
The Impact of 52-Week Single Inhaler Device Triple Therapy versus Dual Therapy on the Mortality of COPD Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , ,
, ,
Abstract
:1. Introduction
2. Methods
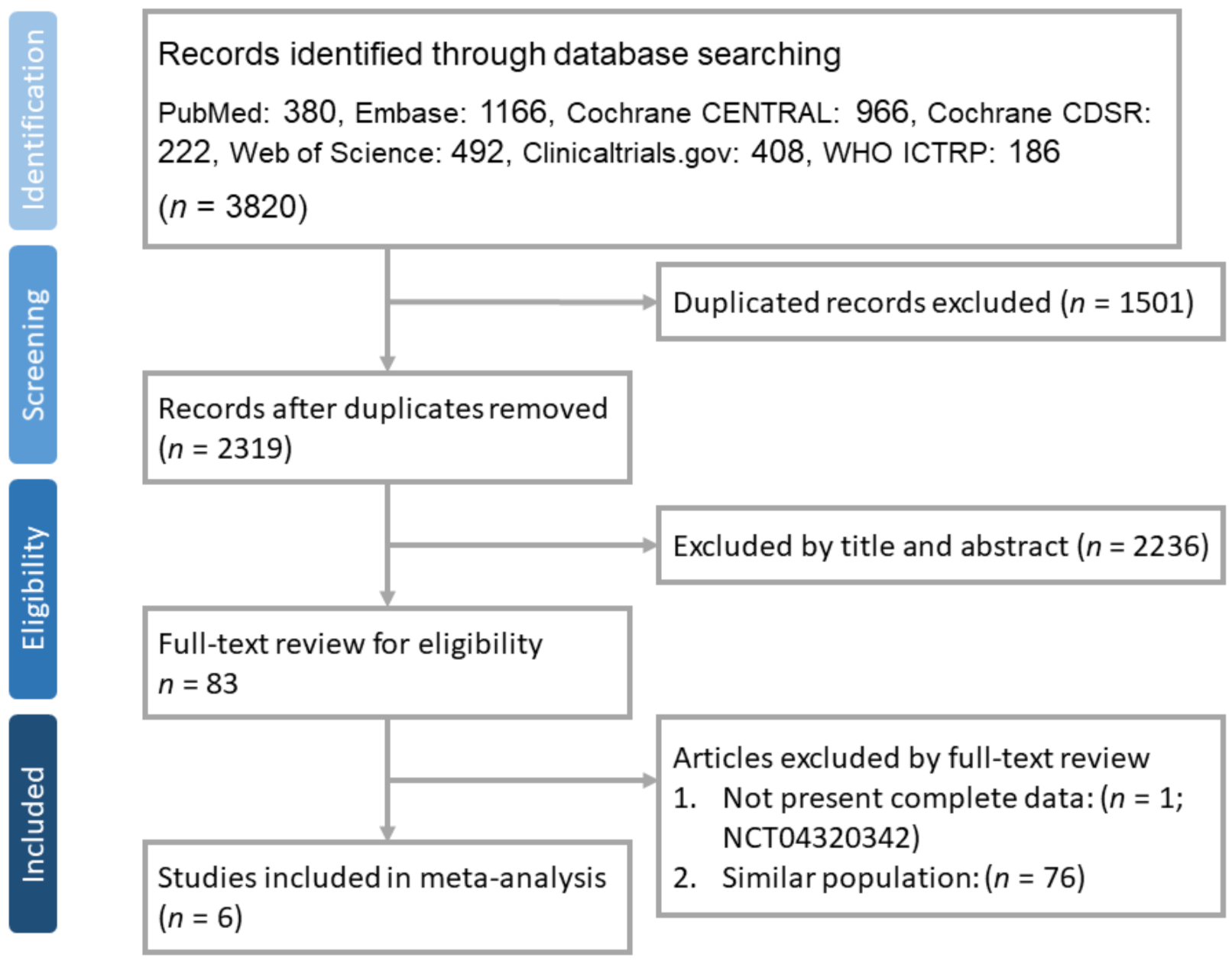
2.1. Study Search and Selection
2.2. Definitions and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Study Basic Characteristics
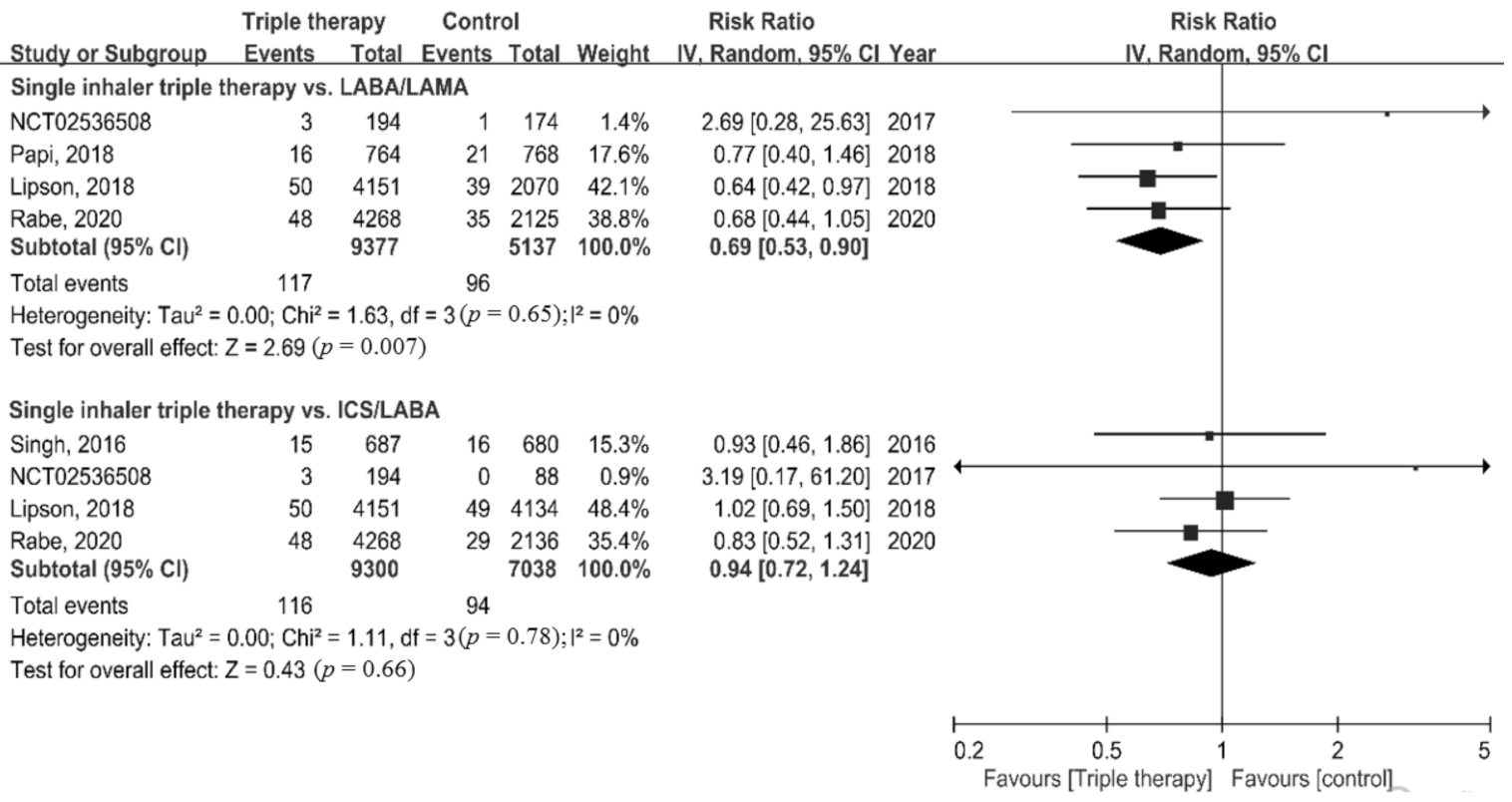
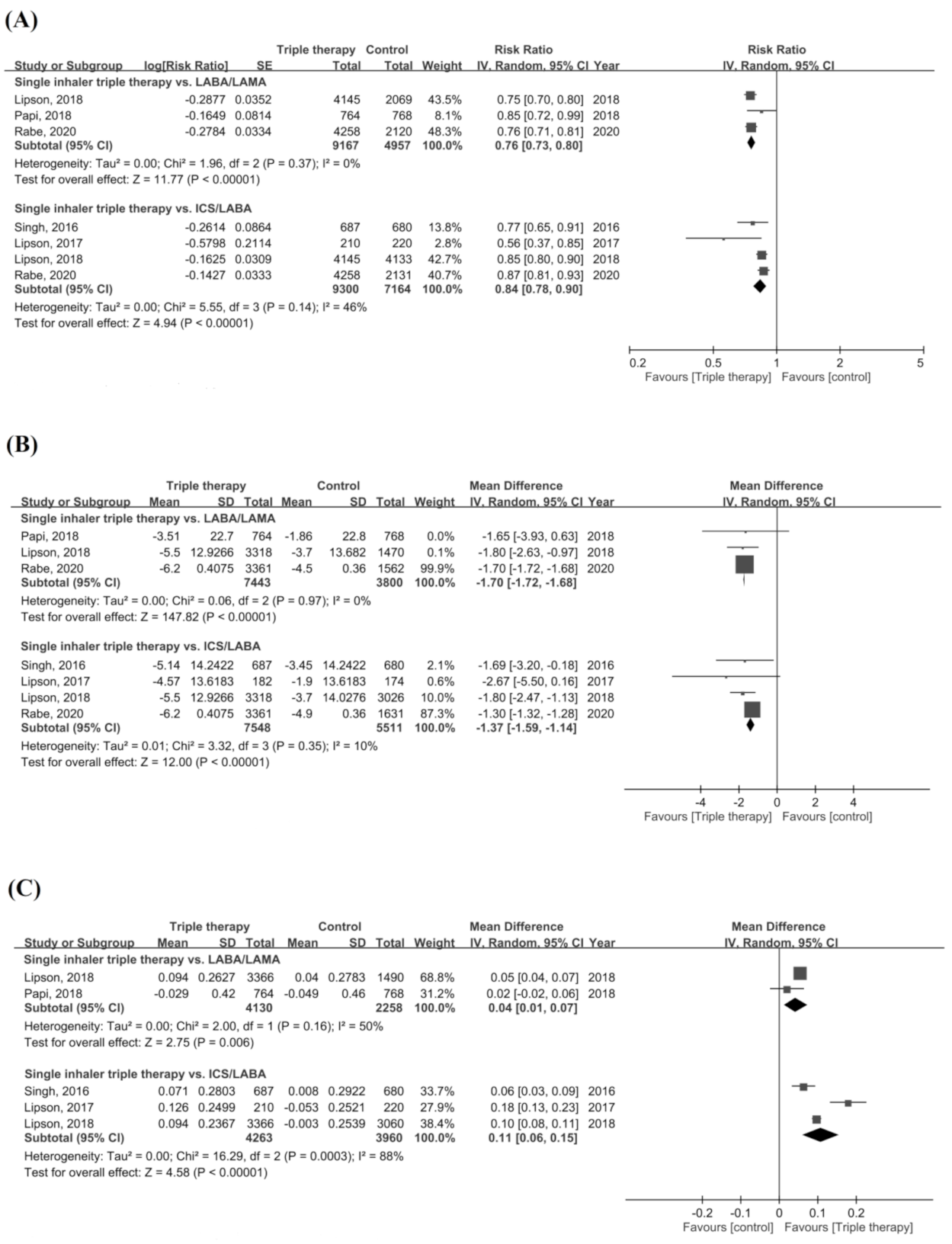
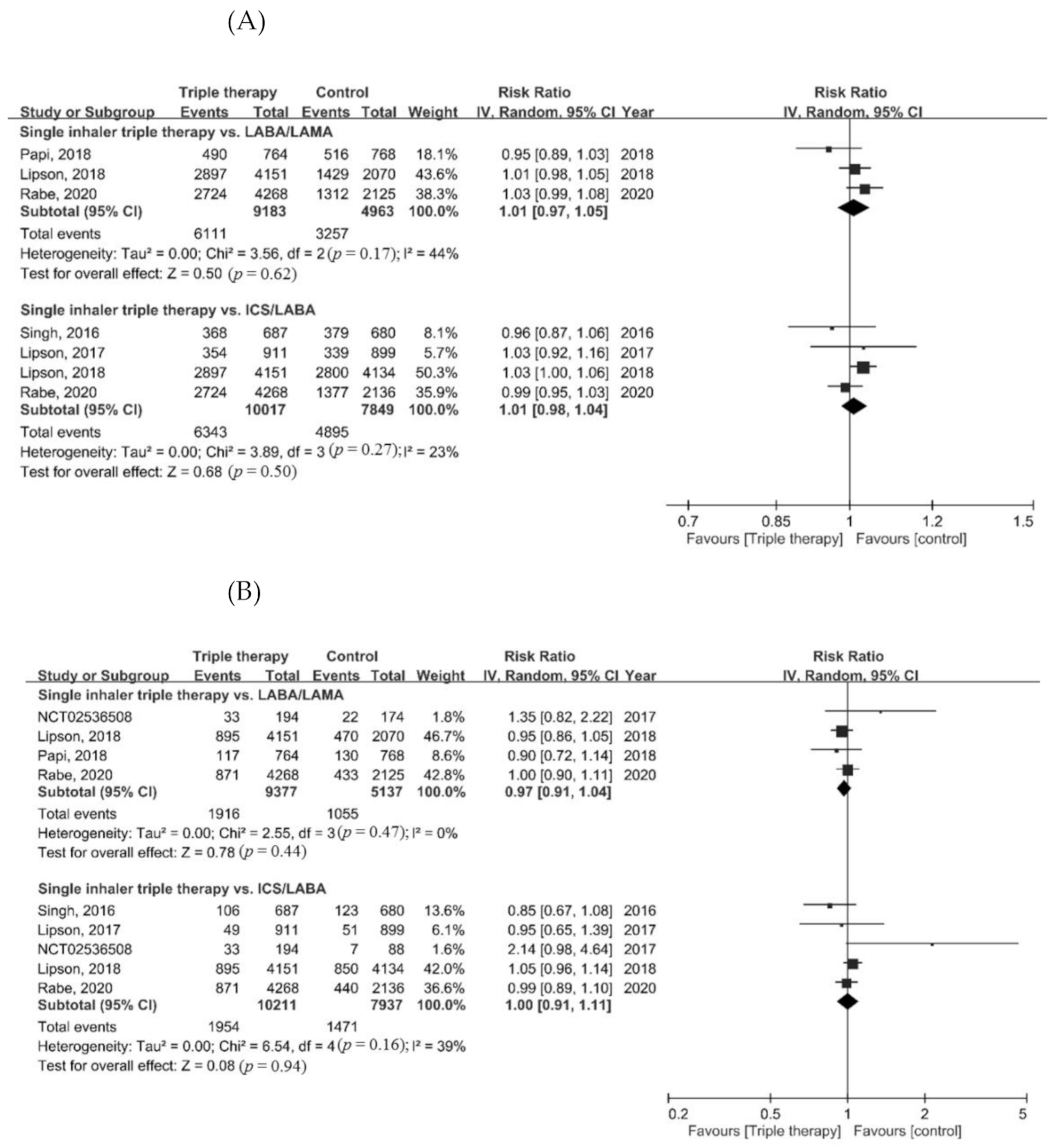
3.2. Outcome Measures
3.3. Sensitivity Analyses
3.4. Meta-Regression
3.5. Quality Assessment
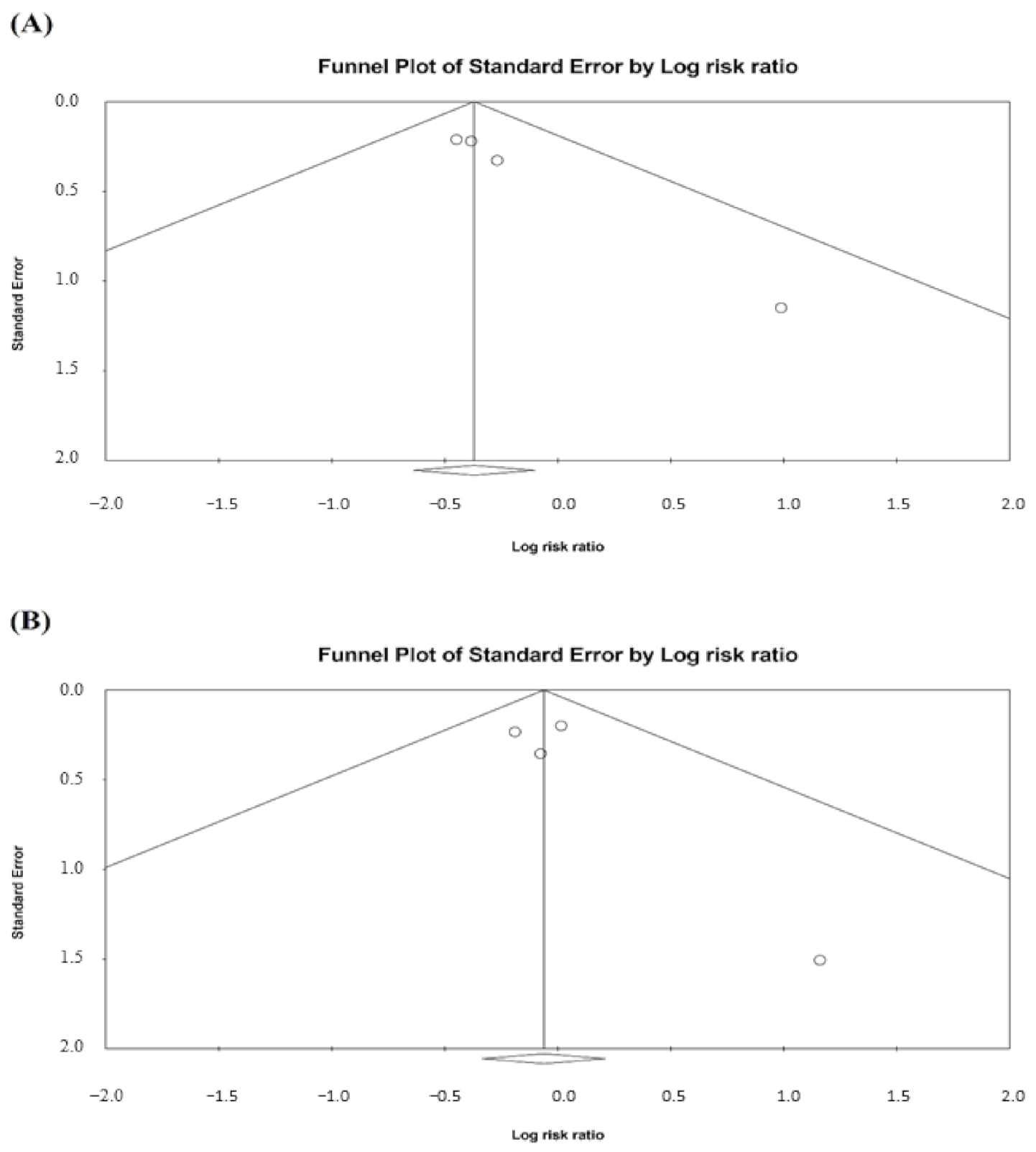
3.6. Publication Bias
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pauwels, R.A.; Buist, A.S.; Calverley, P.M.; Jenkins, C.R.; Hurd, S.S. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am. J. Respir. Crit. Care Med. 2001, 163, 1256–1276. [Google Scholar] [CrossRef] [Green Version]
- Eapen, M.S.; Myers, S.; Walters, E.H.; Sohal, S.S. Airway inflammation in chronic obstructive pulmonary disease (COPD): A true paradox. Expert. Rev. Respir. Med. 2017, 11, 827–839. [Google Scholar] [CrossRef] [PubMed]
- Eapen, M.S.; McAlinden, K.; Tan, D.; Weston, S.; Ward, C.; Muller, H.K.; Walters, E.H.; Sohal, S.S. Profiling cellular and inflammatory changes in the airway wall of mild to moderate COPD. Respirology 2017, 22, 1125–1132. [Google Scholar] [CrossRef] [PubMed]
- Nici, L.; Mammen, M.J.; Charbek, E.; Alexander, P.E.; Au, D.H.; Boyd, C.M.; Criner, G.J.; Donaldson, G.C.; Dreher, M.; Fan, V.S.; et al. Pharmacologic management of chronic obstructive pulmonary disease. An official American thoracic society clinical practice guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e56–e69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaduzo, S.; McGovern, V.; Roberts, J.; Scullion, J.E.; Singh, D. When to use single-inhaler triple therapy in COPD: A practical approach for primary care health care professionals. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 391–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanfleteren, L.; Fabbri, L.M.; Papi, A.; Petruzzelli, S.; Celli, B. Triple therapy (ICS/LABA/LAMA) in COPD: Time for a reappraisal. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 3971–3981. [Google Scholar] [CrossRef] [Green Version]
- Lipworth, B.; Kuo, C.R.; Jabbal, S. Current appraisal of single inhaler triple therapy in COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 3003–3009. [Google Scholar] [CrossRef] [Green Version]
- Ahn, J.H.; Chung, J.H.; Shin, K.C.; Choi, E.Y.; Jin, H.J.; Lee, M.S.; Nam, M.J.; Lee, K.H. Critical inhaler handling error is an independent risk factor for frequent exacerbations of chronic obstructive pulmonary disease: Interim results of a single center prospective study. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 2767–2775. [Google Scholar] [CrossRef] [Green Version]
- Collier, D.J.; Wielders, P.; van der Palen, J.; Heyes, L.; Midwinter, D.; Collison, K.; Preece, A.; Barnes, N.; Sharma, R. Critical error frequency and the impact of training with inhalers commonly used for maintenance treatment in chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 1301–1313. [Google Scholar] [CrossRef]
- Navaie, M.; Dembek, C.; Cho-Reyes, S.; Yeh, K.; Celli, B.R. Device use errors with soft mist inhalers: A global systematic literature review and meta-analysis. Chron. Respir. Dis. 2020, 17. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Garcia, C.; Barreiro, E.; Muñoz-Gall, X.; Bustamante-Madariaga, V.; de-Granda-Orive, I.; Gonzalez-Barcala, F.J. Common errors in inhalation therapy: Impact and solutions. Clin. Respir. J. 2020, 14, 1001–1010. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Marín, A.; Huerta, A.; Carcedo, D.; Villacampa, A.; Puig-Junoy, J. Estimation of the clinical and economic impact of an improvement in adherence based on the use of once-daily single-inhaler triple therapy in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 1643–1654. [Google Scholar] [CrossRef] [PubMed]
- Ismaila, A.S.; Risebrough, N.; Schroeder, M.; Shah, D.; Martin, A.; Goodall, E.C.; Ndirangu, K.; Criner, G.; Dransfield, M.; Halpin, D.M.; et al. Cost-effectiveness of once-daily single-inhaler triple therapy in COPD: The IMPACT trial. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 2681–2695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogart, M.; Stanford, R.H.; Laliberté, F.; Germain, G.; Wu, J.W.; Duh, M.S. Medication adherence and persistence in chronic obstructive pulmonary disease patients receiving triple therapy in a USA commercially insured population. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 343–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Palen, J.; Moeskops-van Beurden, W.; Dawson, C.M.; James, W.Y.; Preece, A.; Midwinter, D.; Barnes, N.; Sharma, R. A randomized, open-label, single-visit, crossover study simulating triple-drug delivery with Ellipta compared with dual inhaler combinations in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 2515–2523. [Google Scholar] [CrossRef] [Green Version]
- Ichinose, M.; Fukushima, Y.; Inoue, Y.; Hataji, O.; Ferguson, G.T.; Rabe, K.F.; Hayashi, N.; Okada, H.; Takikawa, M.; Bourne, E.; et al. Long-term safety and efficacy of budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler formulated using co-suspension delivery technology in Japanese patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 2993–3002. [Google Scholar] [CrossRef] [Green Version]
- Ichinose, M.; Fukushima, Y.; Inoue, Y.; Hataji, O.; Ferguson, G.T.; Rabe, K.F.; Hayashi, N.; Okada, H.; Takikawa, M.; Bourne, E.; et al. Efficacy and safety of budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler formulated using co-suspension delivery technology in Japanese patients with COPD: A subgroup analysis of the KRONOS study. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 2979–2991. [Google Scholar] [CrossRef] [Green Version]
- Kato, M.; Tomii, K.; Hashimoto, K.; Nezu, Y.; Ishii, T.; Jones, C.E.; Kilbride, S.; Gross, A.S.; Clifton, C.S.; Lipson, D.A. The IMPACT study—Single inhaler triple therapy (FF/UMEC/VI) versus FF/VI snd UMEC/VI in patients with COPD: Efficacy and safety in a Japanese population. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 2849–2861. [Google Scholar] [CrossRef] [Green Version]
- Ritondo, B.L.; Puxeddu, E.; Calzetta, L.; Cazzola, M.; Rogliani, P. Efficacy and safety of triple combination therapy for treating chronic obstructive pulmonary disease: An expert review. Expert Opin. Pharmacother. 2021, 22, 611–620. [Google Scholar] [CrossRef]
- Lipson, D.A.; Barnhart, F.; Brealey, N.; Brooks, J.; Criner, G.J.; Day, N.C.; Dransfield, M.T.; Halpin, D.M.G.; Han, M.K.; Jones, C.E.; et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N. Engl. J. Med. 2018, 378, 1671–1680. [Google Scholar] [CrossRef]
- Papi, A.; Vestbo, J.; Fabbri, L.; Corradi, M.; Prunier, H.; Cohuet, G.; Guasconi, A.; Montagna, I.; Vezzoli, S.; Petruzzelli, S.; et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): A double-blind, parallel group, randomised controlled trial. Lancet 2018, 391, 1076–1084. [Google Scholar] [CrossRef]
- Singh, D.; Papi, A.; Corradi, M.; Pavlišová, I.; Montagna, I.; Francisco, C.; Cohuet, G.; Vezzoli, S.; Scuri, M.; Vestbo, J. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): A double-blind, parallel group, randomised controlled trial. Lancet 2016, 388, 963–973. [Google Scholar] [CrossRef] [Green Version]
- Vestbo, J.; Papi, A.; Corradi, M.; Blazhko, V.; Montagna, I.; Francisco, C.; Cohuet, G.; Vezzoli, S.; Scuri, M.; Singh, D. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): A double-blind, parallel group, randomised controlled trial. Lancet 2017, 389, 1919–1929. [Google Scholar] [CrossRef] [Green Version]
- Rabe, K.F.; Martinez, F.J.; Ferguson, G.T.; Wang, C.; Singh, D.; Wedzicha, J.A.; Trivedi, R.; St Rose, E.; Ballal, S.; McLaren, J.; et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N. Engl. J. Med. 2020, 383, 35–48. [Google Scholar] [CrossRef]
- Singh, D.; Fabbri, L.M.; Vezzoli, S.; Petruzzelli, S.; Papi, A. Extrafine triple therapy delays COPD clinically important deterioration vs ICS/LABA, LAMA, or LABA/LAMA. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 531–546. [Google Scholar] [CrossRef] [Green Version]
- Lipson, D.A.; Crim, C.; Criner, G.J.; Day, N.C.; Dransfield, M.T.; Halpin, D.M.G.; Han, M.K.; Jones, C.E.; Kilbride, S.; Lange, P.; et al. Reduction in all-cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2020, 201, 1508–1516. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.C.; Chen, C.H.; Lin, C.Y.H.; Wang, C.Y.; Wang, Y.H. The effects of single inhaler triple therapy vs single inhaler dual therapy or separate triple therapy for the management of chronic obstructive pulmonary disease: A systematic review and meta-analysis of randomized controlled trials. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 1539–1548. [Google Scholar] [CrossRef] [Green Version]
- Mammen, M.J.; Lloyd, D.R.; Kumar, S.; Ahmed, A.S.; Pai, V.; Kunadharaju, R.; Gupta, S.; Nici, L.; Aaron, S.D.; Alexander, P.E. Triple therapy versus dual or monotherapy with long-acting bronchodilators for chronic obstructive pulmonary disease. A systematic review and meta-analysis. Ann. Am. Thorac. Soc. 2020, 17, 1308–1318. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Zhu, J.; Liu, Y.; Lai, W.; Lin, C.; Qiu, K.; Wu, J.; Yao, W. Triple therapy in the management of chronic obstructive pulmonary disease: Systematic review and meta-analysis. BMJ 2018, 363, k4388. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calzetta, L.; Cazzola, M.; Matera, M.G.; Rogliani, P. Adding a LAMA to ICS/LABA therapy: A meta-analysis of triple combination therapy in COPD. Chest 2019, 155, 758–770. [Google Scholar] [CrossRef] [PubMed]
- Lipson, D.A.; Barnacle, H.; Birk, R.; Brealey, N.; Locantore, N.; Lomas, D.A.; Ludwig-Sengpiel, A.; Mohindra, R.; Tabberer, M.; Zhu, C.Q.; et al. FULFIL trial: Once-daily triple therapy for patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2017, 196, 438–446. [Google Scholar] [CrossRef] [Green Version]
- Study to Assess the Safety and Tolerability of PT010, PT009 and PT003 in Subjects with Moderate to Very Severe Chronic Obstructive Pulmonary Disease. Available online: https://clinicaltrials.gov/ct2/show/study/NCT02536508 (accessed on 23 July 2021).
- Cazzola, M.; Rogliani, P.; Calzetta, L.; Matera, M.G. Triple therapy versus single and dual long-acting bronchodilator therapy in COPD: A systematic review and meta-analysis. Eur. Respir. J. 2018, 52, 1801586. [Google Scholar] [CrossRef]
- Liu, T.; Xiang, Z.J.; Hou, X.M.; Chai, J.J.; Yang, Y.L.; Zhang, X.T. Blood eosinophil count-guided corticosteroid therapy and as a prognostic biomarker of exacerbations of chronic obstructive pulmonary disease: A systematic review and meta-analysis. Ther. Adv. Chronic Dis. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Vedel-Krogh, S.; Nordestgaard, B.G.; Lange, P.; Vestbo, J.; Nielsen, S.F. Blood eosinophil count and risk of pneumonia hospitalisations in individuals with COPD. Eur. Respir. J. 2018, 51, 1800120. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease. 2021 Global Strategy for Prevention, Diagnosis and Management of Copd. Available online: https://goldcopd.org/2021-gold-reports/ (accessed on 27 July 2021).
- Janson, C.; Stratelis, G.; Miller-Larsson, A.; Harrison, T.W.; Larsson, K. Scientific rationale for the possible inhaled corticosteroid intraclass difference in the risk of pneumonia in COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 3055–3064. [Google Scholar] [CrossRef] [Green Version]
- Miravitlles, M.; Auladell-Rispau, A.; Monteagudo, M.; Vázquez-Niebla, J.C.; Mohammed, J.; Nuñez, A.; Urrútia, G. Systematic review on long-term adverse effects of inhaled corticosteroids in the treatment of COPD. Eur. Respir. Rev. 2021, 30, 210075. [Google Scholar] [CrossRef]
- Huang, T.M.; Kuo, K.C.; Wang, Y.H.; Wang, C.Y.; Lai, C.C.; Wang, H.C.; Chen, L.; Yu, C.J. Risk of active tuberculosis among COPD patients treated with fixed combinations of long-acting beta2 agonists and inhaled corticosteroids. BMC Infect. Dis. 2020, 20, 706. [Google Scholar] [CrossRef]
- Koarai, A.; Yamada, M.; Ichikawa, T.; Fujino, N.; Kawayama, T.; Sugiura, H. Triple versus LAMA/LABA combination therapy for patients with COPD: A systematic review and meta-analysis. Respir. Res. 2021, 22, 183. [Google Scholar] [CrossRef]
- Long, H.; Xu, H.; Janssens, J.P.; Guo, Y. Single-inhaler triple vs single-inhaler dual therapy in patients with chronic obstructive pulmonary disease: A meta-analysis of randomized control trials. Respir. Res. 2021, 22, 209. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, S.; Barnes, N.; Brusselle, G.; Compton, C.; Criner, G.J.; Dransfield, M.T.; Halpin, D.M.G.; Han, M.K.; Hartley, B.; Lange, P.; et al. Blood eosinophils and treatment response with triple and dual combination therapy in chronic obstructive pulmonary disease: Analysis of the IMPACT trial. Lancet Respir. Med. 2019, 7, 745–756. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Site | No of Participants | Study Period | Inclusion Criteria | Inhalation Therapy | Primary Outcome | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| FEV1 | Exacerbation history in previous year | Symptom scores | Excluded asthma | Others | Fixed triple | Comparator | |||||
| Lipson et al., 2018 (IMPACT) [20] | 37 countries | 10,355 | 2014–2017 | FEV1 of 50-80% | ≥1 moderate/severe exacerbation if FEV1 < 50% or ≥2 moderate exacerbations or one severe exacerbation if FEV1 of 50-80% | CAT score ≥ 10 | No | ≥40 years; MCID: 2 point; use LAMA, a LABA, or an ICS alone or in combination | FF/UME/VIL | FF/VIL or UME/VIL | Annual rate of moderate or severe COPD exacerbations |
| Papi et al., 2018 (TRIBUTE) [21] | 187 sites in 17 countries | 1532 | 2015–2017 | FEV1 < 50% | ≥1 moderate or severe exacerbation | CAT score ≥ 10 | Yes | ≥40 years; current or ex-smoker; used ICS/LABA, ICS/LAMA or LABA/LAMA for ≥2 months | BDP/FOR/GB | IND/GB | Moderate to severe COPD exacerbation rate for 52 weeks |
| Singh et al., 2016 (TRIOLOGY) [22] | 159 sites in 14 countries | 1368 | 2014–2016 | FEV1 < 50% | ≥1 moderate/severe exacerbation | CAT score ≥ 10 | Yes | ≥40 years; current or ex-smoker; used ICS/LABA, ICS/LAMA or LABA/LAMA for ≥2 months | BDP/FOR/GB | BDP/FOR | Moderate to severe COPD exacerbation rate for 52 weeks |
| Rabe et al., 2020 (ETHOS) [24] | 740 sites in 26 countries | 8509 | 2015–2019 | FEV1 of 25-65%; | ≥1 moderate/severe exacerbation if FEV1 < 50% or ≥2 moderate exacerbations or one severe exacerbation if FEV1 ≥ 50% | CAT score ≥ 10 | Yes | 40 to 80 years; MICD: 2 point; receiving at least two inhaled maintenance therapies at the time of screening; a smoking history of at least 10 pack-years | BUD/FOR/GB | GB/FOR or BUD/FOR | Annual rate of moderate or severe COPD exacerbations |
| Lipson et al., 2017 (FULFIL)—extension population [33] | 160 sites in 15 countries | 430 | 2015–2016 | FEV1 < 50% or 50%-80% | ≥2 moderate exacerbations or ≥1 severe exacerbation if FEV1 ≥ 50% | CAT score ≥ 10 | Yes | ≥40 years; receiving daily maintenance therapy for COPD for at least 3 months | FF/UME/VIL | BUD/FOR | Lung functionand health-related quality of life |
| NCT02536508 [34] | 64 cites in US | 627 | 2015–2017 | NA | NA | NA | No | 40 to 80 years, moderate to very severe COPD | BUD/FOR/GB | GB/FOR or BUD/FOR | Percent change from baseline in BMD of the lumbar spine |
| ICS/LABA | LAMA/LABA | |||
|---|---|---|---|---|
| Outcome | Slope | p | Slope | p |
| Mortality | −0.16 | 0.545 | −0.74 | 0.006 |
| Annual rate of moderate/severe exacerbation | −0.31 | <0.001 | −0.50 | <0.001 |
| Change of SGRQ | −2.67 | <0.001 | −3.09 | <0.001 |
| Change of FEV1 | NA | NA | ||
| Adverse event | 0.00 | 0.997 | 0.03 | 0.272 |
| Serious adverse event | −0.01 | 0.911 | −0.05 | 0.421 |
| Pneumonia | −0.10 | 0.479 | 0.71 | <0.001 |
| Cardiovascular event | 0.14 | 0.328 | −0.36 | 0.157 |
| Respiratory tract infection | 0.16 | 0.247 | 0.11 | 0.673 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, C.-C.; Chen, C.-H.; Chen, K.-H.; Wang, C.-Y.; Huang, T.-M.; Wang, Y.-H.; Wang, H.-C. The Impact of 52-Week Single Inhaler Device Triple Therapy versus Dual Therapy on the Mortality of COPD Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Life 2022, 12, 173. https://doi.org/10.3390/life12020173
Lai C-C, Chen C-H, Chen K-H, Wang C-Y, Huang T-M, Wang Y-H, Wang H-C. The Impact of 52-Week Single Inhaler Device Triple Therapy versus Dual Therapy on the Mortality of COPD Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Life. 2022; 12(2):173. https://doi.org/10.3390/life12020173
Chicago/Turabian StyleLai, Chih-Cheng, Chao-Hsien Chen, Kuang-Hung Chen, Cheng-Yi Wang, Tsan-Ming Huang, Ya-Hui Wang, and Hao-Chien Wang. 2022. "The Impact of 52-Week Single Inhaler Device Triple Therapy versus Dual Therapy on the Mortality of COPD Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Life 12, no. 2: 173. https://doi.org/10.3390/life12020173
APA StyleLai, C. -C., Chen, C. -H., Chen, K. -H., Wang, C. -Y., Huang, T. -M., Wang, Y. -H., & Wang, H. -C. (2022). The Impact of 52-Week Single Inhaler Device Triple Therapy versus Dual Therapy on the Mortality of COPD Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Life, 12(2), 173. https://doi.org/10.3390/life12020173