
The Role of SARS-CoV-2 Testing on Hospitalizations in California

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Exposure and Outcome
2.3. Model
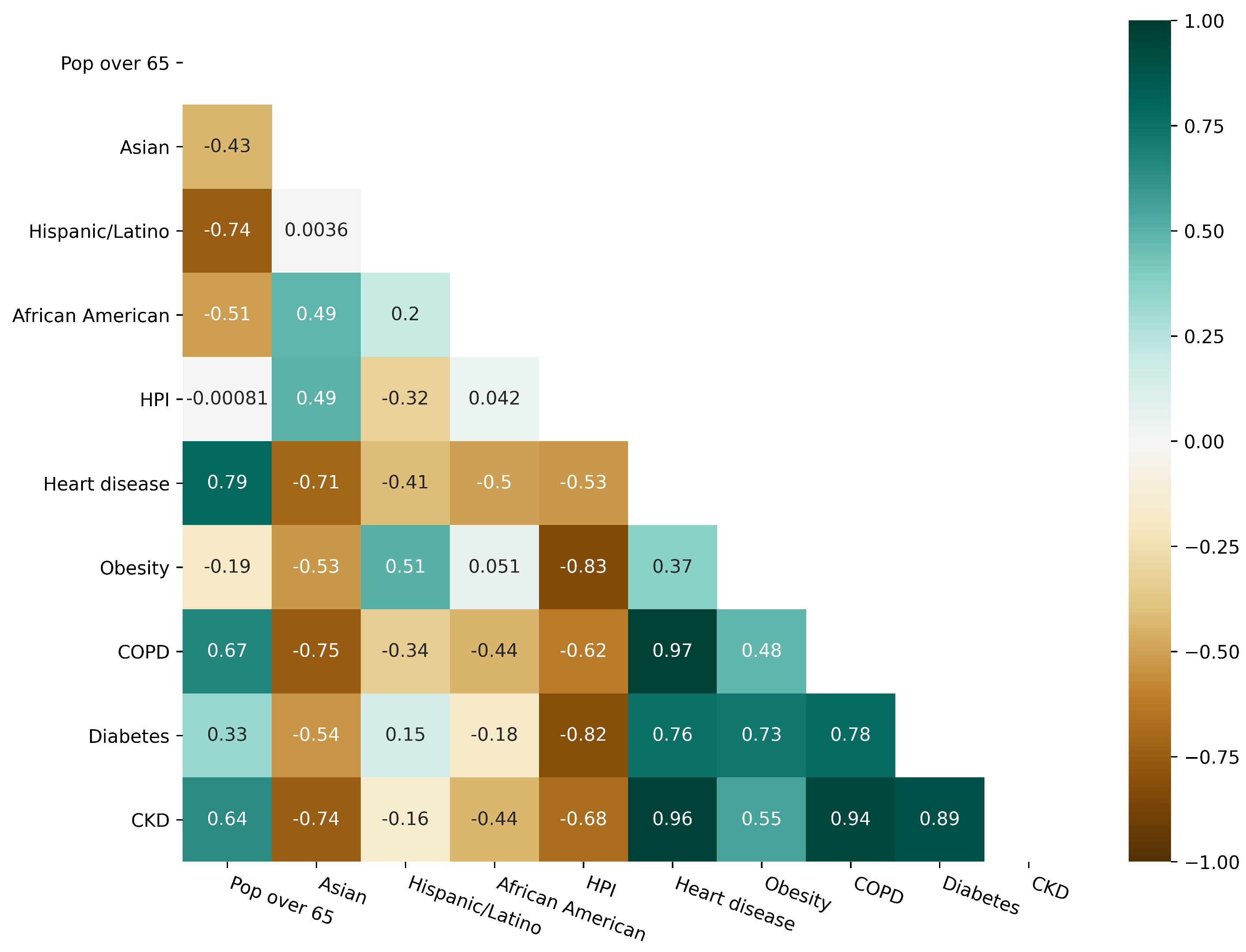
2.4. Variable Correlation
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Variable Description
Appendix A.1. Demographic Variables

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Description |
|---|---|
| Pop over 65 | Percentage of population ages 65 and above |
| Asian | Percentage of Asian population |
| Hispanic/Latino | Percentage of Hispanic or Latino population |
| African American | Percentage of Black or African American population |
| HPI | Healthy Places Index |
| Variable | Description |
|---|---|
| Heart disease | Prevalence of heart disease |
| Obesity | Prevalence of obesity |
| COPD | Prevalence of chronic obstructive pulmonary disease |
| Diabetes | Prevalence of diabetes |
| CKD | Prevalence of chronic kidney disease |
| Variable | VIF |
|---|---|
| Pop over 65 | 299.79 |
| Asian | 11.19 |
| Hispanic/Latino | 73.89 |
| African American | 6.50 |
| HPI | 11.71 |
| Heart disease | 3846.96 |
| Obesity | 235.79 |
| COPD | 1648.60 |
| Diabetes | 1430.87 |
| CKD | 3342.10 |
Appendix A.2. Mobility Trends
| County | Explained Variance | County | Explained Variance | County | Explained Variance |
|---|---|---|---|---|---|
| Alameda | 0.62 | Mendocino | 0.60 | San Mateo | 0.65 |
| Amador | 0.43 | Merced | 0.68 | Santa Barbara | 0.67 |
| Butte | 0.56 | Monterey | 0.66 | Santa Clara | 0.60 |
| Contra Costa | 0.63 | Napa | 0.56 | Santa Cruz | 0.60 |
| El Dorado | 0.50 | Nevada | 0.58 | Shasta | 0.51 |
| Fresno | 0.67 | Orange | 0.68 | Solano | 0.60 |
| Humboldt | 0.60 | Placer | 0.50 | Sonoma | 0.66 |
| Imperial | 0.67 | Riverside | 0.65 | Stanislaus | 0.62 |
| Kern | 0.60 | Sacramento | 0.66 | Tehama | 0.4 |
| Kings | 0.61 | San Bernardino | 0.62 | Tulare | 0.57 |
| Lake | 0.65 | San Diego | 0.71 | Tuolumne | 0.47 |
| Los Angeles | 0.73 | San Francisco | 0.73 | Ventura | 0.56 |
| Madera | 0.51 | San Joaquin | 0.68 | Yolo | 0.66 |
| Marin | 0.62 | San Luis Obispo | 0.65 | Yuba | 0.54 |
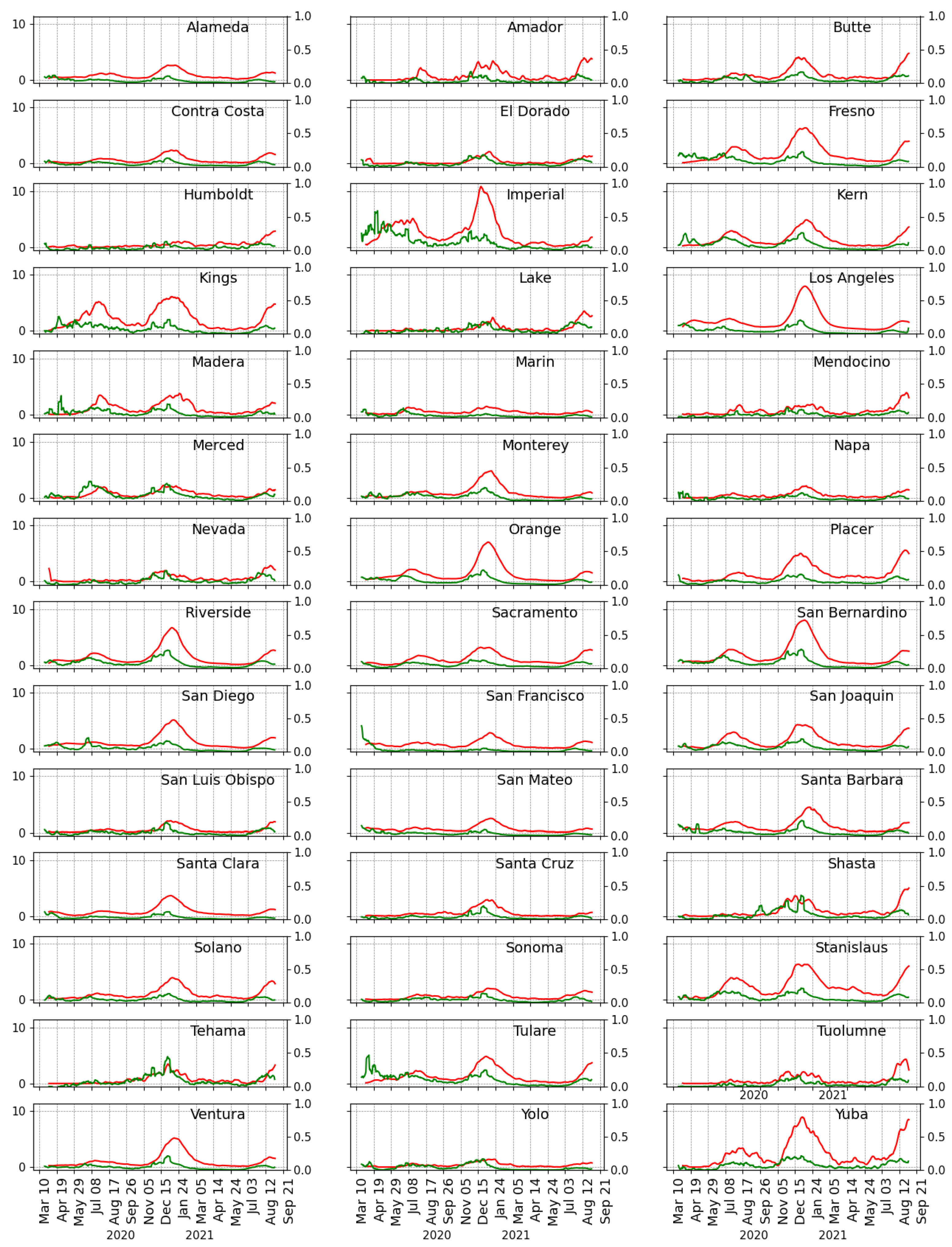
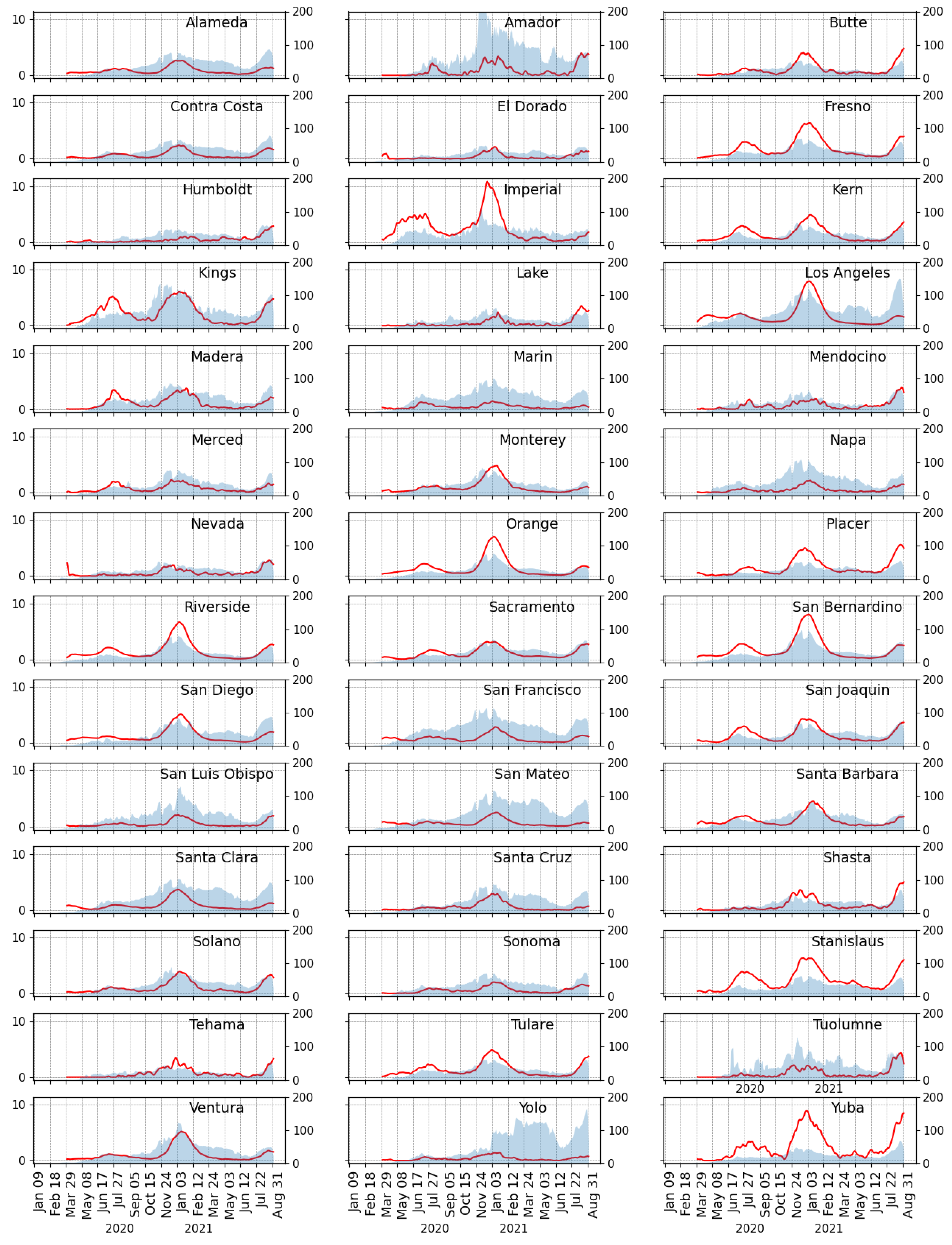
Appendix B. Hospitalizations and Testings

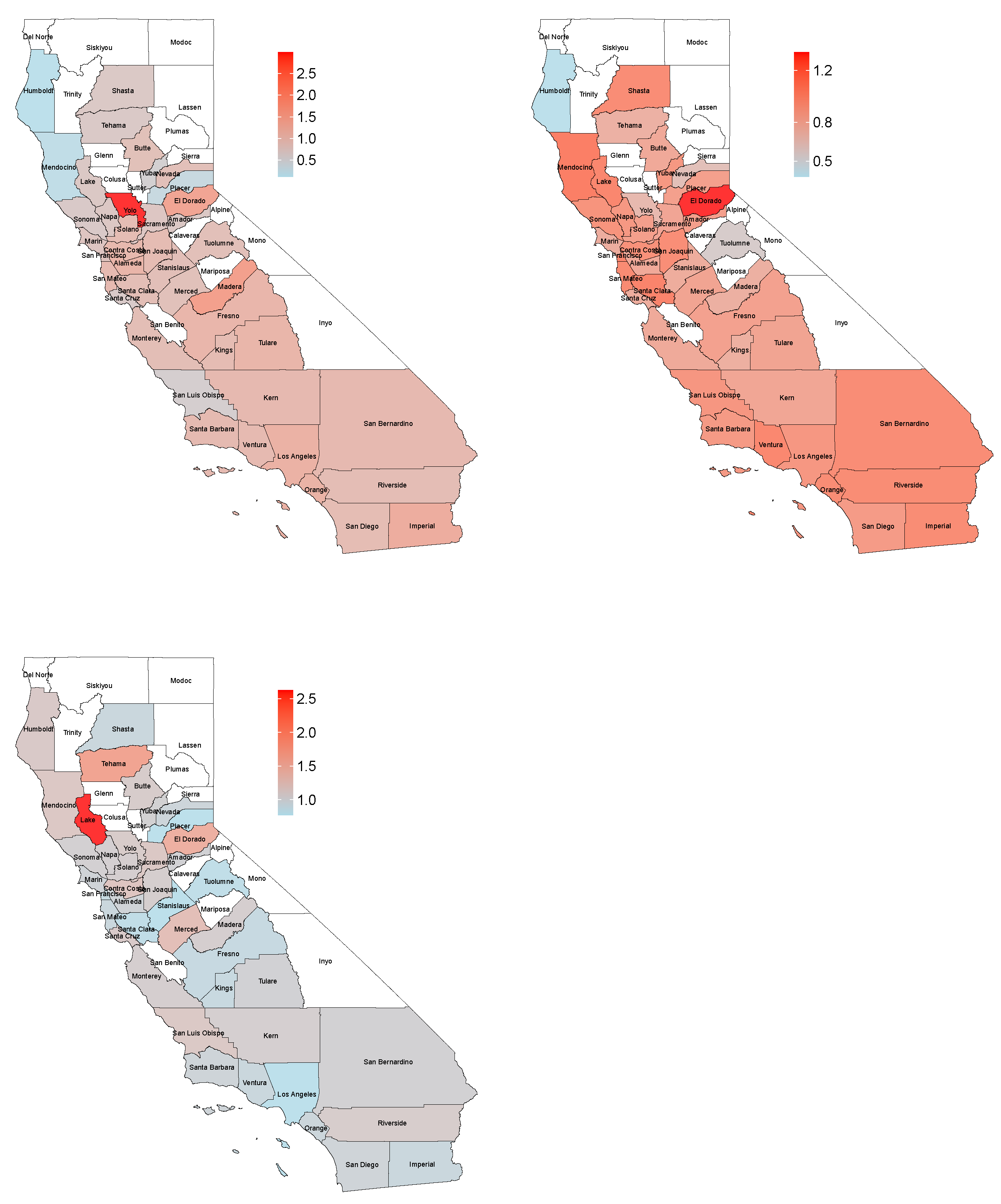
Appendix C. Maps

References
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar]
- Johns Hopkins Coronavirus Resource Center. COVID-19 Map. Available online: https://coronavirus.jhu.edu/map.html (accessed on 5 October 2021).
- Nicola, M.; Sohrabi, C.; Mathew, G.; Kerwan, A.; Al-Jabir, A.; Griffin, M.; Agha, M.; Agha, R. Health policy and leadership models during the COVID-19 pandemic-review article. Int. J. Surg. 2020, 81, 122–129. [Google Scholar] [CrossRef]
- Ebrahim, S.H.; Ahmed, Q.A.; Gozzer, E.; Schlagenhauf, P.; Memish, Z.A. Covid-19 and community mitigation strategies in a pandemic. BMJ 2020, 368, m1066. [Google Scholar] [CrossRef] [Green Version]
- Hadfield, J.; Megill, C.; Bell, S.M.; Huddleston, J.; Potter, B.; Callender, C.; Sagulenko, P.; Bedford, T.; Neher, R.A. Nextstrain: Real-time tracking of pathogen evolution. Bioinformatics 2018, 34, 4121–4123. [Google Scholar] [CrossRef]
- Bonet, M.; Blanco, I.; JM, A.P.; Clotet, B.; Ara Del Rey, J. A cost-benefit analysis of the COVID-19 asymptomatic mass testing strategy in the north metropolitan area of Barcelona. Int. J. Environ. 2021, 18, 7028. [Google Scholar]
- Wang, C.J.; Ng, C.Y.; Brook, R.H. Response to COVID-19 in Taiwan: Big data analytics, new technology, and proactive testing. JAMA 2020, 323, 1341–1342. [Google Scholar] [CrossRef]
- Cao, S.; Gan, Y.; Wang, C.; Bachmann, M.; Wei, S.; Gong, J.; Huang, Y.; Wang, T.; Li, L.; Lu, K.; et al. Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nat. Commun. 2020, 11, 5917. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y. Large-scale national screening for COVID-19 in China. J. Med. Virol. 2020, 92, 2266–2268. [Google Scholar] [CrossRef] [PubMed]
- Burki, T. Mass testing for COVID-19. Lancet Microbe 2020, 1, e317. [Google Scholar] [CrossRef]
- Louie, J.K.; Scott, H.M.; DuBois, A.; Sturtz, N.; Lu, W.; Stoltey, J.; Masinde, G.; Cohen, S.; Sachdev, D.; Philip, S.; et al. Lessons from mass-testing for Coronavirus disease 2019 in long-term care facilities for the elderly in San Francisco. Clin. Infect. Dis. 2021, 72, 2018–2020. [Google Scholar] [CrossRef]
- Pilecco, F.B.; Coelho, C.G.; Fernandes, Q.H.R.F.; Silveira, I.H.; Pescarini, J.M.; Ortelan, N.; Gabrielli, L.; Aquino, E.M.; Barreto, M.L. The effect of laboratory testing on COVID-19 monitoring indicators: An analysis of the 50 countries with the highest number of cases. Epidemiol. Serv. Saude 2021, 30. [Google Scholar] [CrossRef]
- Hsiang, S.; Allen, D.; Annan-Phan, S.; Bell, K.; Bolliger, I.; Chong, T.; Druckenmiller, H.; Huang, L.Y.; Hultgren, A.; Krasovich, E.; et al. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature 2020, 584, 262–267. [Google Scholar] [CrossRef]
- Larremore, D.B.; Wilder, B.; Lester, E.; Shehata, S.; Burke, J.M.; Hay, J.A.; Milind, T.; Mina, M.J.; Parker, R. Test sensitivity is secondary to frequency and turnaround time for COVID-19 surveillance. MedRxiv 2020. [Google Scholar] [CrossRef]
- Pavelka, M.; Van-Zandvoort, K.; Abbott, S.; Sherratt, K.; Majdan, M.; COVID, C.; Analỳz, I.Z.; Jarčuška, P.; Krajčí, M.; Flasche, S.; et al. The impact of population-wide rapid antigen testing on SARS-CoV-2 prevalence in Slovakia. Science 2021, 372, 635–641. [Google Scholar] [CrossRef]
- Robinson Meyer, A.C.M. How Bad Is the Coronavirus Outbreak? Here’s a Key Number. The Atlantic. 2020. Available online: https://www.theatlantic.com/technology/archive/2020/04/us-coronavirus-outbreak-out-control-test-positivity-rate/610132/ (accessed on 5 October 2021).
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 Pandemic. Nat. Rev. Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef]
- Neilan, A.M.; Losina, E.; Bangs, A.C.; Flanagan, C.; Panella, C.; Eskibozkurt, G.; Mohareb, A.; Hyle, E.P.; Scott, J.A.; Weinstein, M.C.; et al. Clinical impact, costs, and cost-effectiveness of expanded severe acute respiratory syndrome Coronavirus 2 testing in Massachusetts. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Wei, C.; Lee, C.; Hsu, T.; Hsu, W.; Chan, C.; Chen, S.; Chen, C. Correlation of population mortality of COVID-19 and testing coverage: A comparison among 36 OECD countries. Epidemiol. Infect. 2021, 149, e1. [Google Scholar] [CrossRef]
- Wikipedia. COVID-19 Pandemic in California. Available online: https://en.wikipedia.org/wiki/COVID-19_pandemic_in_California (accessed on 5 October 2021).
- State of California. California Takes Action to Combat COVID-19 | California Governor. Available online: https://www.gov.ca.gov/california-takes-action-to-combat-covid-19/ (accessed on 5 October 2021).
- Office of Governor Gavin Newsom. As California Fully Reopens, Governor Newsom Announces Plans to Lift Pandemic Executive Orders. 11 June 2021. Available online: https://www.gov.ca.gov/2021/06/11/as-california-fully-reopens-governor-newsom-announces-plans-to-lift-pandemic-executive-orders/ (accessed on 22 September 2021).
- Mossburg, C. Here’s What You Need to Know about California’s Reopening. CNN. Available online: https://edition.cnn.com/us/live-news/coronavirus-pandemic-vaccine-updates-06-15-21/index.html (accessed on 5 October 2021).
- USAFacts. California Coronavirus Cases and Deaths. Available online: https://usafacts.org/visualizations/coronavirus-covid-19-spread-map/state/california (accessed on 5 October 2021).
- Manduffie, D. Covid Ravaging the Central Valley, California’s New Virus Epicenter. 4 August 2020. Available online: https://www.courthousenews.com/covid-ravaging-the-central-valley-californias-new-virus-epicenter/ (accessed on 5 October 2021).
- Stringini, M.; Hiramoto, K. Is Los Angeles County the New “Epicenter” of the COVID-19 pandemic? 21 December 2020. Available online: https://www.foxla.com/news/is-los-angeles-county-the-new-epicenter-of-the-covid-19-pandemic (accessed on 5 October 2021).
- Vercammen, P.; Melissa Alonso, S.C. LA County Records more than 1 million Coronavirus Cases. 17 January 2021. Available online: https://edition.cnn.com/2021/01/16/health/los-angeles-county-million-coronavirus/index.html (accessed on 5 October 2021).
- abc-7NEWS. California Has Lowest COVID-19 Case Rate in US. Available online: https://abc7news.com/california-covid-ca-coronavirus-rate-pandemic/11033019/ (accessed on 5 October 2021).
- CBS News. California Reports Lowest COVID-19 Case Rate in the Country. Available online: https://www.cbsnews.com/news/california-covid-lowest-positivity-rate/ (accessed on 5 October 2021).
- California Goverment. Tracking COVID-19 in California—Coronavirus COVID-19 Response. Available online: https://covid19.ca.gov/state-dashboard/ (accessed on 16 September 2021).
- Californial Department of Public Health. COVID-19 Time-Series Metrics by County and State—Datasets—California Health and Human Services Open Data Portal. Available online: https://data.chhs.ca.gov/dataset/covid-19-time-series-metrics-by-county-and-state (accessed on 16 September 2021).
- US Census Bureau. 2019 Data Profiles | American Community Survey. Available online: https://www.census.gov/acs/www/data/data-tables-and-tools/data-profiles/ (accessed on 16 September 2021).
- The California Healthy Places Index (HPI). Data & Reports—California Healthy Places Index. Available online: https://healthyplacesindex.org/data-reports/ (accessed on 16 September 2021).
- COVID-19 Community Mobility Reports. Google 2020. Available online: https://www.google.com/covid19/mobility/ (accessed on 9 November 2021).
- Furuse, Y.; Ko, Y.K.; Ninomiya, K.; Suzuki, M.; Oshitani, H. Relationship of test positivity rates with COVID-19 epidemic dynamics. Int. J. Environ. 2021, 18, 4655. [Google Scholar]
- Fenga, L.; Gaspari, M. Predictive capacity of covid-19 test positivity rate. Sensors 2021, 21, 2435. [Google Scholar] [CrossRef]
- Kafle, R.C.; Kim, D.Y.; Malandro, M.E.; Holt, M.M. Modeling COVID-19 positivity rates and hospitalizations in Texas. Model Assist. Stat. Appl. 2021, 16, 53–58. [Google Scholar] [CrossRef]
- Al Dallal, A.; AlDallal, U.; Al Dallal, J. Positivity rate: An indicator for the spread of COVID-19. Curr. Med. Res. 2021, 2067–2076. [Google Scholar] [CrossRef]
- Laird, N.M.; Ware, J.H. Random-effects models for longitudinal data. Biometrics 1982, 38, 963–974. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Chowkwanyun, M.; Reed, A.L., Jr. Racial health disparities and Covid-19—Caution and context. N. Engl. J. Med. 2020, 383, 201–203. [Google Scholar] [CrossRef]
- Escobar, G.J.; Adams, A.S.; Liu, V.X.; Soltesz, L.; Chen, Y.F.I.; Parodi, S.M.; Ray, G.T.; Myers, L.C.; Ramaprasad, C.M.; Dlott, R.; et al. Racial disparities in COVID-19 testing and outcomes: Retrospective cohort study in an integrated health system. Ann. Intern. Med. 2021, 174, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Ogedegbe, G.; Ravenell, J.; Adhikari, S.; Butler, M.; Cook, T.; Francois, F.; Iturrate, E.; Jean-Louis, G.; Jones, S.A.; Deborah Onakomaiya, E.A.; et al. Assessment of racial/ethnic disparities in hospitalization and mortality in patients with COVID-19 in New York City. JAMA Netw. Open 2020, 3, e2026881. [Google Scholar] [CrossRef]
- Podewils, L.J.; Burket, T.L.; Mettenbrink, C.; Steiner, A.; Seidel, A.; Scott, K.; Cervantes, L.; Hasnain-Wynia, R. Disproportionate incidence of COVID-19 infection, hospitalizations, and deaths among persons identifying as Hispanic or Latino—Denver, Colorado March–October 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1812–1816. [Google Scholar] [CrossRef]
- Hooper, M.W.; Nápoles, A.M.; Pérez-Stable, E.J. COVID-19 and racial/ethnic disparities. JAMA 2020, 323, 2466–2467. [Google Scholar] [CrossRef]
- This Time Must Be Different: Disparities during the COVID-19 Pandemic. 2020. Available online: https://www.acpjournals.org/doi/full/10.7326/M20-2247 (accessed on 5 October 2021).
- Bhowmik, T.; Tirtha, S.D.; Iraganaboina, N.C.; Eluru, N. A comprehensive analysis of COVID-19 transmission and mortality rates at the county level in the United States considering socio-demographics, health indicators, mobility trends and health care infrastructure attributes. PLoS ONE 2021, 16, e0249133. [Google Scholar] [CrossRef]
- Gottumukkala, R.; Katragadda, S.; Bhupatiraju, R.T.; Kamal, M.; Raghavan, V.; Chu, H.; Kolluru, R.; Ashkar, Z. Exploring the relationship between mobility and COVID- 19 infection rates for the second peak in the United States using phase-wise association. BMC Public Health 2021, 21, 1669. [Google Scholar] [CrossRef] [PubMed]
- Nouvellet, P.; Bhatia, S.; Cori, A.; Ainslie, K.E.; Baguelin, M.; Bhatt, S.; Boonyasiri, A.; Brazeau, N.F.; Cattarino, L.; Cooper, L.V.; et al. Reduction in mobility and COVID-19 transmission. Nat. Commun. 2021, 12, 1090. [Google Scholar] [CrossRef]
- Badr, H.S.; Du, H.; Marshall, M.; Dong, E.; Squire, M.M.; Gardner, L.M. Association between mobility patterns and COVID-19 transmission in the USA: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 1247–1254. [Google Scholar] [CrossRef]
- Bergman, N.K.; Fishman, R. Mobility levels and Covid-19 transmission rates. medRxiv 2020. [Google Scholar] [CrossRef]
- Gatalo, O.; Tseng, K.; Hamilton, A.; Lin, G.; Klein, E. Associations between phone mobility data and COVID-19 cases. Lancet Infect. Dis. 2021, 21, e111. [Google Scholar] [PubMed]
- Apple. COVID-19 Mobility Trends Reports. Available online: https://covid19.apple.com/mobility (accessed on 5 October 2021).
- Distancing Metrics, S. SafeGraph. 2020. Available online: https://docs.safegraph.com/docs/social-distancing-metrics (accessed on 5 October 2021).
- California Health and Human Services Open Data Portal. COVID-19 Hospital Data. Available online: https://data.chhs.ca.gov/dataset/covid-19-hospital-data (accessed on 5 October 2021).



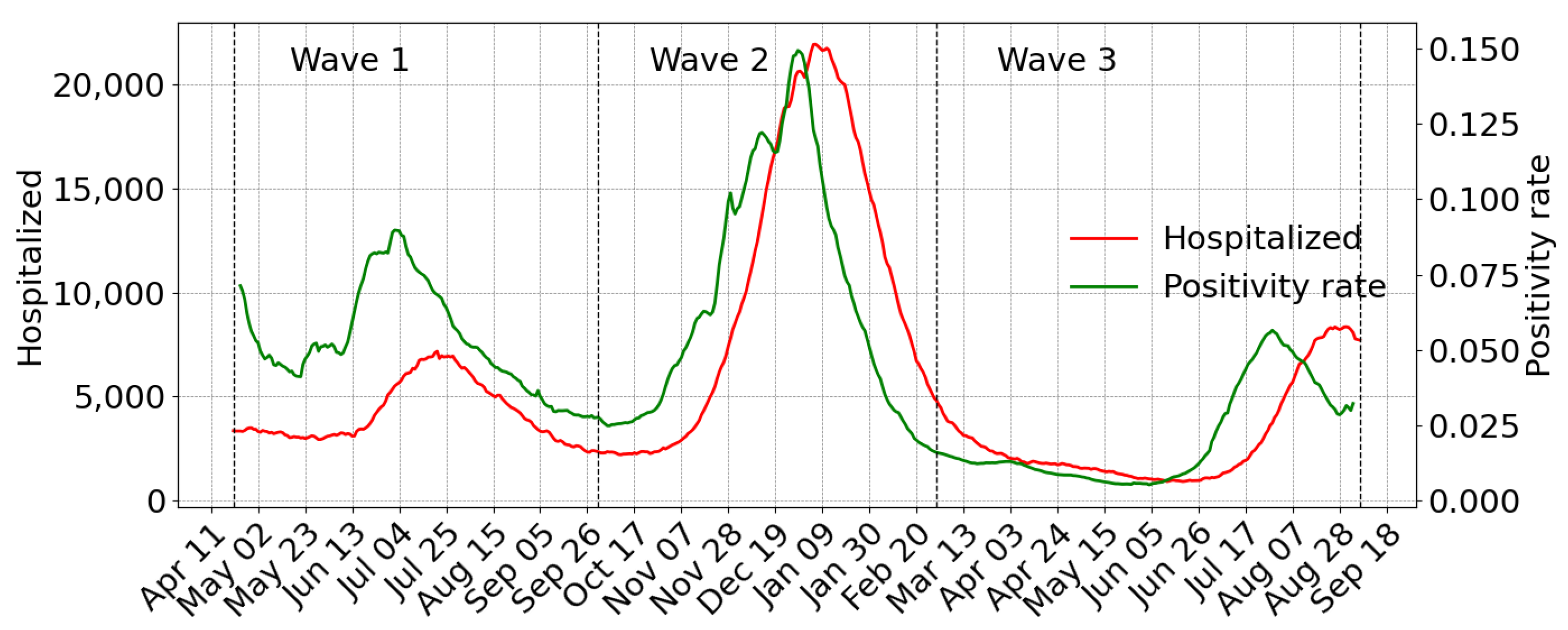
| 1st Wave | 2nd Wave | 3rd Wave | ||||
|---|---|---|---|---|---|---|
| Variable | Estimate * (95% CI) | p-Value | Estimate * (95% CI) | p-Value | Estimate * (95% CI) | p-Value |
| Positivity rate | 0.9 (0.6, 1.4) | <0.001 | 0.9 (0.8, 0.9) | <0.001 | 1.1 (0.9, 1.2) | <0.001 |
| Pop over 65 | −13.2 (−30.6, 8.5) | 0.246 | 3.1 (−3.8, 10.6) | 0.416 | −7.7 (−15.1, −0.1) | 0.060 |
| Asian | 0.8 (−7.2, 9.4) | 0.861 | 3.4 (0.7, 6.1) | 0.020 | −0.5 (−3.9, 2.9) | 0.763 |
| Hispanic/Latino | 7.4 (2.1, 12.9) | 0.010 | 0.9 (−0.6, 2.5) | 0.259 | −0.6 (−2.3, 1.3) | 0.535 |
| African American | 16.6 (0.1, 35.9) | 0.070 | 0.1 (−4.7, 5.1) | 0.982 | 1.8 (−4.3, 8.2) | 0.582 |
| HPI ** | 4.9 (2.4, 7.4) | <0.001 | −0.4 (−1.2, 0.3) | 0.266 | 0.2 (−0.7, 1.2) | 0.686 |
| Mobility | 4.9 (1.9, 7.9) | <0.001 | −2.8 (−3.4, −2.1) | <0.001 | 0.1 (−1.7, 1.8) | 0.950 |
| County | Wave 1 | Wave 2 | Wave 3 | County | Wave 1 | Wave 2 | Wave 3 |
|---|---|---|---|---|---|---|---|
| Yolo | 2.99 | 0.70 | 1.10 | Santa Clara | 0.95 | 1.08 | 0.82 |
| Madera | 1.64 | 0.77 | 1.05 | Stanislaus | 0.92 | 0.80 | 0.78 |
| El Dorado | 1.52 | 1.34 | 1.53 | Nevada | 0.92 | 0.64 | 0.94 |
| Imperial | 1.34 | 1.02 | 0.92 | Tuolumne | 0.91 | 0.55 | 0.80 |
| Los Angeles | 1.23 | 0.95 | 0.78 | Butte | 0.90 | 0.82 | 1.10 |
| Orange | 1.22 | 1.02 | 0.94 | Merced | 0.90 | 0.86 | 1.30 |
| Alameda | 1.18 | 0.82 | 0.98 | San Francisco | 0.82 | 1.06 | 0.87 |
| Tulare | 1.15 | 0.86 | 1.00 | Marin | 0.79 | 0.79 | 0.98 |
| Fresno | 1.14 | 0.88 | 0.87 | Sacramento | 0.75 | 0.85 | 1.16 |
| Contra Costa | 1.09 | 0.99 | 1.21 | Napa | 0.73 | 0.95 | 1.04 |
| San Bernardino | 1.06 | 1.01 | 1.02 | Lake | 0.71 | 1.06 | 2.62 |
| Kern | 1.06 | 0.84 | 1.05 | Amador | 0.71 | 0.90 | 1.01 |
| San Mateo | 1.04 | 1.03 | 0.91 | Shasta | 0.70 | 1.02 | 0.91 |
| Ventura | 1.04 | 1.05 | 0.91 | Tehama | 0.69 | 0.76 | 1.70 |
| Santa Barbara | 1.04 | 0.93 | 0.97 | Sonoma | 0.67 | 0.97 | 1.03 |
| San Joaquin | 1.01 | 1.01 | 1.06 | Santa Cruz | 0.66 | 0.79 | 1.12 |
| Kings | 1.00 | 0.77 | 0.89 | San Luis Obispo | 0.55 | 0.95 | 1.15 |
| San Diego | 0.99 | 0.92 | 0.97 | Yuba | 0.52 | 0.95 | 1.02 |
| Solano | 0.99 | 0.90 | 1.06 | Placer | 0.29 | 0.89 | 0.77 |
| Riverside | 0.97 | 1.02 | 1.09 | Mendocino | 0.18 | 1.10 | 1.17 |
| Monterey | 0.95 | 0.81 | 1.05 | Humboldt | 0.12 | 0.38 | 1.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montesinos-López, J.C.; Daza-Torres, M.L.; García, Y.E.; Barboza, L.A.; Sanchez, F.; Schmidt, A.J.; Pollock, B.H.; Nuño, M. The Role of SARS-CoV-2 Testing on Hospitalizations in California. Life 2021, 11, 1336. https://doi.org/10.3390/life11121336
Montesinos-López JC, Daza-Torres ML, García YE, Barboza LA, Sanchez F, Schmidt AJ, Pollock BH, Nuño M. The Role of SARS-CoV-2 Testing on Hospitalizations in California. Life. 2021; 11(12):1336. https://doi.org/10.3390/life11121336
Chicago/Turabian StyleMontesinos-López, José Cricelio, Maria L. Daza-Torres, Yury E. García, Luis A. Barboza, Fabio Sanchez, Alec J. Schmidt, Brad H. Pollock, and Miriam Nuño. 2021. "The Role of SARS-CoV-2 Testing on Hospitalizations in California" Life 11, no. 12: 1336. https://doi.org/10.3390/life11121336
APA StyleMontesinos-López, J. C., Daza-Torres, M. L., García, Y. E., Barboza, L. A., Sanchez, F., Schmidt, A. J., Pollock, B. H., & Nuño, M. (2021). The Role of SARS-CoV-2 Testing on Hospitalizations in California. Life, 11(12), 1336. https://doi.org/10.3390/life11121336