
Long-Chain Polyunsaturated Fatty Acid Status at Birth and Development of Childhood Allergy: A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Literature Search
2.3. Study Selection, Risk of Bias Assessment
2.4. Data Extraction and Synthesis
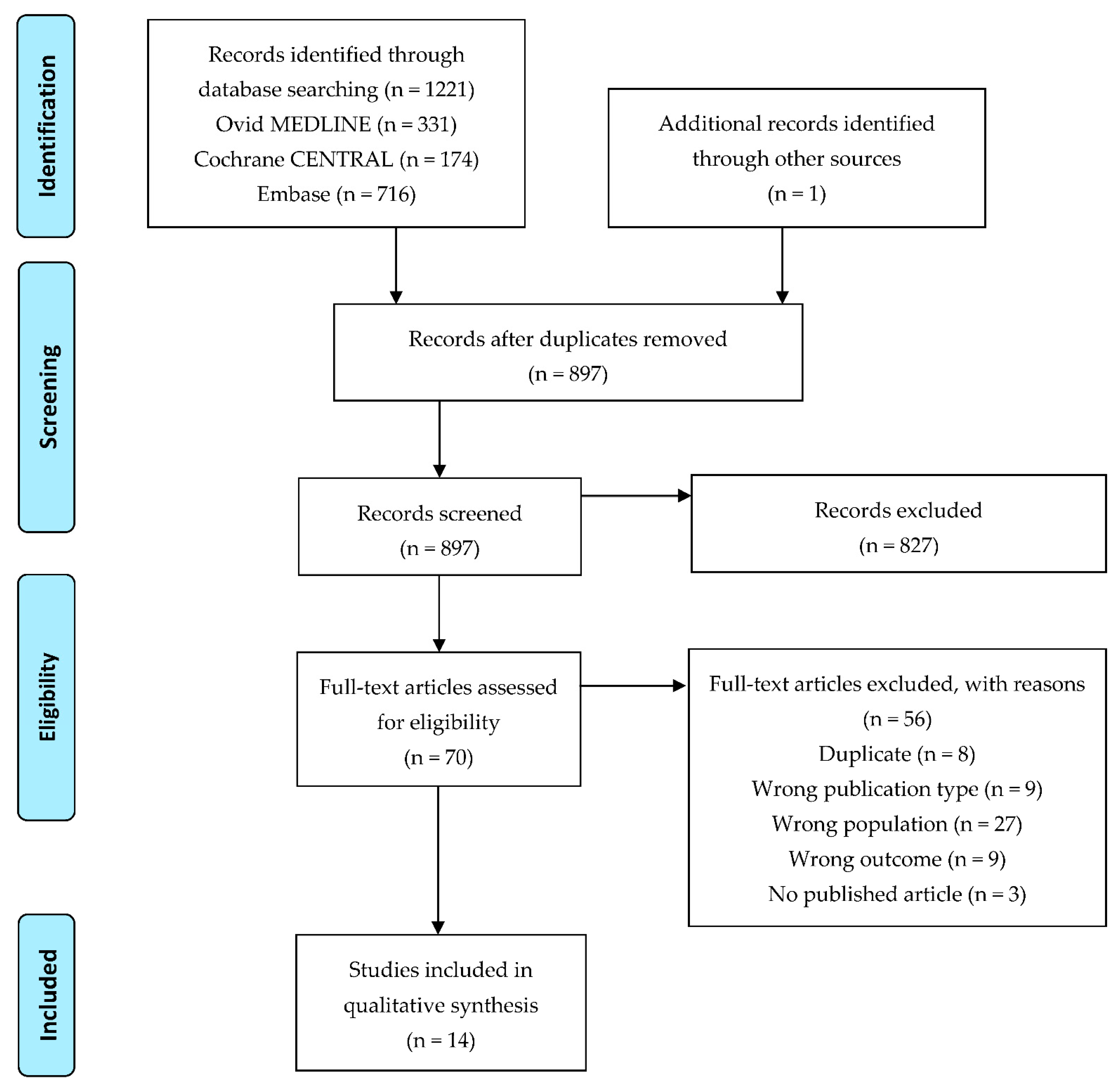
3. Results
3.1. Description of Included Studies

{kind=link}
| First Author, Year of Publication | Study Type | Place of Study | Subgroup of Infants | Type of Sample | Investigated Immune-Related Diseases/Factors |
|---|---|---|---|---|---|
| Barden AE, 2004 [75] | RCT | Subiaco, Australia | Maternal fish oil or olive oil supplementation during pregnancy | Cord blood RBC | Cord plasma F2-isoprostanes |
| Barman M, 2019 [81] | Birth cohort study | Sweden | Mothers living on a farm/not | Cord blood serum PL | Allergy at 18 and 36 months |
| Barman M, 2020 [82] | Birth cohort study | Sweden | Mothers living on a farm/not | Cord blood serum PL | Allergy at 1, 3, 5, and 8 years |
| Best KP, 2018 [76] | RCT | Australia | Maternal n-3 LCPUFA or placebo supplementation | Cord blood plasma PL | Allergic symptoms at 1, 3, and 6 years |
| Byberg K, 2008 [86] | Nested case-control study | Stavanger, Norway | Atopic/non-atopic | Cord blood plasma | Atopy, sCD23, and IgE at 3 years |
| Dirix CEH, 2009 [83] | Birth cohort study | Maastricht, The Netherlands | No | Cord blood plasma PL; umbilical artery and vein walls PL | Immune-related measurements at 7 years |
| Furuhjelm C, 2011 [77] | RCT | Sweden | Maternal n-3 LCPUFA or placebo supplementation | Cord blood plasma PL | Allergic symptoms up to 2 years |
| Galli E, 1994 [88] | Cohort study | Rome, Italy | Atopic/non-atopic | Cord blood serum PL | Atopy in the first 12 months |
| Montes R, 2013 [84] | Birth cohort study | Sabadell, Spain | Atopic/non-atopic | Cord blood plasma | Atopic eczema at 6 and 14 months |
| Mozurkewich EL, 2016 [78] | RCT | Michigan, USA | Maternal EPA/DHA/placebo supplementation | Cord blood plasma | Specialized pro-resolving mediators in cord plasma |
| Mozurkewich EL, 2018 [79] | RCT | Michigan, USA | Maternal EPA/DHA/placebo supplementation | Cord blood plasma | Cytokines in cord plasma |
| Newson RB, 2004 [85] | Birth cohort study | UK | No | Cord blood RBC PL | Wheezing and eczema at 18–30 and 30–42 months |
| See VHL, 2017 [80] | RCT | Subiaco, Australia | Maternal fish oil or olive oil supplementation during pregnancy | Cord blood RBC | Pro-resolving mediators at birth and 12 years |
| Yu G, 1996 [87] | Case-control study | Linköping, Sweden | Allergy: yes/no | Cord blood serum PL | Allergy during the first 6 years |
3.2. Fatty Acid Status at Birth and Development of Allergy in Childhood
3.3. Relationship of Fatty Acid Status at Birth to Odds Ratios and Relative Risks of Allergy in Children
3.4. Correlation between Fatty Acids and Allergy-Related Laboratory Parameters at Birth
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Janssen, C.I.; Kiliaan, A.J. Long-Chain Polyunsaturated Fatty Acids (LCPUFA) from genesis to senescence: The influence of LCPUFA on neural development, aging, and neurodegeneration. Prog. Lipid Res. 2014, 53, 1–17. [Google Scholar] [CrossRef]
- Crawford, M.A.; Hassam, A.G.; Williams, G. Essential fatty acids and fetal brain growth. Lancet 1976, 1, 452–453. [Google Scholar] [CrossRef]
- Middleton, P.; Gomersall, J.C.; Gould, J.F.; Shepherd, E.; Olsen, S.F.; Makrides, M. Omega-3 fatty acid addition during pregnancy. Cochrane Database Syst. Rev. 2018, 11, CD003402. [Google Scholar] [CrossRef]
- Shek, L.P.; Chong, M.F.; Lim, J.Y.; Soh, S.E.; Chong, Y.S. Role of dietary long-chain polyunsaturated fatty acids in infant allergies and respiratory diseases. Clin. Dev. Immunol. 2012, 2012, 730568. [Google Scholar] [CrossRef] [Green Version]
- Hwang, I.; Cha, A.; Lee, H.; Yoon, H.; Yoon, T.; Cho, B.; Lee, S.; Park, Y. N-3 polyunsaturated fatty acids and atopy in Korean preschoolers. Lipids 2007, 42, 345–349. [Google Scholar] [CrossRef]
- Adams, S.; Lopata, A.L.; Smuts, C.M.; Baatjies, R.; Jeebhay, M.F. Relationship between serum omega-3 fatty acid and asthma endpoints. Int. J. Environ. Res. Public Health 2018, 16, 43. [Google Scholar] [CrossRef] [Green Version]
- Jaudszus, A.; Gruen, M.; Watzl, B.; Ness, C.; Roth, A.; Lochner, A.; Barz, D.; Gabriel, H.; Rothe, M.; Jahreis, G. Evaluation of suppressive and pro-resolving effects of EPA and DHA in human primary monocytes and T-helper cells. J. Lipid Res. 2013, 54, 923–935. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Choi, Y.R.; Kim, M.; Park, J.M.; Kang, M.; Oh, J.; Lee, C.J.; Park, S.; Kang, S.M.; Manabe, I.; et al. Common and differential effects of docosahexaenoic acid and eicosapentaenoic acid on helper T-cell responses and associated pathways. BMB Rep. 2021, 54, 278–283. [Google Scholar] [CrossRef]
- Prescott, S.L.; Dunstan, J.A. Prenatal fatty acid status and immune development: The pathways and the evidence. Lipids 2007, 42, 801–810. [Google Scholar] [CrossRef]
- Bruschi, M.; Santucci, L.; Petretto, A.; Bartolocci, M.; Marchisio, M.; Ghiggeri, G.M.; Verrina, E.; Ramenghi, L.A.; Panfoli, I.; Candiano, G. Association between maternal omega-3 polyunsaturated fatty acids supplementation and preterm delivery: A proteomic study. FASEB J. 2020, 34, 6322–6334. [Google Scholar] [CrossRef] [Green Version]
- Trebble, T.M.; Wootton, S.A.; Miles, E.A.; Mullee, M.; Arden, N.K.; Ballinger, A.B.; Stroud, M.A.; Burdge, G.C.; Calder, P.C. Prostaglandin E2 production and T cell function after fish-oil supplementation: Response to antioxidant cosupplementation. Am. J. Clin. Nutr. 2003, 78, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles, E.A.; Childs, C.E.; Calder, P.C. Long-Chain Polyunsaturated Fatty Acids (LCPUFAs) and the developing immune system: A narrative review. Nutrients 2021, 13, 247. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement. Syst Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Littlewood, A.; Marshall, C.; Metzendorf, M.-I.; Noel-Storr, A.; Rader, T.; Shokraneh, F.; Thomas, J.; et al. Chapter 4: Searching for and selecting studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., Welch, V., Eds.; Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 27 January 2022).
- Byron, C.W.; Small, K.; Brodley, C.E.; Lau, J.; Trikalinos, T.A. Deploying an interactive machine learning system in an evidence-based practice center: Abstrackr. In Proceedings of the IHI ‘12: ACM International Health Informatics Symposium, Miami, FL, USA, 28–30 January 2012; pp. 819–824. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Chase, P.; Boulware, D.; Krischer, J.; Rodriguez, H.; Donaldson, D.; Chritton, S.; Muller, S.; Clare-Salzler, M. Inflammatory cytokines in the pre-autoimmune phase of type 1 diabetes. Diabetes 2010, 59, A502. [Google Scholar]
- Scalabrin, D.; Mitmesser, S.; Birch, E.; Khoury, J.; Bean, J.; Harris, C.; Berseth, C. Lower incidence and less recurrence of allergic manifestations is observed in children who received docosahexaenoic acid/arachidonic acid in infancy via breast milk or supplemented formula. Allergy 2011, 66, 711. [Google Scholar] [CrossRef]
- Nct. Nutritional Intervention to Prevent Diabetes. 2006. Available online: https://clinicaltrials.gov/show/NCT00333554 (accessed on 27 January 2022).
- Mozurkewich, E.L.; Clinton, C.M.; Romero, V.C.; Berman, D.R.; Barks, J.; Djuric, Z.; Dalli, J.; Serhan, C.N. Omega-3 fatty acid-derived pro-resolving lipid mediators in the human fetus: An exploratory secondary analysis of the mothers, omega-3, & mental health study. Reprod. Sci. 2013, 20, 297A. [Google Scholar]
- Mozurkewich, E.L.; Clinton, C.M.; Romero, V.C.; Tyner, J.; Brown, S.; Williams, J.Z.; Schrader, R.; Djuric, Z. Prenatal omega-3 fatty acid supplementation reduces pro-inflammatory cytokine production in umbilical cord blood: A secondary analysis of the mothers, omega-3, & mental health study. Reprod. Sci. 2013, 20, 248A. [Google Scholar]
- Barman, M.; Nilsson, S.; Torinsson Naluai, A.; Sandin, A.; Wold, A.; Sandberg, A.S. Single nucleotide polymorphisms in fatty acid desaturases is associated with cord blood long chain PUFA proportions and development of allergy. Allergy 2015, 70, 402. [Google Scholar] [CrossRef] [Green Version]
- Chase, P.; Boulware, D.; Krischer, J.; Daniels, M.; Nathan, B.; Chritton, S.; Muller, S.; Clare-Salzler, M. Vitamin D and inflammatory cytokine levels in infants at high genetic risk for type 1 diabetes. Diabetes 2010, 59, A467. [Google Scholar]
- Calder, P.C. Early life programming of immune and lung function: Can we now exclude a role of arachidonic acid exposure? Br. J. Nutr. 2009, 102, 331–333. [Google Scholar] [CrossRef] [Green Version]
- Ciaccio, C.E.; Girdhar, M. Effect of maternal ω3 fatty acid supplementation on infant allergy. Ann. Allergy Asthma Immunol. 2014, 112, 191–194. [Google Scholar] [CrossRef] [Green Version]
- Gomez, R.; Romero, R.; Edwin, S.S.; David, C. Pathogenesis of preterm labor and preterm premature rupture of membranes associated with intraamniotic infection. Infect. Dis. Clin. North. Am. 1997, 11, 135–176. [Google Scholar] [CrossRef]
- Calder, P.C. Polyunsaturated fatty acids and cytokine profiles: A clue to the changing prevalence of atopy? Clin. Exp. Allergy 2003, 33, 412–415. [Google Scholar] [CrossRef]
- Guesry, P. The role of nutrition in brain development. Prev. Med. 1998, 27, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Loppi, M.; Businco, L.; Arcese, G.; Ziruolo, G.; Nisini, R. Cord blood mononuclear leukocytes of neonates at risk of atopy have a deficiency of arachidonic acid. J. Investig. Allergol. Clin. Immunol. 1994, 4, 272–276. [Google Scholar]
- Gold, D.R.; Willwerth, B.M.; Tantisira, K.G.; Finn, P.W.; Schaub, B.; Perkins, D.L.; Tzianabos, A.; Ly, N.P.; Schroeter, C.; Gibbons, F.; et al. Associations of cord blood fatty acids with lymphocyte proliferation, IL-13, and IFN-gamma. J. Allergy Clin. Immunol. 2006, 117, 931–938. [Google Scholar] [CrossRef] [Green Version]
- Dunstan, J.A.; Mori, T.A.; Barden, A.; Beilin, L.J.; Taylor, A.L.; Holt, P.G.; Prescott, S.L. Fish oil supplementation in pregnancy modifies neonatal allergen-specific immune responses and clinical outcomes in infants at high risk of atopy: A randomized, controlled trial. J. Allergy Clin. Immunol. 2003, 112, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Espiritu, M.M.; Lin, H.; Foley, E.; Tsang, V.; Rhee, E.; Perlman, J.; Cunningham-Rundles, S. Omega-3 fatty acids modulate neonatal cytokine response to endotoxin. J. Perinat. Med. 2016, 44, 711–721. [Google Scholar] [CrossRef] [PubMed]
- See, V.H.L.; Mas, E.; Prescott, S.L.; Beilin, L.J.; Burrows, S.; Barden, A.E.; Huang, R.C.; Mori, T.A. Effects of postnatal omega-3 fatty acid supplementation on offspring pro-resolving mediators of inflammation at 6 months and 5 years of age: A double blind, randomized controlled clinical trial. Prostaglandins Leukot Essent Fat. Acids 2017, 126, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Nct. Assessment of Arachidonic Acid Supplementation in Infant Formula on the Immune Response of Infants. 2014. Available online: https://clinicaltrials.gov/show/NCT02092857 (accessed on 27 January 2022).
- D’Vaz, N.; Amarasekera, M.; Dunstan, J.; Meldrum, S.; Lee-Pullen, T.; Metcalfe, J.; Holt, B.; Serralha, M.; Tulic, M.; Mori, T.; et al. Basic and clinical immunology-3020. Fish oil supplementation in early infancy modulates developing infant immune responses but not clinical allergy. World Allergy Organ. J. 2013, 6, P196. [Google Scholar] [CrossRef] [Green Version]
- Lucas, A.; Stafford, M.; Morley, R.; Abbott, R.; Stephenson, T.; MacFadyen, U.; Elias-Jones, A.; Clements, H. Efficacy and safety of long-chain polyunsaturated fatty acid supplementation of infant-formula milk: A randomised trial. Lancet 1999, 354, 1948–1954. [Google Scholar] [CrossRef]
- D’Vaz, N.; Meldrum, S.J.; Dunstan, J.A.; Lee-Pullen, T.F.; Metcalfe, J.; Holt, B.J.; Serralha, M.; Tulic, M.K.; Mori, T.A.; Prescott, S.L. Fish oil supplementation in early infancy modulates developing infant immune responses. Clin. Exp. Allergy 2012, 42, 1206–1216. [Google Scholar] [CrossRef]
- Foiles, A.M.; Kerling, E.H.; Wick, J.A.; Scalabrin, D.M.F.; Colombo, J.; Carlson, S.E. Formula with long-chain polyunsaturated fatty acids reduces incidence of allergy in early childhood. Pediatr. Allergy Immunol. 2016, 27, 156–161. [Google Scholar] [CrossRef] [Green Version]
- Scalabrin, D.M.; Birch, E.E.; Khoury, J.C.; Bean, J.; Harris, C.L.; Mitmesser, S.H.; Berseth, C.L. Impact of early nutrition on incidence of allergic manifestations in the first 3 years of life. J. Allergy Clin. Immunol. 2011, 127, AB33. [Google Scholar] [CrossRef]
- Lapillonne, A.; Pastor, N.; Zhuang, W.; Scalabrin, D.M.F. Infants fed formula with added long chain polyunsaturated fatty acids have reduced incidence of respiratory illnesses and diarrhea during the first year of life. BMC Pediatrics 2014, 14, 168. [Google Scholar] [CrossRef] [Green Version]
- Miklavcic, J.J.; Larsen, B.M.K.; Mazurak, V.C.; Scalabrin, D.M.F.; MacDonald, I.M.; Shoemaker, G.K.; Casey, L.; Van Aerde, J.E.; Clandinin, M.T. Reduction of arachidonate is associated with increase in B-cell activation marker in infants: A randomized trial. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 446–453. [Google Scholar] [CrossRef]
- Gibson, R.A.; Barclay, D.; Marshall, H.; Moulin, J.; Maire, J.C.; Makrides, M. Safety of supplementing infant formula with long-chain polyunsaturated fatty acids and Bifidobacterium lactis in term infants: A randomised controlled trial. Br. J. Nutr. 2009, 101, 1706–1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meldrum, S.J.; D’Vaz, N.; Dunstan, J.; Mori, T.A.; Prescott, S.L. The Infant Fish Oil Supplementation Study (IFOS): Design and research protocol of a double-blind, randomised controlled n-3 LCPUFA intervention trial in term infants. Contemp. Clin. Trials 2011, 32, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Field, C.J.; Van Aerde, J.E.; Goruk, S.; Clandinin, M.T. Effect of feeding a formula supplemented with long-chain polyunsaturated fatty acids for 14 weeks improves the ex vivo response to a mitogen and reduces the response to a soy protein in infants at low risk for allergy. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, K.; Hoppu, U.; Hämäläinen, M.; Linderborg, K.; Moilanen, E.; Isolauri, E. Breast milk fatty acids may link innate and adaptive immune regulation: Analysis of soluble CD14, prostaglandin E2, and fatty acids. Pediatr. Res. 2006, 59, 723–727. [Google Scholar] [CrossRef] [Green Version]
- Granot, E.; Golan, D.; Berry, E.M. Breast-fed and formula-fed infants do not differ in immunocompetent cell cytokine production despite differences in cell membrane fatty acid composition. Am. J. Clin. Nutr. 2000, 72, 1202–1205. [Google Scholar] [CrossRef] [Green Version]
- Lumia, M.; Luukkainen, P.; Takkinen, H.M.; Kaila, M.; Nwaru, B.I.; Nevalainen, J.; Salminen, I.; Uusitalo, L.; Niinistö, S.; Tuokkola, J.; et al. Cow’s milk allergy and the association between fatty acids and childhood asthma risk. J. Allergy Clin. Immunol. 2014, 134, 488–490. [Google Scholar] [CrossRef]
- Van Gool, C.J.A.W.; Thijs, C.; Dagnelie, P.C.; Henquet, C.J.M.; Van Houwelingen, A.C.; Schrander, J.; Menheere, P.P.C.A.; Van Den Brandt, P.A. Determinants of neonatal IgE level: Parity, maternal age, birth season and perinatal essential fatty acid status in infants of atopic mothers. Allergy 2004, 59, 961–968. [Google Scholar] [CrossRef] [Green Version]
- Granot, E.; Jakobovich, E.; Rabinowitz, R.; Levy, P.; Schlesinger, M. DHA supplementation during pregnancy and lactation affects infants’ cellular but not humoral immune response. Mediat. Inflamm. 2011, 2011, 493925. [Google Scholar] [CrossRef] [Green Version]
- Chase, H.P.; Boulware, D.; Rodriguez, H.; Donaldson, D.; Chritton, S.; Rafkin-Mervis, L.; Krischer, J.; Skyler, J.S.; Clare-Salzler, M.; Lescheck, E.; et al. Effect of docosahexaenoic acid supplementation on inflammatory cytokine levels in infants at high genetic risk for type 1 diabetes. Pediatr. Diabetes 2015, 16, 271–279. [Google Scholar] [CrossRef] [Green Version]
- Argaw, A.; Wondafrash, M.; Bouckaert, K.P.; Kolsteren, P.; Lachat, C.; Belachew, T.; De Meulenaer, B.; Huybregts, L. Effects of n-3 long-chain PUFA supplementation to lactating mothers and their breastfed children on child growth and morbidity: A 2 × 2 factorial randomized controlled trial in rural Ethiopia. Am. J. Clin. Nutr. 2018, 107, 454–464. [Google Scholar] [CrossRef]
- Niinistö, S.; Takkinen, H.M.; Erlund, I.; Ahonen, S.; Toppari, J.; Ilonen, J.; Veijola, R.; Knip, M.; Vaarala, O.; Virtanen, S.M. Fatty acid status in infancy is associated with the risk of type 1 diabetes-associated autoimmunity. Diabetologia 2017, 60, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Ellul, S.; Marx, W.; Collier, F.; Saffery, R.; Tang, M.; Burgner, D.; Carlin, J.; Vuillermin, P.; Ponsonby, A.L. Plasma metabolomic profiles associated with infant food allergy with further consideration of other early life factors. Prostaglandins Leukot. Essent. Fat. Acids 2020, 159, 102099. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, K.; Barman, M.; Moberg, S.; Sjöberg, A.; Brekke, H.K.; Hesselmar, B.; Sandberg, A.S.; Wold, A.E. Serum fatty acids in infants, reflecting family fish consumption, were inversely associated with allergy development but not related to farm residence. Acta Paediatr. 2016, 105, 1462–1471. [Google Scholar] [CrossRef] [PubMed]
- Keelan, J.A.; Mas, E.; D’Vaz, N.; Dunstan, J.A.; Li, S.; Barden, A.E.; Mark, P.J.; Waddell, B.J.; Prescott, S.L.; Mori, T.A. Effects of maternal n-3 fatty acid supplementation on placental cytokines, pro-resolving lipid mediators and their precursors. Reproduction 2015, 149, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Furuhjelm, C.; Warstedt, K.; Larsson, J.; Fredriksson, M.; Böttcher, M.F.; Fälth-Magnusson, K.; Duchén, K. Fish oil supplementation in pregnancy and lactation may decrease the risk of infant allergy. Acta Paediatr. 2009, 98, 1461–1467. [Google Scholar] [CrossRef]
- Palmer, D.J.; Sullivan, T.; Gold, M.S.; Prescott, S.L.; Heddle, R.; Gibson, R.A.; Makrides, M. Randomized controlled trial of fish oil supplementation in pregnancy on childhood allergies. Allergy 2013, 68, 1370–1376. [Google Scholar] [CrossRef]
- Nct. DHA-1 for Lactating Mothers. 2012. Available online: https://clinicaltrials.gov/show/NCT01732874 (accessed on 28 January 2022).
- Kankaanpaa, P.; Nurmela, K.; Erkkila, A.; Kalliomaki, M.; Holmberg-Marttila, D.; Salminen, S.; Isolauri, E. Polyunsaturated fatty acids in maternal diet, breast milk, and serum lipid fatty acids of infants in relation to atopy. Allergy 2001, 56, 633–638. [Google Scholar] [CrossRef] [Green Version]
- Beck, M.; Zelczak, G.; Lentze, M.J. Abnormal fatty acid composition in umbilical cord blood of infants at high risk of atopic disease. Acta Paediatr. 2000, 89, 279–284. [Google Scholar] [CrossRef]
- Moodley, T.; Vella, C.; Djahanbakhch, O.; Branford-White, C.J.; Crawford, M.A. Arachidonic and docosahexaenoic acid deficits in Preterm neonatal mononuclear cell membranes. Implications for the immune response at birth. Nutr. Health 2009, 20, 167–185. [Google Scholar] [CrossRef]
- Yu, G.; Björkstén, B. Serum levels of phospholipid fatty acids in mothers and their babies in relation to allergic disease. Eur. J. Pediatr. 1998, 157, 298–303. [Google Scholar] [CrossRef]
- Barman, M.; Nilsson, S.; Naluai, Å.T.; Sandin, A.; Wold, A.E.; Sandberg, A.S. Single nucleotide polymorphisms in the FADS gene cluster but not the ELOVL2 gene are associated with serum polyunsaturated fatty acid composition and development of allergy (in a Swedish birth cohort). Nutrients 2015, 7, 10100–10115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuhjelm, C.; Jenmalm, M.C.; Fälth-Magnusson, K.; DuchIn, K. Th1 and Th2 chemokines, vaccine-induced immunity, and allergic disease in infants after maternal ω-3 fatty acid supplementation during pregnancy and lactation. Pediatr. Res. 2011, 69, 259–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krauss-Etschmann, S.; Hartl, D.; Rzehak, P.; Heinrich, J.; Shadid, R.; del Carmen Ramírez-Tortosa, M.; Campoy, C.; Pardillo, S.; Schendel, D.J.; Decsi, T.; et al. Decreased cord blood IL-4, IL-13, and CCR4 and increased TGF-β levels after fish oil supplementation of pregnant women. J. Allergy Clin. Immunol. 2008, 121, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Romero, V.C.; Somers, E.C.; Stolberg, V.; Clinton, C.; Chensue, S.; Djuric, Z.; Berman, D.R.; Treadwell, M.C.; Vahratian, A.M.; Mozurkewich, E. Developmental programming for allergy: A secondary analysis of the mothers, Omega-3, and mental health study. Am. J. Obstet. Gynecol. 2013, 208, e311–e316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, D.J.; Sullivan, T.; Gold, M.S.; Prescott, S.L.; Heddle, R.; Gibson, R.A.; Makrides, M. Effect of n-3 long chain polyunsaturated fatty acid supplementation in pregnancy on infants’ allergies in first year of life: Randomised controlled trial. BMJ 2012, 344, e184. [Google Scholar] [CrossRef] [Green Version]
- Harris, C.; Demmelmair, H.; Von Berg, A.; Lehmann, I.; Flexeder, C.; Koletzko, B.; Heinrich, J.; Standl, M. Associations between fatty acids and low-grade inflammation in children from the LISAplus birth cohort study. Eur. J. Clin. Nutr. 2017, 71, 1303–1311. [Google Scholar] [CrossRef] [Green Version]
- Chuang, S.L.; Wang, Y.; Demertzi, E.; Willetts, S.; Talbot, I.; Johnson, M.; Pantelidis, P.; Crawford, M.; Ogundipe, E. Fatty acid profiles in pregnancy and cord blood related to meconium microbiota. J. Matern. Fetal Neonatal. Med. 2014, 27, 331. [Google Scholar] [CrossRef]
- Balogun, K.; Balmert, L.; Jao, J.; Sun, S.; Bazinet, R.; Serghides, L. Maternal and cord plasma bioactive eicosanoid profiles differ in HIV+ and HIV−women. Top Antivir. Med. 2020, 28, 295–296. [Google Scholar]
- Nct. Docosahexaenoic Acid (DHA) Supplementation in High Risk Pregnancies. 2019. Available online: https://clinicaltrials.gov/show/NCT04069195 (accessed on 28 January 2022).
- Barden, A.E.; Mori, T.A.; Dunstan, J.A.; Taylor, A.L.; Thornton, A.; Croft, K.D.; Beilin, L.J.; Prescott, S.L. Fish oil supplementation in pregnancy lowers F2-isoprostanes in neonates at high risk of atopy. Free Radic. Res. 2004, 38, 233–239. [Google Scholar] [CrossRef]
- Best, K.P.; Sullivan, T.R.; Palmer, D.J.; Gold, M.; Martin, J.; Kennedy, D.; Makrides, M. Prenatal omega-3 LCPUFA and symptoms of allergic disease and sensitization throughout early childhood—A longitudinal analysis of long-term follow-up of a randomized controlled trial. World Allergy Organ J. 2018, 11, 10. [Google Scholar] [CrossRef]
- Furuhjelm, C.; Warstedt, K.; Fagerås, M.; Fälth-Magnusson, K.; Larsson, J.; Fredriksson, M.; Duchén, K. Allergic disease in infants up to 2 years of age in relation to plasma omega-3 fatty acids and maternal fish oil supplementation in pregnancy and lactation. Pediatr. Allergy Immunol. 2011, 22, 505–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozurkewich, E.L.; Greenwood, M.; Clinton, C.; Berman, D.; Romero, V.; Djuric, Z.; Qualls, C.; Gronert, K. Pathway markers for pro-resolving lipid mediators in maternal and umbilical cord blood: A secondary analysis of the mothers, Omega-3, and mental health study. Front. Pharmacol. 2016, 7, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozurkewich, E.L.; Berman, D.R.; Vahratian, A.; Clinton, C.M.; Romero, V.C.; Chilimigras, J.L.; Vazquez, D.; Qualls, C.; Djuric, Z. Effect of prenatal EPA and DHA on maternal and umbilical cord blood cytokines. BMC Pregnancy Childbirth 2018, 18, 261. [Google Scholar] [CrossRef] [PubMed]
- See, V.H.L.; Mas, E.; Prescott, S.L.; Beilin, L.J.; Burrows, S.; Barden, A.E.; Huang, R.C.; Mori, T.A. Effects of prenatal n-3 fatty acid supplementation on offspring resolvins at birth and 12 years of age: A double-blind, randomised controlled clinical trial. Br. J. Nutr. 2017, 118, 971–980. [Google Scholar] [CrossRef] [Green Version]
- Barman, M.; Jonsson, K.; Wold, A.E.; Sandberg, A.S. Exposure to a farm environment during pregnancy increases the proportion of arachidonic acid in the cord sera of offspring. Nutrients 2019, 11, 238. [Google Scholar] [CrossRef] [Green Version]
- Barman, M.; Rabe, H.; Hesselmar, B.; Johansen, S.; Sandberg, A.S.; Wold, A.E. Cord blood levels of epa, a marker of fish intake, correlate with infants’ T-and B-lymphocyte phenotypes and risk for allergic disease. Nutrients 2020, 12, 3000. [Google Scholar] [CrossRef]
- Dirix, C.E.H.; Hogervorst, J.G.F.; Rump, P.; Hendriks, J.J.E.; Bruins, M.; Hornstra, G. Prenatal arachidonic acid exposure and selected immune-related variables in childhood. Br. J. Nutr. 2009, 102, 387–397. [Google Scholar] [CrossRef] [Green Version]
- Montes, R.; Chisaguano, A.M.; Castellote, A.I.; Morales, E.; Sunyer, J.; López-Sabater, M.C. Fatty-acid composition of maternal and umbilical cord plasma and early childhood atopic eczema in a Spanish cohort. Eur. J. Clin. Nutr. 2013, 67, 658–663. [Google Scholar] [CrossRef]
- Newson, R.B.; Shaheen, S.O.; Henderson, A.J.; Emmett, P.M.; Sherriff, A.; Calder, P.C. Umbilical cord and maternal blood red cell fatty acids and early childhood wheezing and eczema. J. Allergy Clin. Immunol. 2004, 114, 531–537. [Google Scholar] [CrossRef]
- Byberg, K.; Øymar, K.; Aksnes, L. Fatty acids in cord blood plasma, the relation to soluble CD23 and subsequent atopy. Prostaglandins Leukot Essent Fat. Acids 2008, 78, 61–65. [Google Scholar] [CrossRef]
- Yu, G.; Kjellman, N.I.M.; Björkstén, B. Phospholipid fatty acids in cord blood: Family history and development of allergy. Acta Paediatr. 1996, 85, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Galli, E.; Picardo, M.; Chini, L.; Passi, S.; Moschese, V.; Terminali, O.; Paone, F.; Fraioli, G.; Rossi, P. Analysis of polyunsaturated fatty acids in newborn sera: A screening tool for atopic disease? Br. J. Dermatol. 1994, 130, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Jasani, B.; Simmer, K.; Patole, S.K.; Rao, S.C. Long chain polyunsaturated fatty acid supplementation in infants born at term. Cochrane Database Syst. Rev. 2017, 3, CD000376. [Google Scholar] [CrossRef] [PubMed]
- Bahreynian, M.; Feizi, A.; Kelishadi, R. Is fatty acid composition of breast milk different in various populations? A systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2020, 71, 909–920. [Google Scholar] [CrossRef] [PubMed]
- Commission Delegated Regulation (EU) 2016/127 of 25 September 2015 Supplementing Regulation (EU) No 609/2013 of the European Parliament and of the Council as Regards the Specific Compositional and Information Requirements for Infant Formula and Follow-on Formula and as Regards Requirements on Information Relating to Infant and Young Child Feeding. Available online: http://data.europa.eu/eli/reg_del/2016/127/2021-07-15 (accessed on 1 February 2022).
- Koletzko, B.; Bergmann, K.; Brenna, J.T.; Calder, P.C.; Campoy, C.; Clandinin, M.T.; Colombo, J.; Daly, M.; Decsi, T.; Demmelmair, H.; et al. Should formula for infants provide arachidonic acid along with DHA? A position paper of the European Academy of Paediatrics and the Child Health Foundation. Am. J. Clin. Nutr. 2020, 111, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Tounian, P.; Bellaiche, M.; Legrand, P. ARA or no ARA in infant formulae, that is the question. Arch. Pediatr. 2021, 28, 69–74. [Google Scholar] [CrossRef]
- Barden, A.E.; Mas, E.; Mori, T.A. n-3 Fatty acid supplementation and proresolving mediators of inflammation. Curr. Opin. Lipidol. 2016, 27, 26–32. [Google Scholar] [CrossRef]
- Hogenkamp, A.; Ehlers, A.; Garssen, J.; Willemsen, L.E.M. Allergy modulation by N-3 long chain polyunsaturated fatty acids and fat soluble nutrients of the Mediterranean diet. Front. Pharmacol. 2020, 11, 1244. [Google Scholar] [CrossRef]
- Ranade, P.S.; Rao, S.S. Maternal long-chain PUFA supplementation during protein deficiency improves brain fatty acid accretion in rat pups by altering the milk fatty acid composition of the dam. J. Nutr. Sci. 2013, 2, e5. [Google Scholar] [CrossRef] [Green Version]
- Wohlford, E.M.; Huang, P.F.; Elhawary, J.R.; Millette, L.A.; Contreras, M.G.; Witonsky, J.; Holweg, C.T.J.; Oh, S.S.; Lee, C.; Merenda, C.; et al. Racial/ethnic differences in eligibility for asthma biologics among pediatric populations. J. Allergy Clin. Immunol. 2021, 148, 1324–1331. [Google Scholar] [CrossRef]
- Allaire, J.; Couture, P.; Leclerc, M.; Charest, A.; Marin, J.; Lepine, M.C.; Talbot, D.; Tchernof, A.; Lamarche, B. A randomized, crossover, head-to-head comparison of eicosapentaenoic acid and docosahexaenoic acid supplementation to reduce inflammation markers in men and women: The Comparing EPA to DHA (ComparED) Study. Am. J. Clin. Nutr. 2016, 104, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Huang, T.; Zheng, J.; Wu, K.; Li, D. Effect of marine-derived n-3 polyunsaturated fatty acids on C-reactive protein, interleukin 6 and tumor necrosis factor alpha: A meta-analysis. PLoS ONE 2014, 9, e88103. [Google Scholar] [CrossRef] [Green Version]
- Vors, C.; Allaire, J.; Marin, J.; Lepine, M.C.; Charest, A.; Tchernof, A.; Couture, P.; Lamarche, B. Inflammatory gene expression in whole blood cells after EPA vs. DHA supplementation: Results from the ComparED study. Atherosclerosis 2017, 257, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Asztalos, I.B.; Gleason, J.A.; Sever, S.; Gedik, R.; Asztalos, B.F.; Horvath, K.V.; Dansinger, M.L.; Lamon-Fava, S.; Schaefer, E.J. Effects of eicosapentaenoic acid and docosahexaenoic acid on cardiovascular disease risk factors: A randomized clinical trial. Metabolism 2016, 65, 1636–1645. [Google Scholar] [CrossRef]
- Vors, C.; Allaire, J.; Mejia, S.B.; Khan, T.A.; Sievenpiper, J.L.; Lamarche, B. Comparing the effects of docosahexaenoic and eicosapentaenoic acids on inflammation markers using pairwise and network meta-analyses of randomized controlled trials. Adv. Nutr. 2021, 12, 128–140. [Google Scholar] [CrossRef]
- Klemens, C.M.; Berman, D.R.; Mozurkewich, E.L. The effect of perinatal omega-3 fatty acid supplementation on inflammatory markers and allergic diseases: A systematic review. BJOG 2011, 118, 916–925. [Google Scholar] [CrossRef] [Green Version]
- Gunaratne, A.W.; Makrides, M.; Collins, C.T. Maternal prenatal and/or postnatal n-3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood. Cochrane Database Syst. Rev. 2015, 7, CD010085. [Google Scholar] [CrossRef]
- Lin, J.; Zhang, Y.; Zhu, X.; Wang, D.; Dai, J. Effects of supplementation with omega-3 fatty acids during pregnancy on asthma or wheeze of children: A systematic review and meta-analysis. J. Matern. Fetal Neonatal Med. 2020, 33, 1792–1801. [Google Scholar] [CrossRef]

| First Author, Year of Publ. | Age at Allergy Investigation | Type of Sample | Type of Allergy | Fatty Acids in Allergic Patients |
|---|---|---|---|---|
| Yu G, 1996 [87] | in the first 6 years | Cord blood serum PL | Allergic disease | LA, DHGLA, AA: →; EPA, DPA, DHA: → |
| Byberg K, 2008 [86] | 3 years | Cord blood plasma | Atopy | LA, GLA, DHGLA, AA: →; EPA: ↓; ALA, DHA: → |
| Montes R, 2013 [84] | 14 months | Cord blood plasma | Atopy | LA, GLA, DHGLA, AA: →; ALA, EPA, DPA, DHA: → |
| Barman M, 2019 [81] | 36 months | Cord blood serum PL | Allergy | AA: → |
| Barman M, 2020 [82] | 3 years | Cord blood serum PL | Allergy | EPA: ↓; ALA, DPA, DHA: →; LA, DHGLA, AA: → |
| 8 years | EPA: ↓; ALA, DPA, DHA: →; LA, DHGLA, AA: → | |||
| Galli E, 1994 [88] | 12 months | Cord blood serum PL | Atopy | LA: →; DHGLA, AA: ↓ |
| Furuhjelm C, 2011 [77] | 0–24 months | Cord blood plasma PL | >1 Allergic symptoms | EPA: ↓; DHA: →; AA/EPA: ↑ |
| First Author, Year of Publ. | Group | Age at Investigation | Type of Allergy | RR/OR |
|---|---|---|---|---|
| Best KP, 2018 [76] | n-3 LCPUFA supplementation | 1 years | Wheeze symptoms with sensitization | adjusted RR: 0.52 (p = 0.03) |
| 1 years | Egg sensitization | adjusted RR: 0.62 (p = 0.02) | ||
| 6 years | D. farinae sensitization | adjusted RR: 0.62 (p = 0.02) | ||
| Barman M, 2020 [82] | Cord blood EPA | 3 years | Allergy | OR: 0.20 (p = 0.045) |
| Byberg K, 2008 [86] | High EPA in cord blood (upper quartile) | 3 years | Atopy | RR: 0.3 (p = 0.03) |
| Montes R, 2013 [84] | Cord plasma DHA | 6 and 14 months | Eczema | adjusted OR: 0.50 (p = 0.01) |
| Cord plasma n-3 LCPUFA | adjusted OR: 0.49 (p = 0.00) | |||
| Newson RB, 2004 [85] | Cord RBC AA/EPA | 18–30 months | Eczema | adjusted OR: 1.14 (p = 0.044) |
| Cord RBC LA/ALA | 30–42 months | Wheezing | adjusted OR: 1.04 (p = 0.019) | |
| Cord RBC ALA/n-3 | adjusted OR: 0.98 (p = 0.040) |
| First Author, Year of Publ. | Age at Investigation | Fatty Acid | Dependent Variable | β or r (p) |
|---|---|---|---|---|
| Barden AE, 2004 [75] | Birth | Cord RBC EPA | Cord plasma F2-isoprostanes | r = −0.351 (p = 0.001) |
| Cord RBC EPA | Urinary F2-isoprostanes | r = −0.290 (p = 0.017) | ||
| Cord RBC DHA | r = −0.241 (p = 0.05) | |||
| Byberg K, 2008 [86] | Birth | n-3 PUFA | sCD23 | r = −0.28 (p = 0.018) |
| DHA | r = −0.26 (p = 0.031) | |||
| EPA | r = −0.26 (p = 0.03) | |||
| DPA | r = −0.2 (p = 0.026) | |||
| Mozurkewich EL, 2018 [79] | Birth | Cord blood DHA | IL 1β | Neg. corr. (p = 0.03) |
| Mozurkewich EL, 2016 [78] | Birth | Log cord plasma DHA * | log 4-HDHA | r = 0.51 (p < 0.001) |
| log 14-HDHA | r = 0.47 (p < 0.001) | |||
| log 17-HDHA | r = 0.34 (p < 0.02) | |||
| See, 2017 [80] | Birth | Cord RBC EPA | 18-HEPE | B = 151.4 (p < 0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Decsi, T.; Marosvölgyi, T.; Muszil, E.; Bódy, B.; Szabó, É. Long-Chain Polyunsaturated Fatty Acid Status at Birth and Development of Childhood Allergy: A Systematic Review. Life 2022, 12, 526. https://doi.org/10.3390/life12040526
Decsi T, Marosvölgyi T, Muszil E, Bódy B, Szabó É. Long-Chain Polyunsaturated Fatty Acid Status at Birth and Development of Childhood Allergy: A Systematic Review. Life. 2022; 12(4):526. https://doi.org/10.3390/life12040526
Chicago/Turabian StyleDecsi, Tamás, Tamás Marosvölgyi, Eszter Muszil, Blanka Bódy, and Éva Szabó. 2022. "Long-Chain Polyunsaturated Fatty Acid Status at Birth and Development of Childhood Allergy: A Systematic Review" Life 12, no. 4: 526. https://doi.org/10.3390/life12040526
APA StyleDecsi, T., Marosvölgyi, T., Muszil, E., Bódy, B., & Szabó, É. (2022). Long-Chain Polyunsaturated Fatty Acid Status at Birth and Development of Childhood Allergy: A Systematic Review. Life, 12(4), 526. https://doi.org/10.3390/life12040526