitis: A meta-analysis. Am. J. Phys. Med. Rehabil. 2013, 92, 606–620. [Google Scholar] [CrossRef]
- Chang, K.V.; Chen, S.Y.; Chen, W.S.; Tu, Y.K.; Chien, K.L. Comparative effectiveness of focused shock wave therapy of different intensity levels and radial shock wave therapy for treating plantar fasciitis: A systematic review and network meta-analysis. Arch. Phys. Med. Rehabil. 2012, 93, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Chen, S.J.; Huang, P.J.; Huang, H.T.; Cheng, Y.M.; Shih, C.L. Efficacy of Different Energy Levels Used in Focused and Radial Extracorporeal Shockwave Therapy in the Treatment of Plantar Fasciitis: A Meta-Analysis of Randomized Placebo-Controlled Trials. J. Clin. Med. 2019, 8, 1497. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Y.; Wu, Q.; Mi, B.; Zhou, W.; Liu, Y.; Liu, J.; Xue, H.; Hu, L.; Panayi, A.C.; Liu, G. Comparison of efficacy of shock-wave therapy versus corticosteroids in plantar fasciitis: A meta-analysis of randomized controlled trials. Arch. Orthop. Trauma Surg. 2019, 139, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Wang, K.; Sun, H.; Luo, X.; Wang, P.; Fang, S.; Chen, H.; Sun, X. Clinical effects of extracorporeal shock-wave therapy and ultrasound-guided local corticosteroid injections for plantar fasciitis in adults: A meta-analysis of randomized controlled trials. Medicine 2018, 97, e13687. [Google Scholar] [CrossRef]
- Li, H.; Xiong, Y.; Zhou, W.; Liu, Y.; Liu, J.; Xue, H.; Hu, L.; Panayi, A.C.; Mi, B.; Liu, G. Shock-wave therapy improved outcome with plantar fasciitis: A meta-analysis of randomized controlled trials. Arch. Orthop. Trauma Surg. 2019, 139, 1763–1770. [Google Scholar] [CrossRef]
- Roerdink, R.L.; Dietvorst, M.; van der Zwaard, B.; van der Worp, H.; Zwerver, J. Complications of extracorporeal shockwave therapy in plantar fasciitis: Systematic review. Int. J. Surg. 2017, 46, 133–145. [Google Scholar] [CrossRef]
- Lee, S.Y.; McKeon, P.; Hertel, J. Does the use of orthoses improve self-reported pain and function measures in patients with plantar fasciitis? A meta-analysis. Phys. Ther. Sport 2009, 10, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Mendes, A.; Silva, H.J.A.; Costa, A.R.A.; Pinheiro, Y.T.; Lins, C.A.A.; de Souza, M.C. Main types of insoles described in the literature and their applicability for musculoskeletal disorders of the lower limbs: A systematic review of clinical studies. J. Bodyw. Mov. Ther. 2020, 24, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Schuitema, D.; Greve, C.; Postema, K.; Dekker, R.; Hijmans, J.M. Effectiveness of Mechanical Treatment for Plantar Fasciitis: A Systematic Review. J. Sport Rehabil. 2020, 29, 657–674. [Google Scholar] [CrossRef]
- Hawke, F.; Burns, J.; Radford, J.A.; du Toit, V. Custom-made foot orthoses for the treatment of foot pain. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef]
- Whittaker, G.A.; Munteanu, S.E.; Menz, H.B.; Tan, J.M.; Rabusin, C.L.; Landorf, K.B. Foot orthoses for plantar heel pain: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Rasenberg, N.; Riel, H.; Rathleff, M.S.; Bierma-Zeinstra, S.M.A.; van Middelkoop, M. Efficacy of foot orthoses for the treatment of plantar heel pain: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1040–1046. [Google Scholar] [CrossRef]
- Healy, A.; Farmer, S.; Pandyan, A.; Chockalingam, N. A systematic review of randomised controlled trials assessing effectiveness of prosthetic and orthotic interventions. PLoS ONE 2018, 13, e0192094. [Google Scholar] [CrossRef] [Green Version]
- Podolsky, R.; Kalichman, L. Taping for plantar fasciitis. J. Back Musculoskelet. Rehabil. 2015, 28, 1–6. [Google Scholar] [CrossRef]
- van de Water, A.T.; Speksnijder, C.M. Efficacy of taping for the treatment of plantar fasciosis: A systematic review of controlled trials. J. Am. Podiatr. Med. Assoc. 2010, 100, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Clark, R.J.; Tighe, M. The effectiveness of acupuncture for plantar heel pain: A systematic review. Acupunct. Med. 2012, 30, 298–306. [Google Scholar] [CrossRef]
- Thiagarajah, A.G. How effective is acupuncture for reducing pain due to plantar fasciitis? Singap. Med. J. 2017, 58, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Cotchett, M.P.; Landorf, K.B.; Munteanu, S.E. Effectiveness of dry needling and injections of myofascial trigger points associated with plantar heel pain: A systematic review. J. Foot Ankle Res. 2010, 3, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, C.; Ma, H. Effectiveness of trigger point dry needling for plantar heel pain: A meta-analysis of seven randomized controlled trials. J. Pain Res. 2017, 10, 1933–1942. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, S.A.; Sampaio, L.M.; Caires, J.R.; Fernandes, G.H.C.; Marsico, A.; Serra, A.J.; Leal-Junior, E.C.; de Carvalho, P.T.C. Parameters and Effects of Photobiomodulation in Plantar Fasciitis: A Meta-Analysis and Systematic Review. Photobiomodul. Photomed. Laser Surg. 2019, 37, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Jiang, W.; Tang, C.; Zhang, X.; Xiang, J. Clinical efficacy of low-level laser therapy in plantar fasciitis: A systematic review and meta-analysis. Medicine 2019, 98, e14088. [Google Scholar] [CrossRef] [PubMed]
- Huffer, D.; Hing, W.; Newton, R.; Clair, M. Strength training for plantar fasciitis and the intrinsic foot musculature: A systematic review. Phys. Ther. Sport 2017, 24, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Sweeting, D.; Parish, B.; Hooper, L.; Chester, R. The effectiveness of manual stretching in the treatment of plantar heel pain: A systematic review. J. Foot Ankle Res. 2011, 4, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siriphorn, A.; Eksakulkla, S. Calf stretching and plantar fascia-specific stretching for plantar fasciitis: A systematic review and meta-analysis. J. Bodyw. Mov. Ther. 2020, 24, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Woitzik, E.; Jacobs, C.; Wong, J.J.; Côté, P.; Shearer, H.M.; Randhawa, K.; Sutton, D.; Southerst, D.; Varatharajan, S.; Brison, R.J.; et al. The effectiveness of exercise on recovery and clinical outcomes of soft tissue injuries of the leg, ankle, and foot: A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Man. Ther. 2015, 20, 633–645. [Google Scholar] [CrossRef]
- Brantingham, J.W.; Bonnefin, D.; Perle, S.M.; Cassa, T.K.; Globe, G.; Pribicevic, M.; Hicks, M.; Korporaal, C. Manipulative therapy for lower extremity conditions: Update of a literature review. J. Manip. Physiol. Ther. 2012, 35, 127–166. [Google Scholar] [CrossRef]
- Clar, C.; Tsertsvadze, A.; Court, R.; Hundt, G.L.; Clarke, A.; Sutcliffe, P. Clinical effectiveness of manual therapy for the management of musculoskeletal and non-musculoskeletal conditions: Systematic review and update of UK evidence report. Chiropr. Man. Therap. 2014, 22, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piper, S.; Shearer, H.M.; Côté, P.; Wong, J.J.; Yu, H.; Varatharajan, S.; Southerst, D.; Randhawa, K.A.; Sutton, D.A.; Stupar, M.; et al. The effectiveness of soft-tissue therapy for the management of musculoskeletal disorders and injuries of the upper and lower extremities: A systematic review by the Ontario Protocol for Traffic Injury management (OPTIMa) collaboration. Man. Ther. 2016, 21, 18–34. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.J.; Corbett, R.; Donner, C.; Hertel, J. Does manual therapy improve pain and function in patients with plantar fasciitis? A systematic review. J. Man. Manip. Ther. 2018, 26, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Mischke, J.J.; Jayaseelan, D.J.; Sault, J.D.; Emerson Kavchak, A.J. The symptomatic and functional effects of manual physical therapy on plantar heel pain: A systematic review. J. Man. Manip. Ther. 2017, 25, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanderson, L.M.; Bryant, A. Effectiveness and safety of prolotherapy injections for management of lower limb tendinopathy and fasciopathy: A systematic review. J. Foot Ankle Res. 2015, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Clijsen, R.; Taeymans, J.; Baeyens, J.P.; Barel, A.O.; Clarys, P. The Effects of iontophoresis in the Treatment of Musculoskeletal Disorders-A Systematic Review And Meta-Analysis. Drug Deliv. Lett. 2012, 2, 180–194. [Google Scholar]
- Malahias, M.A.; Cantiller, E.B.; Kadu, V.V.; Müller, S. The clinical outcome of endoscopic plantar fascia release: A current concept review. Foot Ankle Surg. 2020, 26, 19–24. [Google Scholar] [CrossRef]
- Mao, D.W.; Chandrakumara, D.; Zheng, Q.; Kam, C.; Kon Kam King, C. Endoscopic plantar fasciotomy for plantar fasciitis: A systematic review and network meta-analysis of the English literature. Foot 2019, 41, 63–73. [Google Scholar] [CrossRef]
- Sutton, D.A.; Nordin, M.; Côté, P.; Randhawa, K.; Yu, H.; Wong, J.J.; Stern, P.; Varatharajan, S.; Southerst, D.; Shearer, H.M.; et al. The Effectiveness of Multimodal Care for Soft Tissue Injuries of the Lower Extremity: A Systematic Review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. J. Manip. Physiol. Ther. 2016, 39, 95–109.e102. [Google Scholar] [CrossRef]
- Yu, H.; Randhawa, K.; Côté, P.; Optima, C. The Effectiveness of Physical Agents for Lower-Limb Soft Tissue Injuries: A Systematic Review. J. Orthop. Sports Phys. Ther. 2016, 46, 523–554. [Google Scholar] [CrossRef]
- Atkins, D.; Crawford, F.; Edwards, J.; Lambert, M. A systematic review of treatments for the painful heel. Rheumatology 1999, 38, 968–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uden, H.; Boesch, E.; Kumar, S. Plantar fasciitis—To jab or to support? A systematic review of the current best evidence. J. Multidiscip. Healthc. 2011, 4, 155–164. [Google Scholar] [CrossRef] [Green Version]
- Assad, S.; Ahmad, A.; Kiani, I.; Ghani, U.; Wadhera, V.; Tom, T.N. Novel and Conservative Approaches towards Effective Management of Plantar Fasciitis. Cureus 2016, 8, e913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Boloushi, Z.; López-Royo, M.P.; Arian, M.; Gómez-Trullén, E.M.; Herrero, P. Minimally invasive non-surgical management of plantar fasciitis: A systematic review. J. Bodyw. Mov. Ther. 2019, 23, 122–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvioli, S.; Guidi, M.; Marcotulli, G. The effectiveness of conservative, non-pharmacological treatment, of plantar heel pain: A systematic review with meta-analysis. Foot 2017, 33, 57–67. [Google Scholar] [CrossRef]
- Hsiao, M.Y.; Hung, C.Y.; Chang, K.V.; Chien, K.L.; Tu, Y.K.; Wang, T.G. Comparative effectiveness of autologous blood-derived products, shock-wave therapy and corticosteroids for treatment of plantar fasciitis: A network meta-analysis. Rheumatology 2015, 54, 1735–1743. [Google Scholar] [CrossRef] [Green Version]
- Tsikopoulos, K.; Vasiliadis, H.S.; Mavridis, D. Injection therapies for plantar fasciopathy (‘plantar fasciitis’): A systematic review and network meta-analysis of 22 randomised controlled trials. Br. J. Sports Med. 2016, 50, 1367–1375. [Google Scholar] [CrossRef]
- Li, X.; Zhang, L.; Gu, S.; Sun, J.; Qin, Z.; Yue, J.; Zhong, Y.; Ding, N.; Gao, R. Comparative effectiveness of extracorporeal shock wave, ultrasound, low-level laser therapy, noninvasive interactive neurostimulation, and pulsed radiofrequency treatment for treating plantar fasciitis: A systematic review and network meta-analysis. Medicine 2018, 97, e12819. [Google Scholar] [CrossRef]
- Li, H.; Lv, H.; Lin, T. Comparison of efficacy of eight treatments for plantar fasciitis: A network meta-analysis. J. Cell. Physiol. 2018, 234, 860–870. [Google Scholar] [CrossRef] [Green Version]
- Drake, C.; Mallows, A.; Littlewood, C. Psychosocial variables and presence, severity and prognosis of plantar heel pain: A systematic review of cross-sectional and prognostic associations. Musculoskelet. Care 2018, 16, 329–338. [Google Scholar] [CrossRef] [Green Version]
- Anderson, M.J.; Browning, W.M., 3rd; Urband, C.E.; Kluczynski, M.A.; Bisson, L.J. A Systematic Summary of Systematic Reviews on the Topic of the Anterior Cruciate Ligament. Orthop. J. Sports Med. 2016, 4, 2325967116634074. [Google Scholar] [CrossRef] [Green Version]
- Jancuska, J.; Matthews, J.; Miller, T.; Kluczynski, M.A.; Bisson, L.J. A Systematic Summary of Systematic Reviews on the Topic of the Rotator Cuff. Orthop. J. Sports Med. 2018, 6, 2325967118797891. [Google Scholar] [CrossRef] [Green Version]
- de Sa, D.; Lian, J.; Sheean, A.J.; Inman, K.; Drain, N.; Ayeni, O.; Mauro, C. A Systematic Summary of Systematic Reviews on the Topic of Hip Arthroscopic Surgery. Orthop. J. Sports Med. 2018, 6, 2325967118796222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jomaa, G.; Kwan, C.-K.; Fu, S.-C.; Ling, S.K.-K.; Chan, K.-M.; Yung, P.S.-H.; Rolf, C. A systematic review of inflammatory cells and markers in human tendinopathy. BMC Musculoskelet. Disord. 2020, 21, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baksh, N.; Hannon, C.P.; Murawski, C.D.; Smyth, N.A.; Kennedy, J.G. Platelet-rich plasma in tendon models: A systematic review of basic science literature. Arthroscopy 2013, 29, 596–607. [Google Scholar] [CrossRef]
- Yan, R.; Gu, Y.; Ran, J.; Hu, Y.; Zheng, Z.; Zeng, M.; Heng, B.C.; Chen, X.; Yin, Z.; Chen, W.; et al. Intratendon Delivery of Leukocyte-Poor Platelet-Rich Plasma Improves Healing Compared with Leukocyte-Rich Platelet-Rich Plasma in a Rabbit Achilles Tendinopathy Model. Am. J. Sports Med. 2017, 45, 1909–1920. [Google Scholar] [CrossRef] [PubMed]
- Cross, J.A.; Cole, B.J.; Spatny, K.P.; Sundman, E.; Romeo, A.A.; Nicholson, G.P.; Wagner, B.; Fortier, L.A. Leukocyte-Reduced Platelet-Rich Plasma Normalizes Matrix Metabolism in Torn Human Rotator Cuff Tendons. Am. J. Sports Med. 2015, 43, 2898–2906. [Google Scholar] [CrossRef]
- Fitzpatrick, J.; Bulsara, M.; Zheng, M.H. The Effectiveness of Platelet-Rich Plasma in the Treatment of Tendinopathy: A Meta-analysis of Randomized Controlled Clinical Trials. Am. J. Sports Med. 2017, 45, 226–233. [Google Scholar] [CrossRef]
- Deluca, S.; Robinson, D.M.; Yun, P.H.; Rosenberg, C.; Tan, C.O.; Tenforde, A.S. Similar Functional Gains Using Radial versus Combined Shockwave Therapy in Management of Plantar Fasciitis. J. Foot Ankle Surg. 2021, 60, 1098–1102. [Google Scholar] [CrossRef]
- Johnson, C.D.; Tenforde, A.S.; Outerleys, J.; Reilly, J.; Davis, I.S. Impact-Related Ground Reaction Forces Are More Strongly Associated with Some Running Injuries than Others. Am. J. Sports Med. 2020, 48, 3072–3080. [Google Scholar] [CrossRef]
- Malliaras, P.; Barton, C.J.; Reeves, N.D.; Langberg, H. Achilles and patellar tendinopathy loading programmes: A systematic review comparing clinical outcomes and identifying potential mechanisms for effectiveness. Sports Med. 2013, 43, 267–286. [Google Scholar] [CrossRef] [PubMed]
- Jones, I.A.; Togashi, R.C.; Thomas Vangsness, C., Jr. The Economics and Regulation of PRP in the Evolving Field of Orthopedic Biologics. Curr. Rev. Musculoskelet. Med. 2018, 11, 558–565. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rhim, H.C.; Kwon, J.; Park, J.; Borg-Stein, J.; Tenforde, A.S. A Systematic Review of Systematic Reviews on the Epidemiology, Evaluation, and Treatment of Plantar Fasciitis. Life 2021, 11, 1287. https://doi.org/10.3390/life11121287
Rhim HC, Kwon J, Park J, Borg-Stein J, Tenforde AS. A Systematic Review of Systematic Reviews on the Epidemiology, Evaluation, and Treatment of Plantar Fasciitis. Life. 2021; 11(12):1287. https://doi.org/10.3390/life11121287
Chicago/Turabian StyleRhim, Hye Chang, Jangwon Kwon, Jewel Park, Joanne Borg-Stein, and Adam S. Tenforde. 2021. "A Systematic Review of Systematic Reviews on the Epidemiology, Evaluation, and Treatment of Plantar Fasciitis" Life 11, no. 12: 1287. https://doi.org/10.3390/life11121287
APA StyleRhim, H. C., Kwon, J., Park, J., Borg-Stein, J., & Tenforde, A. S. (2021). A Systematic Review of Systematic Reviews on the Epidemiology, Evaluation, and Treatment of Plantar Fasciitis. Life, 11(12), 1287. https://doi.org/10.3390/life11121287