
Microvascular and Morphologic Changes of the Macula over Lifetime

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
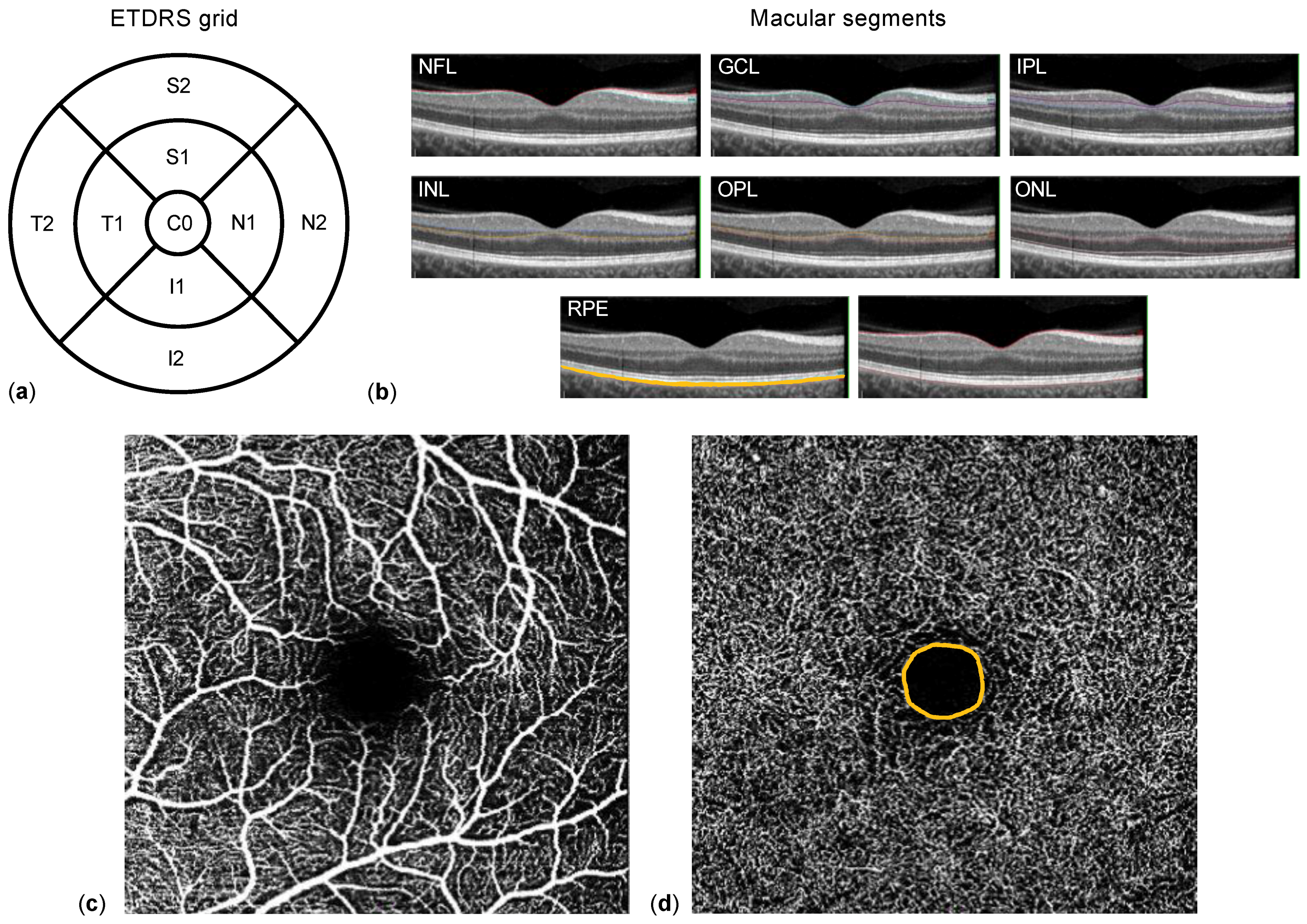
2.2. Data Acquisition
2.3. Statistical Methods
3. Results
3.1. Characteristics of the Study Population
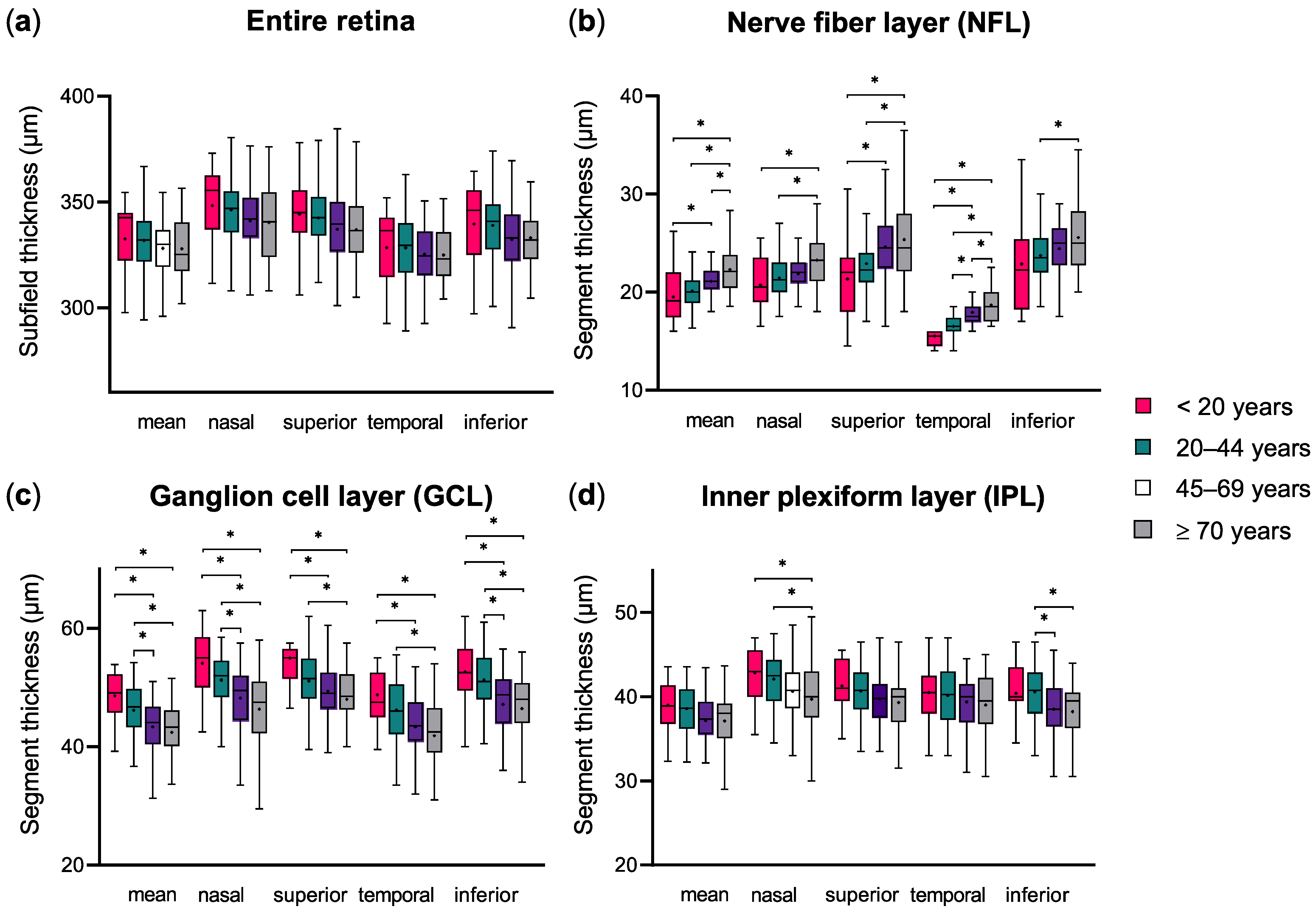
3.2. Changes of Macular Segment Thickness with Age
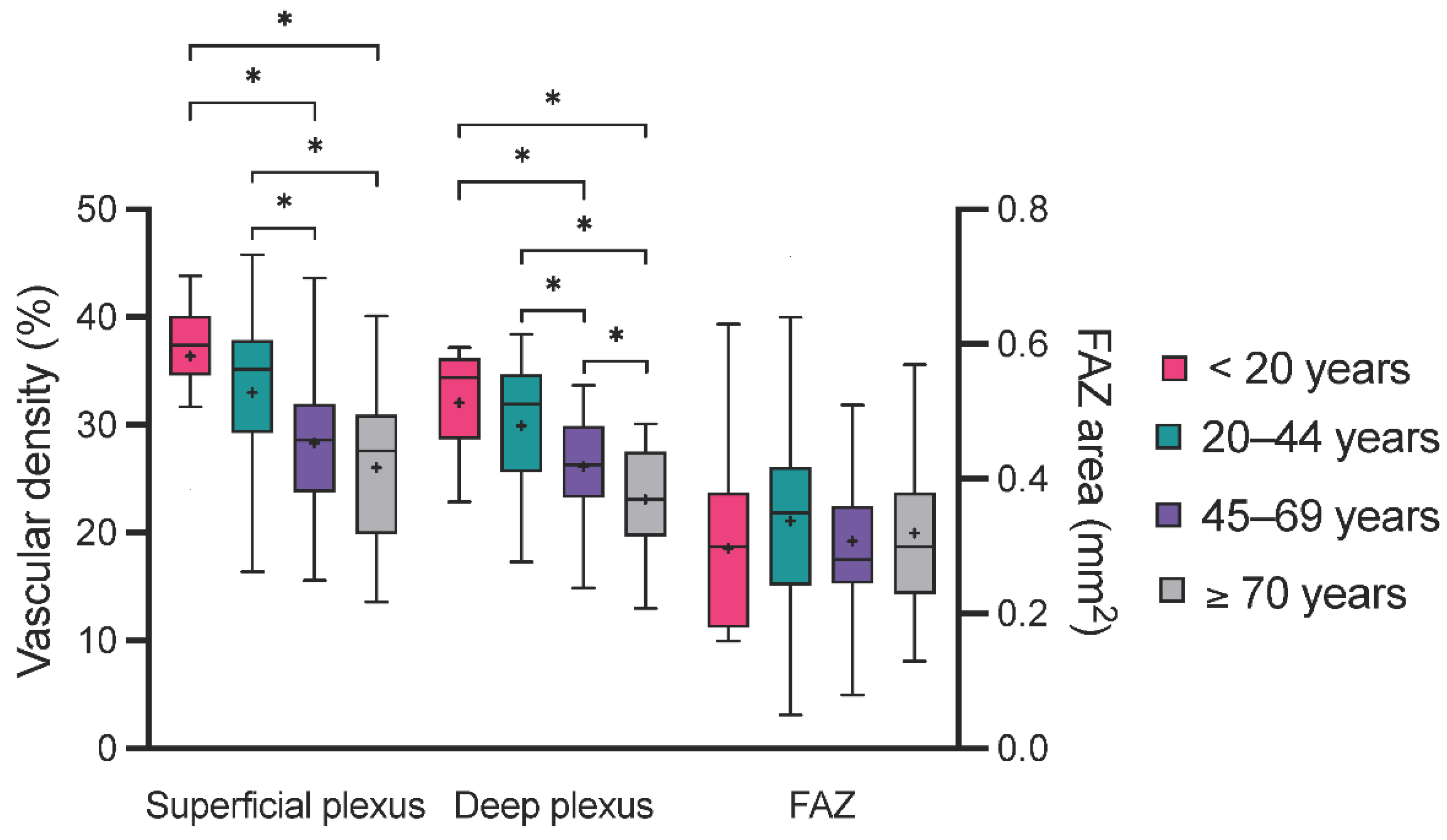
3.3. Age-Related Microvascular Changes of the Macula
3.4. Association between Age, Macular Segment Thickness, and OCTA Parameters
4. Discussion
- Increasing age appears to be associated with a decrease in total macular and inner retinal segment thickness.
- Superficial and deep plexus vascular density seem to diminish with increasing age.
- There is a strong association between OCTA parameters and inner macular segment thickness that is independent of age.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Samuel, M.A.; Zhang, Y.; Meister, M.; Sanes, J.R. Age-Related Alterations in Neurons of the Mouse Retina. J. Neurosci. 2011, 31, 16033–16044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langenegger, S.J.; Funk, J.; Töteberg-Harms, M. Reproducibility of Retinal Nerve Fiber Layer Thickness Measurements Using the Eye Tracker and the Retest Function of Spectralis SD-OCT in Glaucomatous and Healthy Control Eyes. Investig. Ophthalmol. Vis. Sci. 2011, 52, 3338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Freedman, S.F.; Silverstein, E.; Muir, K.; El-Dairi, M. Longitudinal reproducibility of spectral domain optical coherence tomography in children with physiologic cupping and stable glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2019, 23, 262.e1–262.e6. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.; Lin, C.; Schuman, J.; Stinson, W.; Chang, W.; Hee, M.; Flotte, T.; Gregory, K.; Puliafito, C.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasia, F.F.; Freedman, S.F.; Rajani, A.; Holgado, S.; Asrani, S.; El-Dairi, M. Optical coherence tomography in paediatric glaucoma: Time domain versus spectral domain. Br. J. Ophthalmol. 2013, 97, 837–842. [Google Scholar] [CrossRef]
- Eriksson, U.; Alm, A. Macular thickness decreases with age in normal eyes: A study on the macular thickness map protocol in the Stratus OCT. Br. J. Ophthalmol. 2009, 93, 1448–1452. [Google Scholar] [CrossRef]
- Leung, C.K.S.; Yu, M.; Weinreb, R.N.; Ye, C.; Liu, S.; Lai, G.; Lam, D.S.C. Retinal Nerve Fiber Layer Imaging with Spectral-Domain Optical Coherence Tomography: A Prospective Analysis of Age-Related Loss. Ophthalmology 2012, 119, 731–737. [Google Scholar] [CrossRef]
- De Sisternes, L.; Jonna, G.; Moss, J.; Marmor, M.F.; Leng, T.; Rubin, D.L. Automated intraretinal segmentation of SD-OCT images in normal and age-related macular degeneration eyes. Biomed. Opt. Express 2017, 8, 1926. [Google Scholar] [CrossRef] [Green Version]
- Unterlauft, J.D.; Rehak, M.; Böhm, M.R.R.; Rauscher, F.G. Analyzing the impact of glaucoma on the macular architecture using spectral-domain optical coherence tomography. PLoS ONE 2018, 13, e0209610. [Google Scholar] [CrossRef]
- Lever, M.; Wilde, B.; Pförtner, R.; Deuschl, C.; Witzke, O.; Bertram, S.; Eckstein, A.; Rath, P.-M. Orbital aspergillosis: A case report and review of the literature. BMC Ophthalmol. 2021, 21, 22. [Google Scholar] [CrossRef]
- Lever, M.; Glaser, M.; Chen, Y.; Halfwassen, C.; Unterlauft, J.D.; Bechrakis, N.E.; Böhm, M.R.R. Microvascular and Structural Alterations of the Macula in Early to Moderate Glaucoma: An Optical Coherence Tomography-Angiography Study. J. Clin. Med. 2021, 10, 5017. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Martin, E.; Polo, V.; Larrosa, J.M.; Marques, M.L.; Herrero, R.; Martin, J.; Ara, J.R.; Fernandez, J.; Pablo, L.E. Retinal layer segmentation in patients with multiple sclerosis using spectral domain optical coherence tomography. Ophthalmology 2014, 121, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Sari, E.S.; Koc, R.; Yazici, A.; Sahin, G.; Ermis, S.S. Ganglion cell-inner plexiform layer thickness in patients with Parkinson disease and association with disease severity and duration. J. Neuroophthalmol. 2015, 35, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Zhang, L.; Li, Z.; Zhang, X.; Wu, Y.; Yang, H.; Min, B.; Zhang, X.; Ma, D.; Lu, Y. Thinner changes of the retinal nerve fiber layer in patients with mild cognitive impairment and Alzheimer’s disease. BMC Neurol. 2015, 15, 14. [Google Scholar] [CrossRef] [Green Version]
- Peng, P.H.; Lin, H.S.; Lin, S. Nerve fibre layer thinning in patients with preclinical retinopathy. Can. J. Ophthalmol. 2009, 44, 417–422. [Google Scholar] [CrossRef]
- Lommatzsch, A. OCT Angiography. Klin. Monbl. Augenheilkd. 2020, 237, 95–111. [Google Scholar] [CrossRef]
- Takusagawa, H.L.; Liu, L.; Ma, K.N.; Jia, Y.; Gao, S.S.; Zhang, M.; Edmunds, B.; Parikh, M.; Tehrani, S.; Morrison, J.C.; et al. Projection-Resolved Optical Coherence Tomography Angiography of Macular Retinal Circulation in Glaucoma. Ophthalmology 2017, 124, 1589–1599. [Google Scholar] [CrossRef]
- Wang, Q.; Chan, S.; Yang, J.Y.; You, B.; Wang, Y.X.; Jonas, J.B.; Wei, W. Bin Vascular Density in Retina and Choriocapillaris as Measured by Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2016, 168, 95–109. [Google Scholar] [CrossRef]
- Coscas, F.; Sellam, A.; Glacet-Bernard, A.; Jung, C.; Goudot, M.; Miere, A.; Souied, E.H. Normative data for vascular density in superficial and deep capillary plexuses of healthy adults assessed by optical coherence tomography angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT211–OCT223. [Google Scholar] [CrossRef]
- Balaratnasingam, C.; Inoue, M.; Ahn, S.; McCann, J.; Dhrami-Gavazi, E.; Yannuzzi, L.A.; Freund, K.B. Visual Acuity Is Correlated with the Area of the Foveal Avascular Zone in Diabetic Retinopathy and Retinal Vein Occlusion. Ophthalmology 2016, 123, 2352–2367. [Google Scholar] [CrossRef] [PubMed]
- De Carlo, T.E.; Chin, A.T.; Bonini Filho, M.A.; Adhi, M.; Branchini, L.; Salz, D.A.; Baumal, C.R.; Crawford, C.; Reichel, E.; Witkin, A.J.; et al. Detection of microvascular changes in eyes of patients with diabetes but not clinical diabetic retinopathy using optical coherence tomography angiography. Retina 2015, 35, 2364–2370. [Google Scholar] [CrossRef] [PubMed]
- Yarmohammadi, A.; Zangwill, L.M.; Manalastas, P.I.C.; Fuller, N.J.; Diniz-Filho, A.; Saunders, L.J.; Suh, M.H.; Hasenstab, K.; Weinreb, R.N. Peripapillary and Macular Vessel Density in Patients with Primary Open-Angle Glaucoma and Unilateral Visual Field Loss. Ophthalmology 2018, 125, 578–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lommatzsch, C.; Rothaus, K.; Koch, J.M.; Heinz, C.; Grisanti, S. OCTA vessel density changes in the macular zone in glaucomatous eyes. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 1499–1508. [Google Scholar] [CrossRef]
- Fard, M.A.; Ghahvechian, H.; Sahrayan, A.; Subramanian, P.S. Early Macular Vessel Density Loss in Acute Ischemic Optic Neuropathy Compared to Papilledema: Implications for Pathogenesis. Transl. Vis. Sci. Technol. 2018, 7, 10. [Google Scholar] [CrossRef] [PubMed]
- Mataftsi, A.; Dermenoudi, M.; Dastiridou, A.; Tsiampali, C.; Androudi, S.; Brazitikos, P.; Ziakas, N. Optical coherence tomography angiography in children with spontaneously regressed retinopathy of prematurity. Eye 2021, 35, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Carreira, A.R.; Cardoso, J.; Lopes, D.; Loureiro, T.; Sampaio, A.; Fonseca, T.; Vide-Escada, A.; Campos, N. Long-term macular vascular density measured by OCT-A in children with retinopathy of prematurity with and without need of laser treatment. Eur. J. Ophthalmol. 2021, 31, 3337–3341. [Google Scholar] [CrossRef]
- Ooto, S.; Hangai, M.; Tomidokoro, A.; Saito, H.; Araie, M.; Otani, T.; Kishi, S.; Matsushita, K.; Maeda, N.; Shirakashi, M.; et al. Effects of age, sex, and axial length on the three-dimensional profile of normal macular layer structures. Investig. Ophthalmol. Vis. Sci. 2011, 52, 8769–8779. [Google Scholar] [CrossRef]
- Wang, Q.; Wei, W.B.; Wang, Y.X.; Yan, Y.N.; Yang, J.Y.; Zhou, W.J.; Chan, S.Y.; Xu, L.; Jonas, J.B. Thickness of individual layers at the macula and associated factors: The Beijing Eye Study 2011. BMC Ophthalmol. 2020, 20, 49. [Google Scholar] [CrossRef] [Green Version]
- Gao, H.; Hollyfield, J.G. Aging of the human retina: Differential loss of neurons and retinal pigment epithelial cells. Investig. Ophthalmol. Vis. Sci. 1992, 33, 1–17. [Google Scholar]
- Demirkaya, N.; van Dijk, H.W.; van Schuppen, S.M.; Abràmoff, M.D.; Garvin, M.K.; Sonka, M.; Schlingemann, R.O.; Verbraak, F.D. Effect of age on individual retinal layer thickness in normal eyes as measured with spectral-domain optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4934–4940. [Google Scholar] [CrossRef]
- Curcio, C.A.; Allen, K.A. Topography of ganglion cells in human retina. J. Comp. Neurol. 1990, 300, 5–25. [Google Scholar] [CrossRef] [PubMed]
- Sung, K.R.; Wollstein, G.; Bilonick, R.A.; Townsend, K.A.; Ishikawa, H.; Kagemann, L.; Noecker, R.J.; Fujimoto, J.G.; Schuman, J.S. Effects of Age on Optical Coherence Tomography Measurements of Healthy Retinal Nerve Fiber Layer, Macula, and Optic Nerve Head. Ophthalmology 2009, 116, 1119–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Q.; Li, Y.; Cheng, Y.; Qu, Y. Assessment of the effect of age on macular layer thickness in a healthy Chinese cohort using spectral-domain optical coherence tomography. BMC Ophthalmol. 2018, 18, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieves-Moreno, M.; Martínez-de-la-Casa, J.M.; Morales-Fernández, L.; Sánchez-Jean, R.; Sáenz-Francés, F.; García-Feijoó, J. Impacts of age and sex on retinal layer thicknesses measured by spectral domain optical coherence tomography with Spectralis. PLoS ONE 2018, 13, e0194169. [Google Scholar] [CrossRef] [PubMed]
- Iafe, N.A.; Phasukkijwatana, N.; Chen, X.; Sarraf, D. Retinal capillary density and foveal avascular zone area are age-dependent: Quantitative analysis using optical coherence tomography angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5780–5787. [Google Scholar] [CrossRef] [Green Version]
- Cheung, C.Y.; Li, J.; Yuan, N.; Lau, G.Y.L.; Chan, A.Y.F.; Lam, A.; Tang, F.Y.; Tham, C.C.; Pang, C.P.; Chen, L.J.; et al. Quantitative retinal microvasculature in children using swept-source optical coherence tomography: The Hong Kong Children Eye Study. Br. J. Ophthalmol. 2019, 103, 672–679. [Google Scholar] [CrossRef]
- Samara, W.A.; Say, E.A.T.; Khoo, C.T.L.; Higgins, T.P.; Magrath, G.; Ferenczy, S.; Shields, C.L. Correlation of foveal avascular zone size with foveal morphology in normal eyes using optical coherence tomography angiography. Retina 2015, 35, 2188–2195. [Google Scholar] [CrossRef]
- Shahlaee, A.; Pefkianaki, M.; Hsu, J.; Ho, A.C. Measurement of Foveal Avascular Zone Dimensions and its Reliability in Healthy Eyes Using Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2016, 161, 50–55. [Google Scholar] [CrossRef]
- Skalet, A.H.; Liu, L.; Binder, C.; Miller, A.K.; Crilly, R.; Hung, A.Y.; Wilson, D.J.; Huang, D.; Jia, Y. Longitudinal Detection of Radiation-Induced Peripapillary and Macular Retinal Capillary Ischemia Using OCT Angiography. Ophthalmol. Retin. 2020, 4, 320–326. [Google Scholar] [CrossRef]
- Jeon, S.J.; Park, H.Y.L.; Park, C.K. Effect of Macular Vascular Density on Central Visual Function and Macular Structure in Glaucoma Patients. Sci. Rep. 2018, 8, 16009. [Google Scholar] [CrossRef] [Green Version]
- Rommel, F.; Rommel, F.; Rothe, M.; Rothe, M.; Kurz, M.; Kurz, M.; Prasuhn, M.; Prasuhn, M.; Grisanti, S.; Ranjbar, M.; et al. Evaluating diurnal variations in retinal perfusion using optical coherence tomography angiography. Int. J. Retin. Vitr. 2020, 6, 4–9. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Whole Population | Subgroups | ||||
|---|---|---|---|---|---|
| <20 Years | 20–44 Years | 45–69 Years | ≥70 Years | ||
| Patients (n) | 157 | 15 | 56 | 49 | 37 |
| Sex [male: female% (n)] | 41.4:58.6% (65:92) | 67:33% (10:5) | 36:64% (20:36) | 51:49% (25:24) | 41:59% (15:22) |
| Eye [right: left% (n)] | 48.4:51.6% (76:81) | 47:53% (7:8) | 41:59% (23:33) | 45:55% (27:22) | 51:49% (19:18) |
| Age [mean ± SD (y)] | 49.8 ± 21.6 | 14.5 ± 3.0 | 32.0 ± 6.8 | 58.9 ± 6.3 | 76.8 ± 5.0 |
| BCVA [mean ± SD (LogMar)] | 0.0 ± 0.06 | 0.0 ± 0.02 | 0.0 ± 0.11 | 0.1 ± 0.08 | 0.1 ± 0.11 |
| IOP [mean ± SD (mm Hg)] | 15.4 ± 2.9 | 15.4 ± 2.8 | 15.9 ± 2.6 | 15.0 ± 2.8 | 14.5 ± 3.4 |
| Macular Segment | Mean Thickness (µm ± SD) | ANOVA Summary | |||||
|---|---|---|---|---|---|---|---|
| <20 Years | 20–44 Years | 45–69 Years | ≥70 Years | F | R2 | p-Value | |
| Retina | |||||||
| Nasal | 348.3 ± 18.1 | 346.3 ± 15.6 | 341.0 ± 16.1 | 340.3 ± 18.4 | 45.9 | 0.36 | <0.0001 |
| Superior | 344.1 ± 18.7 | 342.4 ± 16.1 | 337.0 ± 19.0 | 336.8 ± 16.5 | 45.8 | 0.36 | <0.0001 |
| Temporal | 328.5 ± 19.0 | 328.3 ± 15.9 | 325.3 ± 16.2 | 324.9 ± 13.1 | 39.4 | 0.32 | <0.0001 |
| Inferior | 339.5 ± 21.2 | 338.9 ± 15.8 | 332.3 ± 16.2 | 332.9 ± 14.0 | 48.1 | 0.37 | <0.0001 |
| Nerve fiber layer (NFL) | |||||||
| Nasal | 20.7 ± 2.7 | 21.2 ± 2.4 | 22.1 ± 2.4 | 23.6 ± 3.8 | 5.6 | 0.098 | 0.0011 |
| Superior | 21.3 ± 4.2 | 22.9 ± 2.8 | 24.6 ± 3.7 | 25.5 ± 5.0 | 6.9 | 0.12 | 0.0002 |
| Temporal | 15.5 ± 1.1 | 16.5 ± 1.4 | 17.9 ± 1.1 | 18.8 ± 2.1 | 3.6 | 0.39 | <0.0001 |
| Inferior | 22.9 ± 4.8 | 23.9 ± 3.0 | 24.4 ± 3.5 | 25.6 ± 3.5 | 3.3 | 0.060 | 0.022 |
| Ganglion cell layer (GCL) | |||||||
| Nasal | 54.1 ± 5.4 | 51.3 ± 4.7 | 48.4 ± 7.8 | 46.7 ± 7.1 | 9.8 | 0.16 | <0.0001 |
| Superior | 55.0 ± 5.5 | 51.1 ± 5.0 | 47.9 ± 8.1 | 48.2 ± 5.9 | 6.7 | 0.12 | 0.0003 |
| Temporal | 48.8 ± 4.6 | 46.2 ± 5.3 | 43.5 ± 7.2 | 42.3 ± 6.9 | 7.7 | 0.13 | <0.0001 |
| Inferior | 52.6 ± 6.2 | 51.3 ± 4.8 | 47.9 ± 7.9 | 46.8 ± 6.7 | 9.0 | 0.15 | <0.0001 |
| Inner plexiform layer (IPL) | |||||||
| Nasal | 42.8 ± 3.1 | 42.1 ± 3.2 | 40.3 ± 4.2 | 40.0 ± 4.6 | 4.5 | 0.080 | 0.0046 |
| Superior | 41.3 ± 2.9 | 40.7 ± 3.1 | 38.9 ± 4.9 | 39.4 ± 3.9 | 2.0 | 0.038 | 0.11 |
| Temporal | 40.5 ± 3.4 | 40.1 ± 3.3 | 39.2 ± 4.6 | 39.1 ± 3.8 | 1.3 | 0.024 | 0.024 |
| Inferior | 40.4 ± 3.8 | 40.6 ± 3.0 | 38.5 ± 3.9 | 38.4 ± 3.7 | 5.0 | 0.087 | 0.0024 |
| Retinal pigment epithelium (RPE) | |||||||
| Nasal | 83.0 ± 2.0 | 83.4 ± 2.3 | 83.0 ± 2.6 | 81.4 ± 3.1 | 6.0 | 0.11 | 0.0007 |
| Superior | 81.6 ± 2.4 | 82.4 ± 2.3 | 82.0 ± 2.8 | 80.7 ± 2.7 | 4.0 | 0.073 | 0.0092 |
| Temporal | 81.5 ± 1.9 | 82.1 ± 2.1 | 82.0 ± 2.4 | 80.6 ± 2.5 | 4.9 | 0.088 | 0.0027 |
| Inferior | 81.0 ± 2.1 | 81.4 ± 2.1 | 80.9 ± 2.4 | 79.7 ± 2.5 | 5.1 | 0.091 | 0.0023 |
| Parameter Estimate | 95% CI | R2 | p-Value | |
|---|---|---|---|---|
| Retina | ||||
| Nasal | −0.13 | −0.25 to −0.010 | 0.029 | 0.034 |
| Superior | −0.12 | −0.25 to 0.0051 | 0.023 | 0.060 |
| Temporal | −0.064 | −0.18 to 0.050 | 0.0079 | 0.27 |
| Inferior | −0.13 | −0.25 to −0.016 | 0.031 | 0.026 |
| Nerve fiber layer (NFL) | ||||
| Nasal | 0.035 | 0.018 to 0.053 | 0.091 | 0.0001 |
| Superior | 0.056 | 0.031 to 0.082 | 0.11 | <0.0001 |
| Temporal | 0.052 | 0.043 to 0.060 | 0.47 | <0.0001 |
| Inferior | 0.042 | 0.017 to 0.067 | 0.068 | 0.0011 |
| Ganglion cell layer (GCL) | ||||
| Nasal | −0.022 | −0.15 to −0.063 | 0.13 | <0.0001 |
| Superior | −0.082 | −0.12 to −0.040 | 0.089 | 0.0002 |
| Temporal | −0.096 | −0.14 to −0.054 | 0.12 | <0.0001 |
| Inferior | −0.10 | −0.14 to −0.059 | 0.13 | <0.0001 |
| Inner plexiform layer (IPL) | ||||
| Nasal | −0.047 | −0.075 to −0.018 | 0.064 | 0.0014 |
| Superior | −0.030 | −0.058 to −0.0029 | 0.030 | 0.031 |
| Temporal | −0.023 | −0.047 to 0.0024 | 0.021 | 0.076 |
| Inferior | −0.043 | −0.068 to −0.018 | 0.069 | 0.0009 |
| Retinal pigment epithelium (RPE) | ||||
| Nasal | −0.037 | −0.057 to −0.018 | 0.083 | 0.0003 |
| Superior | −0.026 | −0.045 to −0.0073 | 0.047 | 0.0068 |
| Temporal | −0.025 | −0.042 to −0.0082 | 0.053 | 0.0038 |
| Inferior | −0.032 | −0.049 to −0.015 | 0.081 | 0.0003 |
| Subgroups | ANOVA Summary | ||||||
|---|---|---|---|---|---|---|---|
| <20 Years | 20–44 Years | 45–69 Years | ≥70 Years | F | R2 | p-Value | |
| FAZ area (mm2) | 0.30 ± 0.13 | 0.34 ± 0.14 | 0.31 ± 0.12 | 0.32 ± 0.11 | 0.71 | 0.014 | 0.55 |
| SCP vascular density (%) | 36.4 ± 4.8 | 33.0 ± 6.6 | 28.4 ± 5.9 | 26.1 ± 6.9 | 15.2 | 0.23 | <0.0001 |
| DCP vascular density (%) | 32.1 ± 4.8 | 30.0 ± 6.0 | 26.2 ± 4.6 | 23.1 ± 4.8 | 18.0 | 0.26 | <0.0001 |
| Parameter Estimate | 95% CI | R2 | p-Value | |
|---|---|---|---|---|
| FAZ area | −0.00013 | −0.0010 to 0.00078 | 0.00053 | 0.77 |
| SCP vascular density | −0.15 | −0.20 to −0.11 | 0.22 | <0.0001 |
| DCP vascular density | −0.14 | −0.18 to −0.10 | 0.26 | <0.0001 |
| Parameter Estimate | 95% CI | p-Value | R2 | |
|---|---|---|---|---|
| Retina | ||||
| Superficial plexus | 1.5 | 0.98 to 2.0 | <0.0001 | 0.28 |
| Deep plexus | −0.55 | −1.2 to 0.052 | 0.073 | |
| NFL | ||||
| Superficial plexus | 0.19 | 0.11 to 0.26 | <0.0001 | 0.21 |
| Deep plexus | −0.29 | −0.38 to −0.20 | <0.0001 | |
| GCL | ||||
| Superficial plexus | 0.80 | 0.63 to 0.97 | <0.0001 | 0.42 |
| Deep plexus | −0.49 | −0.69 to −0.29 | <0.0001 | |
| IPL | ||||
| Superficial plexus | 0.44 | 0.34 to 0.55 | <0.0001 | 0.39 |
| Deep plexus | −0.25 | −0.37 to −0.13 | <0.0001 | |
| RPE | ||||
| Superficial plexus | 0.00044 | −0.095 to 0.096 | 0.99 | 0.0029 |
| Deep plexus | 0.022 | −0.092 to 0.14 | 0.71 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lever, M.; Chen, Y.; Glaser, M.; Unterlauft, J.D.; Lommatzsch, C.; Bechrakis, N.E.; Böhm, M.R.R. Microvascular and Morphologic Changes of the Macula over Lifetime. Life 2022, 12, 568. https://doi.org/10.3390/life12040568
Lever M, Chen Y, Glaser M, Unterlauft JD, Lommatzsch C, Bechrakis NE, Böhm MRR. Microvascular and Morphologic Changes of the Macula over Lifetime. Life. 2022; 12(4):568. https://doi.org/10.3390/life12040568
Chicago/Turabian StyleLever, Mael, Ying Chen, Moritz Glaser, Jan Darius Unterlauft, Claudia Lommatzsch, Nikolaos E. Bechrakis, and Michael R. R. Böhm. 2022. "Microvascular and Morphologic Changes of the Macula over Lifetime" Life 12, no. 4: 568. https://doi.org/10.3390/life12040568
APA StyleLever, M., Chen, Y., Glaser, M., Unterlauft, J. D., Lommatzsch, C., Bechrakis, N. E., & Böhm, M. R. R. (2022). Microvascular and Morphologic Changes of the Macula over Lifetime. Life, 12(4), 568. https://doi.org/10.3390/life12040568