
A Prospective Approach to Integration of AI Fracture Detection Software in Radiographs into Clinical Workflow


Abstract
:1. Introduction
2. Materials and Methods
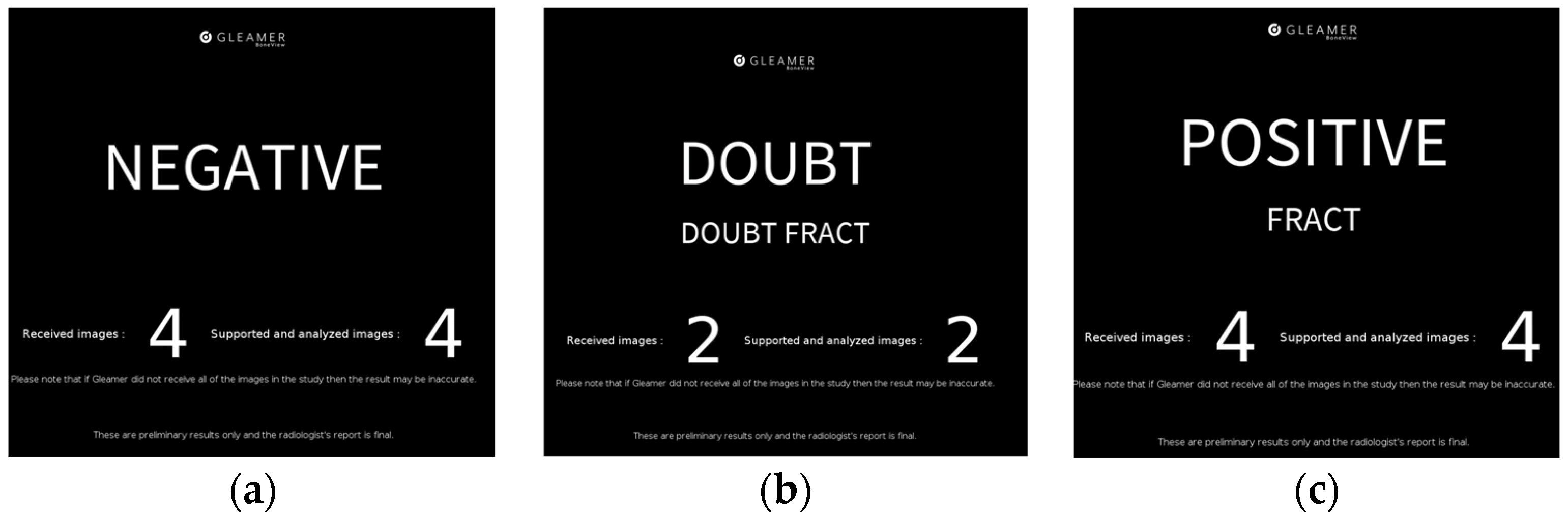
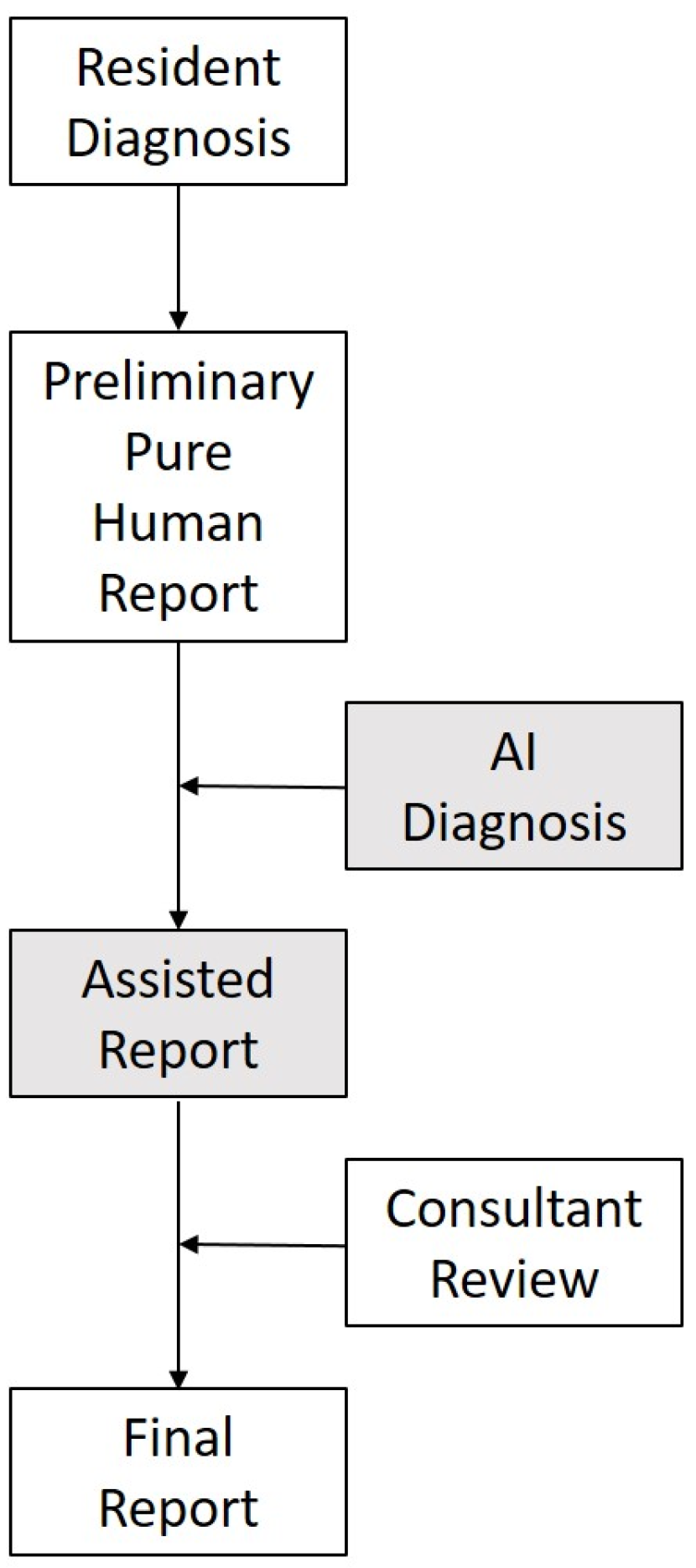
2.1. Integration into Clinical Workflow
2.2. Inclusion and Exclusion
- Full radiographic exam of one anatomic region with one or multiple images;
- Inquiry for fracture;
- Primary review by either of two residents.
- Exclusion Criteria:
- Follow-up imaging for known fractures;
- Skeletal radiographs with other inquiry (i.e., inflammatory disease, post-surgical radiographs, etc.);
- Non-processable radiographs: full chest radiographs, abdomen radiographs, cervical spine radiographs, radiographs of the skull or face.
2.3. Statistical Analysis
3. Results
3.1. Dataset
3.2. General Sensitivity and Specificity
3.3. Sensitivity and Specificity by Anatomical Region
3.4. Foreign Material
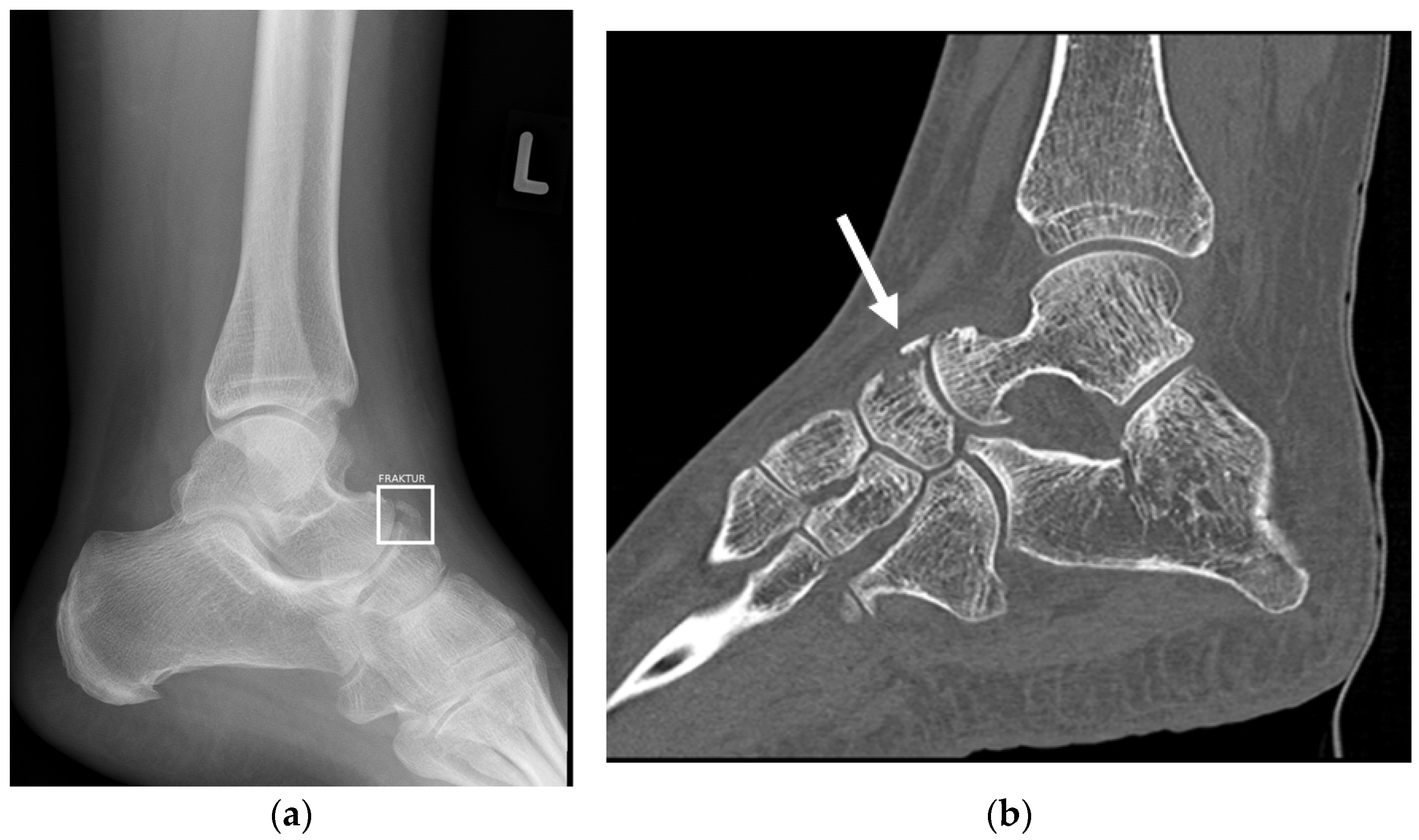
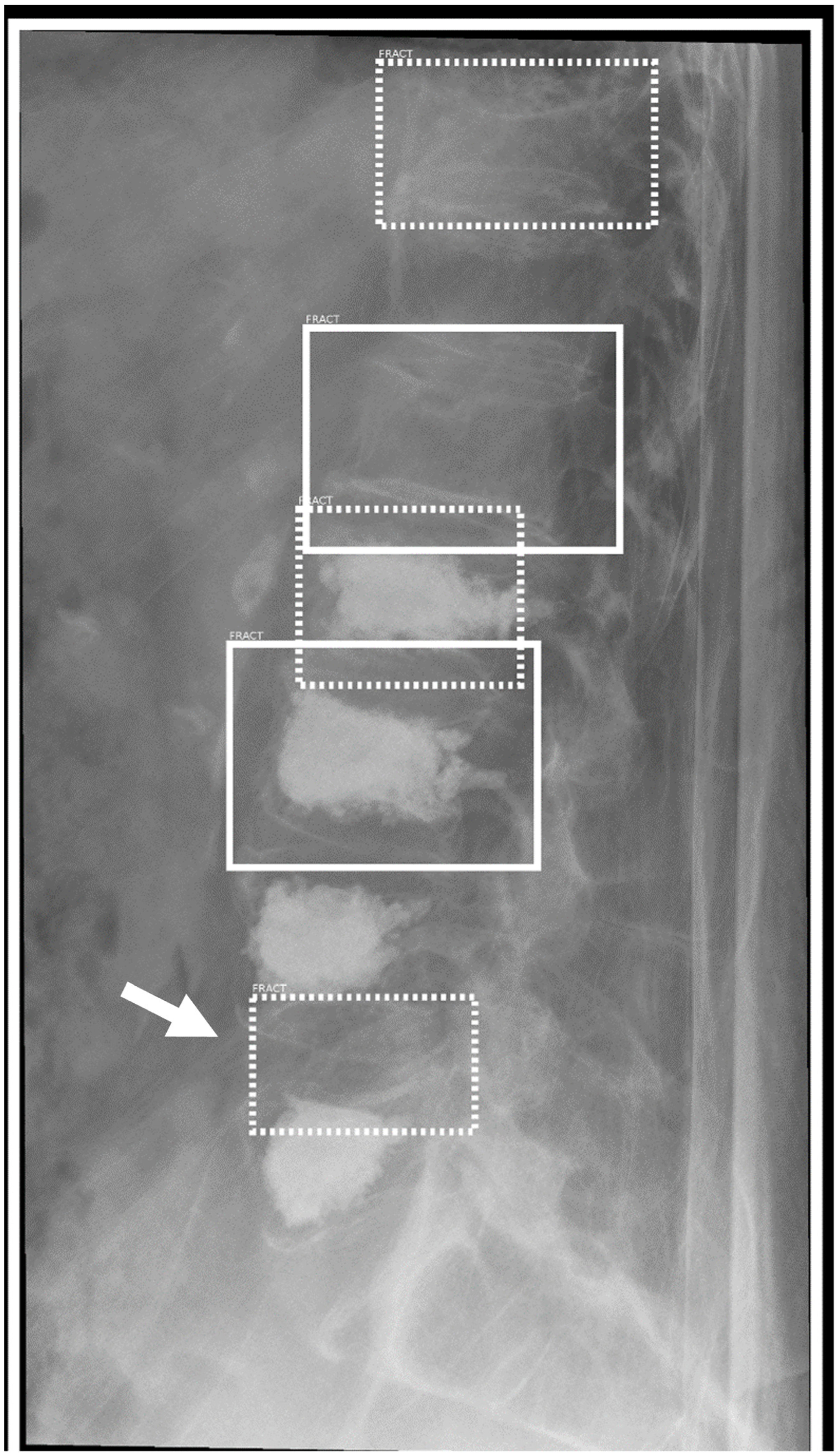
3.5. Obvious and Nonobvious Fracture
3.6. Fractures in Children
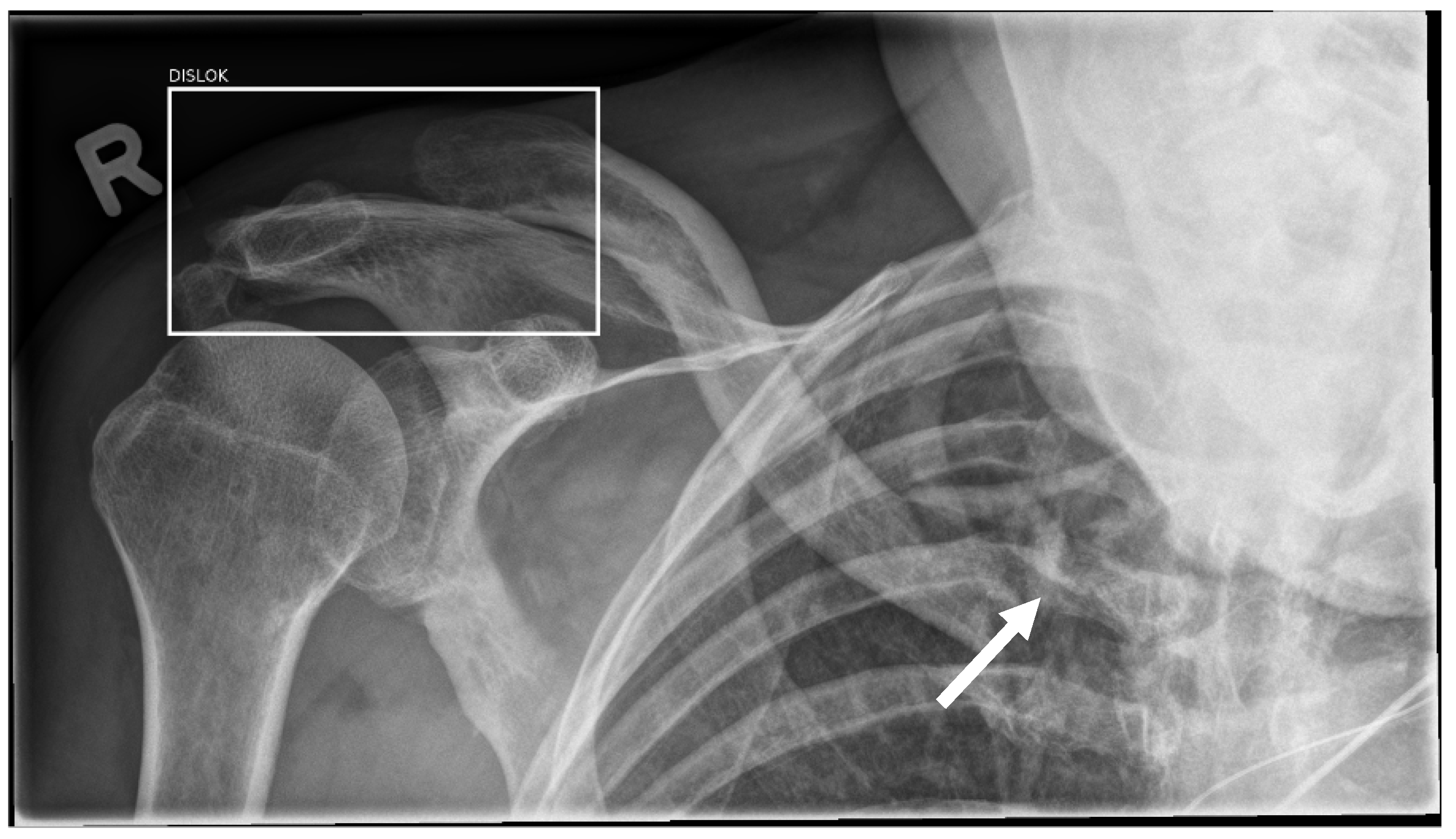
3.7. Effusion and Dislocation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjamens, S.; Dhunnoo, P.; Mesko, B. The State of Artificial Intelligence-based FDA-Approved Medical Devices and Algorithms: An Online Database. NPJ Digit. Med. 2020, 3, 118. [Google Scholar] [CrossRef] [PubMed]
- Artificial Intelligence and Machine Learning (AI/ML)-Enabled Medical Devices. Available online: https://www.fda.gov/medical-devices/software-medical-device-samd/artificial-intelligence-and-machine-learning-aiml-enabled-medical-devices (accessed on 21 October 2022).
- van Leeuwen, K.G.; Schalekamp, S.; Rutten, M.; van Ginneken, B.; de Rooij, M. Artificial Intelligence in Radiology: 100 Commercially Available Products and their Scientific Evidence. Eur. Radiol. 2021, 31, 3797–3804. [Google Scholar] [CrossRef]
- Guermazi, A.; Tannoury, C.; Kompel, A.J.; Murakami, A.M.; Ducarouge, A.; Gillibert, A.; Li, X.; Tournier, A.; Lahoud, Y.; Jarraya, M.; et al. Improving Radiographic Fracture Recognition Performance and Efficiency Using Artificial Intelligence. Radiology 2021, 302, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Duron, L.; Ducarouge, A.; Gillibert, A.; Laine, J.; Allouche, C.; Cherel, N.; Zhang, Z.; Nitche, N.; Lacave, E.; Pourchot, A.; et al. Assessment of an AI Aid in Detection of Adult Appendicular Skeletal Fractures by Emergency Physicians and Radiologists: A Multicenter Cross-sectional Diagnostic Study. Radiology 2021, 300, 120–129. [Google Scholar] [CrossRef]
- Wei, C.J.; Tsai, W.C.; Tiu, C.M.; Wu, H.T.; Chiou, H.J.; Chang, C.Y. Systematic Analysis of Missed Extremity Fractures in Emergency Radiology. Acta Radiol. 2006, 47, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Hallas, P.; Ellingsen, T. Errors in Fracture Diagnoses in the Emergency Department--Characteristics of Patients and Diurnal Variation. BMC Emerg. Med. 2006, 6, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, A.; Berritto, D.; Russo, A.; Riccitiello, F.; Caruso, M.; Belfiore, M.P.; Papapietro, V.R.; Carotti, M.; Pinto, F.; Giovagnoni, A.; et al. Traumatic Fractures in Adults: Missed Diagnosis on Plain Radiographs in the Emergency Department. Acta Biomed. 2018, 89, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Wood, G.; Knapp, K.M.; Rock, B.; Cousens, C.; Roobottom, C.; Wilson, M.R. Visual Expertise in Detecting and Diagnosing Skeletal Fractures. Skeletal Radiol. 2013, 42, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Whang, J.S.; Baker, S.R.; Patel, R.; Luk, L.; Castro, A., 3rd. The Causes of Medical Malpractice Suits Against Radiologists in the United States. Radiology 2013, 266, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, D.; Kompel, A.J.; Ventre, J.; Ducarouge, A.; Nguyen, T.; Regnard, N.E.; Guermazi, A. Automated Detection of Acute Appendicular Skeletal Fractures in Pediatric Patients using Deep Learning. Skeletal Radiol. 2022, 51, 2129–2139. [Google Scholar] [CrossRef]
- Nguyen, T.; Maarek, R.; Hermann, A.L.; Kammoun, A.; Marchi, A.; Khelifi-Touhami, M.R.; Collin, M.; Jaillard, A.; Kompel, A.J.; Hayashi, D.; et al. Assessment of an Artificial Intelligence Aid for the Detection of Appendicular Skeletal Fractures in Children and Young Adults by Senior and Junior Radiologists. Pediatr Radiol. 2022, 52, 2215–2226. [Google Scholar] [CrossRef] [PubMed]
- Kuo, R.Y.L.; Harrison, C.; Curran, T.A.; Jones, B.; Freethy, A.; Cussons, D.; Stewart, M.; Collins, G.S.; Furniss, D. Artificial Intelligence in Fracture Detection: A Systematic Review and Meta-Analysis. Radiology 2022, 304, 211785. [Google Scholar] [CrossRef]
- Bluthgen, C.; Becker, A.S.; Vittoria de Martini, I.; Meier, A.; Martini, K.; Frauenfelder, T. Detection and Localization of Distal Radius Fractures: Deep Learning System Versus Radiologists. Eur. J. Radiol. 2020, 126, 108925. [Google Scholar] [CrossRef]
- Lindsey, R.; Daluiski, A.; Chopra, S.; Lachapelle, A.; Mozer, M.; Sicular, S.; Hanel, D.; Gardner, M.; Gupta, A.; Hotchkiss, R.; et al. Deep Neural Network Improves Fracture Detection by Clinicians. Proc. Natl. Acad. Sci. USA 2018, 115, 11591–11596. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.T.; Wang, Y.; Chen, H.W.; Hsiao, P.M.; Yeh, C.N.; Hsieh, C.H.; Miao, S.; Xiao, J.; Liao, C.H.; Lu, L. A Scalable Physician-level Deep Learning Algorithm Detects Universal Trauma on Pelvic Radiographs. Nat. Commun. 2021, 12, 1066. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | ||
|---|---|---|---|---|---|
| Full set | Human | 84.74% (±0.4) | 97.11% (±0.01) | 93.11% (±0.03) | 93.24% (±0.02) |
| AI only | 86.92% (±0.03) | 84.67% (±0.03) | 72.33% (±0.04) | 93.35% (±0.02) | |
| Combined | 91.28% (±0.03) | 97.36% (±0.01) | 94.10% (±0.02) | 96.03% (±0.01) | |
| Reviewer 1 | Human | 85.85% (±0.05) | 97.29% (±0.01) | 93.41% (±0.03) | 93.90% (±0.02) |
| AI only | 84.34% (±0.05) | 84.49% (±0.03) | 76.61% (±0.06) | 92.67% (±0.02) | |
| Combined | 90.91% (±0.04) | 97.98% (±0.01) | 95.24% (±0.03) | 96.02 (±0.02) | |
| Reviewer 2 | Human | 83.43% (±0.06) | 96.88% (±0.02) | 92.76% (±0.04) | 92.43% (±0.03) |
| AI only | 89.94% (±0.05) | 79.89% (±0.04) | 68.16% (±0.06) | 93.31% (±0.03) | |
| Combined | 91.71% (±0.04) | 96.60% (±0.02) | 92.81% (±0.04) | 96.06% (±0.02) |
| Human Only | AI Only | Combined | ||||
|---|---|---|---|---|---|---|
| Region | Sensitivity | Specificity | Sensitivity | Sensitivity | Sensitivity | Sensitivity |
| Spine | 92.39% | 98.43% | 89.13% | 62.20% | 94.57% | 100.00% |
| Ribs | 64.29% | 91.89% | 78.57% | 72.97% | 78.57% | 91.89% |
| Shoulder/clavicle | 88.89% | 96.88% | 91.11% | 84.38% | 93.33% | 96.88% |
| Elbow/arm | 76.00% | 96.55% | 80.00% | 89.66% | 88.00% | 96.55% |
| Wrist/hand | 78.26% | 96.06% | 86.96% | 89.76% | 95.65% | 95.28% |
| Hip/pelvis | 93.22% | 99.79% | 88.13% | 89.76% | 93.22% | 98.79% |
| Knee/leg | 86.96% | 97.74% | 86.96% | 93.98% | 91.30% | 98.50% |
| Ankle/foot | 82.86% | 95.58% | 88.57% | 88.50% | 88.57% | 95.58% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oppenheimer, J.; Lüken, S.; Hamm, B.; Niehues, S.M. A Prospective Approach to Integration of AI Fracture Detection Software in Radiographs into Clinical Workflow. Life 2023, 13, 223. https://doi.org/10.3390/life13010223
Oppenheimer J, Lüken S, Hamm B, Niehues SM. A Prospective Approach to Integration of AI Fracture Detection Software in Radiographs into Clinical Workflow. Life. 2023; 13(1):223. https://doi.org/10.3390/life13010223
Chicago/Turabian StyleOppenheimer, Jonas, Sophia Lüken, Bernd Hamm, and Stefan Markus Niehues. 2023. "A Prospective Approach to Integration of AI Fracture Detection Software in Radiographs into Clinical Workflow" Life 13, no. 1: 223. https://doi.org/10.3390/life13010223
APA StyleOppenheimer, J., Lüken, S., Hamm, B., & Niehues, S. M. (2023). A Prospective Approach to Integration of AI Fracture Detection Software in Radiographs into Clinical Workflow. Life, 13(1), 223. https://doi.org/10.3390/life13010223