

The PEA Bead Test as a Screening Tool for Olfactory Dysfunction: A Preliminary Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sniffing Bead Test
2.3. YOF Test
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hummel, T.; Podlesek, D. Clinical Assessment of Olfactory Function. Chem. Senses 2021, 46, bjab053. [Google Scholar] [CrossRef] [PubMed]
- Albers, M.W.; Tabert, M.H.; Devanand, D.P. Olfactory Dysfunction as a Predictor of Neurodegenerative Disease. Curr. Neurol. Neurosci. Rep. 2006, 6, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, L.; Schriever, V.A.; Croy, I. Human Olfactory Dysfunction: Causes and Consequences. Cell Tissue Res. 2021, 383, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Karamali, K.; Elliott, M.; Hopkins, C. COVID-19 Related Olfactory Dysfunction. Curr. Opin. Otolaryngol. Head. Neck Surg. 2022, 30, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.G.; Kim, J.; Nam, J.S.; Park, J.J.; Cho, H.J.; Yoon, J.H.; Kim, C.H. Development of a Korean Culture-Friendly Olfactory Function Test and Optimization of a Diagnostic Cutoff Value. Clin. Exp. Otorhinolaryngol. 2020, 13, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.C.; Simões, J.; Silva, F.; Silva, E.D.; Hummel, C.; Hummel, T.; Paiva, A. Cultural Adaptation of the Portuguese Version of the “Sniffin’ Sticks” Smell Test: Reliability, Validity, and Normative Data. PLoS ONE 2016, 11, e0148937. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wang, Z.; Zhao, C.; Wei, X. Applicability of Sniffin’ Sticks Identification Test as a Screening Tool for Olfactory Dysfunction in Northeast China. Med. Sci. Monit. 2023, 29, e938903. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, H.S.; Kim, M.; Kim, S.H.; Cho, S.W.; Kim, J.Y. Validation of Olfactory Questionnaire in Koreans: An Alternative for Conventional Psychophysical Olfactory Tests. J. Korean Med. Sci. 2021, 36, e34. [Google Scholar] [CrossRef]
- Niklassen, A.S.; Christensen, K.B.; Fjaeldstad, A.W.; Ovesen, T. Development and Psychometric Validation of the Taste And Smell Tool for Evaluation (TASTE) Questionnaire. JAMA Otolaryngol. Head. Neck Surg. 2022, 148, 1164–1172. [Google Scholar] [CrossRef]
- Guo, Y.; Wu, D.; Sun, Z.; Yao, L.; Liu, J.; Wei, Y. Prognostic Value of Olfactory Evoked Potentials in Patients with Post-infectious Olfactory Dysfunction. Eur. Arch. Otorhinolaryngol. 2021, 278, 3839–3846. [Google Scholar] [CrossRef]
- Kamrava, S.K.; Hosseini, S.F.; Farhadi, M.; Jalessi, M.; Talebi, A.; Amini, E.; Alizadeh, R. Cultural Adaptation of the Iranian Version of the “Sniffin’ Sticks” Olfactory Test. Med. J. Islam. Repub. Iran. 2021, 35, 153. [Google Scholar] [CrossRef]
- Hedner, M.; Larsson, M.; Arnold, N.; Zucco, G.M.; Hummel, T. Cognitive Factors in Odor Detection, Odor Discrimination, and Odor Identification Tasks. J. Clin. Exp. Neuropsychol. 2010, 32, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Whitcroft, K.L.; Cuevas, M.; Haehner, A.; Hummel, T. Patterns of Olfactory Impairment Reflect Underlying Disease Etiology. Laryngoscope 2017, 127, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, J.W.; Keller, A.; Wong, M.; Jiang, R.S.; Vosshall, L.B. SMELL-S and SMELL-R: Olfactory Tests Not Influenced by Odor-specific Insensitivity or Prior Olfactory Experience. Proc. Natl. Acad. Sci. USA 2017, 114, 11275–11284. [Google Scholar] [CrossRef] [PubMed]
- Min, H.J.; Kim, S.M.; Han, D.H.; Kim, K.S. The Sniffing Bead System, an Olfactory Dysfunction Screening Tool for Geriatric Subjects: A Cross-sectional Study. BMC Geriatr. 2021, 21, 54. [Google Scholar] [CrossRef] [PubMed]
- Attems, J.; Walker, L.; Jellinger, K.A. Olfaction and Aging: A Mini-Review. Gerontology 2015, 61, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.A. On the Interpretation of Χ2 from Contingency Tables, and the Calculation of P. J. R. Stat. Soc. 1922, 85, 87–94. [Google Scholar] [CrossRef]
- Fawcett, T. An Introduction to ROC Analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Patel, Z.M.; Holbrook, E.H.; Turner, J.H.; Adappa, N.D.; Albers, M.W.; Altundag, A.; Appenzeller, S.; Costanzo, R.M.; Croy, I.; Davis, G.E.; et al. International Consensus Statement on Allergy and Rhinology: Olfaction. Int. Forum Allergy Rhinol. 2022, 12, 327–680. [Google Scholar] [CrossRef]
- Eibenstein, A.; Fioretti, A.B.; Lena, C.; Rosati, N.; Amabile, G.; Fusetti, M. Modern Psychophysical Tests to Assess Olfactory Function. Neurol. Sci. 2005, 26, 147–155. [Google Scholar] [CrossRef]
- Eibenstein, A.; Fioretti, A.B.; Lena, C.; Rosati, N.; Ottaviano, I.; Fusetti, M. Olfactory Screening Test: Experience in 102 Italian subjects. Acta Otorhinolaryngol. Ital. 2005, 25, 18–22. [Google Scholar]
- Mueller, C.; Renner, B. A New Procedure for the Short Screening of Olfactory Function Using Five Items from the “Sniffin’ Sticks” Identification Test Kit. Am. J. Rhinol. 2006, 20, 113–116. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Fukazawa, K.; Fujii, M.; Takayasu, S.; Muto, T.; Saito, S.; Takashima, Y.; Sakagami, M. Usefulness of the Odor Stick Identification Test for Japanese Patients with Olfactory Dysfunction. Chem. Senses 2004, 29, 565–571. [Google Scholar] [CrossRef]
- Wilson, D.A.; Stevenson, R.J. Olfactory Perceptual Learning: The Critical Role of Memory in Odor Discrimination. Neurosci. Biobehav. Rev. 2003, 27, 307–328. [Google Scholar] [CrossRef]
- Iannilli, E.; Leopold, D.A.; Hornung, D.E.; Hummel, T. Advances in Understanding Parosmia: An fMRI Study. ORL J. Otorhinolaryngol. Relat. Spec. 2019, 81, 185–192. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Anosmia (n = 35) | Hyposmia (n = 26) | Normosmia (n = 78) | p Value |
|---|---|---|---|---|
| Age | 52.71 (18.8) | 56.62 (17.95) | 43.4 (17.69) | 0.004 |
| Sex | 0.89 | |||
| Male | 24 (68.6%) | 17 (65.4%) | 50 (64.1%) | |
| Female | 11 (31.4%) | 9 (34.6%) | 28 (35.9%) | |
| Diabetes | 0.21 | |||
| Yes | 5 (14.3%) | 1 (3.8%) | 4 (5.1%) | |
| No | 30 (85.7%) | 25 (96.2%) | 74 (94.9%) | |
| Hypertension | 0.3 | |||
| Yes | 8 (22.9%) | 3 (11.5%) | 9 (11.5%) | |
| No | 27 (77.1%) | 23 (88.5%) | 69 (88.5%) | |
| Smoking | 0.06 | |||
| Yes | 21 (60%) | 8 (30.8) | 32 (41%) | |
| No | 14 (40%) | 18 (69.2%) | 46 (59%) | |
| Gustatory dysfunction | <0.001 | |||
| Yes | 18 (51.4%) | 8 (30.8%) | 8 (10.3%) | |
| No | 17 (48.6%) | 18 (69.2%) | 70 (89.7%) | |
| PEA bead test | 0.26 (0.89) | 2.38 (1.83) | 3.73 (1.76) | <0.001 |
| Model | Variable | Beta | SE | 95% Confidence Interval | p Value | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| 1 | Threshold score, R2 = 0.39 | |||||
| (Intercept) | 1.863 | 0.485 | 0.901 | 2.826 | 0.000 *** | |
| Gustatory dysfunction | −1.258 | 0.676 | −2.6 | 0.084 | 0.066 | |
| PEA bead test | 0.826 | 0.125 | 0.578 | 1.075 | 0.000 *** | |
| 2 | Discrimination score, R2 = 0.34 | |||||
| (Intercept) | 7.465 | 0.347 | 6.287 | 8.643 | 0.000 *** | |
| Age | −0.021 | 0.01 | −0.042 | −0.001 | 0.044 * | |
| Diabetes | −2.147 | 0.832 | −3.799 | −0.495 | 0.011 * | |
| Gustatory dysfunction | −1.359 | 0.462 | −2.277 | −0.442 | 0.004 ** | |
| PEA bead test | 0.375 | 0.086 | 0.204 | 0.546 | 0.000 *** | |
| 3 | Identification score, R2 = 0.42 | |||||
| (Intercept) | 7.9 | 0.472 | 6.962 | 8.837 | 0.000 *** | |
| Hypertension | −1.88 | 0.764 | −3.397 | −0.363 | 0.016 * | |
| Gustatory dysfunction | −1.851 | 0.64 | −3.122 | −0.581 | 0.005 ** | |
| PEA bead test | 0.725 | 0.119 | 0.49 | 0.96 | 0.000 *** | |
| 4 | TDI score, R2 = 0.55 | |||||
| (Intercept) | 18.705 | 1.547 | 15.633 | 21.777 | 0.000 *** | |
| Age | −0.06 | 0.027 | −0.112 | −0.006 | 0.030 * | |
| Gustatory dysfunction | −4.172 | 1.209 | −6.574 | −1.77 | 0.001 *** | |
| PEA bead test | 1.818 | 0.224 | 1.372 | 2.264 | 0.000 *** | |
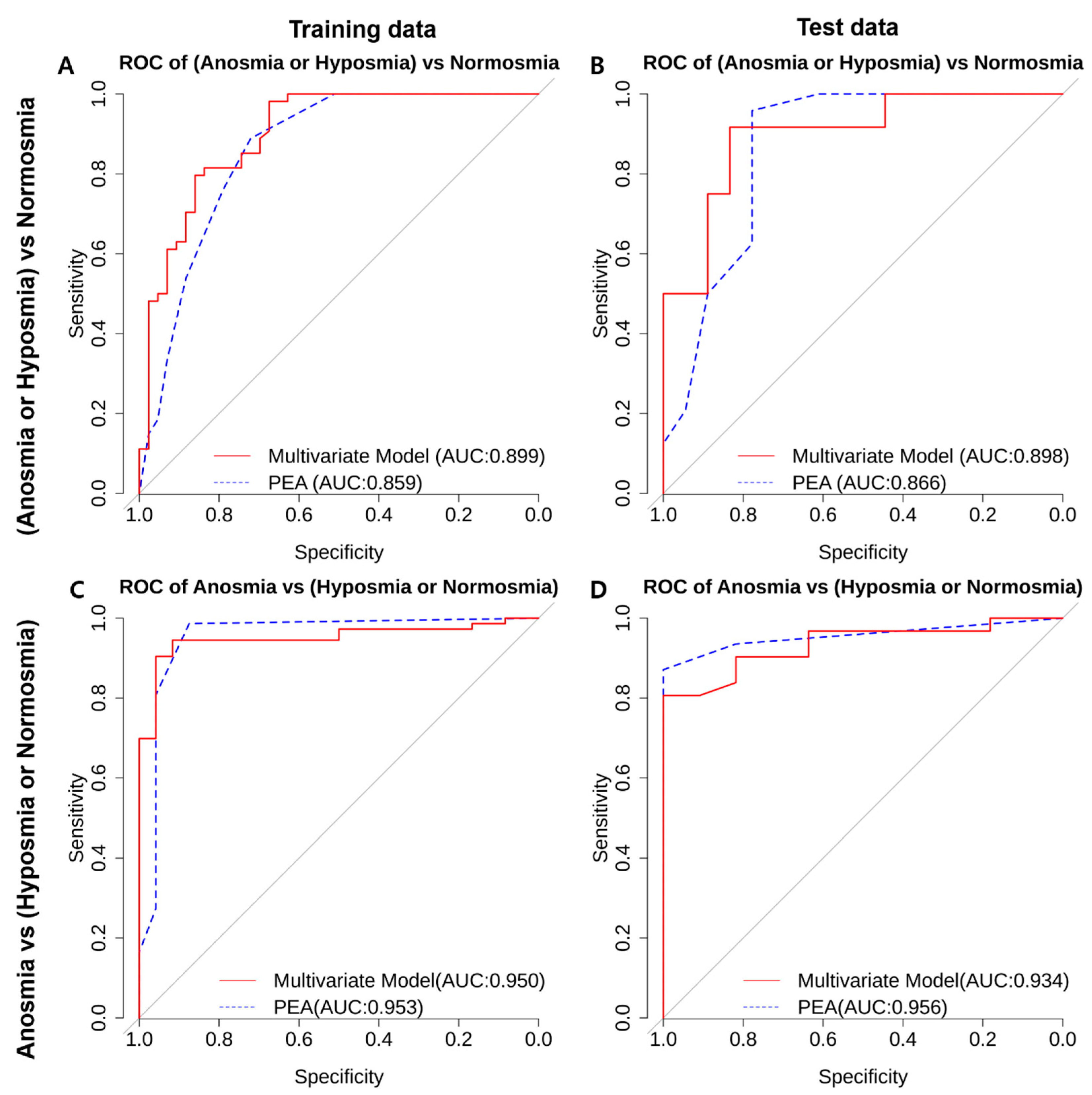
| Model | Cutoff Value | AUC | Sensitivity | Specificity | |
|---|---|---|---|---|---|
| Combined anosmia-hyposmia vs. normosmia | Multivariate | TDI > 18.5 | 0.898 (0.802–0.994) | 0.83 | 0.917 |
| PEA bead test | PEA ≥ 1 | 0.866 (0.739–0.992) | 0.778 | 0.958 | |
| Anosmia vs. combined hyposmia-normosmia) | Multivariate | TDI > 18.5 | 0.934 (0.862–1) | 1 | 0.806 |
| PEA bead test | PEA ≥ 2 | 0.956 (0.902–1) | 1 | 0.871 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.S.; Kwak, I.-Y.; Min, H.J. The PEA Bead Test as a Screening Tool for Olfactory Dysfunction: A Preliminary Study. Life 2023, 13, 2074. https://doi.org/10.3390/life13102074
Kim KS, Kwak I-Y, Min HJ. The PEA Bead Test as a Screening Tool for Olfactory Dysfunction: A Preliminary Study. Life. 2023; 13(10):2074. https://doi.org/10.3390/life13102074
Chicago/Turabian StyleKim, Kyung Soo, Il-Youp Kwak, and Hyun Jin Min. 2023. "The PEA Bead Test as a Screening Tool for Olfactory Dysfunction: A Preliminary Study" Life 13, no. 10: 2074. https://doi.org/10.3390/life13102074
APA StyleKim, K. S., Kwak, I. -Y., & Min, H. J. (2023). The PEA Bead Test as a Screening Tool for Olfactory Dysfunction: A Preliminary Study. Life, 13(10), 2074. https://doi.org/10.3390/life13102074