
Idiopathic Intracranial Hypertension: Evaluation of Admissions and Emergency Readmissions through the Hospital Episode Statistic Dataset between 2002–2020


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection
2.3. Statistical Analysis
2.4. Data Sharing Agreement
3. Results
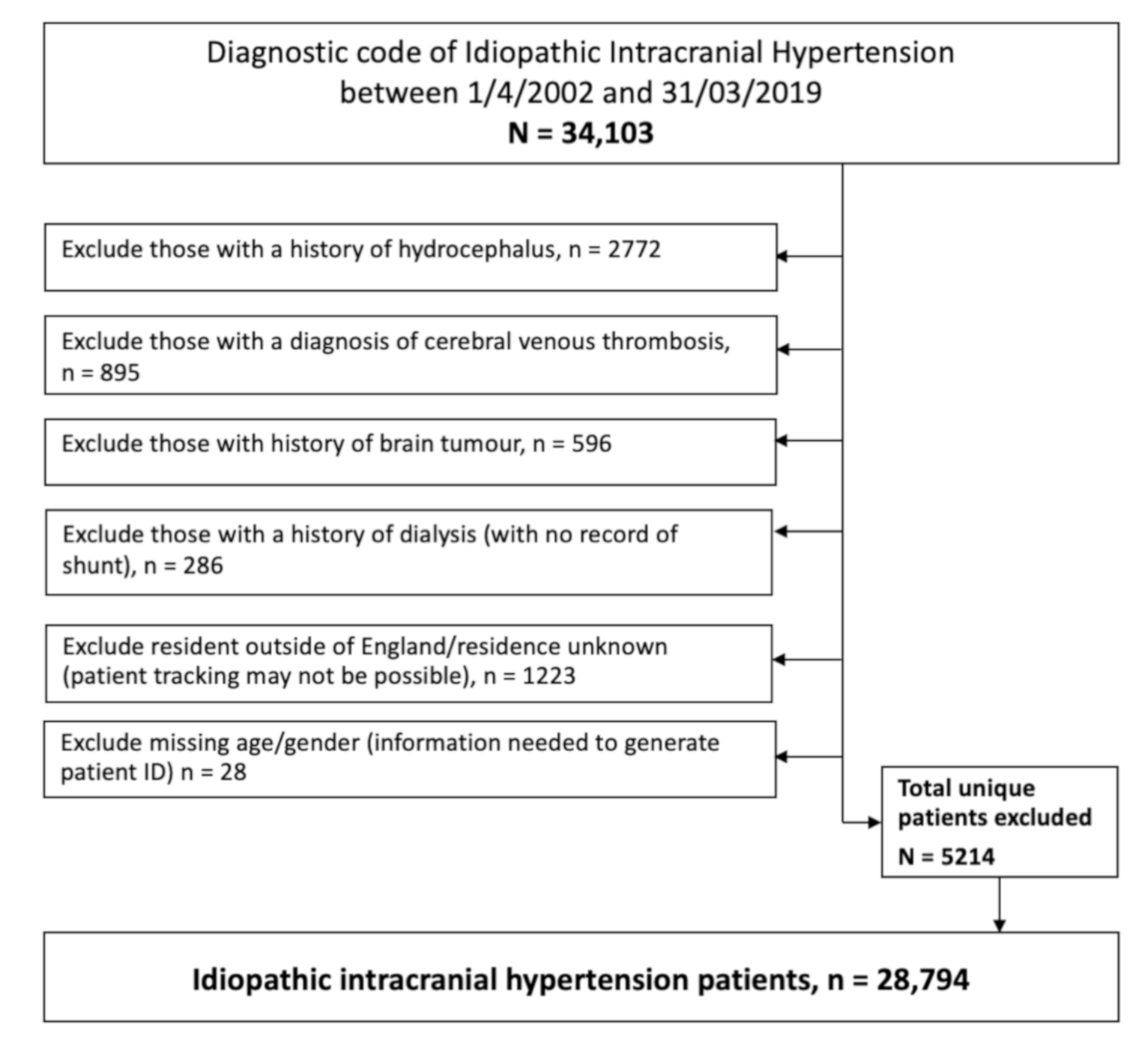
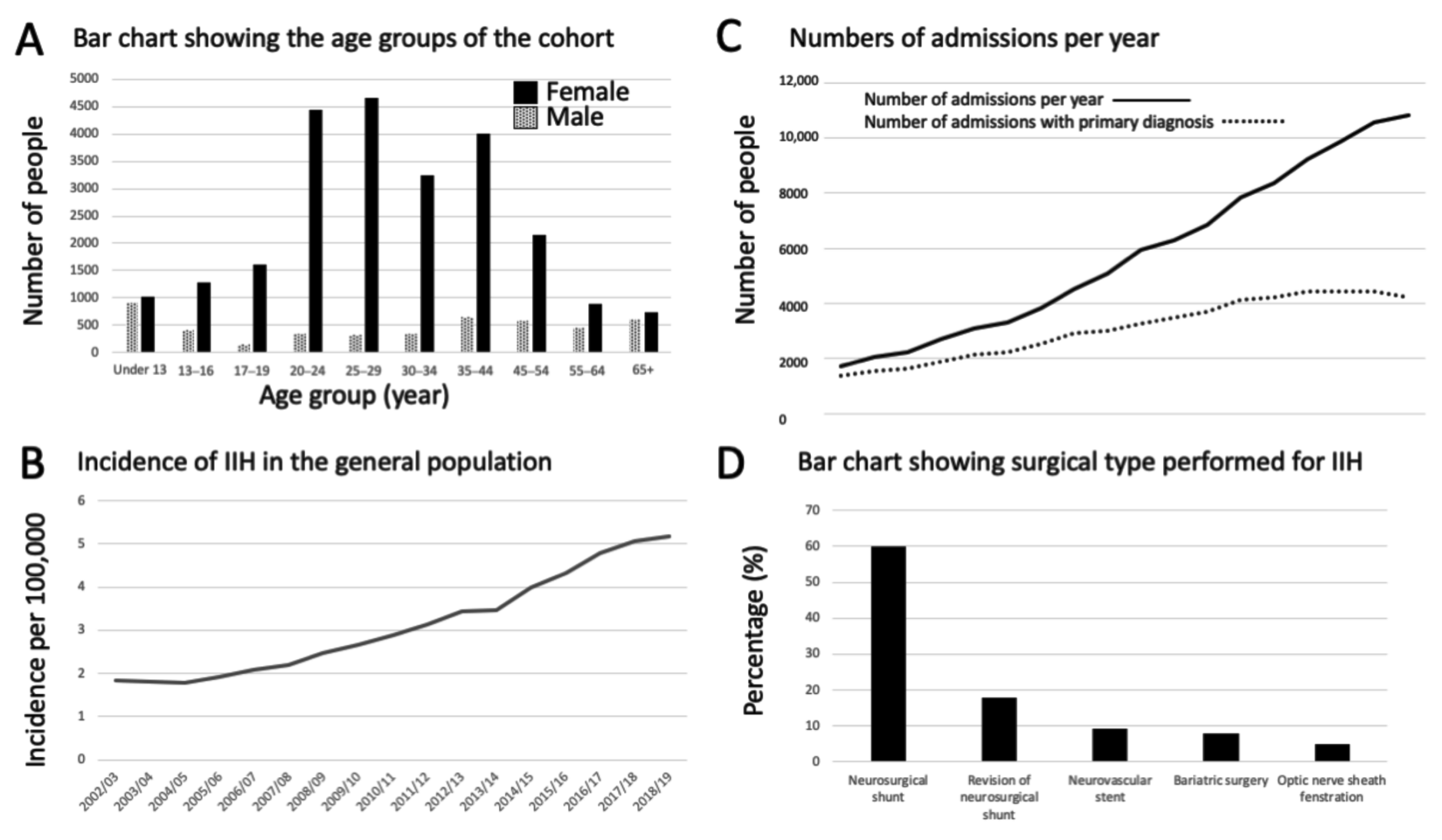
3.1. Baseline Characteristics
3.2. Hospital Admissions
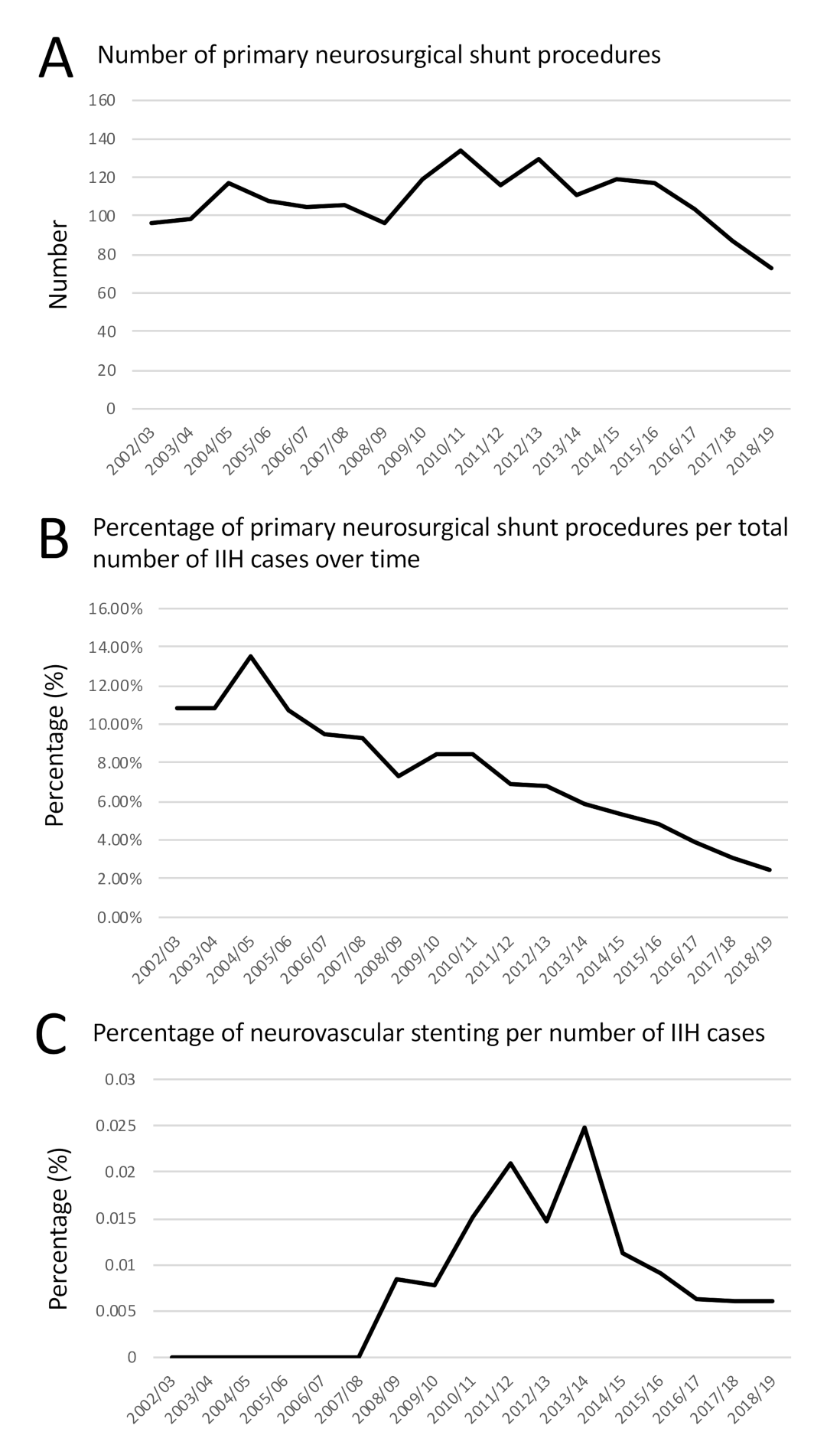
3.3. Management of IIH
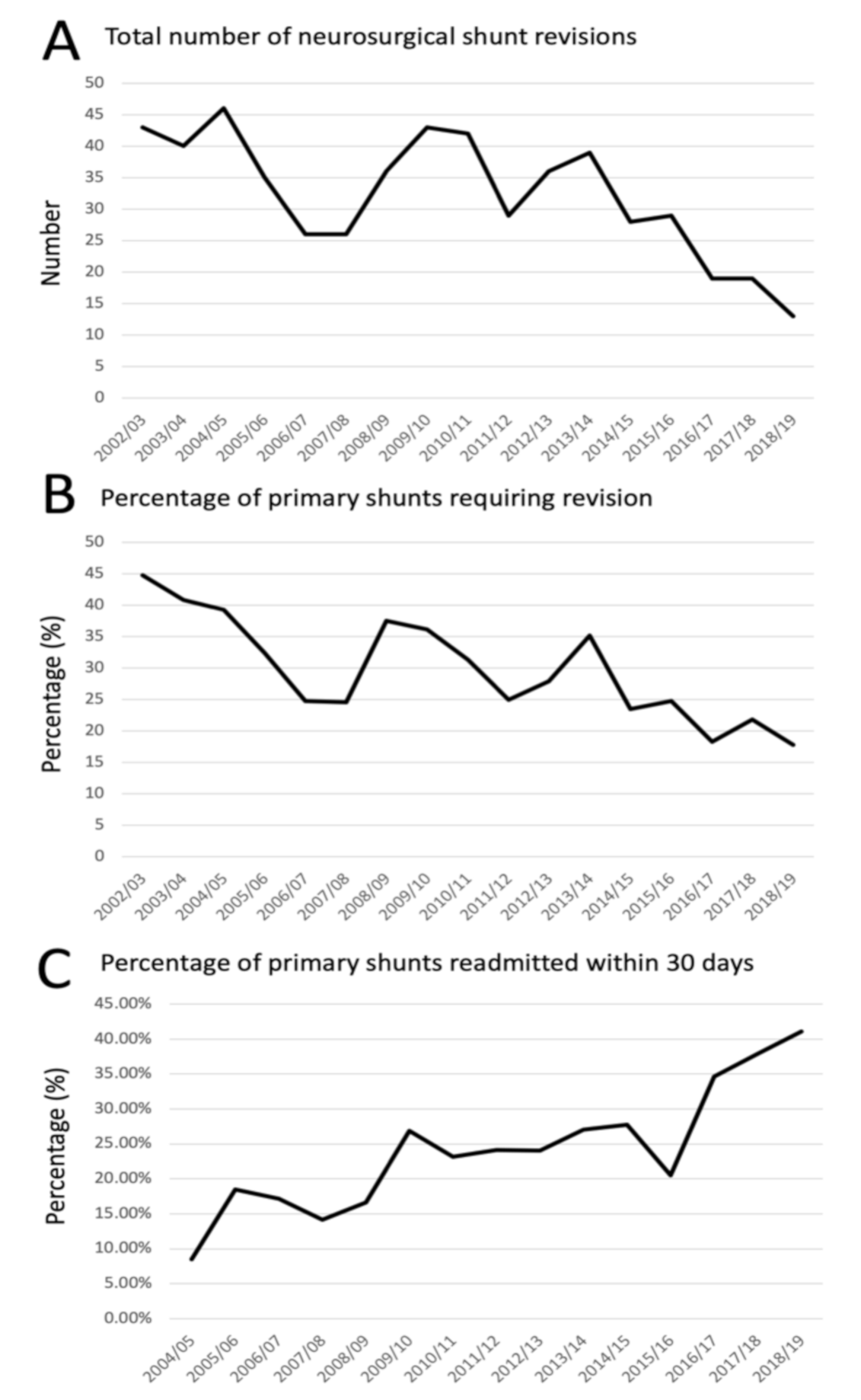
3.4. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grech, O.; Mollan, S.P.; Wakerley, B.R.; Alimajstorovic, Z.; Lavery, G.G.; Sinclair, A.J. Emerging themes in idiopathic intracranial hypertension. J. Neurol. 2020, 267, 3776–3784. [Google Scholar] [CrossRef] [PubMed]
- Virdee, J.; Larcombe, S.; Vijay, V.; Sinclair, A.J.; Dayan, M.; Mollan, S.P. Reviewing the Recent Developments in Idiopathic Intracranial Hypertension. Ophthalmol. Ther. 2020, 9, 767–781. [Google Scholar] [CrossRef] [PubMed]
- Mollan, S.P.; Aguiar, M.; Evison, F.; Frew, E.; Sinclair, A.J. The expanding burden of idiopathic intracranial hypertension. Eye 2019, 33, 478–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adderley, N.J.; Subramanian, A.; Nirantharakumar, K.; Yiangou, A.; Gokhale, K.M.; Mollan, S.P.; Sinclair, A.J. Association between idiopathic intracranial hypertension and risk of cardiovascular diseases in women in the United Kingdom. JAMA Neurol. 2019, 76, 1088–1098. [Google Scholar] [CrossRef] [PubMed]
- McCluskey, G.; Doherty-Allan, R.; McCarron, P.; Loftus, A.M.; Mulholland, D.; McVerry, F.; McCarron, M.O. Meta-analysis and systematic review of population-based epidemiological studies in idiopathic intracranial hypertension. Eur. J. Neurol. 2018, 25, 1218–1227. [Google Scholar] [CrossRef] [PubMed]
- Mulla, Y.; Markey, K.A.; Woolley, R.L.; Patel, S.; Mollan, S.P.; Sinclair, A.J. Headache determines quality of life in idiopathic intracranial hypertension. J. Headache Pain 2015, 16, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakerley, B.R.; Mollan, S.P.; Sinclair, A.J. Idiopathic intracranial hypertension: Update on diagnosis and management. Clin. Med. 2020, 20, 384–388. [Google Scholar] [CrossRef]
- Mollan, S.P.; Hoffmann, J.; Sinclair, A.J. Advances in the understanding of headache in idiopathic intracranial hypertension. Curr. Opin. Neurol. 2019, 32, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Thaller, M.; Tsermoulas, G.; Sun, R.; Mollan, S.P.; Sinclair, A.J. Negative impact of COVID-19 lockdown on papilloedema and idiopathic intracranial hypertension. J. Neurol. Neurosurg. Psychiatry 2020. [Google Scholar] [CrossRef]
- Mollan, S.P.; Tahrani, A.A.; Sinclair, A.J. The Potentially Modifiable Risk Factor in Idiopathic Intracranial Hypertension: Body Weight. Neurol. Clin. Pract. 2021. [Google Scholar] [CrossRef]
- Hornby, C.; Mollan, S.P.; Botfield, H.; O’Reilly, M.W.; Sinclair, A.J. Metabolic Concepts in Idiopathic Intracranial Hypertension and Their Potential for Therapeutic Intervention. J. Neuroophthalmol. 2018, 38, 522–530. [Google Scholar] [CrossRef]
- Botfield, H.F.; Uldall, M.S.; Westgate, C.S.J.; Mitchell, J.L.; Hagen, S.M.; Gonzalez, A.M.; Hodson, D.J.; Jensen, R.H.; Sinclair, A.J. A glucagon-like peptide-1 receptor agonist reduces intracranial pressure in a rat model of hydrocephalus. Sci. Transl. Med. 2017, 9, eaan0972. [Google Scholar] [CrossRef] [Green Version]
- O’Reilly, M.W.; Westgate, C.S.; Hornby, C.; Botfield, H.; Taylor, A.E.; Markey, K.; Mitchell, J.L.; Scotton, W.J.; Mollan, S.P.; Yiangou, A.; et al. A unique androgen excess signature in idiopathic intracranial hypertension is linked to cerebrospinal fluid dynamics. JCI Insight 2019, 4, e125348. [Google Scholar] [CrossRef] [Green Version]
- Hardy, R.S.; Botfield, H.; Markey, K.; Mitchell, J.L.; Alimajstorovic, Z.; Westgate, C.S.J.; Sagmeister, M.; Fairclough, R.J.; Ottridge, R.S.; Yiangou, A.; et al. 11βHSD1 Inhibition with AZD4017 Improves Lipid Profiles and Lean Muscle Mass in Idiopathic Intracranial Hypertension. J. Clin. Endocrinol. Metab. 2021, 106, 174–187. [Google Scholar] [CrossRef]
- Mitchell, J.L.; Mollan, S.P.; Walker, J. A randomised controlled, trial of the GLP-1 receptor agonist Exenatide in Idiopathic Intracranial Hypertension. European Headache Federation meeting 2020 14th European Headache Federation Congress 2020, Meeting Abstracts. J. Headache Pain 2020, in press. [Google Scholar]
- Markey, K.; Mitchell, J.; Botfield, H.; Ottridge, R.S.; Matthews, T.; Krishnan, A.; Woolley, R.; Westgate, C.; Yiangou, A.; Alimajstorovic, Z.; et al. 11β-Hydroxysteroid dehydrogenase type 1 inhibition in idiopathic intracranial hypertension: A double-blind randomized controlled trial. Brain Commun. 2020, 2, fcz050. [Google Scholar] [CrossRef] [Green Version]
- Mollan, S.P.; Mitchell, J.L.; Ottridge, R.S.; Aguiar, M.; Yiangou, A.; Alimajstorovic, Z.; Cartwright, D.M.; Grech, O.; Lavery, G.G.; Westgate, C.S.J.; et al. Bariatric surgery versus community weight management intervention for the treatment of idiopathic intracranial hypertension (IIH:WT): A randomized controlled trial. JAMA Neurol. 2021. [Google Scholar] [CrossRef]
- Ottridge, R.; Mollan, S.P.; Botfield, H.; Frew, E.; Ives, N.J.; Matthews, T.; Mitchell, J.; Rick, C.; Singhal, R.; Woolley, R.; et al. Randomised controlled trial of bariatric surgery versus a community weight loss programme for the sustained treatment of idiopathic intracranial hypertension: The Idiopathic Intracranial Hypertension Weight Trial (IIH:WT) protocol. BMJ Open. 2017, 7, e017426. [Google Scholar] [CrossRef] [Green Version]
- Yiangou, A.; Mitchell, J.L.; Fisher, C.; Edwards, J.; Vijay, V.; Alimajstorovic, Z.; Grech, O.; Lavery, G.G.; Mollan, S.P.; Sinclair, A.J. Erenumab for headaches in idiopathic intracranial hypertension: A prospective open-label evaluation. Headache 2020, 14. [Google Scholar] [CrossRef]
- Piper, R.J.; Kalyvas, A.V.; Young, A.M.H.; Hughes, A.M.; Jamjoom, A.A.B.; Fouyas, I.P. Interventions for idiopathic intracranial hypertension. Cochrane Database Syst. Rev. 2015, 8, CD003434. [Google Scholar] [CrossRef]
- Hassan-Smith, G.; Mollan, S.; Davies, B.; Shaw, S.; Chavda, S.V.; Krishnan, A.; Mallucci, C.L.; Silver, N.; Wakerley, B.R.; Sinclair, A.J. Interdisciplinary consensus on the management of IIH in the UK. J. Neurol. Neurosurg. Psychiatry 2016, 87, e1. [Google Scholar] [CrossRef]
- Mollan, S.P.; Hornby, C.; Mitchell, J.; Sinclair, A.J. Evaluation and management of adult idiopathic intracranial hypertension. Pract. Neurol. 2018, 18, 485–488. [Google Scholar] [CrossRef] [PubMed]
- Mollan, S.P.; Davies, B.; Silver, N.C.; Shaw, S.; Mallucci, C.L.; Wakerley, B.R.; Krishnan, A.; Chavda, S.V.; Ramalingam, S.; Edwards, J.; et al. Idiopathic intracranial hypertension: Consensus guidelines on management. J. Neurol. Neurosurg. Psychiatry 2018, 8, 1088–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, J.; Mollan, S.P.; Paemeleire, K.; Lampl, C.; Jensen, R.H.; Sinclair, A.J. European headache federation guideline on idiopathic intracranial hypertension. J. Headache Pain 2018, 19, 93. [Google Scholar] [CrossRef]
- Mollan, S.; Hemmings, K.; Herd, C.P.; Denton, A.; Williamson, S.; Sinclair, A.J. What are the research priorities for idiopathic intracranial hypertension? A priority setting partnership between patients and healthcare professionals. BMJ Open 2019, 9, e026573. [Google Scholar] [CrossRef] [Green Version]
- International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). Available online: https://www.cdc.gov/nchs/icd/icd10cm.htm (accessed on 23 March 2021).
- Available online: https://datadictionary.nhs.uk/supporting_information/opcs_classification_of_interventions_and_procedures.html (accessed on 23 March 2021).
- The English Indices of Deprivation 2010. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/6320/1870718.pdf (accessed on 23 March 2021).
- Murphy, S.; Friesner, D.L.; Rosenman, R.; Waslo, C.S.; Au, J.; Tanne, E. Emergency department utilization among individuals with idiopathic intracranial hypertension. Int. J. Health Care Qual. Assur. 2019, 32, 152–163. [Google Scholar] [CrossRef]
- Merkler, A.E.; Ch’ang, J.; Parker, W.E.; Murthy, S.B.; Kamel, H. The Rate of Complications after Ventriculoperitoneal Shunt Surgery. World Neurosurg. 2017, 98, 654–658. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, N.; Kashkoush, A.; McDowell, M.M.; Lariviere, W.R.; Ismail, N.; Friedlander, R.M. Comparative durability and costs analysis of ventricular shunts. J. Neurosurg. 2018, 130, 1252–1259. [Google Scholar] [CrossRef] [Green Version]
- Abubaker, K.; Ali, Z.; Raza, K.; Bolger, C.; Rawluk, D.; O’Brien, D. Idiopathic intracranial hypertension: Lumbo-peritoneal shunts versus ventriculoperitoneal shunts—case series and literature review. Br. J. Neurosurg. 2011, 25, 94–99. [Google Scholar] [CrossRef]
- Tarnaris, A.; Toma, A.K.; Watkins, L.D.; Kitchen, N.D. Is there a difference in outcomes of patients with idiopathic intracranial hypertension with the choice of cerebrospinal fluid diversion site: A single centre experience. Clin. Neurol. Neurosurg. 2011, 113, 477–479. [Google Scholar] [CrossRef]
- Hickman, S.J.; Raoof, N.; Panesar, H.; McMullan, J.M.; Pepper, I.M.; Sharrack, B. Visual Outcomes from Shunting for Idiopathic Intracranial Hypertension. Neuroophthalmology 2014, 38, 310–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjornson, A.; Tapply, I.; Nabbanja, E.; Lalou, A.-D.; Czosnyka, M.; Czosnyka, Z.; Muthusamy, B.; Garnett, M. Ventriculo-peritoneal shunting is a safe and effective treatment for idiopathic intracranial hypertension. Br. J. Neurosurg. 2019, 33, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Schipmann, S.; Suero Molina, E.; Windheuser, J.; Doods, J.; Schwake, M.; Wilbers, E.; Alsofy, S.Z.; Warneke, N.; Stummer, W. The 30-day readmission rate in neurosurgery-a useful indicator for quality assessment? Acta Neurochir. 2020, 162, 2659–2669. [Google Scholar] [CrossRef]
- Hirayama, A.; Goto, T.; Faridi, M.K.; Camargo, C.A., Jr.; Hasegawa, K. Age-related differences in the rate and diagnosis of 30-day readmission after hospitalization for acute ischemic stroke. Int. J. Stroke 2018, 13, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Vahidy, F.S.; Donnelly, J.P.; McCullough, L.D.; Tyson, J.E.; Miller, C.C.; Boehme, A.K.; Savitz, S.I.; Albright, K.C. Nationwide Estimates of 30-Day Readmission in Patients with Ischemic Stroke. Stroke 2017, 48, 1386–1388. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.V.; Corado, C.; Bergman, D.; Curran, Y.; Bernstein, R.A.; Naidech, A.M.; Prabhakaran, S. Impact of Poststroke Medical Complications on 30-Day Readmission Rate. J. Stroke Cerebrovasc. Dis. 2015, 24, 1969–1977. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, C.C.; Hernandez, E.A.; Anderson, J.M.; Dye, J.A.; Leung, M.; Buxey, F.; Bergsneider, M.; Afsar-Manesh, N.; Pouratian, N.; Martin, N.A. Analysis of 30-day readmissions among neurosurgical patients: Surgical complication avoidance as key to quality improvement. J. Neurosurg. 2014, 121, 170–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donoho, D.A.; Buchanan, I.A.; Patel, A.; Ding, L.; Cen, S.; Wen, T.; Giannotta, S.L.; Attenello, F.; Mack, W.J. Early Readmission After Ventricular Shunting in Adults with Hydrocephalus: A Nationwide Readmission Database Analysis. World Neurosurg. 2019, 128, e38–e50. [Google Scholar] [CrossRef]
- Sinclair, A.J.; Kuruvath, S.; Sen, D.; Nightingale, P.G.; Burdon, M.A.; Flint, G. Is cerebrospinal fluid shunting in idiopathic intracranial hypertension worthwhile? A 10-year review. Cephalalgia 2011, 31, 1627–1633. [Google Scholar] [CrossRef]
- Gurney, S.P.; Ramalingam, S.; Thomas, A.; Sinclair, A.J.; Mollan, S.P. Exploring the Current Management Idiopathic Intracranial Hypertension, And Understanding the Role of Dural Venous Sinus Stenting. Eye Brain 2020, 12, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Malik, A.I.; Xu, J.; Lee, A.G. Outcomes of optic nerve sheath fenestration from superomedial eyelid crease approach. Orbit 2021, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jefferis, J.M.; Littlewood, R.A.; Pepper, I.M.; Hickman, S.J.; Salvi, S.M. Optic nerve sheath fenestration via a supero-medial eyelid skin crease approach for the treatment of idiopathic intracranial hypertension in a UK population. Eye 2020, 35, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Hamedani, A.G.; Thibault, D.P.; Revere, K.E.; Lee, J.Y.K.; Grady, M.S.; Willis, A.W.; Liu, G.T. Trends in the Surgical Treatment of Pseudotumor Cerebri Syndrome in the United States. JAMA Netw. Open 2020, 3, e2029669. [Google Scholar] [CrossRef] [PubMed]
- Fisayo, A.; Bruce, B.B.; Newman, N.J.; Biousse, V. Overdiagnosis of idiopathic intracranial hypertension. Neurology 2016, 86, 341–350. [Google Scholar] [CrossRef] [Green Version]
- Downie, P.A.; Chen, J.J.; Bhatti, M.T.; Melson, A.T.; Van Stavern, G.P.; McClelland, C.M.; Lindgren, B.R.; Sharieff, J.A.; Lee, M.S. Clinical Characteristics of Idiopathic Intracranial Hypertension in Patients Over 50 Years of Age: A multicenter clinical cohort study. Am. J. Ophthalmol. 2021, 224, 96–101. [Google Scholar] [CrossRef]
- Digre, K.B.; Corbett, J.J. Pseudotumor cerebri in men. Arch. Neurol 1988, 45, 866–872. [Google Scholar] [CrossRef]
- Kesler, A.; Goldhammer, Y.; Gadoth, N. Do men with pseudomotor cerebri share the same characteristics as women? A retrospective review of 141 cases. J. Neuroophthalmol. 2001, 21, 15–17. [Google Scholar] [CrossRef]
- Galvin, J.A.; Van Stavern, G.P. Clinical characterization of idiopathic intracranial hypertension at the Detroit Medical Center. J. Neurol. Sci. 2004, 223, 157–160. [Google Scholar] [CrossRef]
- Mezaal, M.; Saadah, M. Idiopathic intracranial hypertension in Dubai: Nature and prognosis. Acta Neurol. Scand. 2005, 112, 298–302. [Google Scholar] [CrossRef]
- Bruce, B.B.; Kedar, S.; Van Stavern, G.P.; Monaghan, D.; Acierno, M.D.; Braswell, R.A.; Preechawat, P.; Corbett, J.J.; Newman, N.J.; Biousse, V. Idiopathic intracranial hypertension in men. Neurology 2009, 72, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Rehman, O.; Ichhpujani, P.; Kumar, S.; Saroa, R.; Sawal, N. Idiopathic intracranial hypertension and visual function in North Indian population. Eur. J. Ophthalmol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Blanch, R.J.; Vasseneix, C.; Liczkowski, A.; Yiangou, A.; Aojula, A.; Micieli, J.A.; Mollan, S.P.; Newman, N.J.; Biousse, V.; Bruce, B.B.; et al. Differing presenting features of idiopathic intracranial hypertension in the UK and US. Eye 2019, 33, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, C.A.; Paley, G.L.; Xiao, R.; Kesler, A.; Eyal, O.; Ko, M.W.; Ko, M.W.; Boisvert, C.J.; Avery, R.A.; Salpietro, V.; et al. Pediatric Idiopathic Intracranial Hypertension: Age, Gender, and Anthropometric Features at Diagnosis in a Large, Retrospective, Multisite Cohort. Ophthalmology 2016, 123, 2424–2431. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Males (Number (%)) | Females (Number (%)) | All People (Number (%)) |
|---|---|---|---|
| Under 13 | 907 (19.01%) | 1023 (4.26%) | 1930 (6.68%) |
| 13–16 | 403 (8.45%) | 1278 (5.32%) | 1681 (5.82%) |
| 17–19 | 154 (3.23%) | 1604 (6.68%) | 1758 (6.09%) |
| 20–24 | 349 (7.31%) | 4444 (18.50%) | 4793 (16.59%) |
| 25–29 | 320 (6.71%) | 4649 (19.35%) | 4969 (17.20%) |
| 30–34 | 339 (7.10%) | 3238 (13.48%) | 3577 (12.38%) |
| 35–44 | 642 (13.45%) | 4010 (16.69%) | 4652 (16.10%) |
| 45–54 | 588 (12.32%) | 2146 (8.93%) | 2734 (9.46%) |
| 55–64 | 461 (9.66%) | 899 (3.74%) | 1360 (4.71%) |
| 65+ | 609 (12.76%) | 731 (3.04%) | 1340 (4.64%) |
| Total Number | 4772 | 24,022 | 28,794 |
| Deprivation Quintile | Males | Females | Total |
|---|---|---|---|
| 1—Most Deprived | 1304 (27.33%) | 7034 (29.28%) | 8338 (27.99%) |
| 2 | 1003 (21.02%) | 5698 (23.72%) | 6701 (22.49%) |
| 3 | 928 (19.45%) | 4376 (18.22%) | 5304 (17.80%) |
| 4 | 773 (16.20%) | 3669 (15.27%) | 4442 (14.91%) |
| 5—Least Deprived | 708 (14.84%) | 3001 (12.49%) | 3709 (12.45%) |
| Unknown | 56 (1.17%) | 244 (1.02%) | 300 (1.01%) |
| Number of Additional Admissions in the First Year of Diagnosis | Number of Patients (% of Total Number of Patients) |
|---|---|
| 0 | 18,046 (62.67%) |
| 1 | 5221 (18.13%) |
| 2 | 2352 (8.17%) |
| 3 | 1143 (3.97%) |
| 4 | 665 (2.31%) |
| 5 | 420 (1.46%) |
| 6 | 309 (1.07%) |
| 7 | 199 (0.69%) |
| 8 | 116 (0.40%) |
| 9 | 86 (0.30%) |
| 10+ | 237 (0.82%) |
| Diagnosis Year | Number of Subsequent Admissions Following Diagnosis | |||||
|---|---|---|---|---|---|---|
| 0 | 1 to 2 | More than 2 | ||||
| 2002/03 | 554 | 62.32% | 220 | 24.75% | 115 | 12.94% |
| 2003/04 | 581 | 64.06% | 222 | 24.48% | 104 | 11.47% |
| 2004/05 | 527 | 60.92% | 228 | 26.36% | 110 | 12.72% |
| 2005/06 | 620 | 61.75% | 261 | 26.00% | 123 | 12.25% |
| 2006/07 | 680 | 61.71% | 295 | 26.77% | 127 | 11.52% |
| 2007/08 | 703 | 61.67% | 301 | 26.40% | 136 | 11.93% |
| 2008/09 | 802 | 61.31% | 351 | 26.83% | 155 | 11.85% |
| 2009/10 | 837 | 59.57% | 385 | 27.40% | 183 | 13.02% |
| 2010/11 | 994 | 62.83% | 399 | 25.22% | 189 | 11.95% |
| 2011/12 | 1031 | 61.48% | 438 | 26.12% | 208 | 12.40% |
| 2012/13 | 1171 | 61.73% | 507 | 26.73% | 219 | 11.54% |
| 2013/14 | 1184 | 62.45% | 498 | 26.27% | 214 | 11.29% |
| 2014/15 | 1395 | 62.28% | 585 | 26.12% | 260 | 11.61% |
| 2015/16 | 1468 | 61.27% | 673 | 28.09% | 255 | 10.64% |
| 2016/17 | 1727 | 64.13% | 697 | 25.88% | 269 | 9.99% |
| 2017/18 | 1823 | 64.55% | 742 | 26.27% | 259 | 9.17% |
| 2018/19 | 1949 | 65.64% | 771 | 25.97% | 249 | 8.39% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mollan, S.P.; Mytton, J.; Tsermoulas, G.; Sinclair, A.J. Idiopathic Intracranial Hypertension: Evaluation of Admissions and Emergency Readmissions through the Hospital Episode Statistic Dataset between 2002–2020. Life 2021, 11, 417. https://doi.org/10.3390/life11050417
Mollan SP, Mytton J, Tsermoulas G, Sinclair AJ. Idiopathic Intracranial Hypertension: Evaluation of Admissions and Emergency Readmissions through the Hospital Episode Statistic Dataset between 2002–2020. Life. 2021; 11(5):417. https://doi.org/10.3390/life11050417
Chicago/Turabian StyleMollan, Susan P., Jemma Mytton, Georgios Tsermoulas, and Alex J. Sinclair. 2021. "Idiopathic Intracranial Hypertension: Evaluation of Admissions and Emergency Readmissions through the Hospital Episode Statistic Dataset between 2002–2020" Life 11, no. 5: 417. https://doi.org/10.3390/life11050417
APA StyleMollan, S. P., Mytton, J., Tsermoulas, G., & Sinclair, A. J. (2021). Idiopathic Intracranial Hypertension: Evaluation of Admissions and Emergency Readmissions through the Hospital Episode Statistic Dataset between 2002–2020. Life, 11(5), 417. https://doi.org/10.3390/life11050417