
Metabolic Actions of a Supplement of Ilex Paraguariensis (An Extract of the Leaf Standardized to 2% I-Deoxinojirimcina), White Mulberry and Chromium Picolinate in Nondiabetic Subjects with Dysglycemia: A Randomized Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Treatments
2.4. Assessments
2.5. Safety Measurements
2.6. Oral Glucose Tolerance Test and Glucose Clamp Technique
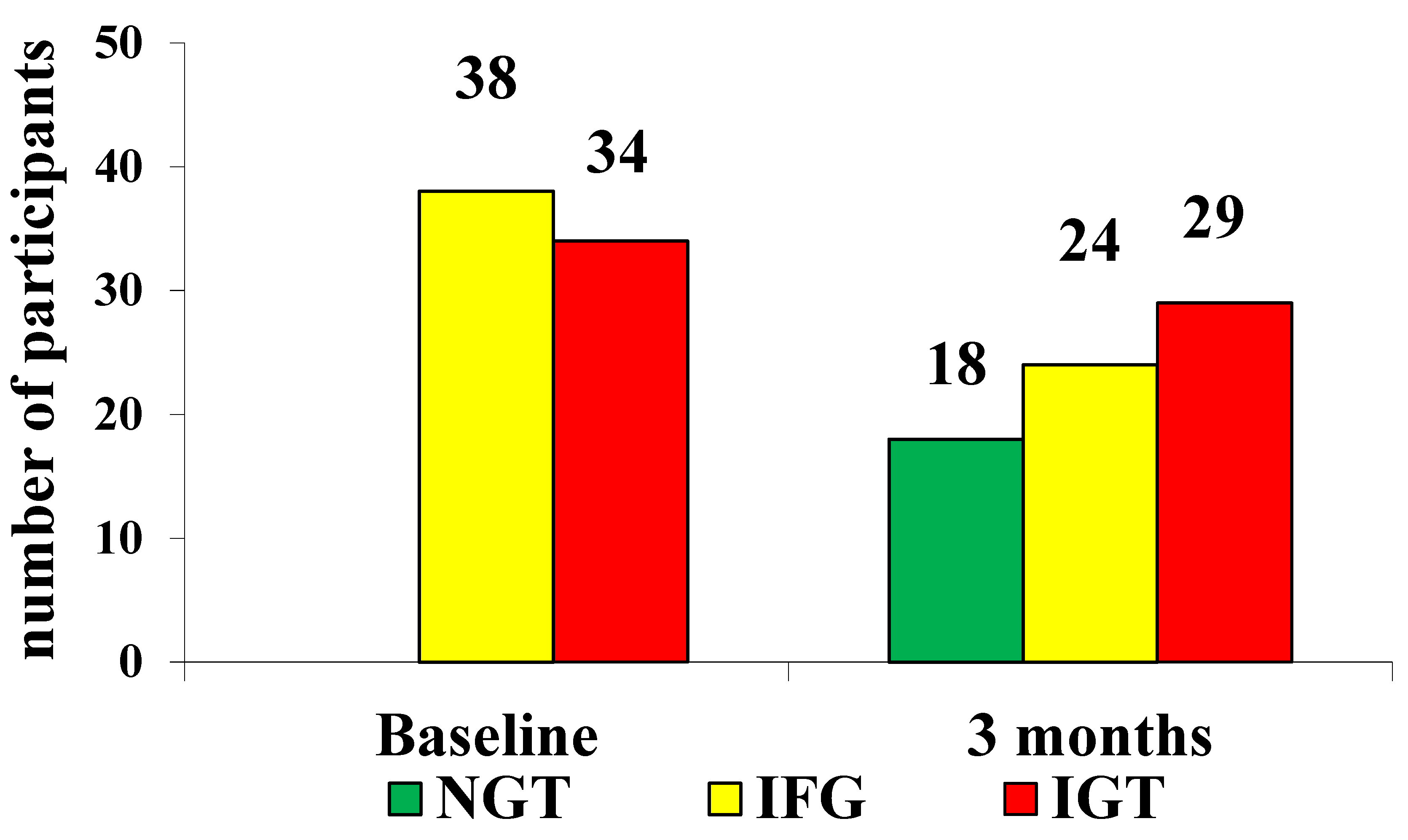
- IFG was defined by glycemia at 120 min from OGTT < 140 mg/dL;
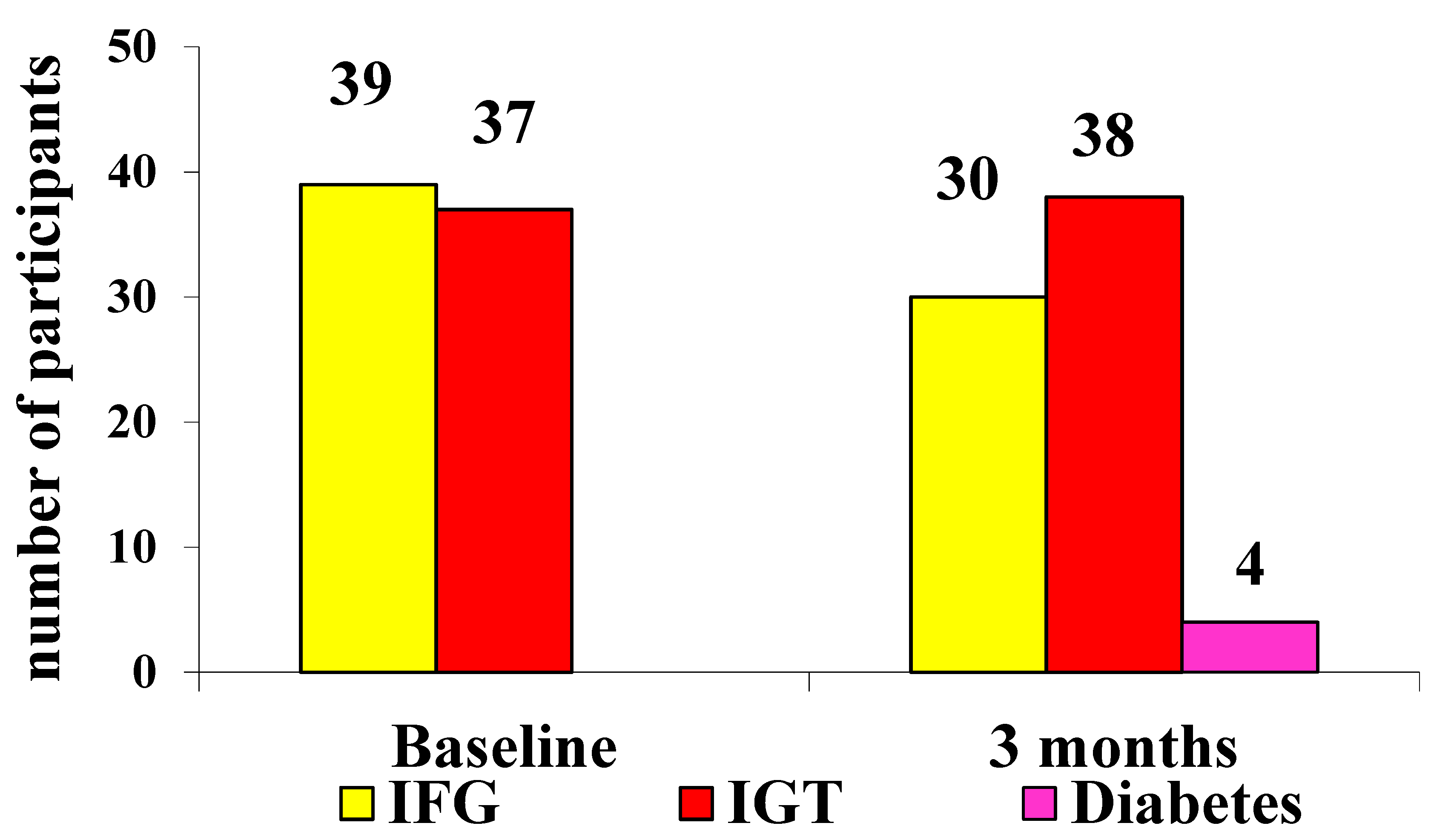
- IGT was defined by glycemia at 120 min from OGTT between 140 mg/dL and 199 mg/dL;
- Type 2 diabetes mellitus was defined by glycemia at 120 min from OGTT ≥ 200 mg/dL.
2.7. Statistical Analysis
3. Results
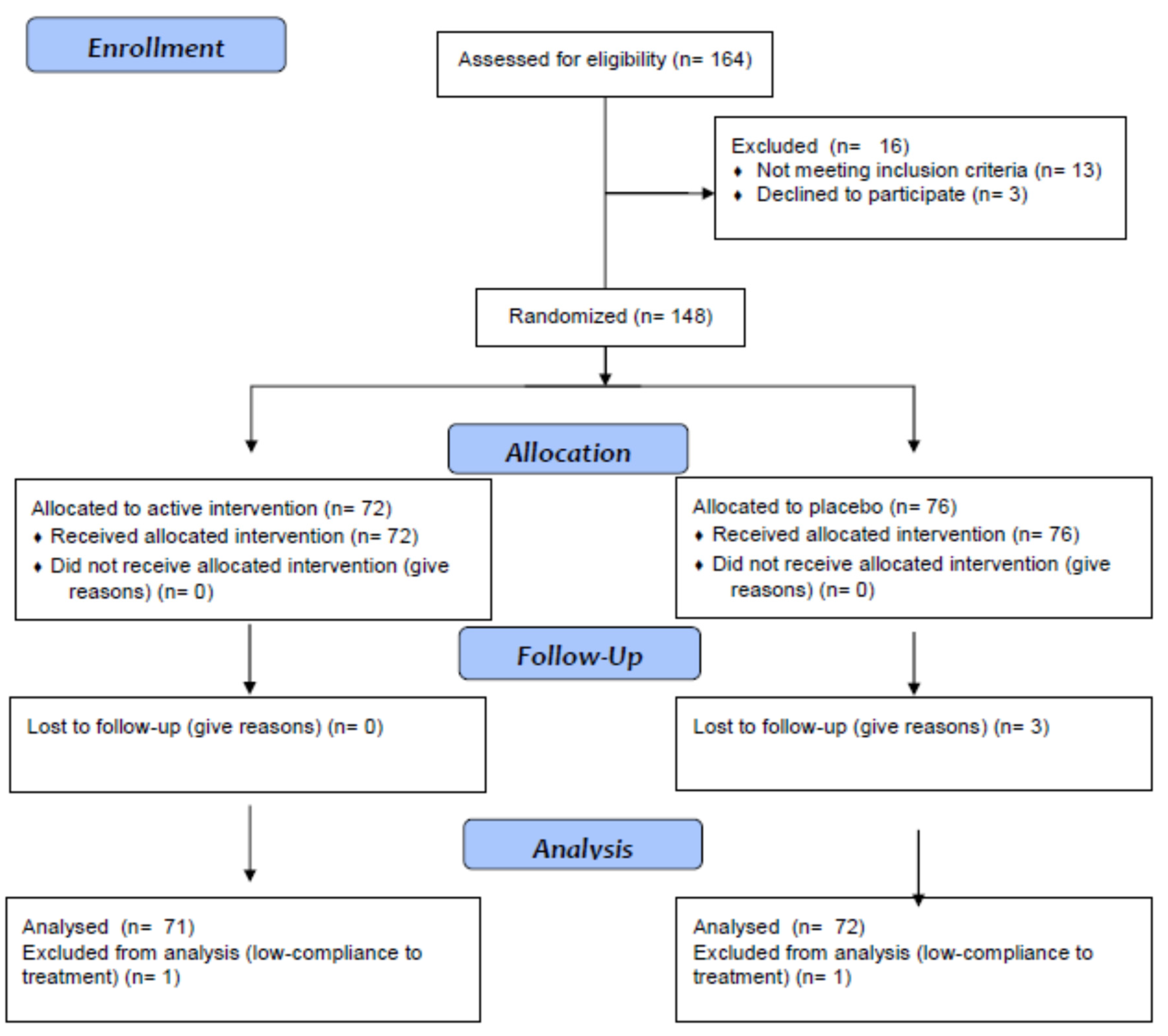
3.1. Study Sample
3.2. Anthropometric Parameters and Glycemic Metabolism
3.3. OGTT Results
3.4. M Value during the Clamp Technique
3.5. Lipid Profile
3.6. Cytokines
3.7. Safety and Treatment Acceptance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Bartnik, M.; Norhammar, A.; Rydén, L. Hyperglycaemia and cardiovascular disease. J. Intern. Med. 2007, 262, 145–156. [Google Scholar] [CrossRef]
- Derosa, G.; D’Angelo, A.; Salvadeo, S.A.T.; Ferrari, I.; Fogari, E.; Gravina, A.; Mereu, R.; Palumbo, I.; Maffioli, P.; Randazzo, S.; et al. Oral Glucose Tolerance Test Effects on Endothelial Inflammation Markers in Healthy Subjects and Diabetic Patients. Horm. Metab. Res. 2010, 42, 8–13. [Google Scholar] [CrossRef]
- Derosa, G.; D’Angelo, A.; Salvadeo, S.A.; Ferrari, I.; Fogari, E.; Gravina, A.; Mereu, R.; Palumbo, I.; Maffioli, P.; Randazzo, S.; et al. Modification of vascular and inflammation biomarkers after OGTT in overweight healthy and diabetic subjects. Microvasc. Res. 2010, 79, 144–149. [Google Scholar] [CrossRef]
- Durazzo, A.; Camilli, E.; D’Addezio, L.; Piccinelli, R.; Mantur-Vierendeel, A.; Marletta, L.; Finglas, P.; Turrini, A.; Sette, S. Development of Dietary Supplement Label Database in Italy: Focus of FoodEx2 Coding. Nutrients 2020, 12, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, G.A.; Stefanuto, A.; Boaventura, B.C.; de Morais, E.C.; da Cavalcante, L.S.; de Andrade, F.; Wazlawik, E.; Di Pietro, P.F.; Maraschin, M.; da Silva, E.L. Mate tea (Ilex paraguariensis) improves glycemic and lipid profiles of type 2 diabetes and pre-diabetes individuals: A pilot study. J. Am. Coll. Nutr. 2011, 30, 320–332. [Google Scholar] [CrossRef]
- de Morais, E.C.; Stefanuto, A.; Klein, G.A.; Boaventura, B.C.; de Andrade, F.; Wazlawik, E.; Di Pietro, P.F.; Maraschin, M.; da Silva, E.L. Consumption of yerba mate (Ilex paraguariensis) improves serum lipid parameters in healthy dyslipidemic subjects and provides an additional LDL-cholesterol reduction in individuals on statin therapy. J. Agric. Food. Chem. 2009, 57, 8316–8324. [Google Scholar] [CrossRef] [PubMed]
- Andersen, T.; Fogh, J. Weight loss and delayed gastric emptying following a South American herbal preparation in overweight patients. J. Hum. Nutr. Diet. 2001, 14, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Thaipitakwong, T.; Numhom, S.; Aramwit, P. Mulberry leaves and their potential effects against cardiometabolic risks: A review of chemical compositions, biological properties and clinical efficacy. Pharm. Biol. 2018, 56, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Yatsunami, K.; Fukuda, E.; Onodera, S.; Mizukami, O.; Hoshino, G.; Kamei, T. Antihyperglycemic effects of propolis mixed with mulberry leaf extract on patients with type 2 diabetes. Altern. Ther. Health Med. 2004, 10, 78–79. [Google Scholar]
- Anderson, R.A. Chromium, Glucose Intolerance and Diabetes. J. Am. Coll. Nutr. 1998, 17, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Broadhurst, C.L.; Domenico, P. Clinical Studies on Chromium Picolinate Supplementation in Diabetes Mellitus—A Review. Diabetes Technol. Ther. 2006, 8, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Derosa, G.; D’Angelo, A.; Maffioli, P. Ilex paraguariensis, white mulberry and chromium picolinate in patients with pre-diabetes. Phytother. Res. 2020, 34, 1377–1384. [Google Scholar] [CrossRef]
- The Council for International Organisation of Medical Sciences. Proposed International Guidelines for Biomedical Research Involving Human Subjects; The Council for International Organisation of Medical Sciences: Geneva, Switzerland, 1982. [Google Scholar]
- European Diabetes Policy Group. A desktop guide to type 2 diabetes mellitus. Diabet. Med. 1999, 16, 716–730. [Google Scholar] [CrossRef]
- Heding, L.G. Determination of total serum insulin (IRI) in insulin-treated diabetic patients. Diabetologia 1972, 8, 260–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, T.M.; Levy, J.; Matthews, D.R. Use and Abuse of HOMA Modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [Green Version]
- Klose, S.; Borner, K. Enzymatische Bestimmung des Gesamtcholesterins mit dem [Enzymatic dosage of total cholesterolemia by Greiner Selective Analyzer (GSA II)]. J. Clin. Chem. Clin. Biochem. 1978, 15, 121–130. [Google Scholar]
- Wahlefeld, A.W. Triglycerides determination after enzymatic hydrolysis. In Methods of Enzymatic Analysis, 2nd ed.; Bergmeyer, H.U., Ed.; Academic Press: New York, NY, USA, 1974; pp. 18–31. [Google Scholar]
- Havel, R.J.; Eder, H.A.; Bragdon, J.H. The distribution and chemical composition of ultracentrifugally separated lipoproteins in human serum. J. Clin. Investig. 1955, 34, 1345–1353. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Schumann, G.; Bonora, R.; Ceriotti, F.; Férard, G.; Ferrero, C.A.; Franck, P.F.; Gella, F.J.; Hoelzel, W.; Jørgensen, P.J.; Kanno, T.; et al. IFCC primary reference procedures for the measurement of catalytic activity concentrations of enzymes at 37 degrees C. International Federation of Clinical Chemistry and Laboratory Medicine. Part 4. Reference procedure for the measurement of catalytic concentration of alanine aminotransferase. Clin. Chem. Lab. Med. 2002, 40, 718–724. [Google Scholar]
- Schumann, G.; Bonora, R.; Ceriotti, F.; Férard, G.; Ferrero, C.A.; Franck, P.F.; Gella, F.J.; Hoelzel, W.; Jørgensen, P.J.; Kanno, T.; et al. IFCC primary reference procedures for the measurement of catalytic activity concentrations of enzymes at 37 degrees C. International Federation of Clinical Chemistry and Laboratory Medicine. Part 5. Reference procedure for the measurement of catalytic concentration of aspartate aminotransferase. Clin. Chem. Lab. Med. 2002, 40, 725–733. [Google Scholar] [PubMed]
- Rifai, N.; Tracy, R.P.; Ridker, P.M. Clinical Efficacy of an Automated High-Sensitivity C-Reactive Protein Assay. Clin. Chem. 1999, 45, 2136–2141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Standards of Medical Care in Diabetes. Diabetes Care 2019, 42 (Suppl. 1), S184–S186. [Google Scholar]
- DeFronzo, R.; Tobin, J.D.; Andres, R. Glucose clamp technique: A method for quantifying insulin secretion and resistance. Am. J. Physiol. Metab. 1979, 237, E214–E223. [Google Scholar] [CrossRef] [PubMed]
- Winer, B.J. Statistical Principles in Experimental Design, 2nd ed.; McGraw-Hill: New York, NY, USA, 1971. [Google Scholar]
- Arçari, D.P.; Santos, J.; Gambero, A.; Ferraz, L.F.C.; Ribeiro, M.L. Modulatory effects of yerba maté (Ilex paraguariensis ) on the PI3K-AKT signaling pathway. Mol. Nutr. Food Res. 2013, 57, 1882–1885. [Google Scholar] [CrossRef] [PubMed]
- Kimura, T.; Nakagawa, K.; Kubota, H.; Kojima, Y.; Goto, Y.; Yamagishi, K.; Oita, S.; Oikawa, A.S.; Miyazawa, T. Food-Grade Mulberry Powder Enriched with 1-Deoxynojirimycin Suppresses the Elevation of Postprandial Blood Glucose in Humans. J. Agric. Food Chem. 2007, 55, 5869–5874. [Google Scholar] [CrossRef]
- Derosa, G.; Cicero, A.F.G.; D’Angelo, A.; Maffioli, P. Ascophyllum nodosum and Fucus vesiculosus on glycemic status and on endothelial damage markers in dysglicemic patients. Phytother. Res. 2019, 33, 791–797. [Google Scholar] [CrossRef]
- Matsumoto, R.L.T.; Bastos, D.H.M.; Mendonça, S.; Nunes, V.S.; Bartchewsky, W.; Ribeiro, M.; Carvalho, P.D.O. Effects of Maté Tea (Ilex paraguariensis) Ingestion on mRNA Expression of Antioxidant Enzymes, Lipid Peroxidation, and Total Antioxidant Status in Healthy Young Women. J. Agric. Food Chem. 2009, 57, 1775–1780. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Ingredients of Glicoset® 1000 | Daily intake (1 Tablet) |
| Chromium picolinate | 100 mcg (250% RDD) |
| Ilex paraguariensis | 1000 mg |
| Morus alba (2% I-deoxinojirimcina) | 50 mg of which 1 mg DNJ |
| Silicon dioxide | 13 mg |
| Magnesium stearate | 13 mg |
| Dicalcium phosphate | 139 mg |
| Microcrystalline cellulose | 84.2 mg |
| Ingredients of Placebo | Daily intake (1 Tablet) |
| Silicon dioxide | 13 mg |
| Magnesium stearate | 13 mg |
| Dicalcium phosphate | 600 mg |
| Microcrystalline cellulose | 609 mg |
| E172 (iron oxides, a food coloring) | 65 mg |
| Parameters | Glicoset® 1000 | Placebo | ||
|---|---|---|---|---|
| Baseline | 3 Months | Baseline | 3 Months | |
| Patients | 72 | 71 | 76 | 72 |
| M/F | 35/37 | 35/36 | 38/38 | 35/37 |
| Smoking status (M/F) | 14/16 | 14/16 | 13/12 | 12/11 |
| IFG (M/F (%)) | 20/18 (52.8) | 13/11 (33.8) | 21/18 (51.3) | 16/14 (41.7) |
| IGT (M/F (%)) | 15/19 (47.2) | 13/16 (40.8) | 17/20 (48.7) | 19/19 (52.8) |
| EU from IFG (M/F (%)) | - | 7/6 (18.3) | - | 0/0 |
| EU from IGT (M/F (%)) | - | 2/3 (7.0) | - | 0/0 |
| IGT from IFG (M/F (%)) | - | 0/0 | - | 3/3 (8.3) |
| D from IFG (M/F (%)) | - | 0/0 | - | 0/0 |
| D from IGT (M/F (%)) | - | 0/0 | - | 1/3 (5.6) |
| Lost to FU from IFG (M/F (%)) | - | 0/1 (1.4) | - | 2/1 (4.2) |
| Lost to FU from IGT (M/F (%)) | - | 0/0 | - | 0/1 (1.4) |
| Parameters | Glicoset® 1000 | Placebo | ||
|---|---|---|---|---|
| Baseline | 3 Months | Baseline | 3 Months | |
| Patients | 72 | 71 | 76 | 72 |
| M/F | 35/37 | 35/36 | 38/38 | 35/37 |
| Age (years) | 53.8 ± 6.4 | - | 52.7 ± 6.1 | - |
| Smoking status (M/F) | 15/16 | 15/15 | 13/16 | 12/14 |
| Height (cm) | 1.68 ± 0.04 | 1.68 ± 0.04 | 1.69 ± 0.05 | 1.69 ± 0.05 |
| Weight (Kg) | 79.2 ± 9.8 | 79.0 ± 9.6 | 78.4 ± 9.4 | 78.6 ± 9.5 |
| BMI (Kg/m2) | 28.1 ± 2.4 | 28.1 ± 2.4 | 27.4 ± 2.1 | 27.5 ± 2.2 |
| WC (cm) | 90.3 ± 3.3 | 90.3 ± 3.3 | 89.7 ± 3.1 | 89.8 ± 3.2 |
| HC (cm) | 87.5 ± 2.8 | 87.4 ± 2.7 | 87.1 ± 2.6 | 87.3 ± 2.8 |
| AC (cm) | 99.2 ± 3.4 | 99.2 ± 3.3 | 98.3 ± 3.1 | 98.4 ± 3.2 |
| FPG (mg/dL) | 114.2 ± 8.6 | 102.2 ± 5.9 *^ | 113.1 ± 8.3 | 115.7 ± 12.8 |
| PPG (mg/dL) | 132.9 ± 9.8 | 120.4 ± 5.0 *^ | 129.8 ± 5.2 | 132.1 ± 5.6 |
| HbA1c (%) | 5.9 ± 0.3 | 5.5 ± 0.1 *^ | 5.7 ± 0.2 | 5.8 ± 0.3 |
| FPI (μU/mL) | 9.1 ± 5.3 | 9.0 ± 5.2 | 8.9 ± 5.1 | 9.0 ± 5.2 |
| HOMA index | 2.53 ± 0.9 | 2.38 ± 0.6 *^ | 2.48 ± 0.9 | 2.58 ± 0.9 |
| TC (mg/dL) | 218.2 ± 17.4 | 197.4 ± 15.3 *^ | 214.7 ± 16.3 | 217.1 ± 16.8 |
| LDL-C (mg/dL) | 148.8 ± 20.2 | 130.7 ± 17.5 *^ | 146.7 ± 19.7 | 147.5 ± 19.9 |
| HDL-C (mg/dL) | 43.2 ± 4.5 | 43.0 ± 4.2 | 42.5 ± 4.2 | 42.7 ± 4.4 |
| Tg (mg/dL) | 131.1 ± 39.1 | 118.5 ± 31.8 *^ | 127.3 ± 38.4 | 134.6 ± 38.7 |
| AST (UI/L) | 18.1 ± 8.6 | 17.5 ± 8.3 | 19.2 ± 9.2 | 18.7 ± 8.9 |
| ALT (UI/L) | 22.0 ± 12.1 | 21.6 ± 11.7 | 22.8 ± 12.6 | 24.1 ± 12.9 |
| Hs-CRP (mg/L) | 1.1 ± 0.6 | 1.0 ± 0.5 | 1.0 ± 0.5 | 1.2 ± 0.7 |
| Glicoset® 1000 | Placebo | ||||
|---|---|---|---|---|---|
| Time (Minutes) | Glycemia (mg/dL) | Subjects n (M/F) | Glycemia (mg/dL) | Subjects n (M/F) | |
| IFG | 0 | 106.7 ± 5.8 | 38 (20/18) | 106.5 ± 5.4 | 39 (21/18) |
| 120 | 122.4 ± 10.5 | 123.4 ± 11.2 | |||
| IGT | 0 | 108.6 ± 6.9 | 34 (15/19) | 109.7 ± 7.5 | 37 (17/20) |
| 120 | 162.1 ± 15.7 | 158.9 ± 14.3 | |||
| Glicoset® 1000 | Placebo | ||||
|---|---|---|---|---|---|
| Time (minutes) | Glycemia (mg/dL) | Subjects n (M/F) | Glycemia (mg/dL) | Subjects n (M/F) | |
| IFG | 0 | 103.6 ± 3.0 | 24 (13/11) | 105.4 ± 4.8 | 30 (16/14) |
| 120 | 114.2 ± 6.5 | 118.5 ± 11.6 | |||
| IGT | 0 | 105.3 ± 5.1 | 29 (13/16) | 108.2 ± 6.9 | 38 (19/19) |
| 120 | 149.4 ± 8.3 | 153.7 ± 11.3 | |||
| N Baseline | N End of Treatment | Baseline | End of Treatment | Delta End of Treatment vs. Baseline | |
|---|---|---|---|---|---|
| Glicoset® 1000 | 72 | 71 | 6.19 ± 0.88 | 8.28 ± 1.27 *° | 2.09 ± 0.92 |
| Placebo | 76 | 71 | 6.04 ± 0.52 | 5.98 ± 0.83 | 0.06 ± 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derosa, G.; D’Angelo, A.; Maffioli, P. Metabolic Actions of a Supplement of Ilex Paraguariensis (An Extract of the Leaf Standardized to 2% I-Deoxinojirimcina), White Mulberry and Chromium Picolinate in Nondiabetic Subjects with Dysglycemia: A Randomized Trial. Life 2021, 11, 709. https://doi.org/10.3390/life11070709
Derosa G, D’Angelo A, Maffioli P. Metabolic Actions of a Supplement of Ilex Paraguariensis (An Extract of the Leaf Standardized to 2% I-Deoxinojirimcina), White Mulberry and Chromium Picolinate in Nondiabetic Subjects with Dysglycemia: A Randomized Trial. Life. 2021; 11(7):709. https://doi.org/10.3390/life11070709
Chicago/Turabian StyleDerosa, Giuseppe, Angela D’Angelo, and Pamela Maffioli. 2021. "Metabolic Actions of a Supplement of Ilex Paraguariensis (An Extract of the Leaf Standardized to 2% I-Deoxinojirimcina), White Mulberry and Chromium Picolinate in Nondiabetic Subjects with Dysglycemia: A Randomized Trial" Life 11, no. 7: 709. https://doi.org/10.3390/life11070709
APA StyleDerosa, G., D’Angelo, A., & Maffioli, P. (2021). Metabolic Actions of a Supplement of Ilex Paraguariensis (An Extract of the Leaf Standardized to 2% I-Deoxinojirimcina), White Mulberry and Chromium Picolinate in Nondiabetic Subjects with Dysglycemia: A Randomized Trial. Life, 11(7), 709. https://doi.org/10.3390/life11070709