


Correlation between Cytogenetic Findings and Spermatogenic Failure in Bulgarian Infertile Men

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yahaya, T.O.; Oladele, E.O. Chromosomal abnormalities predisposing to infertility, testing, and management: A narrative review. Bull. Natl. Res. Cent. 2021, 45, 65. [Google Scholar] [CrossRef]
- Mvuyekure, B.; Mutoni, C. Prevalence of primary infertility caused by chromosomal abnormalities and assessment of clinical manifestations in Rwandan patients. Rwanda Med. J. 2020, 77, 23–27. [Google Scholar]
- El-Dahtory, F.; Yahia, S. Prevalence and patterns of chromosomal abnormalities among Egyptian patients with infertility: A single institution’s 5-year experience. Middle East Fertil. Soc. J. 2022, 27, 10. [Google Scholar] [CrossRef]
- Ohlander, S.J.; Lindgren, M.C.; Lipshultz, L.I. Testosterone and Male Infertility. Urol. Clin. North Am. 2016, 43, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Du, R.C. Impact of chromosomal translocations on male infertility, semen quality, testicular volume and reproductive hormone levels. J. Int. Med. Res. 2012, 40, 2274–2283. [Google Scholar] [CrossRef]
- Yahaya, T.O.; Liman, U.U. Genes predisposing to syndromic and nonsyndromic infertility: A narrative review. Egypt J. Med. Hum. Genet. 2020, 21, 46. [Google Scholar] [CrossRef]
- Harton, G.L.; Tempest, H.G. Chromosomal disorders and male infertility. Asian J. Androl. 2012, 14, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Vicdan, A.; Vicdan, K. Genetic aspects of human male infertility: The frequency of chromosomal abnormalities and Y chromosome microdeletions in severe male factor infertility. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 117, 49–54. [Google Scholar] [CrossRef]
- Mahdi, B.M. Semen Analysis and Insight into Male Infertility. Open Access Maced. J. Med. Sci. 2021, 9, 252–260. [Google Scholar] [CrossRef]
- Kandil, H.; Agarwal, A. Editorial Commentary on Draft of World Health Organization Sixth Edition Laboratory Manual for the Examination and Processing of Human Semen. World J. Mens. Health 2021, 39, 577–580. [Google Scholar] [CrossRef]
- Cocuzza, M.; Alvarenga, C. The epidemiology and etiology of azoospermia. Clinics 2013, 68 (Suppl. 1), 15–26. [Google Scholar] [CrossRef]
- Kuroda, S.; Usui, K. Genetic disorders and male infertility. Reprod. Med. Biol. 2020, 19, 314–322. [Google Scholar] [CrossRef]
- Lissitsina, J.; Mikelsaar, R. Cytogenetic analyses in infertile men. Arch. Androl. 2006, 52, 91–95. [Google Scholar] [CrossRef]
- Malla, T.M.; Zargar, M.H. Cytogenetic Observations in Infertile Men with Varying Clinical Findings: A Case-Only Study from Kashmir, North India. Ann. Genet. Genet. Disord. 2018, 1, 1002. [Google Scholar]
- De Braekeleer, M.; Dao, T.N. Cytogenetic studies in male infertility: A review. Hum. Reprod. 1991, 6, 245–250. [Google Scholar] [CrossRef]
- Kate, U.V.; Pokale, Y.S. Chromosomal aberrations and polymorphic evaluation in males with primary infertility from Indian population. J. Clin. Diagn. Res. 2014, 8, SC01–SC06. [Google Scholar] [CrossRef]
- Li, D.; Zhang, H. Chromosomal abnormalities in men with pregestational and gestational infertility in northeast China. J. Assist. Reprod. Genet. 2012, 29, 829–836. [Google Scholar] [CrossRef] [Green Version]
- Penna Videaú, S.; Araujo, H. Chromosomal abnormalities and polymorphisms in infertile men. Arch. Androl. 2001, 46, 205–210. [Google Scholar] [CrossRef]
- Arafa, M.M.; Majzoub, A. Chromosomal abnormalities in infertile men with azoospermia and severe oligozoospermia in Qatar and their association with sperm retrieval intracytoplasmic sperm injection outcomes. Arab. J. Urol. 2018, 16, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Wang, R. Non-Robertsonian translocations involving chromosomes 13, 14, or 15 in male infertility: 28 cases and a review of the literature. Medicine 2019, 98, e14730. [Google Scholar] [CrossRef]
- Ferguson, K.A.; Chow, V. Silencing of unpaired meiotic chromosomes and altered recombination patterns in an azoospermic carrier of a t(8;13) reciprocal translocation. Hum. Reprod. 2008, 23, 988–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amorini, A.M.; Listorti, I. Antioxidant-Based Therapies in Male Infertility: Do We Have Sufficient Evidence Supporting Their Effectiveness? Antioxidants 2021, 10, 220. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Li, F. Analysis of the clinical features of pericentric inversion of chromosome 9. J. Int. Med. Res. 2020, 48. [Google Scholar] [CrossRef] [PubMed]
- Muthuvel, A.; Ravindran, M. Pericentric inversion of chromosome 9 causing infertility and subsequent successful in vitro fertilization. Niger. Med. J. 2016, 57, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Mozdarani, H.; Meybodi, A.M. Impact of pericentric inversion of Chromosome 9 [inv (9) (p11q12)] on infertility. Indian J. Hum. Genet. 2007, 13, 26–29. [Google Scholar] [CrossRef] [Green Version]
- Slimani, W.; Jelloul, A. Small supernumerary marker chromosomes (sSMC) and male infertility: Characterization of five new cases, review of the literature, and perspectives. J. Assist. Reprod. Genet. 2020, 37, 1729–1736. [Google Scholar] [CrossRef]
- Song, S.H.; Park, S.H. Male Infertility Associated with a Supernumerary Marker Chromosome. World J. Mens Health 2017, 35, 205–208. [Google Scholar] [CrossRef]
- Manvelyan, M.; Riegel, M. Thirty-two new cases with small supernumerary marker chromosomes detected in connection with fertility problems: Detailed molecular cytogenetic characterization and review of the literature. Int. J. Mol. Med. 2008, 21, 705–714. [Google Scholar] [CrossRef] [Green Version]
- Angelova, L.; Tsvetkova, M. Chromosomal polymorphism in Bulgarian patients with reproductive problems—One genetic center experience. J. IMAB 2021, 27, 4133–4138. [Google Scholar] [CrossRef]
- Saran, N.; Kumar, B. Chromosomal Heteromorphisms and Karyotype Abnormalities in Humans. Int. J. Curr. Microbiol. App. Sci. 2017, 6, 2940–2953. [Google Scholar] [CrossRef] [Green Version]
- Madon, P.F.; Athalye, A.S. Polymorphic variants on chromosomes probably play a significant role in infertility. Reprod. Biomed. Online 2005, 11, 726–732. [Google Scholar] [CrossRef]
- Minocherhomji, S.; Athalye, A.S. A case-control study identifying chromosomal polymorphic variations as forms of epigenetic alterations associated with the infertility phenotype. Fertil. Steril. 2009, 92, 88–95. [Google Scholar] [CrossRef]
- Suganya, J.; Kujur, S.B. Chromosomal Abnormalities in Infertile Men from Southern India. J. Clin. Diagn. Res. 2015, 9, 5–10. [Google Scholar] [CrossRef]
- Nagvenkar, P.; Desai, K. Chromosomal studies in infertile men with oligozoospermia & non-obstructive azoospermia. Indian J. Med. Res. 2005, 122, 34–42. [Google Scholar]
- Guo, T.; Qin, Y. The role of male chromosomal polymorphism played in spermatogenesis and the outcome of IVF/ICSI-ET treatment. Int. J. Androl. 2012, 35, 802–809. [Google Scholar] [CrossRef]
- Sahin, F.I.; Yilmaz, Z. Chromosome heteromorphisms: An impact on infertility. J. Assist. Reprod Genet. 2008, 25, 191–195. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Majzoub, A. Sperm DNA Fragmentation: A New Guideline for Clinicians. World J. Mens. Health 2020, 38, 412–471. [Google Scholar] [CrossRef]
- Wright, C.; Milne, S. Sperm DNA damage caused by oxidative stress: Modifiable clinical, lifestyle and nutritional factors in male infertility. Reprod. Biomed. Online 2014, 28, 684–703. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Group n/% | Average Age | Sperm Concentration/mL | Sperm Motility |
|---|---|---|---|
| Normozoospermia 86/9.5% | 34.9 (±5.1) | ≥20 mln/mL | >50% |
| Asthenozoospermia 394/43.8% | 36.8 (±5.9) | ≥20 mln/mL | <50% |
| Oligoasthenozoospermia 182/20.2% | 35.3 (±6.0) | <20 mln/1mL | <50% |
| Severe male factor (severe oligoasthenozoospermia) 100/11.1% | 35.0 (±6.5) | <1 mln/mL | <50% |
| Azoospermia 139/15.4% | 33.3 (±5.9) | Absence of spermatozoa in the ejaculate | |
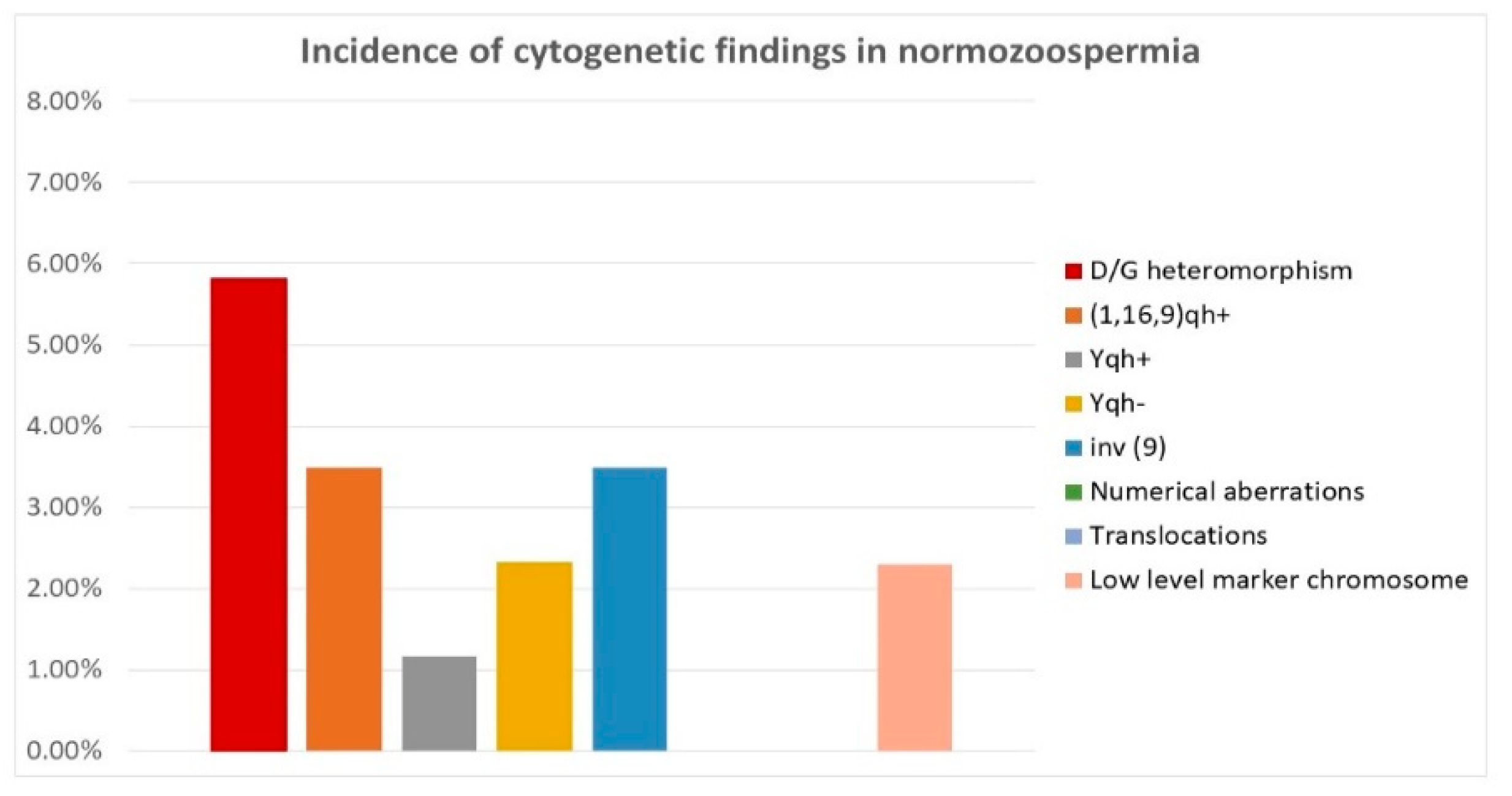
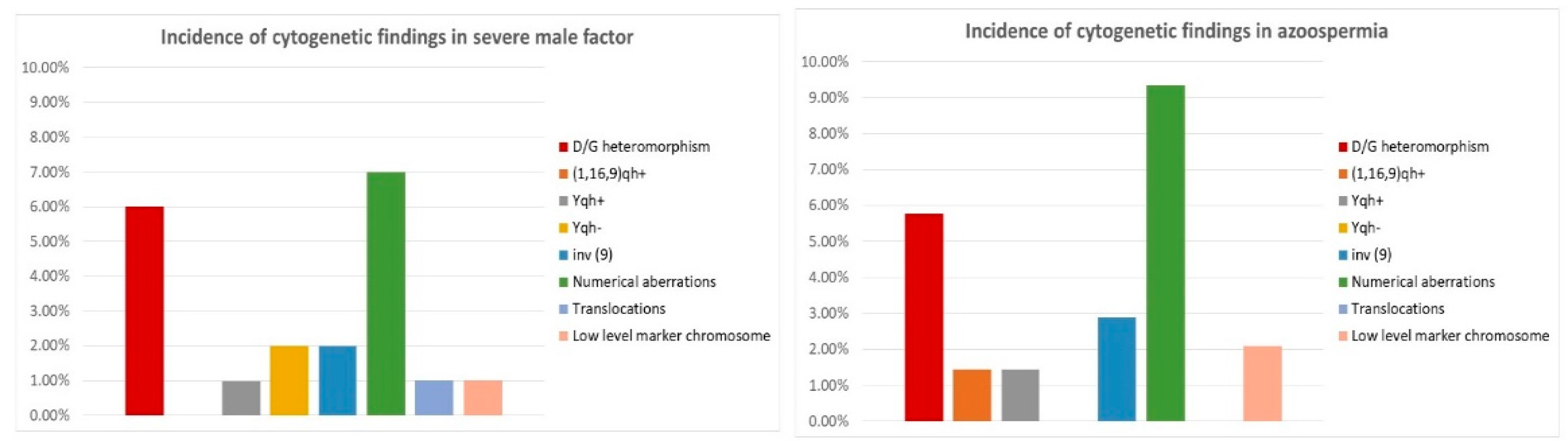
| Chromosomal Finding | Normo-Zoospermia | Astheno-Zoospermia | Oligo-Asthenozoospermia | SMF | Azoospermia |
|---|---|---|---|---|---|
| 46, XY | 80.23% | 81.47% | 81.87% | 80.00% | 75.5% |
| D/G heteromorphism | 5.81% | 7.6% | 5.5% | 6.00% | 5.76% |
| (1,16,9) qh+ | 3.49% | 2.54% | 5.49% | 0.00% | 1.44% |
| Yqh+ | 1.16% | 0.5% | 1.6% | 0.98% | 1.44% |
| Yqh- | 2.32% | 0.8% | 1.1% | 2.00% | 0.0% |
| inv (9) | 3.49% | 1.52% | 3.3% | 2.00% | 2.88% |
| Numerical aberrations | 0.00% | 1.8% | 1.6% | 7.00% p < 0.01 | 9.35% p < 0.01 |
| Translocations | 0.00% | 1.3% | 2.7% | 1.00% | 0.0% |
| Low-level marker chromosome | 2.3% | 2.5% | 5.5% | 1.00% | 2.1% |
| 46, XX | 0% | 0% | 0% | 0% | 2.1% |
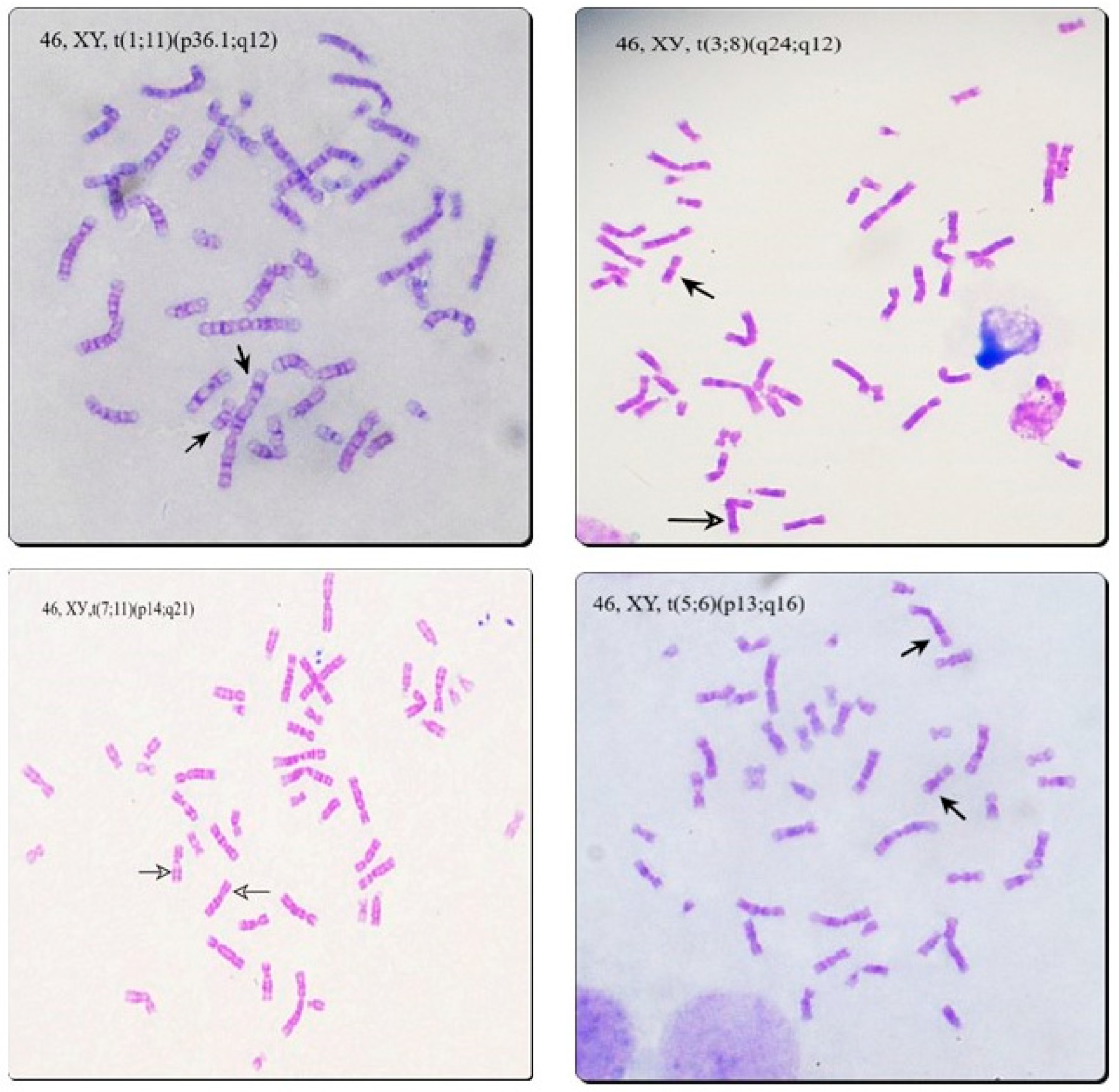
| Asthenozoospermia | Oligoasthenozoospermia | Severe Male Factor |
|---|---|---|
| 46, XY, t (1;11) (p36.1; q12) | 46, XY, t (1p31- > 11q22- > 8q12- > 1p31) | 45, XY, t (13;22) (q10; q10) |
| 45, XY, t (13;14) (q10; q10) | 46, XY, t (5, 6) (p13; q16) | |
| 46, XY, t (3;8) (q24; q12) | 45, XY, t (13;14) (q10; q10) | |
| 45, XY, t (13;14) (q10; q10) | 46, XY, t (7;11) (p14; q21) | |
| 45, XY, t (5;15) (q35; q10) | 46, XY, t (5;15) (q14; q14) |
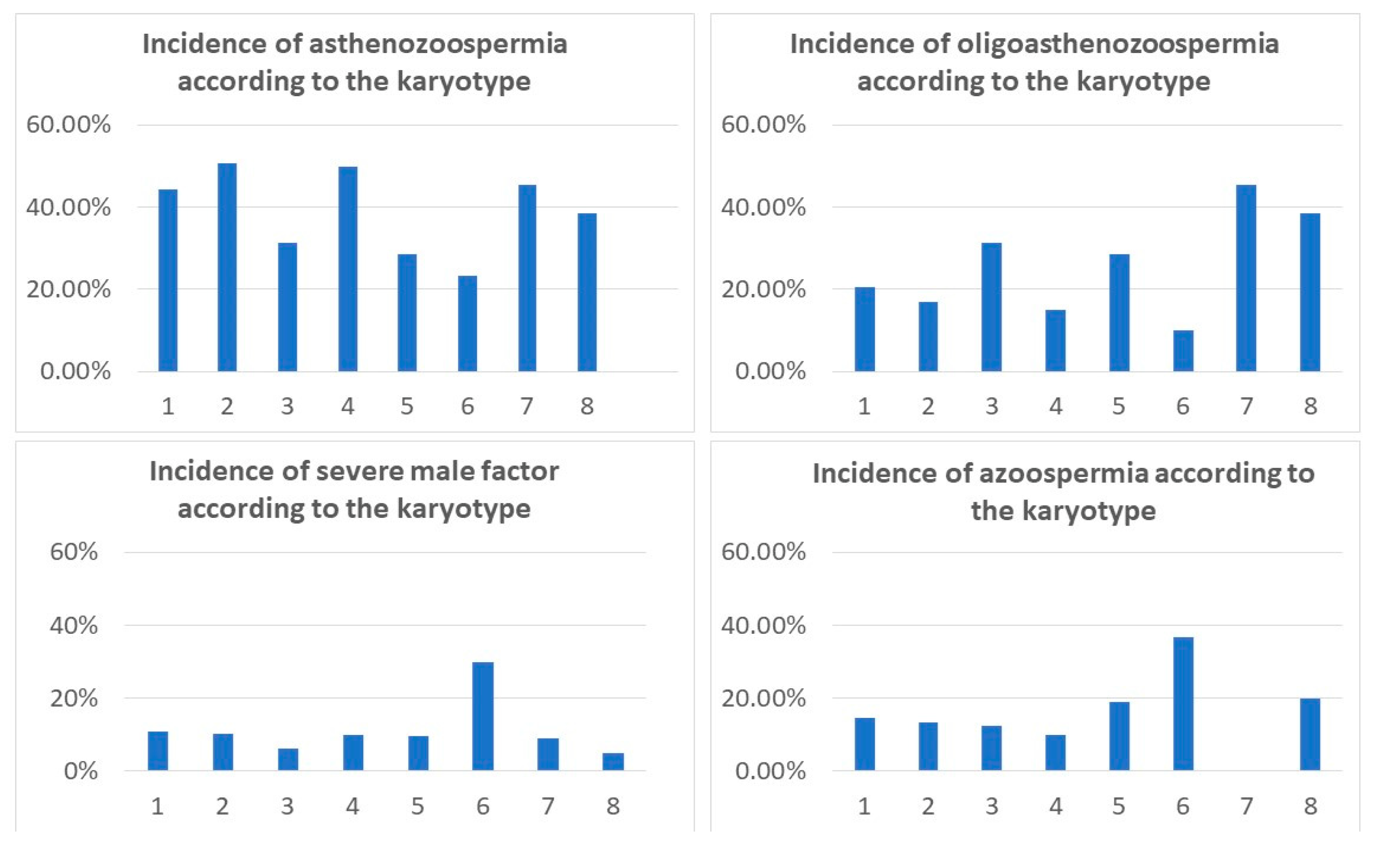
| Cytogenetic Group | Asthenozoospermia | Oligoasthenozoospermia | Severe Male Factor | Azoospermia |
|---|---|---|---|---|
| 46, XY (n = 724) | 321/724 (44.3%) | 149/724 (20.6%) | 80/724 (11%) | 105/724 (14.5%) |
| D/G heteromorphism (n = 59) | 30/59 (50.8%) | 10/59 (17%) | 6/59 (10.2%) | 8/59 (13.5%) |
| Yqh polymorphism (n =1 6) | 5/16 (31.25%) | 5/16 (31.25%) | 1/16 (6.2%) | 2/16 (12.5%) |
| (1,9,16) qh+ (n = 20) | 10/20 (50%) | 3/20 (15%) | 2/20 (10%) | 2/20 (10%) |
| inv(9) (n = 21) | 6/21 (28.6%) | 6/21 (28.6%) | 2/21 (9.5%) | 4/21 (19%) |
| Numerical aberrations (n = 30) | 7/30 (23.3%) | 3/30 (10%) | 9/30 (30%) | 11/30 (36.7%) |
| Klinefeleter syndrome (n = 9) | 0/9 (0.0%) | 0/9 (0.0%) | 0/9 (0.0%) | 9/9 (100%) |
| Poly Y and Mosaic forms (n = 22) | 7/21 (33.3%) | 3/21 (14.3%) | 7/21 (33.3%) | 4/21 (19%) |
| Translocations (n = 11) | 5/11 (45.4%) | 5/11 (45.4%) | 1/11 (9.1%) | 0/11 |
| Low level marker chromosome (n = 26) | 10/26 (38.5%) | 10/26 (38.5%) | 1/26 (3.8%) | 3/26 (11.5%) |
| The Group from Sperm Analysis | Frequency of Chromosomal Polymorphism | Frequency of Chromosomal Aberrations |
|---|---|---|
| Normozoospermia | 16.27% | 3.5% |
| Asthenozoospermia | 15.9% | 5.6% |
| Oligoasthenozoospermia | 13.2% | 9.8% |
| Severe male factor (severe oligoasthenozoospermia) | 11% | 9% |
| Azoospermia | 11.6% | 13.5% |
| Cytogenetic Findings | Testosterone (9.9–27.8 nmol/L) | FSH (1.5–12.4 IU/L) | LH (1.7–8.6 IU/L) | Sterility (%)/Miscarriages (%) |
|---|---|---|---|---|
| Klinefelter syndrome | 5.9 (±3.8) | 33.5 (±16.3) | 20.9 (±10.1) | 100%/0 |
| Mosaic Klinefelter syndrome | 13.6 (±7.1) | 12.0 (±7.9) | 8.8 (±4.7) | 87.5%/12.5% |
| 47,XYY syndrome | 10.0 (±6.3) | 15.3 (±12.4) | 6.9 (±4.2) | 85.7%/14.3% |
| Mosaic marker chromosome | 16.8 (±9.4) | 4.1 (±2.1) | 3.1 (±1.7) | 89%/11% |
| Chromosomal translocations | 14.7 (±8.0) | 6.1 (±4.2) | 5.5 (±3.1) | 63.7%/36.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yovinska, S.; Belemezova, K.; Hristova-Savova, M.; Milachich, T.; Andreeva, P.; Veleva, L.; Buchvarov, Y.; Yunakova, M.; Timeva, T.; Shterev, A.; et al. Correlation between Cytogenetic Findings and Spermatogenic Failure in Bulgarian Infertile Men. Life 2022, 12, 1840. https://doi.org/10.3390/life12111840
Yovinska S, Belemezova K, Hristova-Savova M, Milachich T, Andreeva P, Veleva L, Buchvarov Y, Yunakova M, Timeva T, Shterev A, et al. Correlation between Cytogenetic Findings and Spermatogenic Failure in Bulgarian Infertile Men. Life. 2022; 12(11):1840. https://doi.org/10.3390/life12111840
Chicago/Turabian StyleYovinska, Svetlana, Kalina Belemezova, Mariela Hristova-Savova, Tanya Milachich, Petya Andreeva, Lachezara Veleva, Yuri Buchvarov, Maria Yunakova, Tanya Timeva, Atanas Shterev, and et al. 2022. "Correlation between Cytogenetic Findings and Spermatogenic Failure in Bulgarian Infertile Men" Life 12, no. 11: 1840. https://doi.org/10.3390/life12111840
APA StyleYovinska, S., Belemezova, K., Hristova-Savova, M., Milachich, T., Andreeva, P., Veleva, L., Buchvarov, Y., Yunakova, M., Timeva, T., Shterev, A., & Dimova, I. (2022). Correlation between Cytogenetic Findings and Spermatogenic Failure in Bulgarian Infertile Men. Life, 12(11), 1840. https://doi.org/10.3390/life12111840