
Everolimus-Induced Immune Effects after Heart Transplantation: A Possible Tool for Clinicians to Monitor Patients at Risk for Transplant Rejection

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Groups and Patient Characteristics
2.2. Blood Sampling
2.3. Flow Cytometric Analysis of DC and Treg Subpopulations
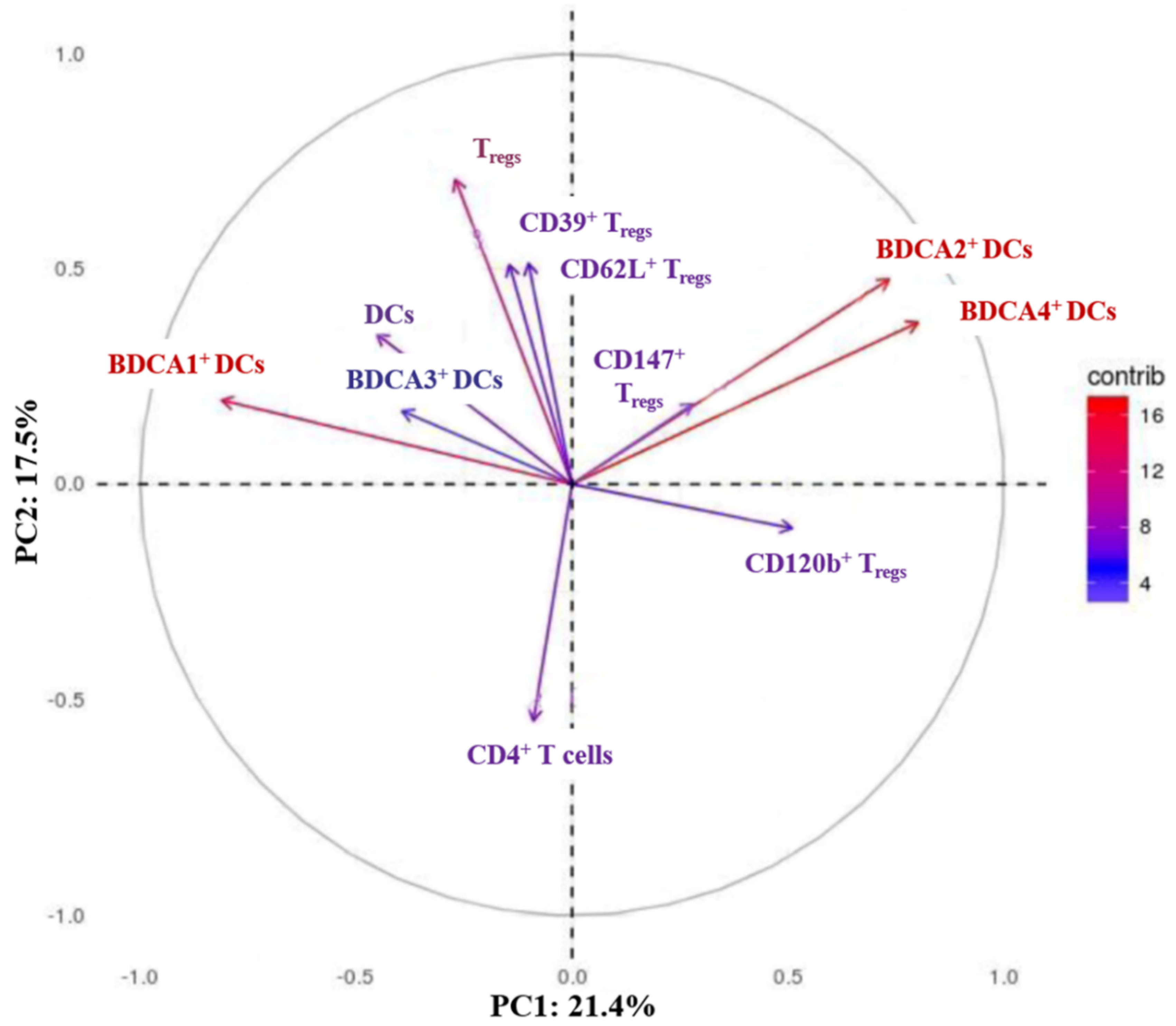
2.4. Principle Component Analysis
2.5. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Immunological Group Comparison
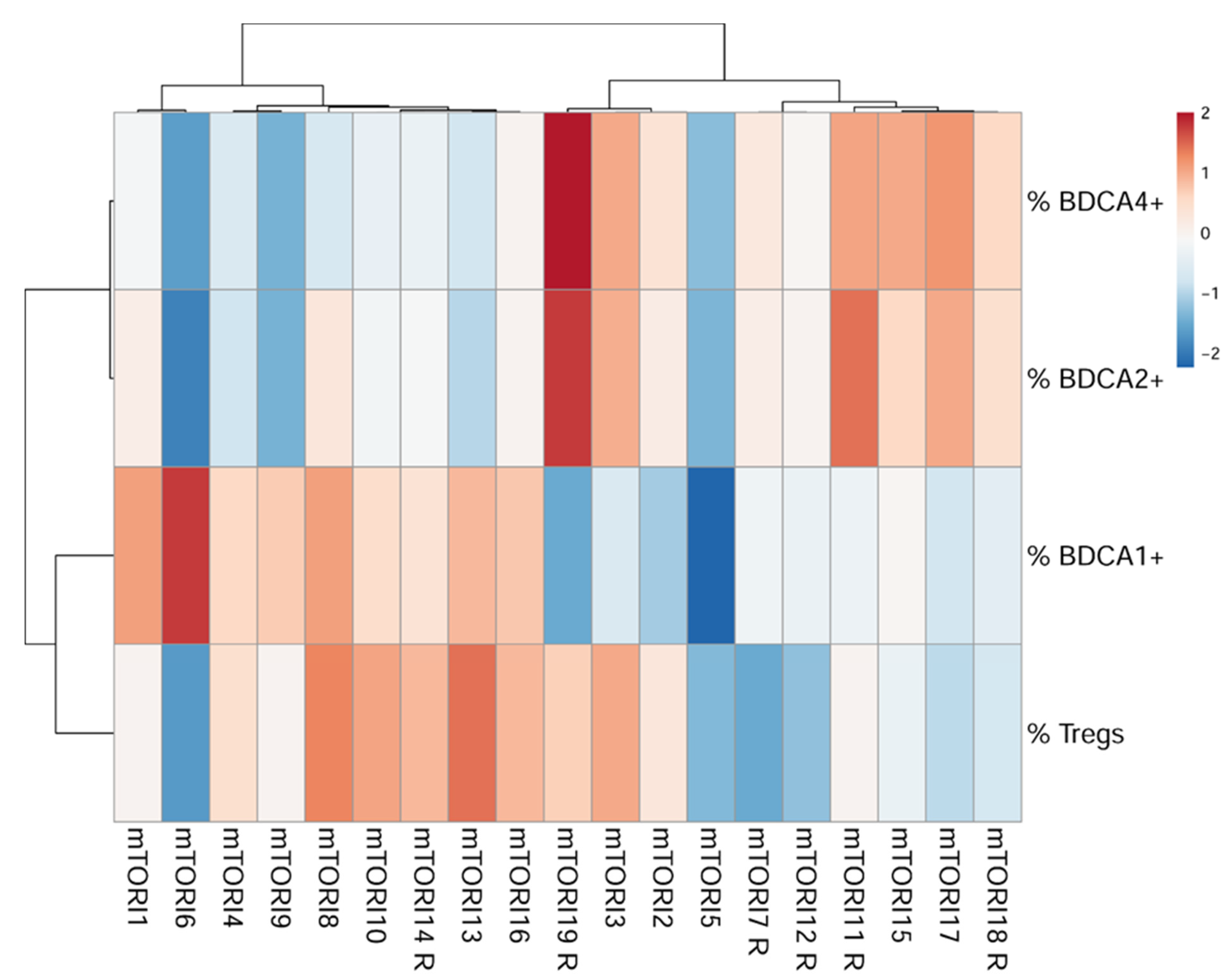
3.3. Creating a Monitoring Tool
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Potena, L.; Pellegrini, C.; Grigioni, F.; Amarelli, C.; Livi, U.; Maccherini, M.; Masciocco, G.; Faggian, G.; Monica, P.L.D.; Gerosa, G.; et al. Optimizing the Safety Profile of Everolimus by Delayed Initiation in De Novo Heart Transplant Recipients: Results of the Prospective Randomized Study EVERHEART. Transplantation 2018, 102, 493–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisen, H.J.; Kobashigawa, J.; Starling, R.C.; Pauly, D.F.; Kfoury, A.; Ross, H.; Wang, S.-S.; Cantin, B.; Van Bakel, A.; Ewald, G.; et al. Everolimus Versus Mycophenolate Mofetil in Heart Transplantation: A Randomized, Multicenter Trial. Arab. Archaeol. Epigr. 2013, 13, 1203–1216. [Google Scholar] [CrossRef] [PubMed]
- Radegran, G.; Arora, S.; Gustafsson, F.; Gullestad, L.; Dellgren, G.; Andersson, B.; Andreassen, A.K.; Jansson, K.; Sigurdardottir, V.; Solbu, D.; et al. Everolimus initiation and early calcineurin inhibitor withdrawal in heart transplant recipients: A randomized trial. Am. J. Transplant. 2014, 14, 1828–1838. [Google Scholar] [CrossRef]
- Barten, M.J.; Hirt, S.W.; Garbade, J.; Bara, C.; Doesch, A.O.; Knosalla, C.; Grinninger, C.; Stypmann, J.; Sieder, C.; Lehmkuhl, H.B.; et al. Comparing everolimus-based immunosuppression with reduction or withdrawal of calcineurin inhibitor reduction from 6 months after heart transplantation: The randomized MANDELA study. Arab. Archaeol. Epigr. 2019, 19, 3006–3017. [Google Scholar] [CrossRef] [PubMed]
- Lehmkuhl, H.B.; Arizon, J.; Viganò, M.; Almenar, L.; Gerosa, G.; Maccherini, M.; Varnous, S.; Musumeci, F.; Hexham, J.M.; Mange, K.C.; et al. Everolimus With Reduced Cyclosporine Versus MMF With Standard Cyclosporine in De Novo Heart Transplant Recipients. Transplantation 2009, 88, 115–122. [Google Scholar] [CrossRef]
- Zuckermann, A.; Osorio-Jaramillo, E.; Aliabadi-Zuckermann, A.Z. mTOR Inhibition and Clinical Transplantation: Heart. Transplantation 2018, 102, S27–S29. [Google Scholar] [CrossRef]
- Arora, S.; Andreassen, A.K.; Karason, K.; Gustafsson, F.; Eiskjær, H.; Bøtker, H.E.; Rådegran, G.; Gude, E.; Ioanes, D.; Solbu, D.; et al. Effect of Everolimus Initiation and Calcineurin Inhibitor Elimination on Cardiac Allograft Vasculopathy in De Novo Heart Transplant Recipients. Circ. Heart Fail. 2018, 11, e004050. [Google Scholar] [CrossRef] [Green Version]
- Stallone, G.; Infante, B.; Di Lorenzo, A.; Rascio, F.; Zaza, G.; Grandaliano, G. mTOR inhibitors effects on regulatory T cells and on dendritic cells. J. Transl. Med. 2016, 14, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klaeske, K.; Lehmann, S.; Büttner, P.; Palitzsch, R.; Fischer, J.; Jawad, K.; Garbade, J.; Borger, M.A.; Barten, M.J.; Dieterlen, M.-T. Identification of the immunological profile in rejection-free heart transplantation. Transpl. Immunol. 2020, 59, 101259. [Google Scholar] [CrossRef] [PubMed]
- Deaglio, S.; Dwyer, K.M.; Gao, W.; Friedman, D.; Usheva, A.; Erat, A.; Chen, J.-F.; Enjyoji, K.; Linden, J.; Oukka, M.; et al. Adenosine generation catalyzed by CD39 and CD73 expressed on regulatory T cells mediates immune suppression. J. Exp. Med. 2007, 204, 1257–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romano, M.; Fanelli, G.; Albany, C.J.; Giganti, G.; Lombardi, G. Past, Present, and Future of Regulatory T Cell Therapy in Transplantation and Autoimmunity. Front. Immunol. 2019, 10, 43. [Google Scholar] [CrossRef] [Green Version]
- Duggleby, R.; Danby, R.D.; Madrigal, A.; Saudemont, A. Clinical Grade Regulatory CD4+ T Cells (Tregs): Moving Toward Cellular-Based Immunomodulatory Therapies. Front. Immunol. 2018, 9, 252. [Google Scholar] [CrossRef]
- Thomson, A.W.; Turnquist, H.R.; Raimondi, G. Immunoregulatory functions of mTOR inhibition. Nat. Rev. Immunol. 2009, 9, 324–337. [Google Scholar] [CrossRef] [Green Version]
- Cegielska, A.; Lisowska, K.A.; Dębska-Ślizień, A.; Imko-Walczuk, B.; Okuniewska, A.; Rutkowski, B. Evaluation of quantitative changes in regulatory T cells in peripheral blood of kidney transplant recipients with skin cancer after conversion to mTOR inhibitors. Adv. Dermatol. Allergol. 2018, 35, 474–480. [Google Scholar] [CrossRef]
- San Segundo, D.; Fernández-Fresnedo, G.; Gago, M.; Beares, I.; Ruiz-Criado, J.; González, M.; Ruiz, J.C.; Gómez-Alamillo, C.; Arias, M.; López-Hoyos, M. Number of peripheral blood regulatory T cells and lymphocyte activation at 3 months after conversion to mTOR inhibitor therapy. Transpl. Proc. 2010, 42, 2871–2873. [Google Scholar] [CrossRef] [PubMed]
- Ma, A.; Qi, S.; Song, L.; Hu, Y.; Dun, H.; Massicotte, E.; Dupuis, M.; Daloze, P.; Chen, H. Adoptive transfer of CD4+CD25+ regulatory cells combined with low-dose sirolimus and anti-thymocyte globulin delays acute rejection of renal allografts in Cynomolgus monkeys. Int. Immunopharmacol. 2011, 11, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Segundo, D.S.; Ruiz, J.C.; Izquierdo, M.; Fernández-Fresnedo, G.; Gómez-Alamillo, C.; Merino, R.; Benito, M.J.; Cacho, E.; Rodrigo, E.; Palomar, R.; et al. Calcineurin Inhibitors, but not Rapamycin, Reduce Percentages of CD4+CD25+FOXP3+ Regulatory T Cells in Renal Transplant Recipients. Transplantation 2006, 82, 550–557. [Google Scholar] [CrossRef]
- Salcido-Ochoa, F.; Tsang, J.; Tam, P.; Falk, K.; Rotzschke, O. Regulatory T cells in transplantation: Does extracellular adenosine triphosphate metabolism through CD39 play a crucial role? Transplant. Rev. 2010, 24, 52–66. [Google Scholar] [CrossRef]
- Dwyer, K.M.; Hanidziar, D.; Putheti, P.; A Hill, P.; Pommey, S.; McRae, J.L.; Winterhalter, A.; Doherty, G.; Deaglio, S.; Koulmanda, M.; et al. Expression of CD39 by Human Peripheral Blood CD4+CD25+ T Cells Denotes a Regulatory Memory Phenotype. Arab. Archaeol. Epigr. 2010, 10, 2410–2420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McRae, J.L.; Chia, J.S.; Pommey, S.A.; Dwyer, K.M. Evaluation of CD4 + CD25 +/− CD39 + T-cell populations in peripheral blood of patients following kidney transplantation and during acute allograft rejection. Nephrology 2017, 22, 505–512. [Google Scholar] [CrossRef]
- Masetti, M.; Potena, L.; Nardozza, M.; Prestinenzi, P.; Taglieri, N.; Saia, F.; Pece, V.; Magnani, G.; Fallani, F.; Coccolo, F.; et al. Differential Effect of Everolimus on Progression of Early and Late Cardiac Allograft Vasculopathy in Current Clinical Practice. Arab. Archaeol. Epigr. 2013, 13, 1217–1226. [Google Scholar] [CrossRef]
- Eisen, H.J.; Hasni, S.F.; Wang, D. The Return of the mTOR Inhibitors: Getting it Right in Patients After Cardiac Transplantation. J. Am. Coll. Cardiol. 2018, 71, 651–653. [Google Scholar] [CrossRef] [PubMed]
- Pilat, N.; Farkas, A.M.; Mahr, B.; Schwarz, C.; Unger, L.; Hock, K.; Oberhuber, R.; Aumayr, K.; Wrba, F.; Wekerle, T. T-regulatory cell treatment prevents chronic rejection of heart allografts in a murine mixed chimerism model. J. Heart Lung Transplant. 2014, 33, 429–437. [Google Scholar] [CrossRef] [Green Version]
- Saber-Moghaddam, N.; Nomani, H.; Sahebkar, A.; Johnston, T.P.; Mohammadpour, A.H. The change of immunosuppressive regimen from calcineurin inhibitors to mammalian target of rapamycin (mTOR) inhibitors and its effect on malignancy following heart transplantation. Int. Immunopharmacol. 2019, 69, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Waldner, M.; Fantus, D.; Solari, M.; Thomson, A.W. New perspectives on mTOR inhibitors (rapamycin, rapalogs and TORKinibs) in transplantation. Br. J. Clin. Pharmacol. 2016, 82, 1158–1170. [Google Scholar] [CrossRef] [Green Version]
- Deluce-Kakwata-Nkor, N.; Lamendour, L.; Chabot, V.; Héraud, A.; Ivanovic, Z.; Halary, F.; Dehaut, F.; Velge-Roussel, F. Differentiation of human dendritic cell subsets for immune tolerance induction. Transfus. Clin. Biol. 2018, 25, 90–95. [Google Scholar] [CrossRef] [Green Version]
- Gehrie, E.; Van der Touw, W.; Bromberg, J.S.; Ochando, J.C. Plasmacytoid Dendritic Cells in Tolerance. Springer Protoc. Handb. 2010, 677, 127–147. [Google Scholar] [CrossRef] [Green Version]
- Dieterlen, M.-T.; John, K.; Reichenspurner, H.; Mohr, F.W.; Barten, M.J. Dendritic Cells and Their Role in Cardiovascular Diseases: A View on Human Studies. J. Immunol. Res. 2016, 2016, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Hackstein, H.; Taner, T.; Logar, A.J.; Thomson, A.W. Rapamycin inhibits macropinocytosis and mannose receptor–mediated endocytosis by bone marrow–derived dendritic cells. Blood 2002, 100, 1084–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackstein, H.; Taner, T.; Zahorchak, A.F.; Morelli, A.E.; Logar, A.J.; Gessner, A.; Thomson, A.W. Rapamycin inhibits IL-4—induced dendritic cell maturation in vitro and dendritic cell mobilization and function in vivo. Blood 2003, 101, 4457–4463. [Google Scholar] [CrossRef]
- Biswas, M.; Sarkar, D.; Kumar, S.R.; Nayak, S.; Rogers, G.L.; Markusic, D.M.; Liao, G.; Terhorst, C.; Herzog, R.W. Synergy between rapamycin and FLT3 ligand enhances plasmacytoid dendritic cell-dependent induction of CD4 + CD25 + FoxP3 + Treg. Blood 2015, 125, 2937–2947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, N.; Isenberg, J.; Thomson, A. Plasmacytoid Dendritic Cells: No Longer an Enigma and Now Key to Transplant Tolerance? Arab. Archaeol. Epigr. 2013, 13, 1125–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, K.; Dieterlen, M.-T.; Tárnok, A.; Garbade, J.; Bittner, H.B.; Mohr, F.W.; Barten, M.J. Role of dendritic cells in the context of acute cellular rejection: Comparison between Tacrolimus- or Cyclosporine A-treated heart transplanted recipients. Cytom. Part B Clin. Cytom. 2014, 86, 362–367. [Google Scholar] [CrossRef]
- Dieterlen, M.-T.; Bittner, H.B.; Pierzchalski, A.; Dhein, S.; Mohr, F.W.; Barten, M.J. Immunological monitoring of extracorporeal photopheresis after heart transplantation. Clin. Exp. Immunol. 2014, 176, 120–128. [Google Scholar] [CrossRef]
- Obregon, C.; Kumar, R.; Pascual, M.A.; Vassalli, G.; Golshayan, D. Update on Dendritic Cell-Induced Immunological and Clinical Tolerance. Front. Immunol. 2017, 8, 1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| mTORI-Group n = 19 | CNI-Group n = 20 | p Value | |
|---|---|---|---|
| age at HTx (years) | 53.8 ± 9.5 | 52.9 ± 10.5 | 0.78 |
| age at study begin (years) | 59.7 ± 8.7 | 56.7 ± 10.9 | 0.96 |
| male gender | 14 (74%) | 14 (70%) | 0.80 |
| BMI (kg/m2) | 26.9 ± 4.8 | 28.0 ± 4.6 | 0.47 |
| diagnosis leading to HTx-listing | 0.62 | ||
| ICM | 6 (32%) | 9 (45%) | |
| DCM | 11 (58%) | 10 (50%) | |
| congenital heart disease | 2 (11%) | 1 (5%) | |
| assist device prior HTx | 6 (32%) | 6 (30%) | 0.92 |
| rejection | 6 (32%) | 11 (55%) | 0.14 |
| CMV-positivity | 0 (0%) | 1 (5%) | 0.32 |
| initial IS therapy | 0.14 | ||
| TAC + MMF + GC | 18 (95%) | 14 (70%) | |
| CsA + MMF + GC | 0 (0%) | 3 (15%) | |
| CsA + ERL + GC | 0 (0%) | 2 (10%) | |
| ERL + MMF + GC | 1 (5%) | 1 (5%) | |
| IS therapy at study begin | |||
| TAC + MMF + GC | - | 15 (75%) | |
| CsA + MMF + GC | - | 5 (25%) | |
| ERL + MMF + GC | 15 (79%) | - | |
| ERL + MMF | 4 (21%) | - | |
| trough level of IS at study begin # | 18 (100%) * | 12 (60%) | <0.01 |
| mTORI-Group n = 19 | CNI-Group n = 20 | p Value | |
|---|---|---|---|
| Hypertension | 8 (42%) | 14 (70%) | 0.11 |
| Cardiac arrhythmia | 0 (0%) | 2 (10%) | 0.48 |
| Pacemaker/ICD | 4 (21%) | 4 (20%) | 1 |
| COPD/Asthma bronchiale | 1 (5%) | 1 (5%) | 1 |
| Diabetes mellitus type 2 | 5 (26%) | 6 (30%) | 1 |
| Hyperlipidemia | 7 (37%) | 10 (50%) | 0.52 |
| Hyperuricemia | 4 (21%) | 6 (30%) | 0.72 |
| Renal insufficiency * | 11 (58%) | 12 (60%) | 1 |
| grade 1 | 2 (11%) | 0 (0%) | 0.23 |
| grade 2 | 3 (16%) | 1 (5%) | 0.34 |
| grade 3 | 6 (32%) | 10 (50%) | 0.33 |
| grade 4 | 0 (0%) | 1 (5%) | 1 |
| Neurological diseases 1 | 3 (16%) | 6 (30%) | 0.45 |
| Hematological diseases 2 | 0 (0%) | 1 (5%) | 1 |
| Neoplasia 3 | 1 (5%) | 4 (20%) | 0.34 |
| Chronic inflammation 4 | 2 (10%) | 2 (10%) | 1 |
| Allergies | 1 (5%) | 3 (15%) | 0.61 |
| mTORI-Group n = 19 | CNI-Group n = 20 | p Value | |
|---|---|---|---|
| DCs/PBMCs [%] | 0.68 ± 0.29 | 0.56 ± 0.28 | 0.18 |
| BDCA1+ mDCs/DCs [%] | 26.4 ± 9.5 | 30.2 ± 9.2 | 0.21 |
| BDCA2+ pDCs/DCs [%] | 58.3 ± 11.5 | 53.3 ± 11.1 | 0.17 |
| BDCA3+ mDCs/DCs [%] | 24.2 ± 10.1 | 27.0 ± 8.4 | 0.36 |
| BDCA4+ pDCs/DCs [%] | 79.6 ± 10.6 | 70.0 ± 27.5 | 0.16 |
| MFI BDCA1 [U] | 16,985 ± 7058 | 15,550 ± 4204 | 0.44 |
| MFI BDCA2 [U] | 19,205 ± 7504 | 20,876 ± 7469 | 0.49 |
| MFI BDCA3 [U] | 1803 ± 412 | 3654 ± 4727 | 0.10 |
| MFI BDCA4 [U] | 2539 ± 1142 | 2077 ± 612 | 0.12 |
| CD4+ T cells/total T cells [%] | 20.7 ± 7.5 | 22.6 ± 8.4 | 0.48 |
| Tregs/total T cells [%] | 11.6 ± 3.5 | 9.0 ± 2.9 | 0.02 |
| CD120b+ Tregs/total T cells [%] | 87.2 ± 8.4 | 86.7 ± 9.3 | 0.85 |
| CD147+ Tregs/total T cells [%] | 97.7 ± 2.8 | 97.3 ± 7.7 | 0.84 |
| CD39+ Tregs/total T cells [%] | 35.5 ± 16.3 | 26.6 ± 10.9 | 0.05 |
| CD62L+ Tregs/total T cells [%] | 86.9 ± 12.5 | 84.3 ± 9.6 | 0.48 |
| MFI CD120b [U] | 1688 ± 323 | 1613 ± 214 | 0.85 |
| MFI CD147 [U] | 1769 ± 389 | 2065 ± 557 | 0.06 |
| MFI CD39 [U] | 783 ± 216 | 901 ± 307 | 0.17 |
| MFI CD62L [U] | 10,491 ± 2530 | 9441 ± 2189 | 0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klaeske, K.; Lehmann, S.; Palitzsch, R.; Büttner, P.; Barten, M.J.; Jawad, K.; Eifert, S.; Saeed, D.; Borger, M.A.; Dieterlen, M.-T. Everolimus-Induced Immune Effects after Heart Transplantation: A Possible Tool for Clinicians to Monitor Patients at Risk for Transplant Rejection. Life 2021, 11, 1373. https://doi.org/10.3390/life11121373
Klaeske K, Lehmann S, Palitzsch R, Büttner P, Barten MJ, Jawad K, Eifert S, Saeed D, Borger MA, Dieterlen M-T. Everolimus-Induced Immune Effects after Heart Transplantation: A Possible Tool for Clinicians to Monitor Patients at Risk for Transplant Rejection. Life. 2021; 11(12):1373. https://doi.org/10.3390/life11121373
Chicago/Turabian StyleKlaeske, Kristin, Sven Lehmann, Robert Palitzsch, Petra Büttner, Markus J. Barten, Khalil Jawad, Sandra Eifert, Diyar Saeed, Michael A. Borger, and Maja-Theresa Dieterlen. 2021. "Everolimus-Induced Immune Effects after Heart Transplantation: A Possible Tool for Clinicians to Monitor Patients at Risk for Transplant Rejection" Life 11, no. 12: 1373. https://doi.org/10.3390/life11121373
APA StyleKlaeske, K., Lehmann, S., Palitzsch, R., Büttner, P., Barten, M. J., Jawad, K., Eifert, S., Saeed, D., Borger, M. A., & Dieterlen, M. -T. (2021). Everolimus-Induced Immune Effects after Heart Transplantation: A Possible Tool for Clinicians to Monitor Patients at Risk for Transplant Rejection. Life, 11(12), 1373. https://doi.org/10.3390/life11121373