
Cardiovascular, Lymphatic, and Ocular Health in Space


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
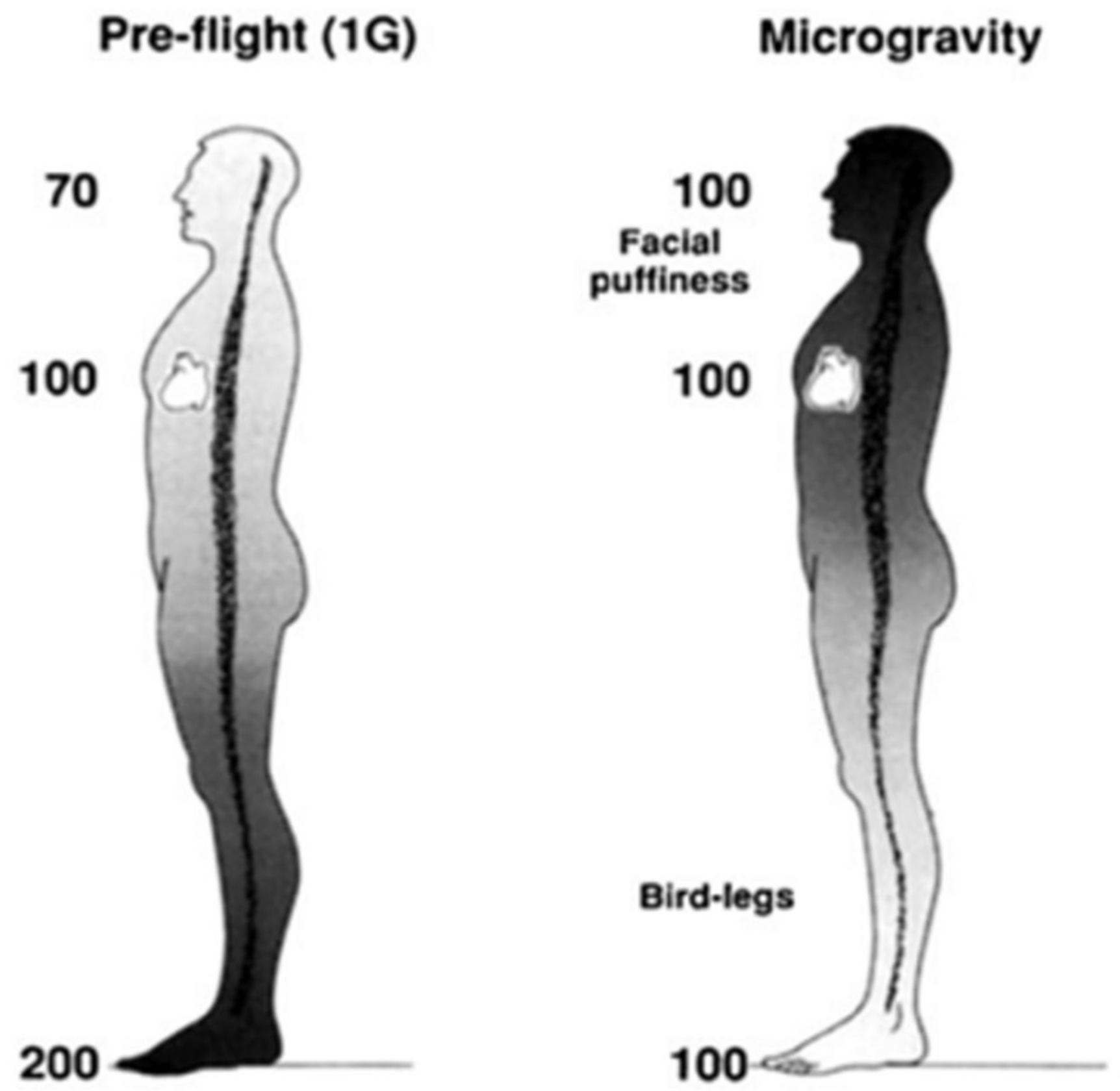
2. Fluid Shifts and Venous Changes Due to Space Travel
3. Microgravity Analogs on the Lymphatic System
4. Ocular Health in Space
4.1. Spaceflight-Associated Neuro-Ocular Syndrome
4.2. Lower Body Negative Pressure to Prevent SANS
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hargens, A.R.; Watenpaugh, D.E. Cardiovascular adaptation to spaceflight. Med. Sci. Sports Exerc. 1996, 28, 977–982. Available online: https://journals.lww.com/acsm-msse/Fulltext/1996/08000/Cardiovascular_adaptation_to_spaceflight.7.aspx (accessed on 3 November 2021). [CrossRef] [PubMed]
- Michel, E.L.; Johnston, R.S.; Dietlein, L.F. Biomedical results of the Skylab Program. Life Sci. Space Res. 1976, 14, 3–18. [Google Scholar]
- Hargens, A.R.; Bhattacharya, R.; Schneider, S.M. Space physiology VI: Exercise, artificial gravity, and countermeasure development for prolonged space flight. Eur. J. Appl. Physiol. 2013, 113, 2183–2192. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Ambesi-Impiombato, F.S.; Beccari, T.; Conte, C.; Cataldi, S.; Curcio, F.; Albi, E. Spaceflight Induced Disorders: Potential Nutritional Countermeasures. Front. Bioeng. Biotechnol. 2021, 9, 666683. Available online: https://www.frontiersin.org/article/10.3389/fbioe.2021.666683 (accessed on 21 January 2022). [CrossRef] [PubMed]
- Patel, Z.S.; Brunstetter, T.J.; Tarver, W.J.; Whitmire, A.M.; Zwart, S.R.; Smith, S.M.; Huff, J.L. Red risks for a journey to the red planet: The highest priority human health risks for a mission to Mars. NPJ Microgravity 2020, 6, 1–13. [Google Scholar] [CrossRef]
- Baldwin, K.M. Effect of spaceflight on the functional, biochemical, and metabolic properties of skeletal muscle. Med. Sci. Sports Exerc. 1996, 28, 983–987. [Google Scholar] [CrossRef]
- Kim, D.S.; Vaquer, S.; Mazzolai, L.; Roberts, L.N.; Pavela, J.; Watanabe, M.; Weerts, G.; Green, D.A. The effect of microgravity on the human venous system and blood coagulation: A systematic review. Exp. Physiol. 2021, 106, 1149–1158. [Google Scholar] [CrossRef]
- Siamwala, J.H.; Reddy, S.H.; Majumder, S.; Kolluru, G.K.; Muley, A.; Sinha, S.; Chatterjee, S. Simulated microgravity perturbs actin polymerization to promote nitric oxide-associated migration in human immortalized Eahy926 cells. Protoplasma 2010, 242, 3–12. [Google Scholar] [CrossRef]
- Harris, K.M.; Petersen, L.G.; Weber, T. Reviving lower body negative pressure as a countermeasure to prevent pathological vascular and ocular changes in microgravity. NPJ Microgravity 2020, 6, 38. [Google Scholar] [CrossRef]
- Shimizu, Y.; Kodama, K.; Nishi, N.; Kasagi, F.; Suyama, A.; Soda, M.; Grant, E.J.; Sugiyama, H.; Sakata, R.; Moriwaki, H.; et al. Radiation exposure and circulatory disease risk: Hiroshima and Nagasaki atomic bomb survivor data, 1950–2003. BMJ 2010, 340, b5349. [Google Scholar] [CrossRef] [Green Version]
- Little, M.P.; Azizova, T.V.; Bazyka, D.; Bouffler, S.D.; Cardis, E.; Chekin, S.; Chumak, V.V.; Cucinotta, F.A.; de Vathaire, F.; Hall, P.; et al. Systematic review and meta-analysis of circulatory disease from exposure to low-level ionizing radiation and estimates of potential population mortality risks. Environ. Health Perspect. 2012, 120, 1503–1511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.F.; Hargens, A.R. Spaceflight-Induced Intracranial Hypertension and Visual Impairment: Pathophysiology and Countermeasures. Physiol. Rev. 2018, 98, 59–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boerma, M.; Nelson, G.A.; Sridharan, V.; Mao, X.W.; Koturbash, I.; Hauer-Jensen, M. Space radiation and cardiovascular disease risk. World J. Cardiol. 2015, 7, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Delp, M.D.; Charvat, J.M.; Limoli, C.L.; Globus, R.K.; Ghosh, P. Apollo Lunar Astronauts Show Higher Cardiovascular Disease Mortality: Possible Deep Space Radiation Effects on the Vascular Endothelium. Sci. Rep. 2016, 6, 29901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magazine, S.; Palus, S. One Idea to Get to Mars: Fill the Walls of a Spaceship With Water. Smithsonian Magazine. Available online: https://www.smithsonianmag.com/smart-news/one-idea-get-mars-fill-spaceships-walls-water-180953428/ (accessed on 18 December 2021).
- Alitalo, K. The lymphatic vasculature in disease. Nat. Med. 2011, 17, 1371–1380. [Google Scholar] [CrossRef]
- Petrova, T.V.; Koh, G.Y. Organ-specific lymphatic vasculature: From development to pathophysiology. J. Exp. Med. 2018, 215, 35–49. [Google Scholar] [CrossRef]
- Jacob, L.; Boisserand, L.S.B.; Geraldo, L.H.M.; de Brito Neto, J.; Mathivet, T.; Antila, S.; Barka, B.; Xu, Y.; Thomas, J.M.; Pestel, J.; et al. Anatomy and function of the vertebral column lymphatic network in mice. Nat. Commun. 2019, 10, 4594. [Google Scholar] [CrossRef]
- Gashev, A.A.; Delp, M.D.; Zawieja, D.C. Inhibition of active lymph pump by simulated microgravity in rats. Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H2295–H2308. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, J.C.; Kwon, S.; Pinal, A.; Bareis, A.; Velasquez, F.C.; Janssen, C.F.; Morrow, J.R.; Fife, C.E.; Karni, R.J.; Sevick-Muraca, E.M. Assessing lymphatic route of CSF outflow and peripheral lymphatic contractile activity during head-down tilt using near-infrared fluorescence imaging. Physiol. Rep. 2020, 8, e14375. [Google Scholar] [CrossRef] [Green Version]
- Hargens, A.R.; Richardson, S. Cardiovascular adaptations, fluid shifts, and countermeasures related to space flight. Physiol. Neurobiol. 2009, 169 (Suppl. S1), S30–S33. [Google Scholar] [CrossRef]
- Zawieja, D.C. Contractile Physiology of Lymphatics. Lymphat. Res. Biol. 2009, 7, 87–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gashev, A.A. Physiologic aspects of lymphatic contractile function: Current perspectives. Ann. N. Y. Acad. Sci. 2002, 979, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, C.; Karni, R.J.; Naqvi, S.; Aldrich, M.B.; Zhu, B.; Morrow, J.R.; Sevick-Muraca, E.M.; Rasmussen, J.C. Head and Neck Lymphedema: Treatment Response to Single and Multiple Sessions of Advanced Pneumatic Compression Therapy. Otolaryngol.-Head Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head Neck Surg. 2019, 160, 622–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, M.H. Monro-Kellie 2.0: The dynamic vascular and venous pathophysiological components of intracranial pressure. J. Cereb. Blood Flow Metab. 2016, 36, 1338–1350. [Google Scholar] [CrossRef] [Green Version]
- Fu, B.M.; Tarbell, J.M. Mechano-sensing and transduction by endothelial surface glycocalyx: Composition, structure, and function. Wiley Interdiscip. Rev. Syst. Biol. Med. 2013, 5, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Weinbaum, S.; Tarbell, J.M.; Damiano, E.R. The structure and function of the endothelial glycocalyx layer. Annu. Rev. Biomed. Eng. 2007, 9, 121–167. [Google Scholar] [CrossRef]
- Reitsma, S.; Slaaf, D.W.; Vink, H.; van Zandvoort, M.A.M.J.; oude Egbrink, M.G.A. The endothelial glycocalyx: Composition, functions, and visualization. Pflug. Arch. 2007, 454, 345–359. [Google Scholar] [CrossRef] [Green Version]
- Revised Starling Equation and the Glycocalyx Model of Transvascular Fluid Exchange: An Improved Paradigm for Prescribing Intravenous Fluid Therapy|BJA: British Journal of Anaesthesia | Oxford Academic. Available online: https://academic.oup.com/bja/article/108/3/384/419160 (accessed on 22 November 2021).
- Drummer, C.; Gerzer, R.; Baisch, F.; Heer, M. Body fluid regulation in micro-gravity differs from that on Earth: An overview. Pflug. Arch. 2000, 441 (Suppl. S2–3), R66–R72. [Google Scholar] [CrossRef]
- Diedrich, A.; Paranjape, S.Y.; Robertson, D. Plasma and blood volume in space. Am. J. Med. Sci. 2007, 334, 80–85. [Google Scholar] [CrossRef]
- Combined Effects of Low-Dose Proton Radiation and Simulated Microgravity on the Mouse Retina and the Hematopoietic System. Available online: https://bioone.org/journals/radiation-research/volume-192/issue-3/RR15219.1/Combined-Effects-of-Low-Dose-Proton-Radiation-and-Simulated-Microgravity/10.1667/RR15219.1.full (accessed on 22 November 2021).
- Li, M.; Holmes, V.; Zhou, Y.; Ni, H.; Sanzari, J.K.; Kennedy, A.R.; Weissman, D. Hindlimb Suspension and SPE-Like Radiation Impairs Clearance of Bacterial Infections. PLoS ONE 2014, 9, e85665. [Google Scholar] [CrossRef]
- Romero-Weaver, A.L.; Lin, L.; Carabe-Fernandez, A.; Kennedy, A.R. Effects of Solar Particle Event-Like Proton Radiation and/or Simulated Microgravity on Circulating Mouse Blood Cells. Gravit. Space Res. Publ. Am. Soc. Gravit. Space Res. 2014, 2, 42. [Google Scholar] [CrossRef]
- Martin Paez, Y.; Mudie, L.I.; Subramanian, P.S. Spaceflight Associated Neuro-Ocular Syndrome (SANS): A Systematic Review and Future Directions. Eye Brain 2020, 12, 105–117. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Sciences Policy; Committee to Review NASA’s Evidence Reports on Human Health Risks. Review of NASA’s Evidence Reports on Human Health Risks: 2016 Letter Report; Liverman, C.T., Masys, D.R., Scott-Conner, C.E.H., Eds.; National Academies Press (US): Washington, DC, USA, 2017. Available online: http://www.ncbi.nlm.nih.gov/books/NBK424965/ (accessed on 18 December 2021).
- Fogarty, J.A.; Otto, C.; Kerstman, E.; Oubre, C.; Wu, J. The Visual Impairment Intracranial Pressure Summit Report; NASA/TP–2011-216160; NASA: Washington, DC, USA, 2011.
- Marshall-Goebel, K.; Barratt, M.; Gibson, C. Ophthalmic changes and increased intracranial pressure associated with long duration spaceflight: An emerging understanding. Acta Astronaut. 2013, 87, 77–87. [Google Scholar] [CrossRef]
- Mader, T.H.; Gibson, C.R.; Pass, A.F.; Kramer, L.A.; Lee, A.G.; Fogarty, J.; Tarver, W.J.; Dervay, J.P.; Hamilton, D.R.; Sargsyan, A.; et al. Optic Disc Edema, Globe Flattening, Choroidal Folds, and Hyperopic Shifts Observed in Astronauts after Long-duration Space Flight. Ophthalmology 2011, 118, 2058–2069. [Google Scholar] [CrossRef] [Green Version]
- Wojcik, P.; Kini, A.; Al Othman, B.; Galdamez, L.A.; Lee, A.G. Spaceflight associated neuro-ocular syndrome. Curr. Opin. Neurol. 2020, 33, 62–67. [Google Scholar] [CrossRef]
- Killer, H.E.; Jaggi, G.P.; Flammer, J.; Miller, N.R.; Huber, A.R.; Mironov, A. Cerebrospinal fluid dynamics between the intracranial and the subarachnoid space of the optic nerve. Is it always bidirectional? Brain J. Neurol. 2007, 130, 514–520. [Google Scholar] [CrossRef]
- Killer, H.E.; Jaggi, G.P.; Miller, N.R.; Huber, A.R.; Landolt, H.; Mironov, A.; Meyer, P.; Remonda, L. Cerebrospinal fluid dynamics between the basal cisterns and the subarachnoid space of the optic nerve in patients with papilloedema. Br. J. Ophthalmol. 2011, 95, 822–827. [Google Scholar] [CrossRef] [Green Version]
- Killer, H.E.; Jaggi, G.P.; Flammer, J.; Miller, N.R.; Huber, A.R. The optic nerve: A new window into cerebrospinal fluid composition? Brain J. Neurol. 2006, 129, 1027–1030. [Google Scholar] [CrossRef] [Green Version]
- Killer, H.E.; Subramanian, P.S. Compartmentalized cerebrospinal fluid. Int. Ophthalmol. Clin. 2014, 54, 95–102. [Google Scholar] [CrossRef]
- Lee, A.G.; Mader, T.H.; Gibson, C.R.; Tarver, W.; Rabiei, P.; Riascos, R.F.; Galdamez, L.A.; Brunstetter, T. Spaceflight associated neuro-ocular syndrome (SANS) and the neuro-ophthalmologic effects of microgravity: A review and an update. NPJ Microgravity 2020, 6, 7. [Google Scholar] [CrossRef] [Green Version]
- Zwart, S.R.; Gregory, J.F.; Zeisel, S.H.; Gibson, C.R.; Mader, T.H.; Kinchen, J.M.; Ueland, P.M.; Ploutz-Snyder, R.; Heer, M.A.; Smith, S.M. Genotype, B-vitamin status, and androgens affect spaceflight-induced ophthalmic changes. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2016, 30, 141–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwart, S.R.; Laurie, S.S.; Chen, J.J.; Macias, B.R.; Lee, S.M.; Stenger, M.; Grantham, B.; Carey, K.; Young, M.; Smith, S.M. Association of Genetics and B Vitamin Status With the Magnitude of Optic Disc Edema During 30-Day Strict Head-Down Tilt Bed Rest. JAMA Ophthalmol. 2019, 137, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Yarmanova, E.N.; Kozlovskaya, I.B.; Khimoroda, N.N.; Fomina, E.V. Evolution of Russian Microgravity Countermeasures. Aerosp. Med. Hum. Perform. 2015, 86 (Suppl. S12), A32–A37. [Google Scholar] [CrossRef] [PubMed]
- Rubber Vacuum Pants that Suck—A Lab Aloft (International Space Station Research). Available online: https://blogs.nasa.gov/ISS_Science_Blog/2015/06/02/rubber-vacuum-pants-that-suck/ (accessed on 18 December 2021).
- Hearon, C.M.; Dias, K.A.; Babu, G.; Marshall, J.E.; Leidner, J.; Peters, K.; Silva, E.; MacNamara, J.P.; Campain, J.; Levine, B.D. Effect of Nightly Lower Body Negative Pressure on Choroid Engorgement in a Model of Spaceflight-Associated Neuro-ocular Syndrome: A Randomized Crossover Trial. JAMA Ophthalmol. 2022, 140, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Esch, B.T.A.; Scott, J.M.; Warburton, D.E.R. Construction of a lower body negative pressure chamber. Adv. Physiol. Educ. 2007, 31, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Hargens, A.R.; Kim, J. Increasing Seated Reaction Forces with Lower Body Negative Pressure. Department of Orthopaedic Surgery, University of California-San Diego, San Diego, CA, USA, 2021. under review. [Google Scholar]
- Kassel, R.; Velichala, S.; Ly, V.; Macias, B.R.; Lee, S.M.C.; Watenpaugh, D.E.; Hargens, A.R. Self-Generated Lower Body Negative Pressure, a No-Power Countermeasure for Deep Space Missions. Department of Orthopaedic Surgery, UC-San Diego Medical Center, University of California-San Diego, San Diego, CA, USA, 2021. to be submitted. [Google Scholar]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ly, V.; Velichala, S.R.; Hargens, A.R. Cardiovascular, Lymphatic, and Ocular Health in Space. Life 2022, 12, 268. https://doi.org/10.3390/life12020268
Ly V, Velichala SR, Hargens AR. Cardiovascular, Lymphatic, and Ocular Health in Space. Life. 2022; 12(2):268. https://doi.org/10.3390/life12020268
Chicago/Turabian StyleLy, Victoria, Suhas Rao Velichala, and Alan R. Hargens. 2022. "Cardiovascular, Lymphatic, and Ocular Health in Space" Life 12, no. 2: 268. https://doi.org/10.3390/life12020268
APA StyleLy, V., Velichala, S. R., & Hargens, A. R. (2022). Cardiovascular, Lymphatic, and Ocular Health in Space. Life, 12(2), 268. https://doi.org/10.3390/life12020268