
Kinetics of Heterogeneous Background in Stargardt’s Disease over Time

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Eligibility Criteria
2.3. Procedures
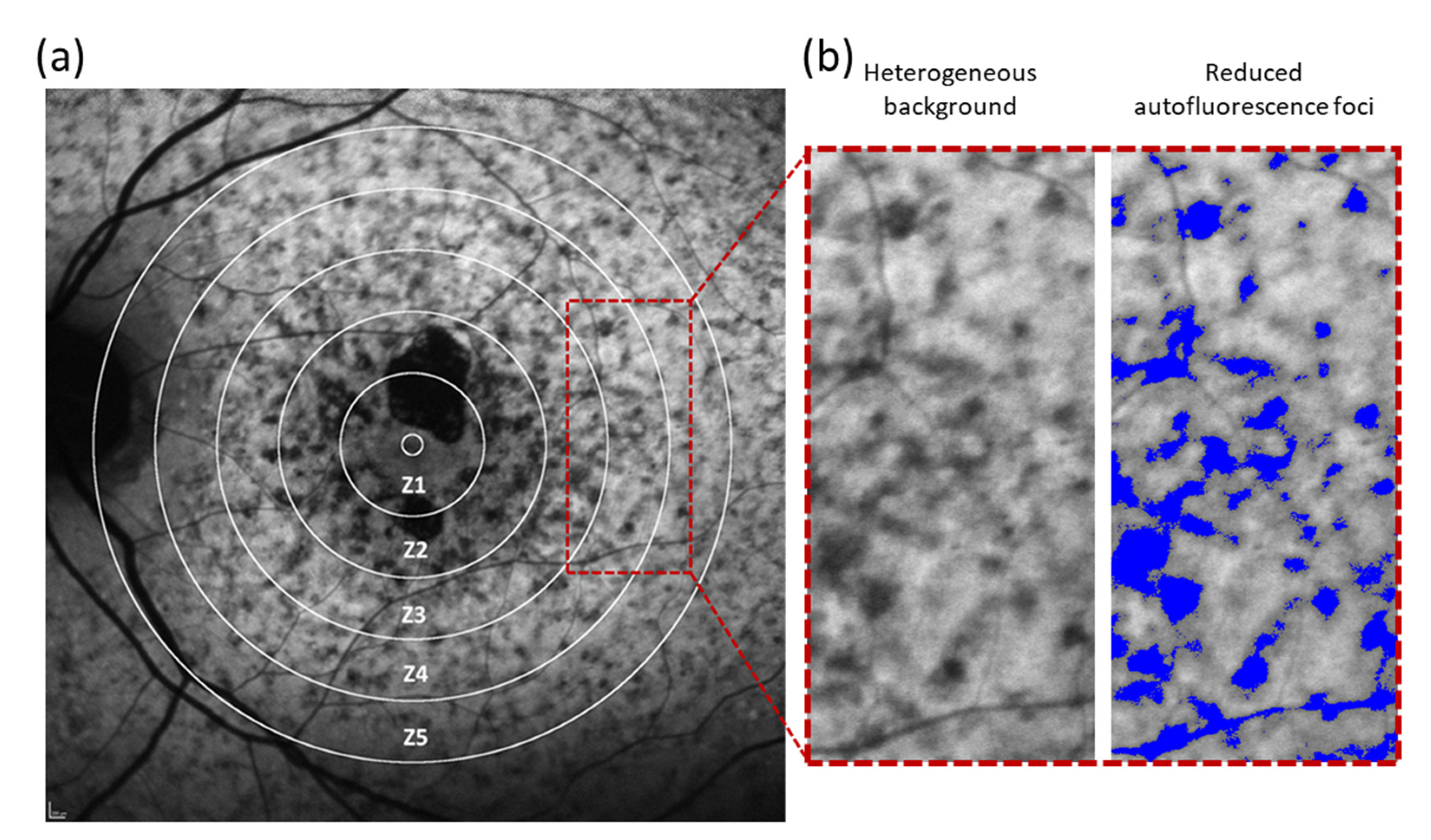
2.4. Processing of FAF Images
2.5. Measuring the Progression of FRA over Time
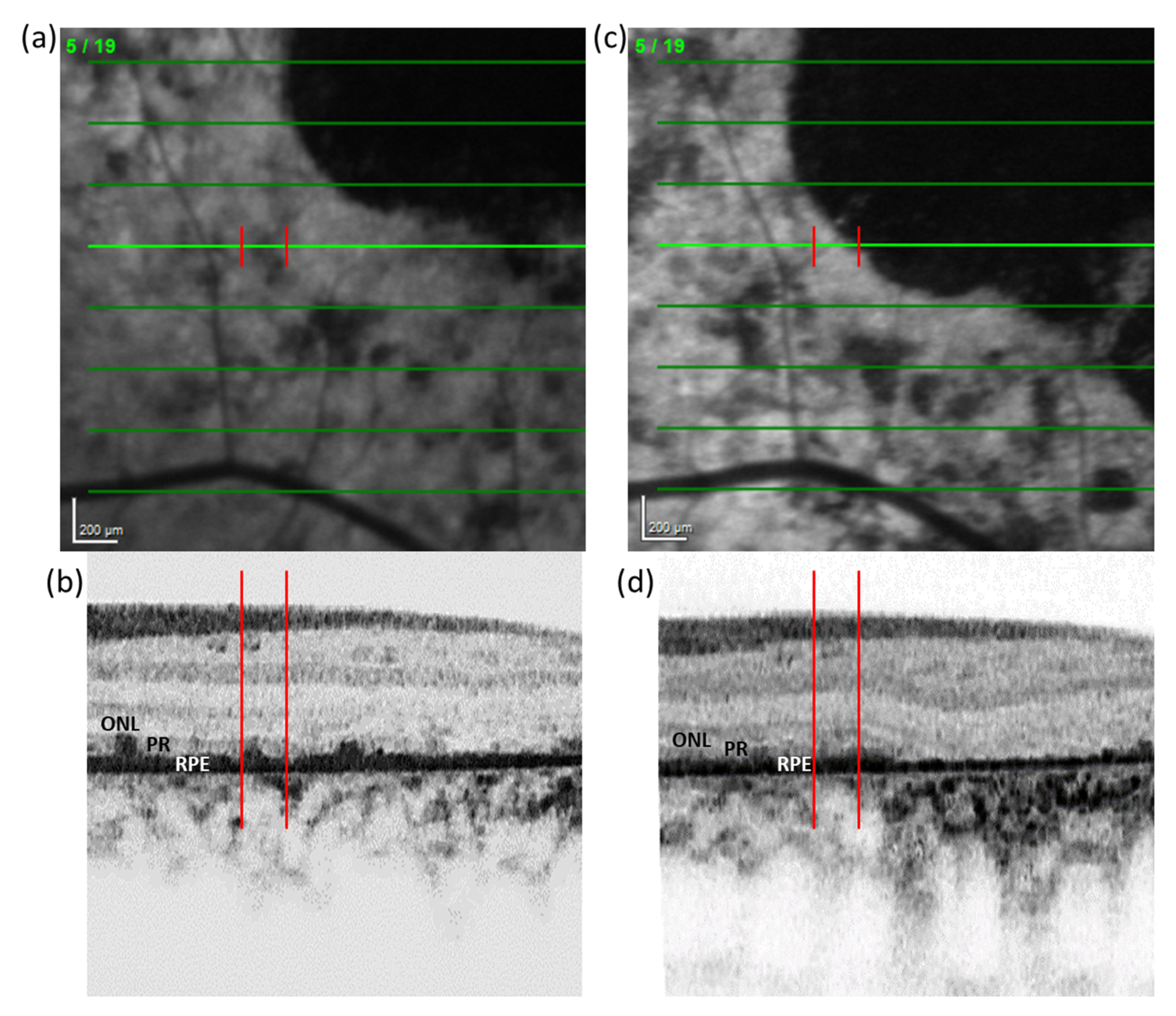
2.6. Correlation of FRA with Structural SD-OCT
2.7. Statistical Analysis
3. Results
3.1. Patients
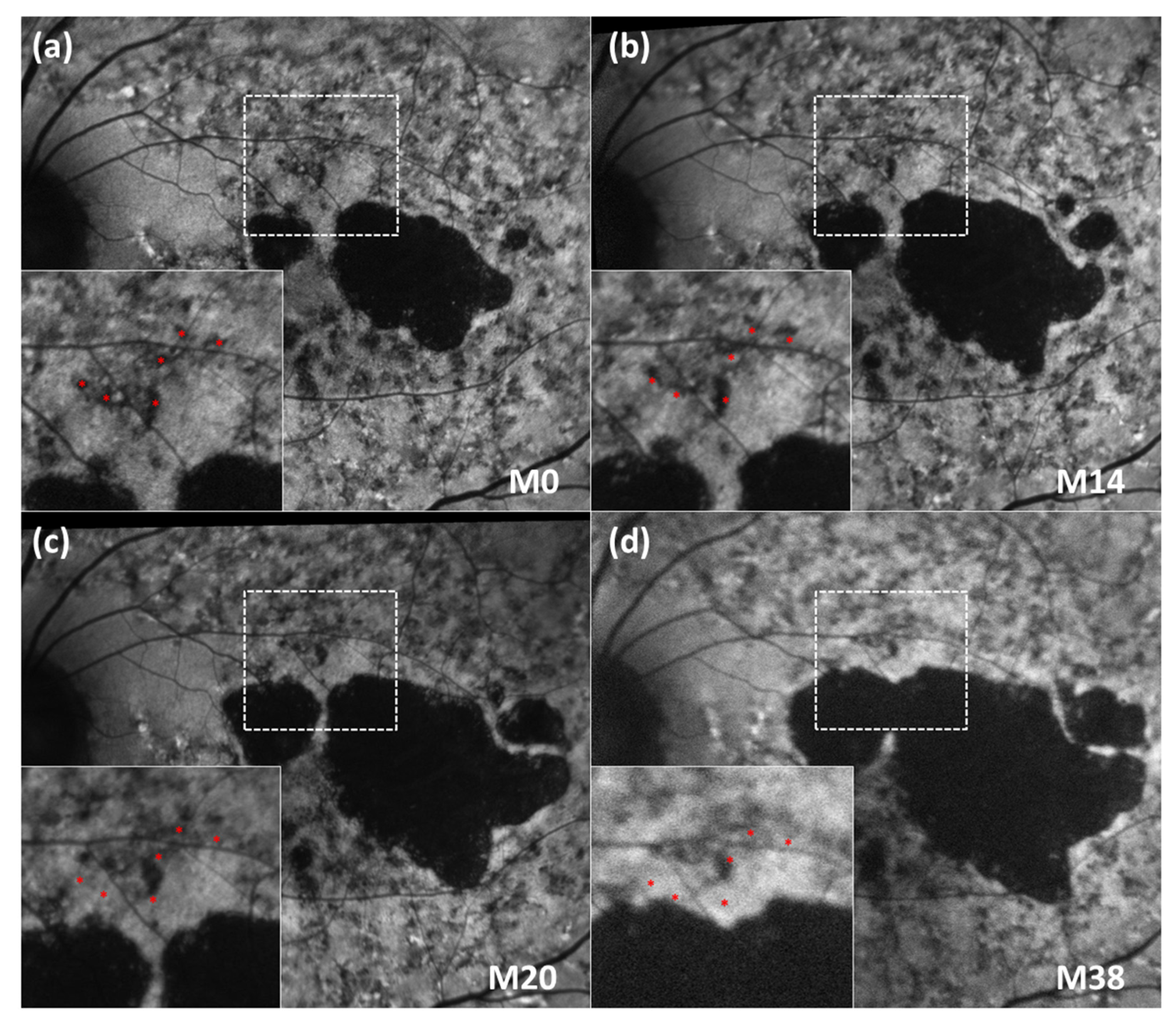
3.2. Movement of FRA in Patients with Heterogeneous Background
3.3. Centrifugal Movement Pattern of FRA
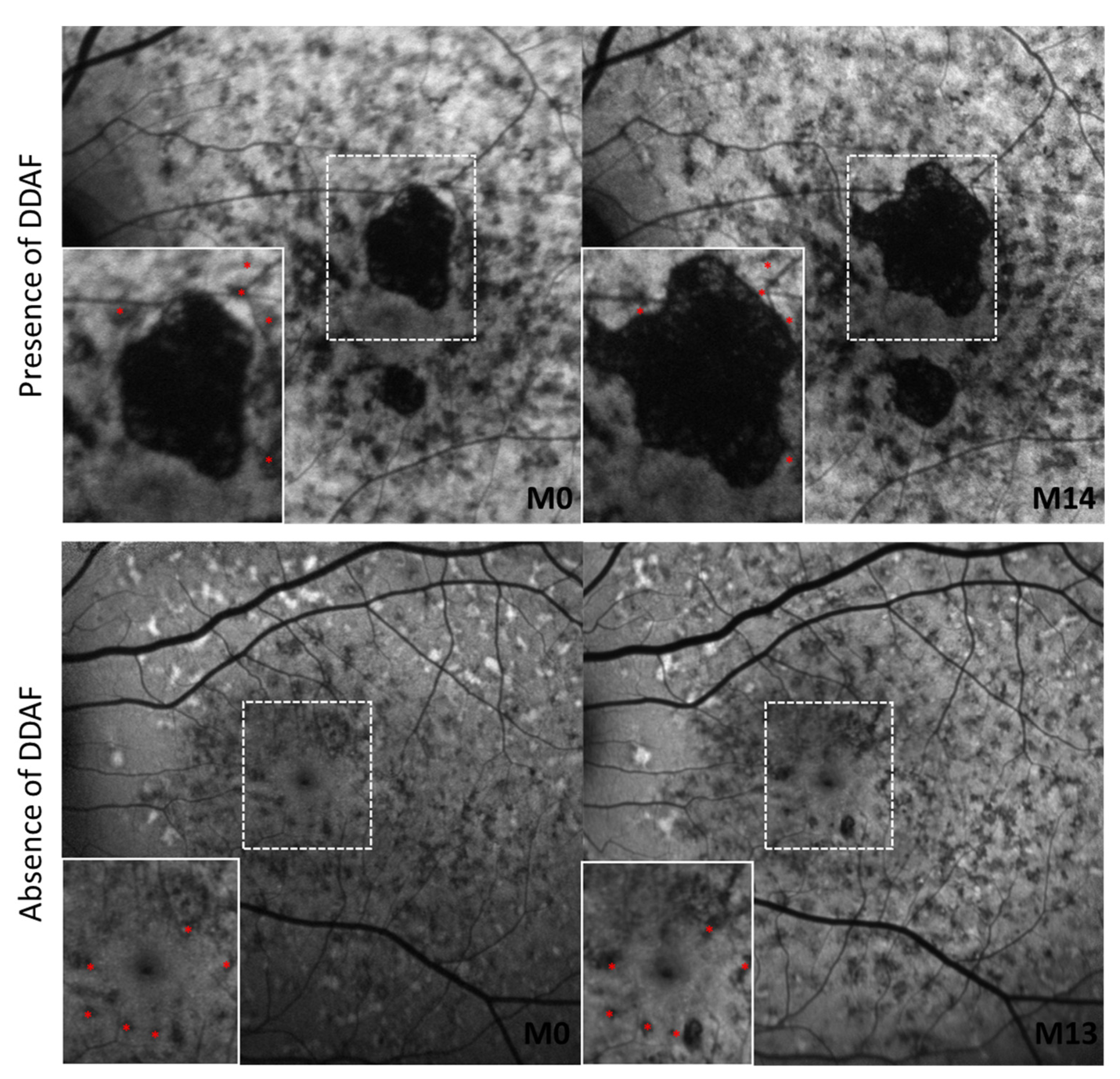
3.4. Influence of DDAF Areas on Displacement of FRA
3.5. Qualitative Analysis of SD-OCT Data at FRA
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blacharsky, P. Fundus flavimaculatus. In Retinal Dystrophies and Degenerations; Raven Press: New York, NY, USA, 1988; pp. 132–139. [Google Scholar]
- Allikmets, R.; Singh, N.; Sun, H.; Shroyer, N.F.; Hutchinson, A.; Chidambaram, A.; Gerrard, B.; Baird, L.; Stauffer, D.; Peiffer, A.; et al. A photoreceptor cell-specific ATP-binding transporter gene (ABCR) is mutated in recessive Stargardt macular dystrophy. Nat. Genet. 1997, 15, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Bither, P.P.; Berns, L.A. Stargardt’s disease: A review of the literature. J. Am. Optom. Assoc. 1988, 59, 106–111. [Google Scholar] [PubMed]
- Burke, T.R.; Duncker, T.; Woods, R.L.; Greenberg, J.P.; Zernant, J.; Tsang, S.H.; Smith, R.T.; Allikmets, R.; Sparrow, J.R.; Delori, F.C. Quantitative Fundus Autofluorescence in Recessive Stargardt Disease. Investig. Opthalmol. Vis. Sci. 2014, 55, 2841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparrow, J.R.; Gregory-Roberts, E.; Yamamoto, K.; Blonska, A.; Ghosh, S.K.; Ueda, K.; Zhou, J. The bisretinoids of retinal pigment epithelium. Prog. Retin. Eye Res. 2012, 31, 121–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piotter, E.; McClements, M.E.; MacLaren, R.E. Therapy Approaches for Stargardt Disease. Biomolecules 2021, 11, 1179. [Google Scholar] [CrossRef] [PubMed]
- Duarri, A.; Rodríguez-Bocanegra, E.; Martínez-Navarrete, G.; Biarnés, M.; García, M.; Ferraro, L.L.; Kuebler, B.; Aran, B.; Izquierdo, E.; Aguilera-Xiol, E.; et al. Transplantation of Human Induced Pluripotent Stem Cell-Derived Retinal Pigment Epithelium in a Swine Model of Geographic Atrophy. Int. J. Mol. Sci. 2021, 22, 10497. [Google Scholar] [CrossRef]
- Strauss, R.W.; Ho, A.; Muñoz, B.; Cideciyan, A.V.; Sahel, J.-A.; Sunness, J.S.; Birch, D.G.; Bernstein, P.S.; Michaelides, M.; Traboulsi, E.I.; et al. The Natural History of the Progression of Atrophy Secondary to Stargardt Disease (ProgStar) Studies. Ophthalmology 2016, 123, 817–828. [Google Scholar] [CrossRef]
- Strauss, R.W.; Muñoz, B.; Ho, A.; Jha, A.; Michaelides, M.; Cideciyan, A.V.; Audo, I.; Birch, D.G.; Hariri, A.H.; Nittala, M.G.; et al. Progression of Stargardt Disease as Determined by Fundus Autofluorescence in the Retrospective Progression of Stargardt Disease Study (ProgStar Report No. 9). JAMA Ophthalmol. 2017, 135, 1232. [Google Scholar] [CrossRef] [PubMed]
- Fujinami, K.; Lois, N.; Mukherjee, R.; McBain, V.A.; Tsunoda, K.; Tsubota, K.; Stone, E.M.; Fitzke, F.W.; Bunce, C.; Moore, A.T.; et al. A Longitudinal Study of Stargardt Disease: Quantitative Assessment of Fundus Autofluorescence, Progression, and Genotype Correlations. Investig. Opthalmol. Vis. Sci. 2013, 54, 8181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cukras, C.A.; Wong, W.T.; Caruso, R.; Cunningham, D.; Zein, W.; Sieving, P.A. Centrifugal expansion of fundus autofluorescence patterns in Stargardt disease over time. Arch. Ophthalmol. 2012, 130, 171–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparrow, J.R.; Marsiglia, M.; Allikmets, R.; Tsang, S.; Lee, W.; Duncker, T.; Zernant, J. Flecks in Recessive Stargardt Disease: Short-Wavelength Autofluorescence, Near-Infrared Autofluorescence, and Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5029–5039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strauss, R.W.; Muñoz, B.; Ho, A.; Jha, A.; Michaelides, M.; Mohand-Said, S.; Cideciyan, A.V.; Birch, D.; Hariri, A.H.; Nittala, M.G.; et al. Incidence of Atrophic Lesions in Stargardt Disease in the Progression of Atrophy Secondary to Stargardt Disease (ProgStar) Study: Report No. 5. JAMA Ophthalmol. 2017, 135, 687. [Google Scholar] [CrossRef] [PubMed]
- McBain, V.A.; Townend, J.; Lois, N. Progression of Retinal Pigment Epithelial Atrophy in Stargardt Disease. Am. J. Ophthalmol. 2012, 154, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Dhooge, P.P.A.; Runhart, E.H.; Lambertus, S.; Bax, N.M.; Groenewoud, J.M.M.; Klevering, B.J.; Hoyng, C.B. Correlation of Morphology and Function of Flecks Using Short-Wave Fundus Autofluorescence and Microperimetry in Patients with Stargardt Disease. Transl. Vis. Sci. Technol. 2021, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Lee, W.; de Carvalho, J.R.L.; Chang, S.; Tsang, S.H.; Allikmets, R.; Sparrow, J.R. Multi-platform imaging in ABCA4-Associated Disease. Sci. Rep. 2019, 9, 6436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiou, M.; Kane, T.; Tanna, P.; Bouzia, Z.; Singh, N.; Kalitzeos, A.; Strauss, R.W.; Fujinami, K.; Michaelides, M. Prospective Cohort Study of Childhood-Onset Stargardt Disease: Fundus Autofluorescence Imaging, Progression, Comparison with Adult-Onset Disease, and Disease Symmetry. Am. J. Ophthalmol. 2020, 211, 159–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charng, J.; Xiao, D.; Mehdizadeh, M.; Attia, M.S.; Arunachalam, S.; Lamey, T.M.; Thompson, J.A.; McLaren, T.L.; De Roach, J.N.; Mackey, D.A.; et al. Deep learning segmentation of hyperautofluorescent fleck lesions in Stargardt disease. Sci. Rep. 2020, 10, 16491. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.L.; Birtel, J.; Herrmann, P.; Holz, F.G.; Issa, P.C.; Gliem, M. Functional Relevance and Structural Correlates of Near Infrared and Short Wavelength Fundus Autofluorescence Imaging in ABCA4-Related Retinopathy. Transl. Vis. Sci. Technol. 2019, 8, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient # | Age (Years) | Sex | Duration of Symptoms (Years) | ABCA4 Mutations | BCVA | Follow-Up (Months) |
|---|---|---|---|---|---|---|
| 1 | 23 | F | 18 | p.Arg212Cys; c.4253 + 5G > A | 46 (20/125) | 14 |
| 2 | 47 | F | 2 | p.Trp700Leu; p.Leu1850Pro | 57 (20/80) | 30 |
| 3 | 34 | M | 1 | p.Pro1486Leu; p.Gly1977Ser | 90 (20/15) | 12 |
| 4 | 42 | F | 27 | p.Arg408X; p.Arg1129Leu | 35 (20/200) | 14 |
| 5 | 18 | F | 3 | p.Trp439 *; c.5714 + 5 G > A | 85 (20/20) | 13 |
| 6 | 36 | M | 2 | p.Trp700Leu; p.Leu1850Pro | 91 (20/15) | 12 |
| 7 | 45 | F | 25 | p.Arg212Cys; p.Gly1961Glu | 55 (20/80) | 12 |
| Patient # | DDAF | Median Rate of FRA Movement (µm/year) | ||||
|---|---|---|---|---|---|---|
| Zone 1 | Zone 2 | Zone 3 | Zone 4 | Zone 5 | ||
| 1 | Present | * | 128 | 101 | 50 | 13 |
| 2 | Present | * | * | 84 | 52 | 39 |
| 3 | Present | 5 | 83 | 17 | 14 | 1 |
| 4 | Present | * | * | * | 10 | 9 |
| 5 | Absent | 1 | 1 | 1 | 1 | 2 |
| 6 | Absent | 1 | 2 | 4 | 2 | 3 |
| 7 | Absent | 3 | 3 | † | † | † |
| Median (IQR) | +2.8 (3.5) | +3 (104) | +17 (90) | +12 (48.8) | +6 (17.8) | |
| Zone | DDAF Present (µm/year) | DDAF Absent (µm/year) | Present–Absent (95% CI) (µm/year) | p-Value |
|---|---|---|---|---|
| 1 | 27 | 2 | +25 (−1 to 52) | 0.05 |
| 2 | 77 | 2 | +75 (38 to 112) | < 0.001 |
| 3 | 67 | 1 | +66 (6 to 105) | 0.001 |
| 4 | 35 | 2 | +34 (−8 to 75) | 0.11 |
| 5 | 30 | 3 | +26 (−39 to 73) | 0.31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Bocanegra, E.; Biarnés, M.; Garcia, M.; Ferraro, L.L.; Fischer, M.D.; Monés, J. Kinetics of Heterogeneous Background in Stargardt’s Disease over Time. Life 2022, 12, 381. https://doi.org/10.3390/life12030381
Rodríguez-Bocanegra E, Biarnés M, Garcia M, Ferraro LL, Fischer MD, Monés J. Kinetics of Heterogeneous Background in Stargardt’s Disease over Time. Life. 2022; 12(3):381. https://doi.org/10.3390/life12030381
Chicago/Turabian StyleRodríguez-Bocanegra, Eduardo, Marc Biarnés, Míriam Garcia, Lucía Lee Ferraro, Manuel Dominik Fischer, and Jordi Monés. 2022. "Kinetics of Heterogeneous Background in Stargardt’s Disease over Time" Life 12, no. 3: 381. https://doi.org/10.3390/life12030381
APA StyleRodríguez-Bocanegra, E., Biarnés, M., Garcia, M., Ferraro, L. L., Fischer, M. D., & Monés, J. (2022). Kinetics of Heterogeneous Background in Stargardt’s Disease over Time. Life, 12(3), 381. https://doi.org/10.3390/life12030381