
Use of Image-Guided Surgical Navigation during Resection of Locally Recurrent Rectal Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
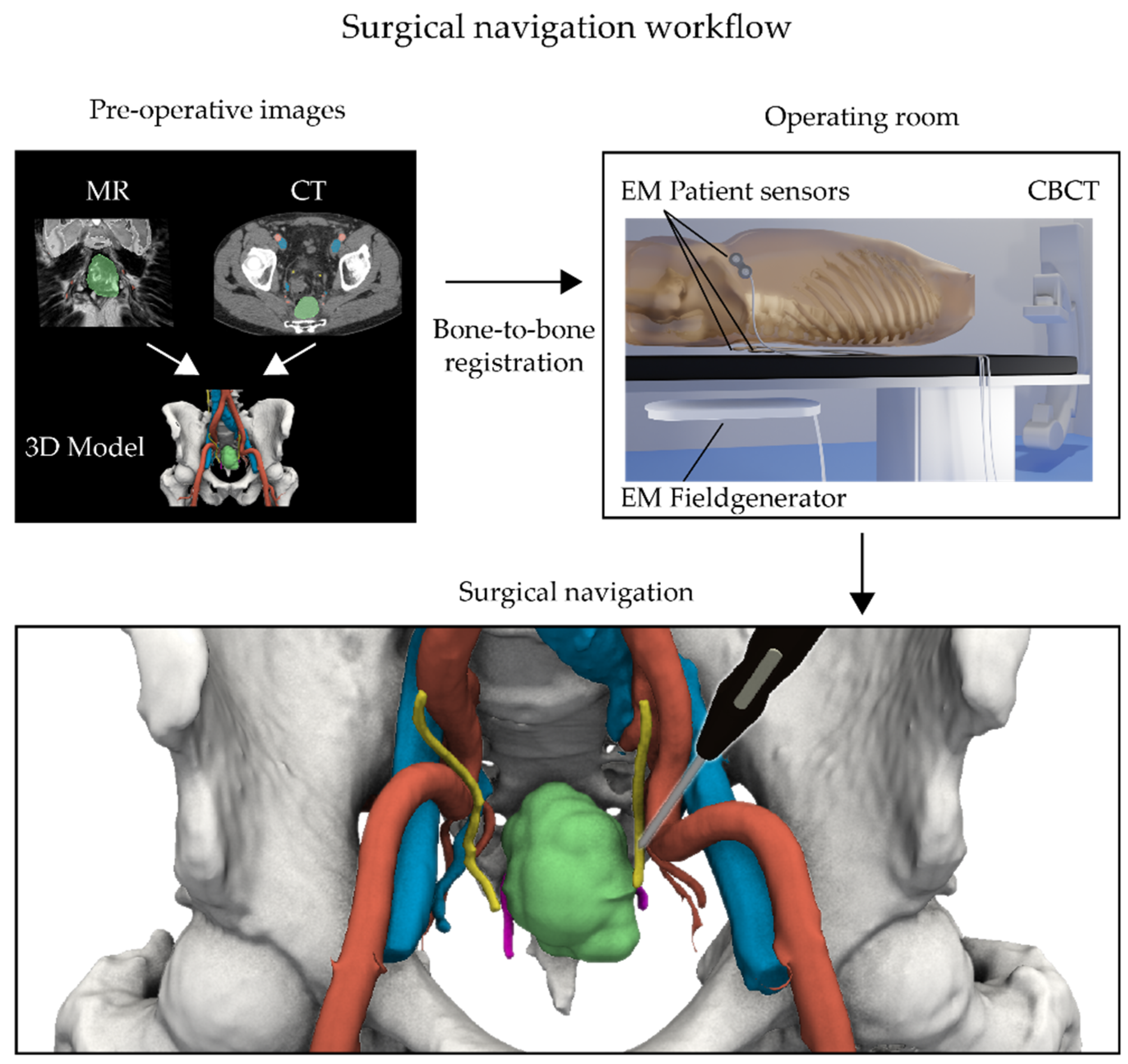
2.2. Surgical Navigation
2.3. Analysis
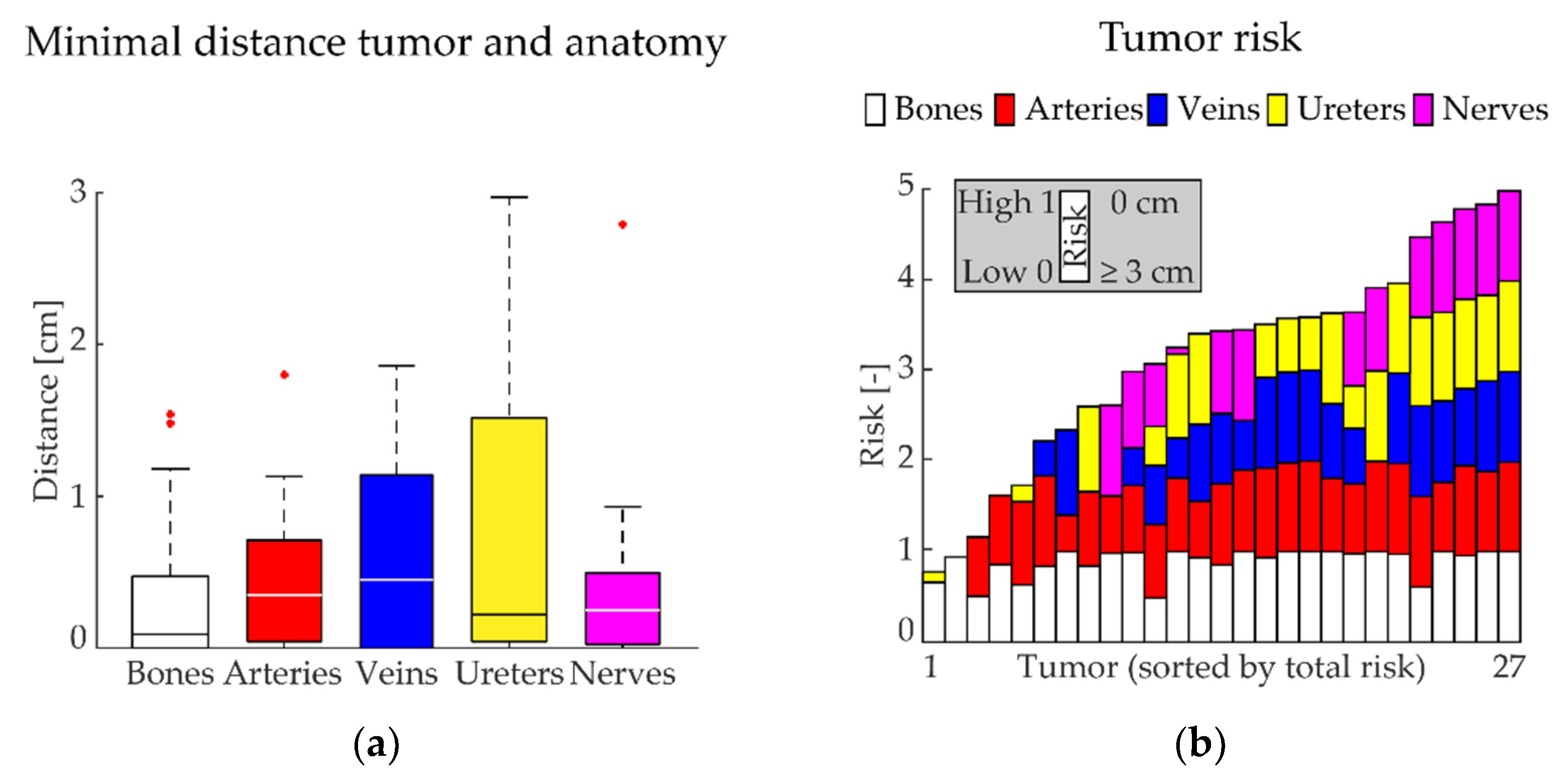
3. Results
3.1. Patient Characteristics
3.2. Surgical Navigation
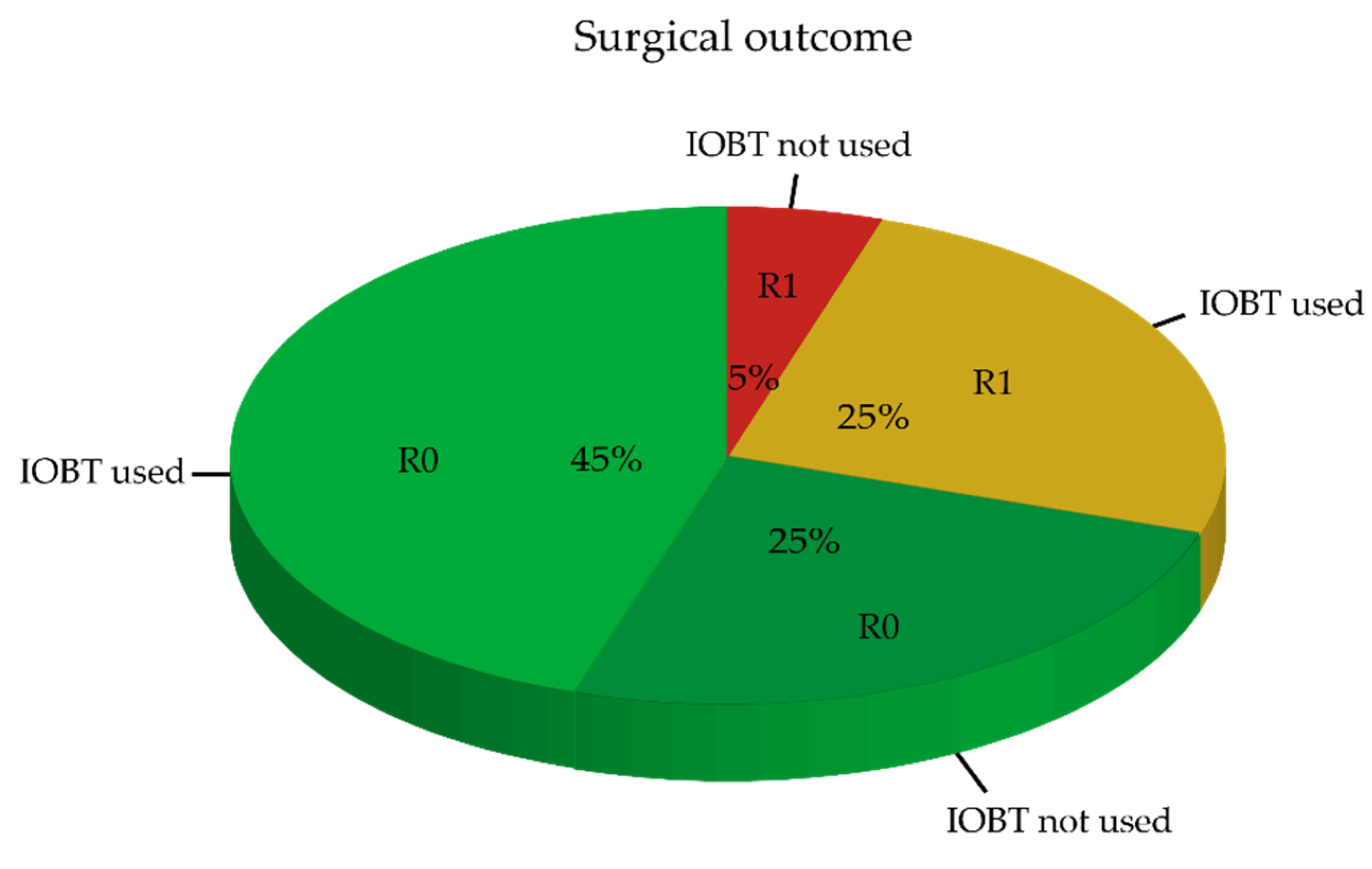
3.3. Surgical Outcome
3.4. Pathological Outcome
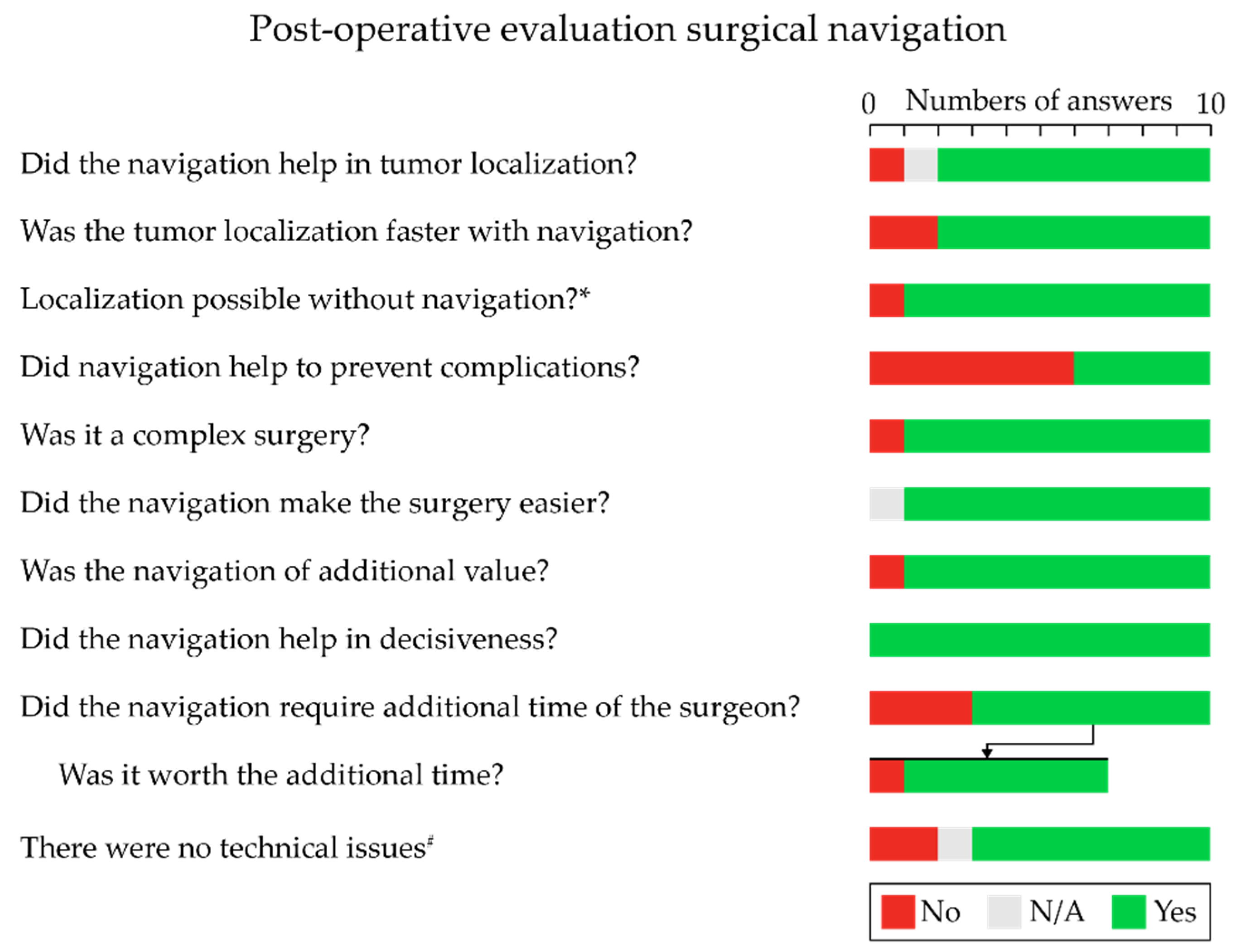
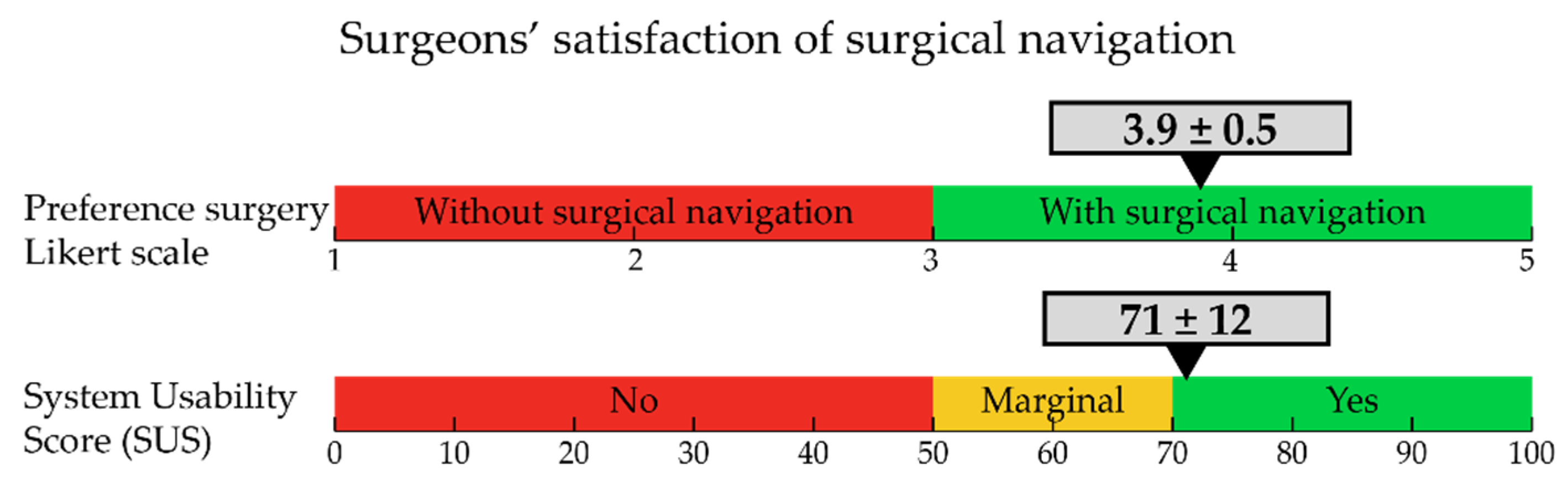
3.5. Surgeon Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rickles, A.S.; Dietz, D.W.; Chang, G.J.; Wexner, S.D.; Berho, M.E.; Remzi, F.H.; Greene, F.L.; Fleshman, J.W.; Abbas, M.A.; Peters, W.; et al. High Rate of Positive Circumferential Resection Margins Following Rectal Cancer Surgery: A Call to Action. Ann. Surg. 2015, 262, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Bonjer, H.J.; Deijen, C.L.; Abis, G.A.; Cuesta, M.A.; van der Pas, M.H.G.M.; de Lange-de Klerk, E.S.M.; Lacy, A.M.; Bemelman, W.A.; Andersson, J.; Angenete, E.; et al. A Randomized Trial of Laparoscopic versus Open Surgery for Rectal Cancer. N. Engl. J. Med. 2015, 372, 1324–1332. [Google Scholar] [CrossRef]
- Bosman, S.J.; Holman, F.A.; Nieuwenhuijzen, G.A.P.; Martijn, H.; Creemers, G.J.; Rutten, H.J.T. Feasibility of reirradiation in the treatment of locally recurrent rectal cancer. Br. J. Surg. 2014, 101, 1280–1289. [Google Scholar] [CrossRef] [PubMed]
- Cyr, D.P.; Zih, F.S.; Wells, B.J.; Swett-Cosentino, J.; Burkes, R.L.; Brierley, J.D.; Cummings, B.; Smith, A.J.; Swallow, C.J. Long-term outcomes following salvage surgery for locally recurrent rectal cancer: A 15-year follow-up study. Eur. J. Surg. Oncol. 2020, 46, 1131–1137. [Google Scholar] [CrossRef]
- Nielsen, M.; Rasmussen, P.; Pedersen, B.; Hagemann-Madsen, R.; Lindegaard, J.; Laurberg, S. Early and Late Outcomes of Surgery for Locally Recurrent Rectal Cancer: A Prospective 10-Year Study in the Total Mesorectal Excision Era. Ann. Surg. Oncol. 2015, 22, 2677–2684. [Google Scholar] [CrossRef]
- Gao, Z.; Gu, J. Surgical treatment of locally recurrent rectal cancer: A narrative review. Ann. Transl. Med. 2021, 9, 1026. [Google Scholar] [CrossRef]
- Kusters, M.; Dresen, R.C.; Martijn, H.; Nieuwenhuijzen, G.A.; van de Velde, C.J.H.; van den Berg, H.A.; Beets-Tan, R.G.H.; Rutten, H.J.T. Radicality of resection and survival after multimodality treatment is influenced by subsite of locally recurrent rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1444–1449. [Google Scholar] [CrossRef]
- Dresen, R.C.; Gosens, M.J.; Martijn, H.; Nieuwenhuijzen, G.A.; Creemers, G.J.; Daniels-Gooszen, A.W.; van den Brule, A.J.; van den Berg, H.A.; Rutten, H.J. Radical resection after IORT-containing multimodality treatment is the most important determinant for outcome in patients treated for locally recurrent rectal cancer. Ann. Surg. Oncol. 2008, 15, 1937–1947. [Google Scholar] [CrossRef]
- Alberda, W.J.; Verhoef, C.; Schipper, M.E.I.; Nuyttens, J.J.; Rothbarth, J.; De Wilt, J.H.W.; Burger, J.W.A. The Importance of a Minimal Tumor-Free Resection Margin in Locally Recurrent Rectal Cancer. Dis. Colon Rectum 2015, 58, 677–685. [Google Scholar] [CrossRef]
- Hagemans, J.A.W.; van Rees, J.M.; Alberda, W.J.; Rothbarth, J.; Nuyttens, J.J.M.E.; van Meerten, E.; Verhoef, C.; Burger, J.W.A. Locally recurrent rectal cancer; long-term outcome of curative surgical and non-surgical treatment of 447 consecutive patients in a tertiary referral centre. Eur. J. Surg. Oncol. 2020, 46, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Mannaerts, G.H.; Martijn, H.; Rutten, H.J.; Hanssens, P.E.; Wiggers, T. [Local tumor control and (disease-free) survival after surgery with pre- and intraoperative radiotherapy for primary non-resectable rectal carcinoma and local recurrence]. Ned. Tijdschr. Geneeskd. 2001, 145, 1460–1466. [Google Scholar] [PubMed]
- Holman, F.A.; Bosman, S.J.; Haddock, M.G.; Gunderson, L.L.; Kusters, M.; Nieuwenhuijzen, G.A.P.; van den Berg, H.; Nelson, H.; Rutten, H.J. Results of a pooled analysis of IOERT containing multimodality treatment for locally recurrent rectal cancer: Results of 565 patients of two major treatment centres. Eur. J. Surg. Oncol. 2017, 43, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Shuman, W.H.; Valliani, A.A.; Chapman, E.K.; Martini, M.L.; Neifert, S.N.; Baron, R.B.; Schupper, A.J.; Steinberger, J.M.; Caridi, J.M. Intraoperative Navigation in Spine Surgery: Effects on Complications and Reoperations. World Neurosurg. 2022, 160, e404–e411. [Google Scholar] [CrossRef] [PubMed]
- Mongen, M.A.; Willems, P.W.A. Current accuracy of surface matching compared to adhesive markers in patient-to-image registration. Acta Neurochir. 2019, 161, 865. [Google Scholar] [CrossRef]
- Elfring, R.; De La Fuente, M.; Radermacher, K. Assessment of optical localizer accuracy for computer aided surgery systems. Comput. Aided Surg. 2010, 15, 1–12. [Google Scholar] [CrossRef]
- Gumprecht, H.K.; Widenka, D.C.; Lumenta, C.B. BrainLab VectorVision Neuronavigation System: Technology and clinical experiences in 131 cases. Neurosurgery 1999, 44, 97–105. [Google Scholar] [CrossRef]
- Nijkamp, J.; Kuhlmann, K.; Sonke, J.-J.; Ruers, T. Image-guided navigation surgery for pelvic malignancies using electromagnetic tracking. In Proceedings of the Medical Imaging 2016: Image-Guided Procedures, Robotic Interventions, and Modeling; SPIE: San Diego, CA, USA, 2016; Volume 9786, p. 97862L. [Google Scholar]
- Nijkamp, J.; Kuhlmann, K.F.D.; Ivashchenko, O.; Pouw, B.; Hoetjes, N.; Lindenberg, M.A.; Aalbers, A.G.J.; Beets, G.L.; van Coevorden, F.; Kok, N.; et al. Prospective study on image-guided navigation surgery for pelvic malignancies. J. Surg. Oncol. 2019, 119, 510–517. [Google Scholar] [CrossRef]
- Kok, E.N.D.; van Veen, R.; Groen, H.C.; Heerink, W.J.; Hoetjes, N.J.; van Werkhoven, E.; Beets, G.L.; Aalbers, A.G.J.; Kuhlmann, K.F.D.; Nijkamp, J.; et al. Association of Image-Guided Navigation With Complete Resection Rate in Patients With Locally Advanced Primary and Recurrent Rectal Cancer. JAMA Netw. Open 2020, 3, e208522. [Google Scholar] [CrossRef]
- Reijers, S.J.M.; Heerink, W.J.; van Veen, R.; Nijkamp, J.; Hoetjes, N.J.; Schrage, Y.; van Akkooi, A.; Beets, G.L.; van Coevorden, F.; Ruers, T.J.M.; et al. Surgical navigation for challenging recurrent or pretreated intra-abdominal and pelvic soft tissue sarcomas. J. Surg. Oncol. 2021, 124, 1173–1181. [Google Scholar] [CrossRef]
- van Leeuwenhoek, A. Consent. Available online: https://www.avl.nl/ons-onderzoek-het-nederlands-kankerinstituut/consent/ (accessed on 16 December 2021).
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An Empirical Evaluation of the System Usability Scale. Intl. J. Hum. –Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.; Beets-Tan, R.G.H.; Lambregts, D.M.J.; Lammering, G.; Nelemans, P.J.; Engelen, S.M.E.; van Dam, R.M.; Jansen, R.L.H.; Sosef, M.; Leijtens, J.W.A.; et al. Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer. J. Clin. Oncol. 2011, 29, 4633–4640. [Google Scholar] [CrossRef]
- Martens, M.H.; Maas, M.; Heijnen, L.A.; Lambregts, D.M.J.; Leijtens, J.W.A.; Stassen, L.P.S.; Breukink, S.O.; Hoff, C.; Belgers, E.J.; Melenhorst, J.; et al. Long-term Outcome of an Organ Preservation Program After Neoadjuvant Treatment for Rectal Cancer. JNCI J. Natl. Cancer Inst. 2016, 108, djw171. [Google Scholar] [CrossRef]
- van der Valk, M.J.M.; Hilling, D.E.; Bastiaannet, E.; Meershoek-Klein Kranenbarg, E.; Beets, G.L.; Figueiredo, N.L.; Habr-Gama, A.; Perez, R.O.; Renehan, A.G.; van de Velde, C.J.H.; et al. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): An international multicentre registry study. Lancet 2018, 391, 2537–2545. [Google Scholar] [CrossRef]
- McCulloch, P.; Altman, D.G.; Campbell, W.B.; Flum, D.R.; Glasziou, P.; Marshall, J.C.; Nicholl, J. No surgical innovation without evaluation: The IDEAL recommendations. Lancet 2009, 374, 1105–1112. [Google Scholar] [CrossRef]
- Hirst, A.; Philippou, Y.; Blazeby, J.; Campbell, B.; Campbell, M.; Feinberg, J.; Rovers, M.; Blencowe, N.; Pennell, C.; Quinn, T.; et al. No Surgical Innovation Without Evaluation: Evolution and Further Development of the IDEAL Framework and Recommendations. Ann. Surg. 2019, 269, 211–220. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Value(s) | |
|---|---|
| Total | 20 |
| Sex | 10 male, 10 female |
| Age (years) at the surgery, median (min–max) | 60 (41–78) |
| Previous surgery | |
| No (complete response after “watch and wait”) * | 2 |
| Yes | 18 |
| Neoadjuvant treatment for the recurrent | |
| Chemotherapy | 1 |
| Chemoradiation | 12 |
| Chemoradiation + chemotherapy | 7 |
| Tumor location | |
| Pelvic wall/presacral/perineal | 15 |
| Staple line recurrence | 3 |
| Recurrence after “watch and wait” # | 2 |
| Type of surgical resection | |
| Open low anterior resection (LAR) | 4 |
| Open abdominoperineal resection (APR) | 5 |
| Extensive local resection | 5 |
| Pelvic exenteration | 6 |
| Value(s) | ||
|---|---|---|
| Successful surgical navigations | 20 (100%) | |
| Setup time surgical navigation (min) | 16 (9–20) | |
| CBCT scanner | ||
| Allura (hybrid operation room) | 15 | |
| Ziehm (mobile 3D C-arm) | 5 | |
| Manual fine-tuning registration during surgery | Yes | No |
| Fine-tune required | 17 | 3 |
| Left–Right (mm) | 3.0 (0–14) | 0 |
| Caudal–Cranial (mm) | 7.0 (0–20) | 0 |
| Posterior–Anterior (mm) | 3.0 (0–13) | 0 |
| Surgical position related to fine-tune | ||
| Straight | 4 | 2 |
| Supine split-leg position | 7 | 1 |
| Supine split-leg position, later leg holders | 1 | - |
| Leg holders | 4 | - |
| Prone | 1 | - |
| Navigation usage | ||
| Available (min) | 254 (104–553) | |
| Pointer used (min) | 13.7 (3.1–44.7) | |
| Relative pointer used (%) | 5.6% (1.1–12.5%) | |
| Value(s) | |
|---|---|
| Total | 27 |
| Tumors per patient | 1 (1–3) |
| Maximum size (cm) | 4.8 (1.5–12.1) |
| Volume (mL) | 10.0 (0.5–125.8) |
| Total risk (0–5) | 3.4 (0.8–5.0) |
| Value(s) | |
|---|---|
| Surgical time (h) | 7.5 (2.7–14.8) |
| Blood loss (mL) | 2350 (460–9300) |
| Intraoperative brachytherapy (IOBT) | |
| Not used | 6 |
| Used | 14 |
| Unexpected intraoperative events | |
| None | 19 |
| Bladder damage | 1 |
| Postoperative complications | |
| Navigation related | - |
| Non-navigation related | 13 |
| Clavien–Dindo | |
| I | 2 |
| II | 2 |
| III | - |
| IIIa | 1 |
| IIIb | 7 |
| IV | - |
| IVa | 1 |
| IVb | - |
| V | - |
| Hospitalization (days) | 8 (3–27) |
| Pathological evaluation | |
| Radical (R0) | 14 |
| Not radical (R1) | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Groen, H.C.; den Hartog, A.G.; Heerink, W.J.; Kuhlmann, K.F.D.; Kok, N.F.M.; van Veen, R.; Hiep, M.A.J.; Snaebjornsson, P.; Grotenhuis, B.A.; Beets, G.L.; et al. Use of Image-Guided Surgical Navigation during Resection of Locally Recurrent Rectal Cancer. Life 2022, 12, 645. https://doi.org/10.3390/life12050645
Groen HC, den Hartog AG, Heerink WJ, Kuhlmann KFD, Kok NFM, van Veen R, Hiep MAJ, Snaebjornsson P, Grotenhuis BA, Beets GL, et al. Use of Image-Guided Surgical Navigation during Resection of Locally Recurrent Rectal Cancer. Life. 2022; 12(5):645. https://doi.org/10.3390/life12050645
Chicago/Turabian StyleGroen, Harald C., Anne G. den Hartog, Wouter J. Heerink, Koert F. D. Kuhlmann, Niels F. M. Kok, Ruben van Veen, Marijn A. J. Hiep, Petur Snaebjornsson, Brechtje A. Grotenhuis, Geerard L. Beets, and et al. 2022. "Use of Image-Guided Surgical Navigation during Resection of Locally Recurrent Rectal Cancer" Life 12, no. 5: 645. https://doi.org/10.3390/life12050645
APA StyleGroen, H. C., den Hartog, A. G., Heerink, W. J., Kuhlmann, K. F. D., Kok, N. F. M., van Veen, R., Hiep, M. A. J., Snaebjornsson, P., Grotenhuis, B. A., Beets, G. L., Aalbers, A. G. J., & Ruers, T. J. M. (2022). Use of Image-Guided Surgical Navigation during Resection of Locally Recurrent Rectal Cancer. Life, 12(5), 645. https://doi.org/10.3390/life12050645