
Cellular Immune Response in Patients Immunized with Three Vaccine Doses of Different Vaccination Schemes Authorized by the Chilean Ministry of Health in January 2022

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
- -
- Coronavac-Coronavac-Vaxzevria (n = 16)
- -
- Comirnaty-Comirnaty-Comirnaty (n = 16)
- -
- Coronavac-Coronavac-Comirnaty (n = 16)
2.1. Evaluation of Humoral Response
2.2. Assessment of the Specific Cellular Response of SARS-CoV-2
- -
- Nil: patient’s baseline gamma interferon measurement
- -
- Original SP: Tube with spike antigen of ancestral virus (Wuhan/Hu-1/2019) and UK/alpha lineage B.1.1.7 variant.
- -
- Variant SP: Tube with spike antigen South African variant/Beta lineage B.1.351 and Brazilian variant/gamma lineage P.1.
- -
- Variant S Delta: Tube with spike antigen variant Delta lineage B.1.617.2.
- -
- NP antigen: tube with antigen corresponding to the nucleocapsid protein.
- -
- Mitogen: positive control tube to rule out lymphocytic anergy.
2.3. Statistical Analysis
2.4. Ethical Considerations and Disclosures
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, L.; Wang, Y.; Ye, D.; Liu, Q. Review of the 2019 novel coronavirus (SARS-CoV-2) based on current evidence. Int. J. Antimicrob. Agents 2020, 55, 105948. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.-S.; Lee, N.-J.; Woo, S.H.; Kim, J.-M.; Kim, H.M.; Jo, H.J.; Park, Y.E.; Han, M.-G. Validation of real-time RT-PCR for detection of SARS-CoV-2 in the early stages of the COVID-19 outbreak in the Republic of Korea. Sci. Rep. 2021, 11, 14817. [Google Scholar] [CrossRef] [PubMed]
- Nature. Available online: https://www.nature.com/articles/d41586-022-00104-8 (accessed on 18 February 2022).
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Park, T.; Lee, S.; Kim, S.; Jeong Kim, M.; Kim, H.; Jun, S.; Kim, S.; Kim, B.; Changkyun Park, E.; Park, D. Spike protein binding prediction with neutralizing antibodies of SARS-CoV-2. bioRxiv 2020. [Google Scholar] [CrossRef]
- Al-Zyoud, W.; Haddad, H. Dynamics prediction of emerging notable spike protein mutations in SARS-CoV-2 implies a need for updated vaccines. Biochimie 2021, 191, 91–103. [Google Scholar] [CrossRef]
- Hastie, K.M.; Li, H.; Bedinger, D.; Schendel, S.L.; Dennison, S.M.; Li, K.; Rayaprolu, V.; Yu, X.; Mann, C.; Zandonatti, M.; et al. Defining variant-resistant epitopes targeted by SARS-CoV-2 antibodies: A global consortium study. Science 2021, 374, 472–478. [Google Scholar] [CrossRef]
- Manisty, C.; Otter, A.D.; Treibel, T.A.; McKnight, Á.; Altmann, D.M.; Brooks, T.; Noursadeghi, M.; Boyton, R.J.; Semper, A.; Moon, J.C. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet 2021, 397, 1057–1058. [Google Scholar] [CrossRef]
- Tarke, A.; Sidney, J.; Methot, N.; Yu, E.D.; Zhang, Y.; Dan, J.M.; Goodwin, B.; Rubiro, P.; Sutherland, A.; Wang, E.; et al. Impact of SARS-CoV-2 variants on the total CD4+ and CD8+ T cell reactivity in infected or vaccinated individuals. Cell Rep. Med. 2021, 2, 100355. [Google Scholar] [CrossRef] [PubMed]
- Geers, D.; Shamier, M.C.; Bogers, S.; den Hartog, G.; Gommers, L.; Nieuwkoop, N.N.; Schmitz, K.S.; Rijsbergen, L.C.; van Osch, J.A.; Dijkhuizen, E.; et al. SARS-CoV-2 variants of concern partially escape humoral but not T-cell responses in COVID-19 convalescent donors and vaccinees. Sci. Immunol. 2021, 6, eabj1750. [Google Scholar] [CrossRef]
- Richter, D.; Guasti, L.; Koehler, F.; Squizzato, A.; Nistri, S.; Christodorescu, R.; Dievart, F.; Gaudio, G.; Asteggiano, R.; Ferrini, M. Late phase of COVID-19 pandemic in General Cardiology. A position paper of the ESC Council for Cardiology Practice. ESC Hearth Fail. 2021, 8, 3483–3494. [Google Scholar] [CrossRef]
- Cascella, M.; Del Gaudio, A.; Vittori, A.; Bimonte, S.; Del Prete, P.; Forte, C.A.; Cuomo, A.; De Blasio, E. COVID-Pain: Acute and Late-Onset Painful Clinical Manifestations in COVID-19–Molecular Mechanisms and Research Perspectives. J. Pain Res. 2021, 14, 2403–2412. [Google Scholar] [CrossRef]
- Bussmann, A.J.C.; Ferraz, C.R.; Lima, A.V.A.; Castro, J.G.S.; Ritter, P.D.; Zaninelli, T.H.; Saraiva-Santos, T.; Verri, W.A.; Borghi, S.M. Association between IL-10 systemic low level and pain during symptomatic SARS-CoV-2 infection. Pain Pract. 2022. [Google Scholar] [CrossRef] [PubMed]
- Sansone, A.; Mollaioli, D.; Ciocca, G.; Colonnello, E.; Limoncin, E.; Balercia, G.; Jannini, E.A. “Mask up to keep it up”: Preliminary evidence of the association between erectile dysfunction and COVID-19. Andrology 2021, 9, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Parra-Lucares, A.; Segura, P.; Rojas, V.; Pumarino, C.; Saint-Pierre, G.; Toro, L. Emergence of SARS-CoV-2 Variants in the World: How Could This Happen? Life 2022, 12, 194. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, A.M.; Spicer, K.B.; Thoroughman, D.; Glick, C.; Winter, K. Reduced Risk of Reinfection with SARS-CoV-2 After COVID-19 Vaccination—Kentucky, May–June 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1081–1083. [Google Scholar] [CrossRef] [PubMed]
- Xing, K.; Tu, X.-Y.; Liu, M.; Liang, Z.-W.; Chen, J.-N.; Li, J.-J.; Jiang, L.-G.; Xing, F.-Q.; Jiang, Y. Efficacy and safety of COVID-19 vaccines: A systematic review. Chin. J. Contemp. Pediatr. 2021, 23, 221–228. [Google Scholar]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Ledford, H. Do vaccines protect against long COVID? What the data say. Nature 2021, 599, 546–548. [Google Scholar] [CrossRef]
- Our World in Data. Coronavirus Pandemic (COVID-19). 2022. Available online: https://ourworldindata.org/coronavirus (accessed on 18 February 2022).
- Vacunas MINSAL. Available online: https://www.minsal.cl/wp-content/uploads/2021/12/Vacunaci%C3%B3n-contra-SARS-CoV-2-en-pre-escolares-3-a-5-a%C3%B1os.pdf (accessed on 18 February 2022).
- Guelfenbein, C.I.; Torretti, J.P.T.; de Pablo, M.E.S. Vacunas SARS CoV-2, estudios en fase III. Rev. Chile. Infectol. 2021, 38, 88–98. [Google Scholar] [CrossRef]
- Knoll, M.D.; Wonodi, C. Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef]
- Jara, A.; Undurraga, E.A.; González, C.; Paredes, F.; Fontecilla, T.; Jara, G.; Pizarro, A.; Acevedo, J.; Leo, K.; Leon, F.; et al. Effectiveness of an Inactivated SARS-CoV-2 Vaccine in Chile. N. Engl. J. Med. 2021, 385, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Halperin, A.S.; Ye, L.; MacKinnon-Cameron, D.; Smith, B.; Cahn, P.E.; Ruiz-Palacios, G.M.; Ikram, A.; Lanas, F.; Guerrero, M.L.; Navarro, S.R.M.; et al. Final efficacy analysis, interim safety analysis, and immunogenicity of a single dose of recombinant novel coronavirus vaccine (adenovirus type 5 vector) in adults 18 years and older: An international, multicentre, randomised, double-blinded, placebo-controlled phase 3 trial. Lancet 2021, 399, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Schultz, B.; Melo-González, F.; Duarte, L.; Gálvez, N.; Pacheco, G.; Soto, G.; Berríos-Rojas, R.; González, L.; Moreno-Tapia, D.; Rivera-Pérez, D.; et al. A booster dose of an inactivated vaccine increases neutralizing antibodies and T cell responses against SARS-CoV-2. medRxiv 2021. [Google Scholar] [CrossRef]
- Schiffner, J.; Backhaus, I.; Rimmele, J.; Schulz, S.; Möhlenkamp, T.; Klemens, J.M.; Zapf, D.; Solbach, W.; Mischnik, A. Long-Term Course of Humoral and Cellular Immune Responses in Outpatients After SARS-CoV-2 Infection. Front. Public Health 2021, 9, 732787. [Google Scholar] [CrossRef]
- Havervall, S.; Ng, H.; Falk, A.J.; Greilert-Norin, N.; Månberg, A.; Marking, U.; Laurén, I.; Gabrielsson, L.; Salomonsson, A.; Aguilera, K.; et al. Robust humoral and cellular immune responses and low risk for reinfection at least 8 months following asymptomatic to mild COVID-19. J. Intern. Med. 2021, 291, 72–80. [Google Scholar] [CrossRef] [PubMed]
- VITROS Immunodiagnostic Products Anti-SARS-CoV-2 IgG Quantitative Reagent Pack. Technical Document. Available online: https://techdocs.orthoclinicaldiagnostics.com/TechDocs/TechDocSearch.aspx?tID=0&culture=en-us (accessed on 24 January 2022).
- STANDARD F SARS-CoV-2 nAb FIA. Technical Document. Available online: https://www.sdbiosensor.com/product/product_view?product_no=175# (accessed on 24 January 2022).
- Covi-FERON FIA (IFN-Gamma) Technical Document. Available online: https://www.sdbiosensor.com/product/product_view?product_no=1241 (accessed on 24 January 2022).
- Torjesen, I. Covid-19: AstraZeneca vaccine is approved in EU with no upper age limit. BMJ 2021, 372, n295. [Google Scholar] [CrossRef]
- Dyer, O. Covid-19: Canada relaxes age limits on AstraZeneca vaccine as Ontario cases surge. BMJ 2021, 373, n1053. [Google Scholar] [CrossRef]
- ISP Chile. Available online: https://www.ispch.cl/wp-content/uploads/2021/12/UCD289.pdf (accessed on 18 February 2022).
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv-Baran, T.; Arbel, Y.S.; Scarfò, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef]
- Re, D.; Barrière, J.; Chamorey, E.; Delforge, M.; Gastaud, L.; Petit, E.; Chaminade, A.; Verrière, B.; Peyrade, F. Low rate of seroconversion after mRNA anti-SARS-CoV-2 vaccination in patients with hematological malignancies. Leuk. Lymphoma 2021, 62, 3308–3310. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Bueno, S.M.; Abarca, K.; González, P.A.; Gálvez, N.M.S.; Soto, J.A.; Duarte, L.F.; Schultz, B.M.; Pacheco, G.A.; González, L.A.; Vázquez, Y.; et al. Safety and Immunogenicity of an Inactivated Severe Acute Respiratory Syndrome Coronavirus 2 Vaccine in a Subgroup of Healthy Adults in Chile. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef] [PubMed]
- Lustig, Y.; Sapir, E.; Regev-Yochay, G.; Cohen, C.; Fluss, R.; Olmer, L.; Indenbaum, V.; Mandelboim, M.; Doolman, R.; Amit, S.; et al. BNT162b2 COVID-19 vaccine and correlates of humoral immune responses and dynamics: A prospective, single-centre, longitudinal cohort study in health-care workers. Lancet Respir. Med. 2021, 9, 999–1009. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Souza, W.M.; Amorim, M.R.; Sesti-Costa, R.; Coimbra, L.D.; Brunetti, N.S.; Toledo-Teixeira, D.A.; de Souza, G.F.; Muraro, S.P.; Parise, P.L.; Barbosa, P.P.; et al. Neutralisation of SARS-CoV-2 lineage P.1 by antibodies elicited through natural SARS-CoV-2 infection or vaccination with an inactivated SARS-CoV-2 vaccine: An immunological study. Lancet Microbe 2021, 2, e527–e535. [Google Scholar] [CrossRef]
- Dashdorj, N.J.; Wirz, O.F.; Röltgen, K.; Haraguchi, E.; Buzzanco, A.S.; Sibai, M.; Wang, H.; Miller, J.A.; Solis, D.; Sahoo, M.K.; et al. Direct comparison of antibody responses to four SARS-CoV-2 vaccines in Mongolia. Cell Host Microbe 2021, 29, 1738–1743.e4. [Google Scholar] [CrossRef]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Coronavac-Coronavac-Comirnaty | Coronavac-Coronavac-Vaxzevria | Comirnaty-Comirnaty-Comirnaty | p Value | |
|---|---|---|---|---|
| n | 16 | 16 | 16 | - |
| Age ( ± SD) | 35.31 ± 7.382 | 59.13 ± 3.828 | 35.94 ± 8.290 | <0.0001 † |
| Arterial Hypertension (%) | 0 (0) | 2 (12.5) | 0 (0) | 0.1241‡ |
| Type 2 Diabetes Mellitus (%) | 0 (0) | 0 (0) | 0 (0) | - |
| Obesity | 0 (0) | 2 (12.5) | 0 (0) | 0.1241 ‡ |
| Smoking | 0 (0) | 2 (12.5) | 0 (0) | 0.1241 ‡ |
| Coronavac-Coronavac-Comirnaty | Coronavac-Coronavac-Vaxzevria | Comirnaty-Comirnaty-Comirnaty | p Value | |
|---|---|---|---|---|
| Nil Tube | 0.1628 ± 0.0712 | 0.1794 ± 0.0940 | 0.1450 ± 0.0000 | >0.9999 š |
| Original SP Tube | 3.236 ± 3.234 | 2.058 ± 1.876 | 3.206 ± 3.617 | >0.9999 š |
| Variant SP Tube | 3.057 ± 3.320 | 3.003 ± 2.972 | 2.811 ± 3.611 | >0.9999 š |
| Spike Delta | 0.9856 ± 1.132 | 0.9603 ± 1.280 | 0.7991 ± 1.167 | >0.9999 š |
| NP Tube | 0.8503 ± 1.879 | 1.172 ± 1.783 | 0.1588 ± 0.0536 | 0.0078 š |
| Mitogen Tube | 10.000 ± 0.000 | 10.000 ± 0.000 | 10.000 ± 0.000 | - |
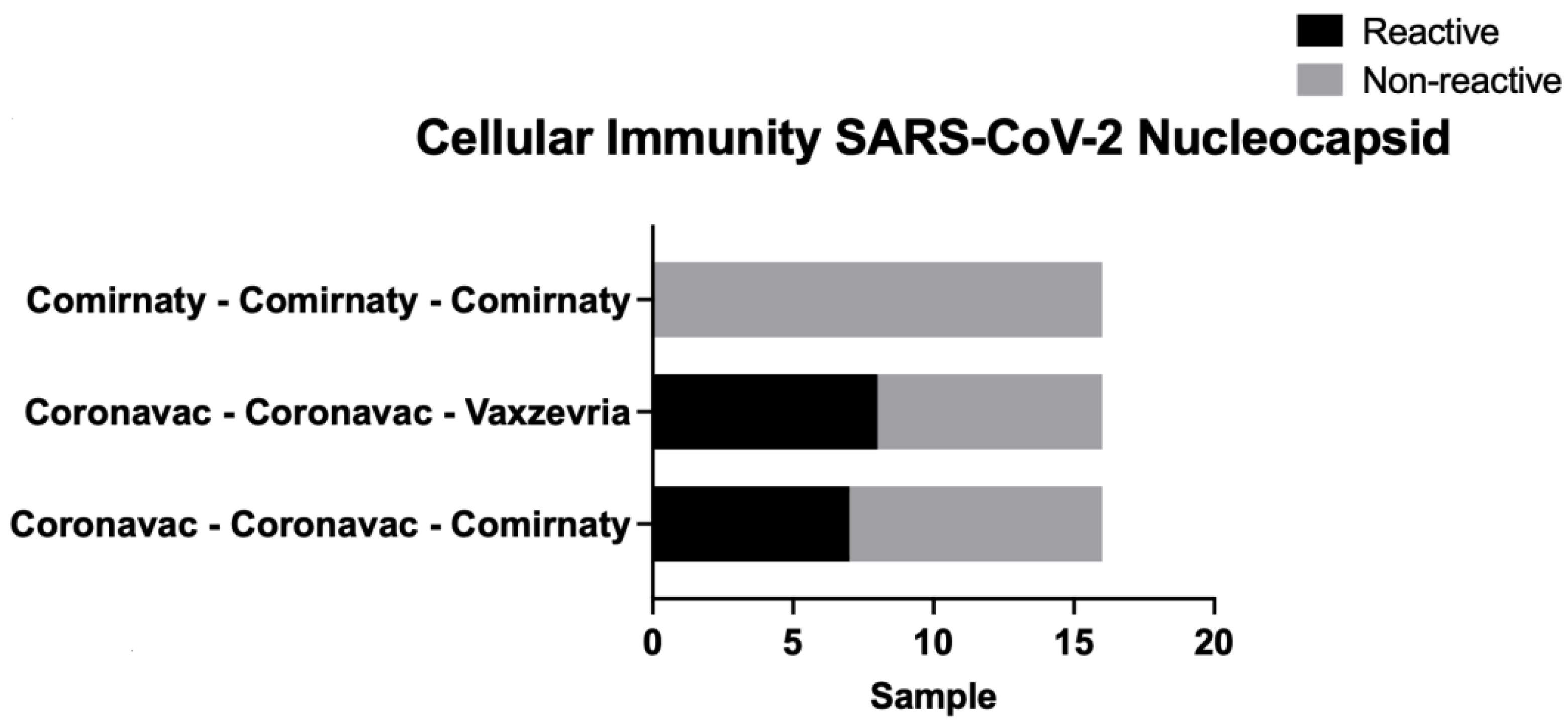
| n ± % | Coronavac-Coronavac-Comirnaty | Coronavac-Coronavac-Vaxzevria | Comirnaty-Comirnaty-Comirnaty | p Value |
|---|---|---|---|---|
| Alpha/Beta | 14 (87.5) | 11 (68.75) | 12 (75) | 0.4380 ‡ |
| Gamma | 15 (93.75) | 13 (81.25) | 12 (75) | 0.3499 ‡ |
| Delta | 8 (50) | 8 (50) | 7 (43.75) | 0.9199 ‡ |
| Nucleocapsid | 7 (43.75) | 8 (50) | 0 (0) | 0.0040 ‡ |
| Coronavac-Coronavac-Comirnaty | Coronavac-Coronavac-Vaxzevria | Comirnaty-Comirnaty-Comirnaty | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Brazil | Delta | Nucleocapsid | Brazil | Delta | Nucleocapsid | Brazil | Delta | Nucleocapsid | |
| p value | 0.0055 | 0.0060 | 0.0023 | 0.0082 | 0.1097 | 0.2210 | 0.9265 | 0.8794 | >0.9999 |
| r | 0.6591 | 0.6535 | 0.7056 | 0.6352 | 0.4153 | 0.3239 | −0.02510 | −0.04127 | - |
| IC 95% | 0.2427–0.8704 | 0.2334–0.8680 | 0.3229–0.8900 | 0.2037–0.8601 | −0.1013–0.7555 | −0.2046–0.7062 | −0.5144–0.4765 | −0.5262–0.4639 | - |
| Coronavac-Coronavac-Comirnaty | Coronavac-Coronavac-Vaxzevria | Comirnaty-Comirnaty-Comirnaty | |
|---|---|---|---|
| p value | <0.0001 | <0.0001 | 0.0161 |
| r | 0.8238 | 0.8618 | 0.5902 |
| IC 95% | 0.5545–0.9369 | 0.6392–0.9512 | 0.1336–0.8401 |
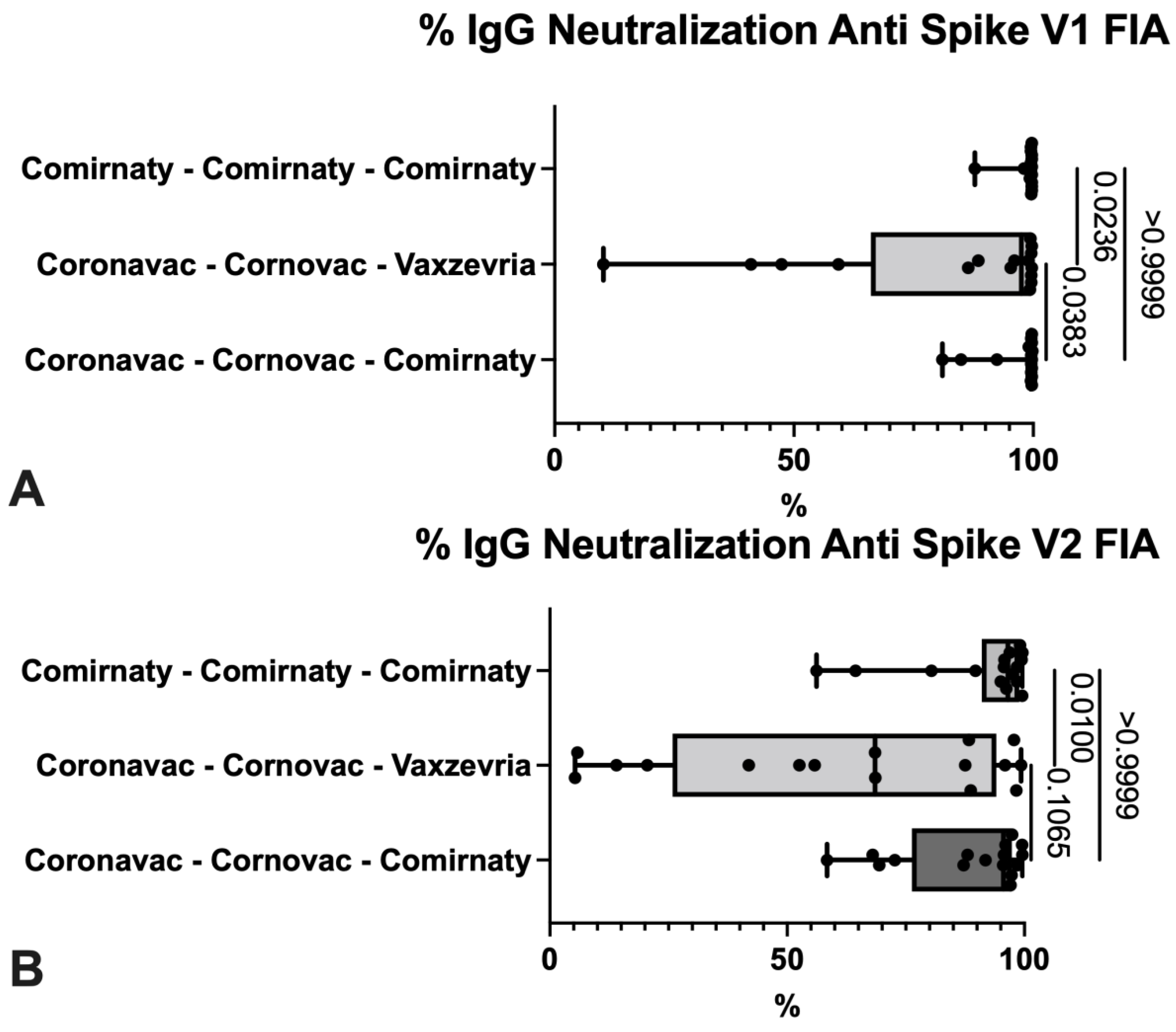
| Coronavac-Coronavac-Comirnaty | Coronavac-Coronavac-Vaxzevria | Comirnaty-Comirnaty-Comirnaty | p Value | |
|---|---|---|---|---|
| V1FIA (ancestral/alfa) | 97.08 ± 5.847 | 82.51 ± 27.60 | 98.78 ± 2.953 | 0.0236 š |
| V2FIA (beta/gamma) | 88.26 ± 13.38 | 61.80 ± 34.84 | 91.39 ± 13.13 | 0.0100 š |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabilo Valenzuela, P.B.; Flores Balter, G.; Saint-Pierre Contreras, G.; Conei Valencia, D.; Moreno Calderón, C.; Bohle Venegas, C.; Guajardo Rivera, M.; Silva Ojeda, F.; Vial Covarrubias, M.J. Cellular Immune Response in Patients Immunized with Three Vaccine Doses of Different Vaccination Schemes Authorized by the Chilean Ministry of Health in January 2022. Life 2022, 12, 534. https://doi.org/10.3390/life12040534
Tabilo Valenzuela PB, Flores Balter G, Saint-Pierre Contreras G, Conei Valencia D, Moreno Calderón C, Bohle Venegas C, Guajardo Rivera M, Silva Ojeda F, Vial Covarrubias MJ. Cellular Immune Response in Patients Immunized with Three Vaccine Doses of Different Vaccination Schemes Authorized by the Chilean Ministry of Health in January 2022. Life. 2022; 12(4):534. https://doi.org/10.3390/life12040534
Chicago/Turabian StyleTabilo Valenzuela, Paz Beatriz, Gabriela Flores Balter, Gustavo Saint-Pierre Contreras, Daniel Conei Valencia, Catalina Moreno Calderón, Constanza Bohle Venegas, Marcia Guajardo Rivera, Francisco Silva Ojeda, and Maria Jesus Vial Covarrubias. 2022. "Cellular Immune Response in Patients Immunized with Three Vaccine Doses of Different Vaccination Schemes Authorized by the Chilean Ministry of Health in January 2022" Life 12, no. 4: 534. https://doi.org/10.3390/life12040534
APA StyleTabilo Valenzuela, P. B., Flores Balter, G., Saint-Pierre Contreras, G., Conei Valencia, D., Moreno Calderón, C., Bohle Venegas, C., Guajardo Rivera, M., Silva Ojeda, F., & Vial Covarrubias, M. J. (2022). Cellular Immune Response in Patients Immunized with Three Vaccine Doses of Different Vaccination Schemes Authorized by the Chilean Ministry of Health in January 2022. Life, 12(4), 534. https://doi.org/10.3390/life12040534