
Point-of-Care Testing for Hepatitis Viruses: A Growing Need


Abstract
:1. Introduction
2. Point-of-Care Testing
2.1. Overview
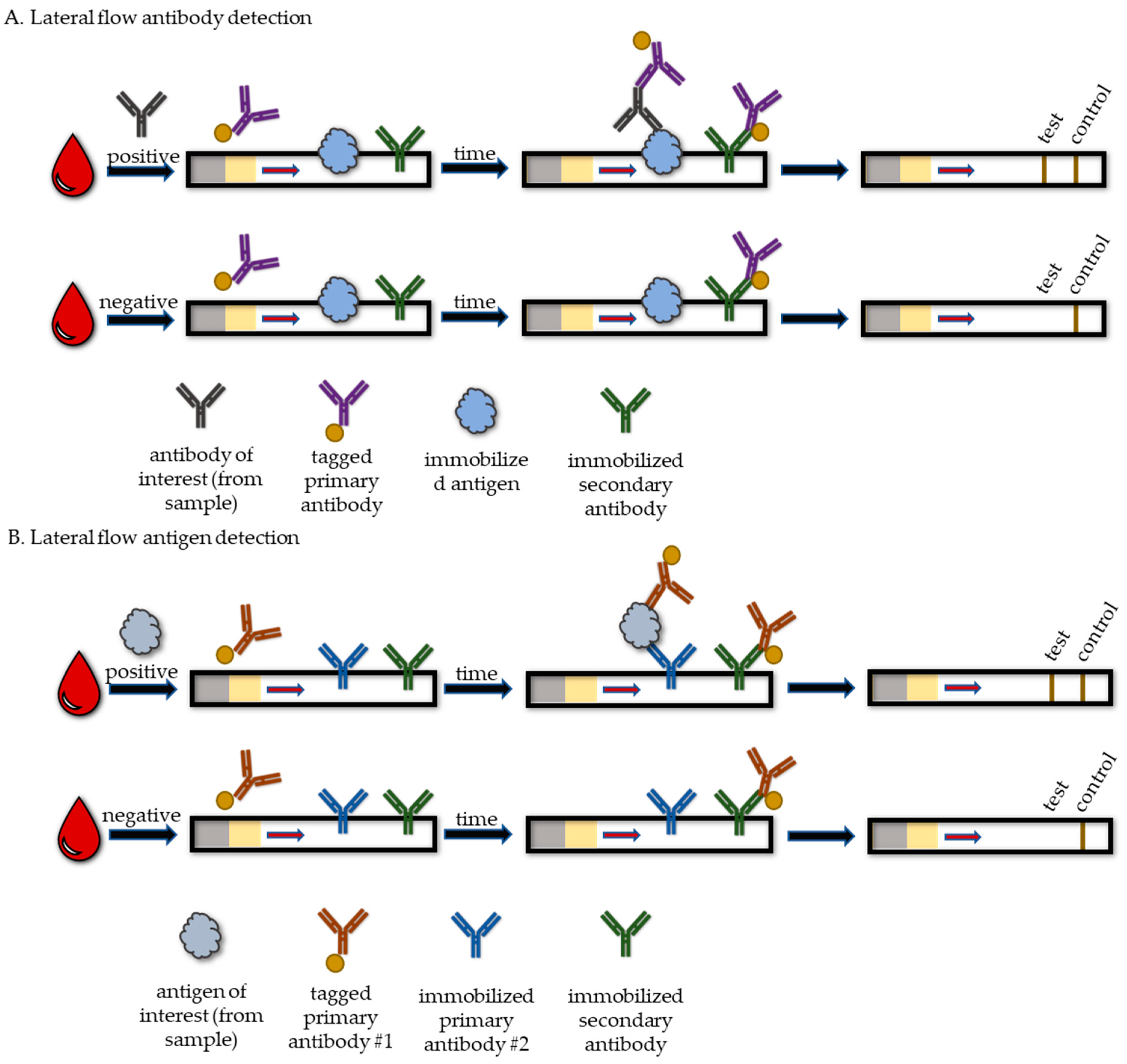
2.2. Lateral Flow Tests
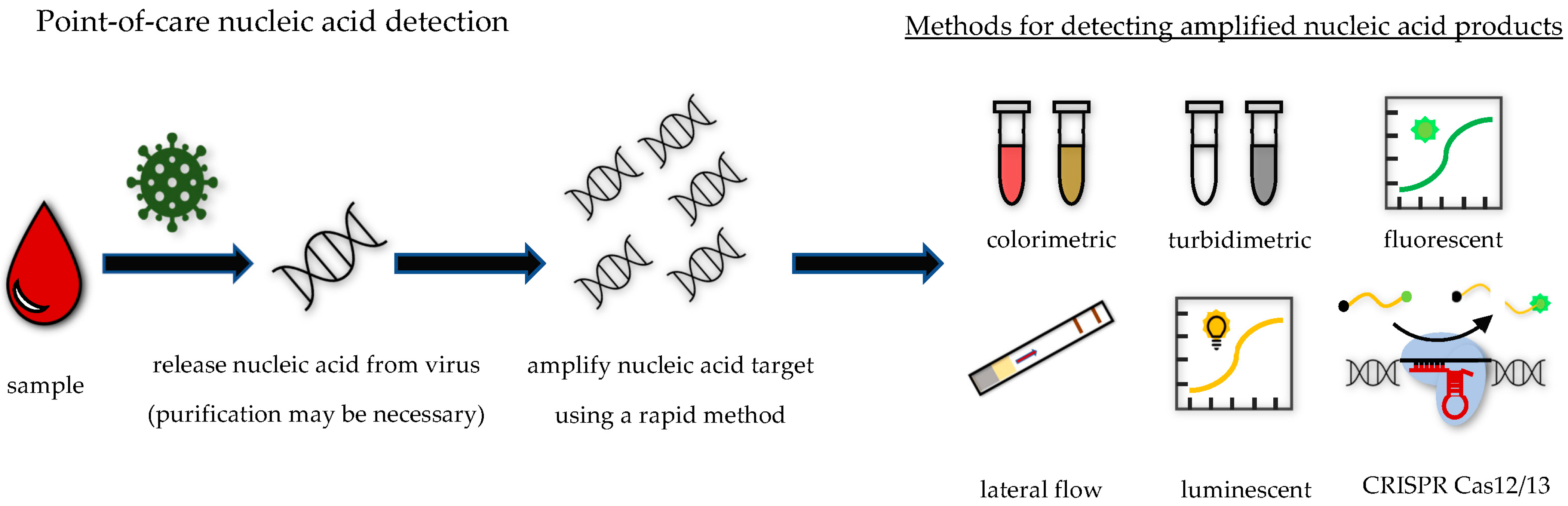
2.3. POC Nucleic Acid Tests
2.4. Multiplex Tests
3. Tests by Viral Agent
3.1. Hepatitis A Virus
3.2. Hepatitis B Virus
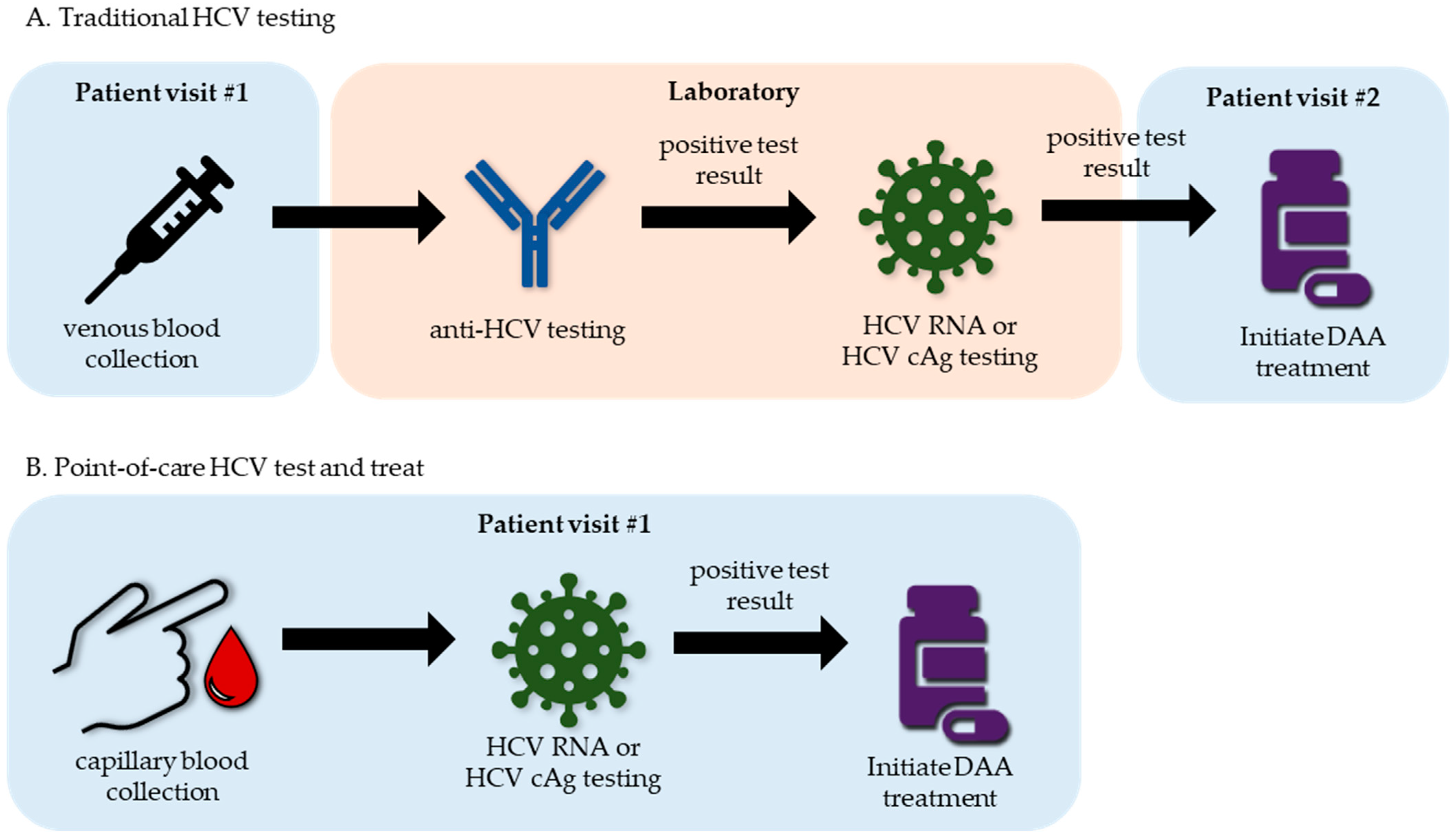
3.3. Hepatits C Virus
3.4. Hepatitis D Virus
3.5. Hepatitis E Virus
4. Clinical Markers of Hepatitis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bae, K.S.; Lee, S.; Lee, J.Y.; Kim, J.H.; Joo, Y.L.; Lee, S.H.; Chung, H.M.; You, K.A. Development of diagnostic systems for wide range and highly sensitive detection of two waterborne hepatitis viruses from groundwater using the conventional reverse transcription nested PCR assay. J. Virol. Methods 2022, 299, 114344. [Google Scholar] [CrossRef]
- Honda, M.; Asakura, H.; Kanda, T.; Somura, Y.; Ishii, T.; Yamana, Y.; Kaneko, T.; Mizutani, T.; Takahashi, H.; Kumagawa, M.; et al. Male-Dominant Hepatitis A Outbreak Observed among Non-HIV-Infected Persons in the Northern Part of Tokyo, Japan. Viruses 2021, 13, 207. [Google Scholar] [CrossRef] [PubMed]
- Shin, E.-C.; Jeong, S.-H. Natural History, Clinical Manifestations, and Pathogenesis of Hepatitis A. Cold Spring Harb. Perspect. Med. 2018, 8, a031708. [Google Scholar] [CrossRef] [PubMed]
- Hakim, M.S.; Wang, W.; Bramer, W.M.; Geng, J.; Huang, F.; de Man, R.A.; Peppelenbosch, M.P.; Pan, Q. The Global Burden of Hepatitis E Outbreaks: A Systematic Review. Liver Int. 2017, 37, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Fattovich, G.; Bortolotti, F.; Donato, F. Natural History of Chronic Hepatitis B: Special Emphasis on Disease Progression and Prognostic Factors. J. Hepatol. 2008, 48, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Westbrook, R.H.; Dusheiko, G. Natural History of Hepatitis C. J. Hepatol. 2014, 61, S58–S68. [Google Scholar] [CrossRef]
- Negro, F. Hepatitis D Virus Coinfection and Superinfection. Cold Spring Harb. Perspect. Med. 2014, 4, a021550. [Google Scholar] [CrossRef]
- Cao, G.; Jing, W.; Liu, J.; Liu, M. The Global Trends and Regional Differences in Incidence and Mortality of Hepatitis A from 1990 to 2019 and Implications for Its Prevention. Hepatol. Int. 2021, 15, 1068–1082. [Google Scholar] [CrossRef]
- World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021: Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-002707-7. [Google Scholar]
- Stockdale, A.J.; Kreuels, B.; Henrion, M.Y.R.; Giorgi, E.; Kyomuhangi, I.; De Martel, C.; Hutin, Y.; Geretti, A.M. The Global Prevalence of Hepatitis D Virus Infection: Systematic Review and Meta-Analysis. J. Hepatol. 2020, 73, 523–532. [Google Scholar] [CrossRef]
- Jing, W.; Liu, J.; Liu, M. The Global Trends and Regional Differences in Incidence of HEV Infection from 1990 to 2017 and Implications for HEV Prevention. Liver Int. 2021, 41, 58–69. [Google Scholar] [CrossRef]
- Nelson, N.P.; Weng, M.K.; Hofmeister, M.G.; Moore, K.L.; Doshani, M.; Kamili, S.; Koneru, A.; Haber, P.; Hagan, L.; Romero, J.R.; et al. Prevention of Hepatitis A Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices, 2020. MMWR Recomm. Rep. 2020, 69, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Bruce, M.G.; Bruden, D.; Hurlburt, D.; Zanis, C.; Thompson, G.; Rea, L.; Toomey, M.; Townshend-Bulson, L.; Rudolph, K.; Bulkow, L.; et al. Antibody Levels and Protection After Hepatitis B Vaccine: Results of a 30-Year Follow-up Study and Response to a Booster Dose. J. Infect. Dis. 2016, 214, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Pawlotsky, J.-M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; Marra, F.; Puoti, M.; Wedemeyer, H. EASL Recommendations on Treatment of Hepatitis C 2018. J. Hepatol. 2018, 69, 461–511. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021; World health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Drain, P.K.; Hyle, E.P.; Noubary, F.; Freedberg, K.A.; Wilson, D.; Bishai, W.R.; Rodriguez, W.; Bassett, I.V. Diagnostic Point-of-Care Tests in Resource-Limited Settings. Lancet Infect. Dis. 2014, 14, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Drain, P.K. Rapid Diagnostic Testing for SARS-CoV-2. N. Engl. J. Med. 2022, 386, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Kettler, H.; White, K.; Hawkes, S. Mapping the Landscape of Diagnostics for Sexually Transmitted Infections: Key Findings and Recommandations; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Land, K.J.; Boeras, D.I.; Chen, X.-S.; Ramsay, A.R.; Peeling, R.W. REASSURED Diagnostics to Inform Disease Control Strategies, Strengthen Health Systems and Improve Patient Outcomes. Nat. Microbiol. 2019, 4, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Cassedy, A.; Parle-McDermott, A.; O’Kennedy, R. Virus Detection: A Review of the Current and Emerging Molecular and Immunological Methods. Front. Mol. Biosci. 2021, 8, 637559. [Google Scholar] [CrossRef]
- Kralik, P.; Ricchi, M. A Basic Guide to Real Time PCR in Microbial Diagnostics: Definitions, Parameters, and Everything. Front. Microbiol. 2017, 8, 108. [Google Scholar] [CrossRef]
- Ince, B.; Sezgintürk, M.K. Lateral Flow Assays for Viruses Diagnosis: Up-to-Date Technology and Future Prospects. TrAC Trends Anal. Chem. 2022, 157, 116725. [Google Scholar] [CrossRef]
- Song, L.-W.; Wang, Y.-B.; Fang, L.-L.; Wu, Y.; Yang, L.; Chen, J.-Y.; Ge, S.-X.; Zhang, J.; Xiong, Y.-Z.; Deng, X.-M.; et al. Rapid Fluorescent Lateral-Flow Immunoassay for Hepatitis B Virus Genotyping. Anal. Chem. 2015, 87, 5173–5180. [Google Scholar] [CrossRef]
- Cho, I.-H.; Irudayaraj, J. Lateral-Flow Enzyme Immunoconcentration for Rapid Detection of Listeria Monocytogenes. Anal. Bioanal. Chem. 2013, 405, 3313–3319. [Google Scholar] [CrossRef] [PubMed]
- Curtis, K.A.; Rudolph, D.L.; Owen, S.M. Sequence-Specific Detection Method for Reverse Transcription, Loop-Mediated Isothermal Amplification of HIV-1. J. Med. Virol. 2009, 81, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, A.; Cerda, A.; Ibarra-Henríquez, C.; Sebastian, V.; Armijo, G.; Lamig, L.; Miranda, C.; Lagos, M.; Solari, S.; Guzmán, A.M.; et al. A Simple RNA Preparation Method for SARS-CoV-2 Detection by RT-QPCR. Sci. Rep. 2020, 10, 16608. [Google Scholar] [CrossRef] [PubMed]
- Joung, J.; Ladha, A.; Saito, M.; Kim, N.-G.; Woolley, A.E.; Segel, M.; Barretto, R.P.J.; Ranu, A.; Macrae, R.K.; Faure, G.; et al. Detection of SARS-CoV-2 with SHERLOCK One-Pot Testing. N. Engl. J. Med. 2020, 383, 1492–1494. [Google Scholar] [CrossRef] [PubMed]
- Ganguli, A.; Mostafa, A.; Berger, J.; Aydin, M.Y.; Sun, F.; Ramirez, S.A.S.D.; Valera, E.; Cunningham, B.T.; King, W.P.; Bashir, R. Rapid Isothermal Amplification and Portable Detection System for SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2020, 117, 22727–22735. [Google Scholar] [CrossRef] [PubMed]
- Myhrvold, C.; Freije, C.A.; Gootenberg, J.S.; Abudayyeh, O.O.; Metsky, H.C.; Durbin, A.F.; Kellner, M.J.; Tan, A.L.; Paul, L.M.; Parham, L.A.; et al. Field-Deployable Viral Diagnostics Using CRISPR-Cas13. Science 2018, 360, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Li, M.; Yue, D.; Chen, H. Solid-phase Extraction Methods for Nucleic Acid Separation. A Review. J. Sep. Sci. 2022, 45, 172–184. [Google Scholar] [CrossRef]
- Bektaş, A.; Covington, M.F.; Aidelberg, G.; Arce, A.; Matute, T.; Núñez, I.; Walsh, J.; Boutboul, D.; Delaugerre, C.; Lindner, A.B.; et al. Accessible LAMP-Enabled Rapid Test (ALERT) for Detecting SARS-CoV-2. Viruses 2021, 13, 742. [Google Scholar] [CrossRef]
- Trick, A.Y.; Chen, F.; Chen, L.; Lee, P.; Hasnain, A.C.; Mostafa, H.H.; Carroll, K.C.; Wang, T. Point-of-Care Platform for Rapid Multiplexed Detection of SARS-CoV-2 Variants and Respiratory Pathogens. Adv. Mater. Technol. 2022, 7, 2101013. [Google Scholar] [CrossRef]
- Sharma, S.; Thomas, E.; Caputi, M.; Asghar, W. RT-LAMP-Based Molecular Diagnostic Set-Up for Rapid Hepatitis C Virus Testing. Biosensors 2022, 12, 298. [Google Scholar] [CrossRef]
- Paul, R.; Ostermann, E.; Wei, Q. Advances in Point-of-Care Nucleic Acid Extraction Technologies for Rapid Diagnosis of Human and Plant Diseases. Biosens. Bioelectron. 2020, 169, 112592. [Google Scholar] [CrossRef] [PubMed]
- Trick, A.Y.; Ngo, H.T.; Nambiar, A.H.; Morakis, M.M.; Chen, F.-E.; Chen, L.; Hsieh, K.; Wang, T.-H. Filtration-Assisted Magnetofluidic Cartridge Platform for HIV RNA Detection from Blood. Lab Chip 2022, 22, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Ďurč, P.; Foret, F.; Kubáň, P. Fast Blood Plasma Separation Device for Point-of-Care Applications. Talanta 2018, 183, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Park, H.; Chung, D.R.; Kim, T.; Park, E.; Kang, M. A Self-Pressure-Driven Blood Plasma-Separation Device for Point-of-Care Diagnostics. Talanta 2022, 247, 123562. [Google Scholar] [CrossRef] [PubMed]
- Vemulapati, S.; Erickson, D. HERMES: Rapid Blood-Plasma Separation at the Point-of-Need. Lab Chip 2018, 18, 3285–3292. [Google Scholar] [CrossRef]
- Notomi, T. Loop-Mediated Isothermal Amplification of DNA. Nucleic Acids Res. 2000, 28, e63. [Google Scholar] [CrossRef]
- Nagamine, K.; Hase, T.; Notomi, T. Accelerated Reaction by Loop-Mediated Isothermal Amplification Using Loop Primers. Mol. Cell. Probes 2002, 16, 223–229. [Google Scholar] [CrossRef]
- Piepenburg, O.; Williams, C.H.; Stemple, D.L.; Armes, N.A. DNA Detection Using Recombination Proteins. PLoS Biol. 2006, 4, e204. [Google Scholar] [CrossRef]
- Farrar, J.S.; Wittwer, C.T. Extreme PCR: Efficient and Specific DNA Amplification in 15–60 Seconds. Clin. Chem. 2015, 61, 145–153. [Google Scholar] [CrossRef]
- Nouwairi, R.L.; Cunha, L.L.; Turiello, R.; Scott, O.; Hickey, J.; Thomson, S.; Knowles, S.; Chapman, J.D.; Landers, J.P. Ultra-Rapid Real-Time Microfluidic RT-PCR Instrument for Nucleic Acid Analysis. Lab Chip 2022, 22, 3424–3435. [Google Scholar] [CrossRef]
- Leber, A.L.; Everhart, K.; Daly, J.A.; Hopper, A.; Harrington, A.; Schreckenberger, P.; McKinley, K.; Jones, M.; Holmberg, K.; Kensinger, B. Multicenter Evaluation of BioFire FilmArray Respiratory Panel 2 for Detection of Viruses and Bacteria in Nasopharyngeal Swab Samples. J. Clin. Microbiol. 2018, 56, e01945-17. [Google Scholar] [CrossRef] [PubMed]
- Hansen, G.; Marino, J.; Wang, Z.-X.; Beavis, K.G.; Rodrigo, J.; Labog, K.; Westblade, L.F.; Jin, R.; Love, N.; Ding, K.; et al. Clinical Performance of the Point-of-Care Cobas Liat for Detection of SARS-CoV-2 in 20 Minutes: A Multicenter Study. J. Clin. Microbiol. 2021, 59, e02811-20. [Google Scholar] [CrossRef] [PubMed]
- Goto, M.; Honda, E.; Ogura, A.; Nomoto, A.; Hanaki, K.-I. Colorimetric Detection of Loop-Mediated Isothermal Amplification Reaction by Using Hydroxy Naphthol Blue. BioTechniques 2009, 46, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Tanner, N.A.; Zhang, Y.; Evans, T.C. Visual Detection of Isothermal Nucleic Acid Amplification Using PH-Sensitive Dyes. BioTechniques 2015, 58, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Fischbach, J.; Xander, N.C.; Frohme, M.; Glökler, J.F. Shining a Light on LAMP Assays’ A Comparison of LAMP Visualization Methods Including the Novel Use of Berberine. BioTechniques 2015, 58, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Lucchi, N.W.; Ljolje, D.; Silva-Flannery, L.; Udhayakumar, V. Use of Malachite Green-Loop Mediated Isothermal Amplification for Detection of Plasmodium Spp. Parasites. PLoS ONE 2016, 11, e0151437. [Google Scholar] [CrossRef]
- Scott, A.T.; Layne, T.R.; O’Connell, K.C.; Tanner, N.A.; Landers, J.P. Comparative Evaluation and Quantitative Analysis of Loop-Mediated Isothermal Amplification Indicators. Anal. Chem. 2020, 92, 13343–13353. [Google Scholar] [CrossRef]
- Kiatpathomchai, W.; Jaroenram, W.; Arunrut, N.; Jitrapakdee, S.; Flegel, T.W. Shrimp Taura Syndrome Virus Detection by Reverse Transcription Loop-Mediated Isothermal Amplification Combined with a Lateral Flow Dipstick. J. Virol. Methods 2008, 153, 214–217. [Google Scholar] [CrossRef]
- Mori, Y.; Kitao, M.; Tomita, N.; Notomi, T. Real-Time Turbidimetry of LAMP Reaction for Quantifying Template DNA. J. Biochem. Biophys. Methods 2004, 59, 145–157. [Google Scholar] [CrossRef]
- Seyrig, G.; Stedtfeld, R.D.; Tourlousse, D.M.; Ahmad, F.; Towery, K.; Cupples, A.M.; Tiedje, J.M.; Hashsham, S.A. Selection of Fluorescent DNA Dyes for Real-Time LAMP with Portable and Simple Optics. J. Microbiol. Methods 2015, 119, 223–227. [Google Scholar] [CrossRef]
- Gadkar, V.J.; Goldfarb, D.M.; Gantt, S.; Tilley, P.A.G. Real-Time Detection and Monitoring of Loop Mediated Amplification (LAMP) Reaction Using Self-Quenching and De-Quenching Fluorogenic Probes. Sci. Rep. 2018, 8, 5548. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Shen, H.; Lin, Q.; Huang, J.; Zhang, C.; Liu, Z.; Sun, M.; Zhang, J.; Liao, M.; Li, Y.; et al. Development of a Cleaved Probe-Based Loop-Mediated Isothermal Amplification Assay for Rapid Detection of African Swine Fever Virus. Front. Cell. Infect. Microbiol. 2022, 12, 884430. [Google Scholar] [CrossRef] [PubMed]
- Gandelman, O.A.; Church, V.L.; Moore, C.A.; Kiddle, G.; Carne, C.A.; Parmar, S.; Jalal, H.; Tisi, L.C.; Murray, J.A.H. Novel Bioluminescent Quantitative Detection of Nucleic Acid Amplification in Real-Time. PLoS ONE 2010, 5, e14155. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.S.; Ma, E.; Harrington, L.B.; Da Costa, M.; Tian, X.; Palefsky, J.M.; Doudna, J.A. CRISPR-Cas12a Target Binding Unleashes Indiscriminate Single-Stranded DNase Activity. Science 2018, 360, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Gootenberg, J.S.; Abudayyeh, O.O.; Kellner, M.J.; Joung, J.; Collins, J.J.; Zhang, F. Multiplexed and Portable Nucleic Acid Detection Platform with Cas13, Cas12a, and Csm6. Science 2018, 360, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Lemon, S.M.; Ott, J.J.; Van Damme, P.; Shouval, D. Type A Viral Hepatitis: A Summary and Update on the Molecular Virology, Epidemiology, Pathogenesis and Prevention. J. Hepatol. 2018, 68, 167–184. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Serrano, E.E.; González-López, O.; Das, A.; Lemon, S.M. Cellular Entry and Uncoating of Naked and Quasi-Enveloped Human Hepatoviruses. eLife 2019, 8, e43983. [Google Scholar] [CrossRef]
- Cook, N.; Bertrand, I.; Gantzer, C.; Pinto, R.M.; Bosch, A. Persistence of Hepatitis A Virus in Fresh Produce and Production Environments, and the Effect of Disinfection Procedures: A Review. Food Environ. Virol. 2018, 10, 253–262. [Google Scholar] [CrossRef]
- Klevens, R.M.; Denniston, M.M.; Jiles-Chapman, R.B.; Murphy, T.V. Decreasing Immunity to Hepatitis A Virus Infection among US Adults: Findings from the National Health and Nutrition Examination Survey (NHANES), 1999–2012. Vaccine 2015, 33, 6192–6198. [Google Scholar] [CrossRef]
- Foster, M.A.; Hofmeister, M.G.; Kupronis, B.A.; Lin, Y.; Xia, G.-L.; Yin, S.; Teshale, E. Increase in Hepatitis A Virus Infections—United States, 2013–2018. Morb. Mortal. Wkly. Rep. 2019, 68, 413–415. [Google Scholar] [CrossRef]
- Link-Gelles, R.; Hofmeister, M.G.; Nelson, N.P. Use of Hepatitis A Vaccine for Post-Exposure Prophylaxis in Individuals over 40 Years of Age: A Systematic Review of Published Studies and Recommendations for Vaccine Use. Vaccine 2018, 36, 2745–2750. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-J.; Jeong, H.S.; Cho, B.-K.; Ji, M.-J.; Kim, J.-H.; Lee, A.-N.; Lee, K.-R.; Cheon, D.-S. Evaluation of an Immunochromatographic Assay for the Detection of Anti-Hepatitis A Virus IgM. Virol. J. 2010, 7, 164. [Google Scholar] [CrossRef] [PubMed]
- Pal, S.; Juyal, D.; Sharma, M.; Kotian, S.; Negi, V.; Sharma, N. An Outbreak of Hepatitis A Virus among Children in a Flood Rescue Camp: A Post-Disaster Catastrophe. Indian J. Med. Microbiol. 2016, 34, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Hortense, R.P.S.; Bienvenue, O.J.; Abdoulaye, T.K.; Lalidia, O.B.; Asséta, K.; Pierre, R.; Nicolas, B. Sero-Prevalence and Risk Factors for Hepatitis A Virus Infection among Pregnant Women at the Samandin Medical Center, Ouagadougou, Burkina Faso. J. Adv. Biol. Biotechnol. 2019, 21, 1–9. [Google Scholar] [CrossRef]
- De Almeida Ribeiro, C.R.; Amado, L.A.; Tourinho, R.S.; Pinto Lima, L.R.; Melgaço, J.G.; De Almeida, A.J.; Bastos, L.S.; Lewis-Ximenez, L.L.; De Paula, V.S. Accuracy of Rapid Test for Diagnosis of Hepatitis A with Different Infection Rate Settings and with Predictive Modeling. Future Microbiol. 2019, 14, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Kweon, O.J.; Lim, Y.K.; Kim, H.R.; Kim, T.; Lee, M. Analytical Performance of Newly Developed Rapid Point-of-care Test for the Simultaneous Detection of Hepatitis A, B, and C Viruses in Serum Samples. J. Med. Virol. 2019, 91, 1056–1062. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Seo, H.S.; Kwon, J.-H.; Kim, H.-T.; Kwon, K.C.; Sim, S.J.; Cha, Y.J.; Lee, J. Multiplex Diagnosis of Viral Infectious Diseases (AIDS, Hepatitis C, and Hepatitis A) Based on Point of Care Lateral Flow Assay Using Engineered Proteinticles. Biosens. Bioelectron. 2015, 69, 213–225. [Google Scholar] [CrossRef]
- Yoneyama, T.; Kiyohara, T.; Shimasaki, N.; Kobayashi, G.; Ota, Y.; Notomi, T.; Totsuka, A.; Wakita, T. Rapid and Real-Time Detection of Hepatitis A Virus by Reverse Transcription Loop-Mediated Isothermal Amplification Assay. J. Virol. Methods 2007, 145, 162–168. [Google Scholar] [CrossRef]
- Sun, M.; Zhong, Y.; Li, X.; Yao, J.; Pan, Y. Simple and Feasible Detection of Hepatitis a Virus Using Reverse Transcription Multienzyme Isothermal Rapid Amplification and Lateral Flow Dipsticks without Standard PCR Laboratory. Artif. Cells Nanomed. Biotechnol. 2023, 51, 233–240. [Google Scholar] [CrossRef]
- Wu, R.; Meng, B.; Corredig, M.; Griffiths, M.W. Rapid Detection of Hepatitis A Virus in Foods Using a Bioluminescent Assay in Real-Time (BART) and Reverse Transcription Loop-Mediated Isothermal Amplification (RT-LAMP) Technology. Food Environ. Virol. 2023, 15, 144–157. [Google Scholar] [CrossRef]
- Velkov, S.; Ott, J.; Protzer, U.; Michler, T. The Global Hepatitis B Virus Genotype Distribution Approximated from Available Genotyping Data. Genes 2018, 9, 495. [Google Scholar] [CrossRef] [PubMed]
- Seeger, C.; Mason, W.S. Molecular Biology of Hepatitis B Virus Infection. Virology 2015, 479–480, 672–686. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.S.F.; McMahon, B.J. Chronic Hepatitis B. Hepatology 2007, 45, 507–539. [Google Scholar] [CrossRef] [PubMed]
- Mast, E.E.; Margolis, H.S.; Fiore, A.E.; Brink, E.W.; Goldstein, S.T.; Wang, S.A.; Moyer, L.A.; Bell, B.P.; Alter, M.J.; Advisory Committee on Immunization Practices (ACIP). A Comprehensive Immunization Strategy to Eliminate Transmission of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP) Part 1: Immunization of Infants, Children, and Adolescents. Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2005, 54, 1–31. [Google Scholar]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S.; Bzowej, N.H.; Wong, J.B. Update on Prevention, Diagnosis, and Treatment of Chronic Hepatitis B: AASLD 2018 Hepatitis B Guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Gish, R.G.; Given, B.D.; Lai, C.-L.; Locarnini, S.A.; Lau, J.Y.N.; Lewis, D.L.; Schluep, T. Chronic Hepatitis B: Virology, Natural History, Current Management and a Glimpse at Future Opportunities. Antivir. Res. 2015, 121, 47–58. [Google Scholar] [CrossRef]
- Lampertico, P.; Agarwal, K.; Berg, T.; Buti, M.; Janssen, H.L.A.; Papatheodoridis, G.; Zoulim, F.; Tacke, F. EASL 2017 Clinical Practice Guidelines on the Management of Hepatitis B Virus Infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef]
- Jeng, W.-J.; Papatheodoridis, G.V.; Lok, A.S.F. Hepatitis B. Lancet 2023, 401, 1039–1052. [Google Scholar] [CrossRef]
- Cryer, A.M.; Imperial, J.C. Hepatitis B in Pregnant Women and Their Infants. Clin. Liver Dis. 2019, 23, 451–462. [Google Scholar] [CrossRef]
- Hadziyannis, S.; Papatheodoridis, G. Hepatitis Be Antigen-Negative Chronic Hepatitis B: Natural History and Treatment. Semin. Liver Dis. 2006, 26, 130–141. [Google Scholar] [CrossRef]
- Simonetti, J.; Bulkow, L.; McMahon, B.J.; Homan, C.; Snowball, M.; Negus, S.; Williams, J.; Livingston, S.E. Clearance of Hepatitis B Surface Antigen and Risk of Hepatocellular Carcinoma in a Cohort Chronically Infected with Hepatitis B Virus. Hepatology 2010, 51, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Gong, Y.; Brok, J.; Boxall, E.H.; Gluud, C. Hepatitis B Immunisation for Newborn Infants of Hepatitis B Surface Antigen-Positive Mothers. Cochrane Database Syst. Rev. 2006, CD004790. [Google Scholar] [CrossRef] [PubMed]
- Terrault, N.A.; Bzowej, N.H.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Murad, M.H. AASLD Guidelines for Treatment of Chronic Hepatitis B: Hepatology, Month 2015. Hepatology 2016, 63, 261–283. [Google Scholar] [CrossRef] [PubMed]
- Liem, K.S.; Gehring, A.J.; Feld, J.J.; Janssen, H.L.A. Challenges with Stopping Long-Term Nucleos(t)Ide Analogue Therapy in Patients with Chronic Hepatitis B. Gastroenterology 2020, 158, 1185–1190. [Google Scholar] [CrossRef] [PubMed]
- Amini, A.; Varsaneux, O.; Kelly, H.; Tang, W.; Chen, W.; Boeras, D.I.; Falconer, J.; Tucker, J.D.; Chou, R.; Ishizaki, A.; et al. Diagnostic Accuracy of Tests to Detect Hepatitis B Surface Antigen: A Systematic Review of the Literature and Meta-Analysis. BMC Infect. Dis. 2017, 17, 698. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, R.P.; Davies, J.; Binks, P.; Dhurrkay, R.G.; Gurruwiwi, G.G.; Bukulatjpi, S.M.; McKinnon, M.; Hosking, K.; Littlejohn, M.; Jackson, K.; et al. Point of Care and Oral Fluid Hepatitis B Testing in Remote Indigenous Communities of Northern Australia. J. Viral Hepat. 2020, 27, 407–414. [Google Scholar] [CrossRef]
- Kabamba, A.T.; Mwamba, C.M.; Dessilly, G.; Dufrasne, F.; Kabamba, B.M.; Longanga, A.O. Evaluation of the Analytical Performance of Six Rapid Diagnostic Tests for the Detection of Viral Hepatitis B and C in Lubumbashi, Democratic Republic of Congo. J. Virol. Methods 2020, 285, 113961. [Google Scholar] [CrossRef] [PubMed]
- Dembele, B.; Affi-Aboli, R.; Kabran, M.; Sevede, D.; Goha, V.; Adiko, A.C.; Kouamé, R.; Allah-Kouadio, E.; Inwoley, A. Evaluation of Four Rapid Tests for Detection of Hepatitis B Surface Antigen in Ivory Coast. J. Immunol. Res. 2020, 2020, 6315718. [Google Scholar] [CrossRef]
- Hirzel, C.; Pfister, S.; Gorgievski-Hrisoho, M.; Wandeler, G.; Zuercher, S. Performance of HBsAg Point-of-Care Tests for Detection of Diagnostic Escape-Variants in Clinical Samples. J. Clin. Virol. 2015, 69, 33–35. [Google Scholar] [CrossRef]
- Robin, L.; Mboumba Bouassa, R.-S.; Nodjikouambaye, Z.A.; Charmant, L.; Matta, M.; Simon, S.; Filali, M.; Mboup, S.; Bélec, L. Analytical Performances of Simultaneous Detection of HIV-1, HIV-2 and Hepatitis C-Specific Antibodies and Hepatitis B Surface Antigen (HBsAg) by Multiplex Immunochromatographic Rapid Test with Serum Samples: A Cross-Sectional Study. J. Virol. Methods 2018, 253, 1–4. [Google Scholar] [CrossRef]
- Mossoro-Kpinde, C.D.; Mireille Kalla, G.C.; Baguida-Bokia, C.; Sombot-Ndicki, S.; Bobossi, C.; Tonen-Wolyec, S.; Mbopi-Kéo, F.-X.; Bélec, L. Diagnostic Performances of Exacto® Triplex Rapid Test for Diagnosis of HIV/HCV/HBsAg: A STROBE-Compliant Multicenter, Cross-Sectional, Field Study in the Central African Republic. Pan Afr. Med. J. 2022, 43, 21. [Google Scholar] [CrossRef] [PubMed]
- Ho, E.; Michielsen, P.; Van Damme, P.; Ieven, M.; Veldhuijzen, I.; Vanwolleghem, T. Point-of-Care Tests for Hepatitis B Are Associated with A Higher Linkage to Care and Lower Cost Compared to Venepuncture Sampling during Outreach Screenings in an Asian Migrant Population. Ann. Glob. Health 2020, 86, 81. [Google Scholar] [CrossRef] [PubMed]
- Seck, A.; Ndiaye, F.; Maylin, S.; Ndiaye, B.; Simon, F.; Funk, A.L.; Fontanet, A.; Takahashi, K.; Akbar, S.M.F.; Mishiro, S.; et al. Poor Sensitivity of Commercial Rapid Diagnostic Tests for Hepatitis B e Antigen in Senegal, West Africa. Am. J. Trop. Med. Hyg. 2018, 99, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Leathers, J.S.; Pisano, M.B.; Re, V.; van Oord, G.; Sultan, A.; Boonstra, A.; Debes, J.D. Evaluation of Rapid Diagnostic Tests for Assessment of Hepatitis B in Resource-Limited Settings. Ann. Glob. Health 2019, 85, 98. [Google Scholar] [CrossRef] [PubMed]
- Ségéral, O.; N’Diaye, D.S.; Prak, S.; Nouhin, J.; Chhun, S.; Khamduang, W.; Chim, K.; Roque-Afonso, A.-M.; Piola, P.; Borand, L.; et al. Usefulness of a Serial Algorithm of HBsAg and HBeAg Rapid Diagnosis Tests to Detect Pregnant Women at Risk of HBV Mother-to-Child Transmission in Cambodia, the ANRS 12328 Pilot Study. J. Clin. Virol. 2018, 109, 29–34. [Google Scholar] [CrossRef]
- Stockdale, A.J.; Silungwe, N.M.; Shawa, I.T.; Kreuels, B.; Gordon, M.A.; Geretti, A.M. Diagnostic Performance Evaluation of Hepatitis B e Antigen Rapid Diagnostic Tests in Malawi. BMC Infect. Dis. 2021, 21, 487. [Google Scholar] [CrossRef]
- Si, J.; Li, J.; Zhang, L.; Zhang, W.; Yao, J.; Li, T.; Wang, W.; Zhu, W.; Allain, J.; Fu, Y.; et al. A Signal Amplification System on a Lateral Flow Immunoassay Detecting for Hepatitis E-antigen in Human Blood Samples. J. Med. Virol. 2019, 91, 1301–1306. [Google Scholar] [CrossRef]
- El-Ghitany, E.M.; Farghaly, A.G. Evaluation of Commercialized Rapid Diagnostic Testing for Some Hepatitis B Biomarkers in an Area of Intermediate Endemicity. J. Virol. Methods 2013, 194, 190–193. [Google Scholar] [CrossRef]
- Cruz, H.M.; de Paula Scalioni, L.; Paula, V.S.d.; Miguel, J.C.; do Ó, K.M.R.; Milagres, F.A.P.; Cruz, M.S.; Bastos, F.I.; Flores, P.P.; Leal, E.; et al. Poor Sensitivity of Rapid Tests for the Detection of Antibodies to the Hepatitis B Virus: Implications for Field Studies. Mem. Inst. Oswaldo Cruz 2017, 112, 209–213. [Google Scholar] [CrossRef]
- Bottero, J.; Boyd, A.; Gozlan, J.; Lemoine, M.; Carrat, F.; Collignon, A.; Boo, N.; Dhotte, P.; Varsat, B.; Muller, G.; et al. Performance of Rapid Tests for Detection of HBsAg and Anti-HBsAb in a Large Cohort, France. J. Hepatol. 2013, 58, 473–478. [Google Scholar] [CrossRef]
- Poiteau, L.; Soulier, A.; Roudot-Thoraval, F.; Hézode, C.; Challine, D.; Pawlotsky, J.-M.; Chevaliez, S. Performance of Rapid Diagnostic Tests for the Detection of Anti-HBs in Various Patient Populations. J. Clin. Virol. 2017, 96, 64–66. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Ouyang, S.; Lin, L.; Wu, L.; Xie, T.; Chen, J.; Li, Z.; Zhu, G.; Ji, T.; Pan, Z.; et al. Diagnostic Accuracy of LAMP Assay for HBV Infection. J. Clin. Lab. Anal. 2020, 34, e23281. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Qiu, F.; Shen, L.-P.; Yan, T.; Zhao, M.; Qi, J.-J.; Chen, C.; Zhao, L.; Wang, L.; Feng, Z.; et al. A Rapid and Sensitive Recombinase Aided Amplification Assay to Detect Hepatitis B Virus without DNA Extraction. BMC Infect. Dis. 2019, 19, 229. [Google Scholar] [CrossRef]
- Yi, T.; Zhang, H.; Liang, H.; Gong, G.; Cai, Y. Betaine-assisted Recombinase Polymerase Assay for Rapid Hepatitis B Virus Detection. Biotechnol. Appl. Biochem. 2021, 68, 469–475. [Google Scholar] [CrossRef]
- Zhang, B.; Zhu, Z.; Li, F.; Xie, X.; Ding, A. Rapid and Sensitive Detection of Hepatitis B Virus by Lateral Flow Recombinase Polymerase Amplification Assay. J. Virol. Methods 2021, 291, 114094. [Google Scholar] [CrossRef]
- Bai, X.; Ma, X.; Li, M.; Li, X.; Fan, G.; Zhang, R.; Wang, R.; Duan, Q.; Shen, X.; Xie, Y.; et al. Field Applicable Detection of Hepatitis B Virus Using Internal Controlled Duplex Recombinase-aided Amplification Assay and Lateral Flow Dipstick Assay. J. Med. Virol. 2020, 92, 3344–3353. [Google Scholar] [CrossRef] [PubMed]
- Mayran, C.; Foulongne, V.; Van De Perre, P.; Fournier-Wirth, C.; Molès, J.-P.; Cantaloube, J.-F. Rapid Diagnostic Test for Hepatitis B Virus Viral Load Based on Recombinase Polymerase Amplification Combined with a Lateral Flow Read-Out. Diagnostics 2022, 12, 621. [Google Scholar] [CrossRef]
- Seok, Y.; Yin, Q.; Bai, H.; Bau, H.H. Sensitive, Single-Pot, Two-Stage Assay for Hepatitis Viruses. Anal. Chem. 2022, 94, 1778–1786. [Google Scholar] [CrossRef]
- Chen, X.; Zhou, Q.; Dong, S.; Wang, S.; Liu, R.; Wu, X.; Li, S. Multiple Cross Displacement Amplification Linked with Nanoparticles-Based Lateral Flow Biosensor in Screening of Hepatitis B Virus in Clinical Application. Infect. Drug Resist. 2021, 14, 1219–1229. [Google Scholar] [CrossRef]
- Ding, X.; Wang, G.; Mu, Y. Single Enzyme-Based Stem-Loop and Linear Primers Co-Mediated Exponential Amplification of Short Gene Sequences. Anal. Chim. Acta 2019, 1081, 193–199. [Google Scholar] [CrossRef]
- Ding, R.; Long, J.; Yuan, M.; Zheng, X.; Shen, Y.; Jin, Y.; Yang, H.; Li, H.; Chen, S.; Duan, G. CRISPR/Cas12-Based Ultra-Sensitive and Specific Point-of-Care Detection of HBV. Int. J. Mol. Sci. 2021, 22, 4842. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Fan, Z.; Xu, L.; Cao, Y.; Chen, S.; Pan, Z.; Gao, Y.; Li, H.; Zheng, S.; Ma, Y.; et al. CRISPR/Cas13a-Assisted Rapid and Portable HBV DNA Detection for Low-Level Viremia Patients. Emerg. Microbes Infect. 2023, 12, e2177088. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Tan, Y.; Wang, S.; Wu, X.; Liu, R.; Yang, X.; Wang, Y.; Tai, J.; Li, S. A CRISPR-Cas12b–Based Platform for Ultrasensitive, Rapid, and Highly Specific Detection of Hepatitis B Virus Genotypes B and C in Clinical Application. Front. Bioeng. Biotechnol. 2021, 9, 743322. [Google Scholar] [CrossRef] [PubMed]
- Nyan, D.-C.; Ulitzky, L.E.; Cehan, N.; Williamson, P.; Winkelman, V.; Rios, M.; Taylor, D.R. Rapid Detection of Hepatitis B Virus in Blood Plasma by a Specific and Sensitive Loop-Mediated Isothermal Amplification Assay. Clin. Infect. Dis. 2014, 59, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Quoc, N.B.; Phuong, N.D.N.; Chau, N.N.B.; Linh, D.T.P. Closed Tube Loop-Mediated Isothermal Amplification Assay for Rapid Detection of Hepatitis B Virus in Human Blood. Heliyon 2018, 4, e00561. [Google Scholar] [CrossRef]
- Vanhomwegen, J.; Kwasiborski, A.; Diop, A.; Boizeau, L.; Hoinard, D.; Vray, M.; Bercion, R.; Ndiaye, B.; Dublineau, A.; Michiyuki, S.; et al. Development and Clinical Validation of Loop-Mediated Isothermal Amplification (LAMP) Assay to Diagnose High HBV DNA Levels in Resource-Limited Settings. Clin. Microbiol. Infect. 2021, 27, 1858.e9–1858.e15. [Google Scholar] [CrossRef]
- Gupta, E.; Khodare, A.; Rani, N.; Singh, G.; Aggarwal, K.; Sharma, M. Performance Evaluation of Xpert HBV Viral Load (VL) Assay: Point-of-Care Molecular Test to Strengthen and Decentralize Management of Chronic Hepatitis B (CHB) Infection. J. Virol. Methods 2021, 290, 114063. [Google Scholar] [CrossRef]
- Marcuccilli, F.; Chevaliez, S.; Muller, T.; Colagrossi, L.; Abbondanza, G.; Beyser, K.; Wlassow, M.; Ortonne, V.; Perno, C.F.; Ciotti, M. Multicenter Evaluation of the Cepheid Xpert® HBV Viral Load Test. Diagnostics 2021, 11, 297. [Google Scholar] [CrossRef]
- Jackson, K.; Tekoaua, R.; Li, X.; Locarnini, S. Real-world Application of the Xpert® HBV Viral Load Assay on Serum and Dried Blood Spots. J. Med. Virol. 2021, 93, 3707–3713. [Google Scholar] [CrossRef]
- Poiteau, L.; Wlassow, M.; Hézode, C.; Pawlotsky, J.-M.; Chevaliez, S. Evaluation of the Xpert HBV Viral Load for Hepatitis B Virus Molecular Testing. J. Clin. Virol. 2020, 129, 104481. [Google Scholar] [CrossRef]
- Hedskog, C.; Parhy, B.; Chang, S.; Zeuzem, S.; Moreno, C.; Shafran, S.D.; Borgia, S.M.; Asselah, T.; Alric, L.; Abergel, A.; et al. Identification of 19 Novel Hepatitis C Virus Subtypes—Further Expanding HCV Classification. Open Forum Infect. Dis. 2019, 6, ofz076. [Google Scholar] [CrossRef] [PubMed]
- Penin, F. Structural Biology of Hepatitis C Virus. Clin. Liver Dis. 2003, 7, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Dubuisson, J.; Cosset, F.-L. Virology and Cell Biology of the Hepatitis C Virus Life Cycle—An Update. J. Hepatol. 2014, 61, S3–S13. [Google Scholar] [CrossRef] [PubMed]
- Schillie, S.; Wester, C.; Osborne, M.; Wesolowski, L.; Ryerson, A.B. CDC Recommendations for Hepatitis C Screening Among Adults—United States, 2020. MMWR Recomm. Rep. 2020, 69, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Colin, C.; Lanoir, D.; Touzet, S.; Meyaud-Kraemer, L.; Bailly, F.; Trepo, C.; The HEPATIS Group. Sensitivity and Specificity of Third-Generation Hepatitis C Virus Antibody Detection Assays: An Analysis of the Literature. J. Viral Hepat. 2001, 8, 87–95. [Google Scholar] [CrossRef]
- Falade-Nwulia, O.; Suarez-Cuervo, C.; Nelson, D.R.; Fried, M.W.; Segal, J.B.; Sulkowski, M.S. Oral Direct-Acting Agent Therapy for Hepatitis C Virus Infection: A Systematic Review. Ann. Intern. Med. 2017, 166, 637. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Testing for HCV Infection: An Update of Guidance for Clinicians and Laboratorians. Morb. Mortal. Wkly. Rep. 2013, 62, 362–365. [Google Scholar]
- Konerman, M.A.; Lok, A.S.F. Hepatitis C Treatment and Barriers to Eradication. Clin. Transl. Gastroenterol. 2016, 7, e193. [Google Scholar] [CrossRef]
- Applegate, T.L.; Fajardo, E.; Sacks, J.A. Hepatitis C Virus Diagnosis and the Holy Grail. Infect. Dis. Clin. North Am. 2018, 32, 425–445. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Hepatitis B and C Testing; World Health Organization: Geneva, Switzerland, 2017; ISBN 978-92-4-154998-1. [Google Scholar]
- Lamoury, F.M.J.; Njouom, R.; Amougou-Atsama, M.; Yiagnigni Mfopou, E.; Berishvili, N.; Sologashvili, M.; Fajardo, E.; Malobela, A.; Macé, A.; Chirehwa, M.; et al. Diagnostic Performance and Usability of the Genedrive® HCV ID Kit in Two Decentralized Settings in Cameroon and Georgia. Diagnostics 2021, 11, 746. [Google Scholar] [CrossRef]
- Llibre, A.; Shimakawa, Y.; Mottez, E.; Ainsworth, S.; Buivan, T.-P.; Firth, R.; Harrison, E.; Rosenberg, A.R.; Meritet, J.-F.; Fontanet, A.; et al. Development and Clinical Validation of the Genedrive Point-of-Care Test for Qualitative Detection of Hepatitis C Virus. Gut 2018, 67, 2017–2024. [Google Scholar] [CrossRef]
- Padhi, A.; Gupta, E.; Singh, G.; Agarwal, R.; Sharma, M.K.; Sarin, S.K. Evaluation of the Point of Care Molecular Diagnostic Genedrive HCV ID Kit for the Detection of HCV RNA in Clinical Samples. Epidemiol. Infect. 2020, 1–23. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.P.; Wu, A.H.B.; Chevaliez, S.; Pawlotsky, J.M.; Hallin, M.; Templeton, K.E. Multicenter Evaluation of the Cepheid Xpert Hepatitis C Virus Viral Load Assay. J. Clin. Microbiol. 2017, 55, 1550–1556. [Google Scholar] [CrossRef] [PubMed]
- Gupta, E.; Agarwala, P.; Kumar, G.; Maiwall, R.; Sarin, S.K. Point-of-Care Testing (POCT) in Molecular Diagnostics: Performance Evaluation of GeneXpert HCV RNA Test in Diagnosing and Monitoring of HCV Infection. J. Clin. Virol. 2017, 88, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Lamoury, F.M.J.; Bajis, S.; Hajarizadeh, B.; Marshall, A.D.; Martinello, M.; Ivanova, E.; Catlett, B.; Mowat, Y.; Marks, P.; Amin, J.; et al. Evaluation of the Xpert HCV Viral Load Finger-Stick Point-of-Care Assay. J. Infect. Dis. 2018, 217, 1889–1896. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, Z.; Mbwambo, J.; Rwegasha, J.; Mgina, N.; Doulla, B.; Mwakale, P.; Tuaillon, E.; Chevaliez, S.; Shimakawa, Y.; Taylor-Robinson, S.D.; et al. In-field Evaluation of Xpert® HCV Viral Load Fingerstick Assay in People Who Inject Drugs in Tanzania. Liver Int. 2020, 40, 514–521. [Google Scholar] [CrossRef]
- Catlett, B.; Hajarizadeh, B.; Cunningham, E.; Wolfson-Stofko, B.; Wheeler, A.; Khandaker-Hussain, B.; Feld, J.J.; Martró, E.; Chevaliez, S.; Pawlotsky, J.M.; et al. Diagnostic Accuracy of Assays Using Point-of-Care Testing or Dried Blood Spot Samples for the Determination of Hepatitis C Virus RNA: A Systematic Review. J. Infect. Dis. 2022, 226, 1005–1021. [Google Scholar] [CrossRef]
- Grebely, J.; Catlett, B.; Jayasinghe, I.; Valerio, H.; Hajarizadeh, B.; Verich, A.; Cunningham, P.; Martinello, M.; Tillakeratne, S.; Silk, D.; et al. Time to Detection of Hepatitis C Virus Infection with the Xpert HCV Viral Load Fingerstick Point-of-Care Assay: Facilitating a More Rapid Time to Diagnosis. J. Infect. Dis. 2020, 221, 2043–2049. [Google Scholar] [CrossRef]
- Agarwal, R.; Gupta, E.; Kumar, G.; Singh, K.K.; Sharma, M.K. Evaluation of True Point of Care Molecular Assay Using Fingerstick Capillary Whole Blood for Diagnosis of Hepatitis C Infection. J. Med Microbiol. 2021, 70, 001332. [Google Scholar] [CrossRef]
- Esfahani, S.N.; Shahhosseiny, M.H.; Yaghmai, P.; Praivar, K.; Moslemi, E.; Amini, H.K. Rapid and Simple Detection of Hepatitis C Virus by Reverse Transcriptase-Loop-Mediated Isothermal Amplification Method. Afr. J. Microbiol. Res. 2010, 4, 2580–2586. [Google Scholar]
- Kargar, M.; Askari, A.; Doosti, A.; Ghorbani-Dalini, S. Loop-Mediated Isothermal Amplification Assay for Rapid Detection of Hepatitis C Virus. Indian J. Virol. 2012, 23, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhang, J.; Hu, J.; Chen, H.; Du, L.; Wu, L.; Ding, Y.; Xiong, S.; Huang, X.; Zhang, Y.; et al. Rapid Detection of Hepatitis C Virus RNA by a Reverse Transcription Loop-Mediated Isothermal Amplification Assay. FEMS Immunol. Med. Microbiol. 2011, 63, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Fang, M.; Li, J.; Lou, G.; Lu, H.; Wu, N. Detection of Hepatitis C Virus by an Improved Loop-Mediated Isothermal Amplification Assay. Arch. Virol. 2011, 156, 1387–1396. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Liu, J.; Sun, D. Detection of HCV Genotypes 1b and 2a by a Reverse Transcription Loop-Mediated Isothermal Amplification Assay. J. Med. Virol. 2017, 89, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Hongjaisee, S.; Doungjinda, N.; Khamduang, W.; Carraway, T.S.; Wipasa, J.; Debes, J.D.; Supparatpinyo, K. Rapid Visual Detection of Hepatitis C Virus Using a Reverse Transcription Loop-Mediated Isothermal Amplification Assay. Int. J. Infect. Dis. 2021, 102, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Nyan, D.-C.; Swinson, K.L. A Method for Rapid Detection and Genotype Identification of Hepatitis C Virus 1–6 by One-Step Reverse Transcription Loop-Mediated Isothermal Amplification. Int. J. Infect. Dis. 2016, 43, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Hongjaisee, S.; Jabjainai, Y.; Sakset, S.; Preechasuth, K.; Ngo-Giang-Huong, N.; Khamduang, W. Comparison of Simple RNA Extraction Methods for Molecular Diagnosis of Hepatitis C Virus in Plasma. Diagnostics 2022, 12, 1599. [Google Scholar] [CrossRef]
- Jogezai, N.; Shabbir, M.I. A Hand-Held Device for Rapid Single Tube Detection of Hepatitis-C Virus. Anal. Methods 2018, 10, 4233–4241. [Google Scholar] [CrossRef]
- Witkowska McConnell, W.; Davis, C.; Sabir, S.R.; Garrett, A.; Bradley-Stewart, A.; Jajesniak, P.; Reboud, J.; Xu, G.; Yang, Z.; Gunson, R.; et al. Paper Microfluidic Implementation of Loop Mediated Isothermal Amplification for Early Diagnosis of Hepatitis C Virus. Nat. Commun. 2021, 12, 6994. [Google Scholar] [CrossRef]
- Xie, C.; Chen, S.; Zhang, L.; He, X.; Ma, Y.; Wu, H.; Zou, B.; Zhou, G. Multiplex Detection of Blood-Borne Pathogens on a Self-Driven Microfluidic Chip Using Loop-Mediated Isothermal Amplification. Anal. Bioanal. Chem. 2021, 413, 2923–2931. [Google Scholar] [CrossRef]
- Kham-Kjing, N.; Ngo-Giang-Huong, N.; Tragoolpua, K.; Khamduang, W.; Hongjaisee, S. Highly Specific and Rapid Detection of Hepatitis C Virus Using RT-LAMP-Coupled CRISPR–Cas12 Assay. Diagnostics 2022, 12, 1524. [Google Scholar] [CrossRef] [PubMed]
- Chia, C.T.; Bender, A.T.; Lillis, L.; Sullivan, B.P.; Martin, C.D.; Burke, W.; Landis, C.; Boyle, D.S.; Posner, J.D. Rapid Detection of Hepatitis C Virus Using Recombinase Polymerase Amplification. PLoS ONE 2022, 17, e0276582. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, Y.; Zhou, J.; Li, M.; Chen, Y.; Liu, Y.; Liu, H.; Ding, P.; Liang, C.; Zhu, X.; et al. Rapid Visual Detection of Hepatitis C Virus Using Reverse Transcription Recombinase-Aided Amplification–Lateral Flow Dipstick. Front. Cell. Infect. Microbiol. 2022, 12, 816238. [Google Scholar] [CrossRef] [PubMed]
- Su, F.; Zou, M.; Wu, H.; Xiao, F.; Sun, Y.; Zhang, C.; Gao, W.; Zhao, F.; Fan, X.; Yan, X.; et al. Sensitive Detection of Hepatitis C Virus Using a Catalytic Hairpin Assembly Coupled with a Lateral Flow Immunoassay Test Strip. Talanta 2022, 239, 123122. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Du, Y.; Li, X.; Du, B. Rapid and Sensitive Detection of Hepatitis C Virus in Clinical Blood Samples Using Reverse Transcriptase Polymerase Spiral Reaction. J. Microbiol. Biotechnol. 2020, 30, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Mikawa, A.Y.; Santos, S.A.T.; Kenfe, F.R.; da Silva, F.H.; da Costa, P.I. Development of a Rapid One-Step Immunochromatographic Assay for HCV Core Antigen Detection. J. Virol. Methods 2009, 158, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.; Sharma, P. Design of a Novel Rapid Immunoassay for Simultaneous Detection of Hepatitis C Virus Core Antigen and Antibodies. Arch. Virol. 2020, 165, 627–641. [Google Scholar] [CrossRef]
- Khuroo, M.S.; Khuroo, N.S.; Khuroo, M.S. Diagnostic Accuracy of Point-of-Care Tests for Hepatitis C Virus Infection: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0121450. [Google Scholar] [CrossRef]
- Tang, W.; Chen, W.; Amini, A.; Boeras, D.; Falconer, J.; Kelly, H.; Peeling, R.; Varsaneux, O.; Tucker, J.D.; Easterbrook, P. Diagnostic Accuracy of Tests to Detect Hepatitis C Antibody: A Meta-Analysis and Review of the Literature. BMC Infect. Dis. 2017, 17, 695. [Google Scholar] [CrossRef]
- Chevaliez, S.; Roudot-Thoraval, F.; Hézode, C.; Pawlotsky, J.-M.; Njouom, R. Performance of Rapid Diagnostic Tests for HCV Infection in Serum or Plasma. Future Microbiol. 2021, 16, 713–719. [Google Scholar] [CrossRef]
- de Paula Scalioni, L.; Cruz, H.M.; de Paula, V.S.; Miguel, J.C.; Marques, V.A.; Villela-Nogueira, C.A.; Milagres, F.A.P.; Cruz, M.S.; Bastos, F.I.; Andrade, T.M.; et al. Performance of Rapid Hepatitis C Virus Antibody Assays among High- and Low-Risk Populations. J. Clin. Virol. 2014, 60, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Uusküla, A.; Talu, A.; Rannap, J.; Barnes, D.M.; Jarlais, D.D. Rapid Point-of-Care (POC) Testing for Hepatitis C Antibodies in a Very High Prevalence Setting: Persons Injecting Drugs in Tallinn, Estonia. Harm. Reduct. J. 2021, 18, 39. [Google Scholar] [CrossRef] [PubMed]
- Koo, V.; Tian, F.; Wong, W.W.L. Cost-effectiveness Analysis of Hepatitis C Virus (HCV) Point-of-care Assay for HCV Screening. Liver Int. 2022, 42, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Shih, S.T.F.; Cheng, Q.; Carson, J.; Valerio, H.; Sheehan, Y.; Gray, R.T.; Cunningham, E.B.; Kwon, J.A.; Lloyd, A.R.; Dore, G.J.; et al. Optimizing Point-of-Care Testing Strategies for Diagnosis and Treatment of Hepatitis C Virus Infection in Australia: A Model-Based Cost-Effectiveness Analysis. Lancet Reg. Health—West. Pac. 2023, 36, 100750. [Google Scholar] [CrossRef] [PubMed]
- Duchesne, L.; Hejblum, G.; Njouom, R.; Touré Kane, C.; d’Aquin Toni, T.; Moh, R.; Sylla, B.; Rouveau, N.; Attia, A.; Lacombe, K. Model-Based Cost-Effectiveness Estimates of Testing Strategies for Diagnosing Hepatitis C Virus Infection in Central and Western Africa. PLoS ONE 2020, 15, e0238035. [Google Scholar] [CrossRef]
- Lafferty, L.; Cochrane, A.; Sheehan, Y.; Treloar, C.; Grebely, J.; Lloyd, A.R. “That Was Quick, Simple, and Easy”: Patient Perceptions of Acceptability of Point-of-Care Hepatitis C RNA Testing at a Reception Prison. Int. J. Drug Policy 2022, 99, 103456. [Google Scholar] [CrossRef]
- Kronfli, N.; Dussault, C.; Chalifoux, S.; Kavoukian, H.; Klein, M.B.; Cox, J. A Randomized Pilot Study Assessing the Acceptability of Rapid Point-of-Care Hepatitis C Virus (HCV) Testing among Male Inmates in Montreal, Canada. Int. J. Drug Policy 2020, 85, 102921. [Google Scholar] [CrossRef]
- Walker, J.G.; Ivanova, E.; Jamil, M.S.; Ong, J.J.; Easterbrook, P.; Fajardo, E.; Johnson, C.C.; Luhmann, N.; Terris-Prestholt, F.; Vickerman, P.; et al. Cost-effectiveness of Hepatitis C virus self-testing in four settings. PLoS Glob. Public Health 2023, 3, e0001667. [Google Scholar] [CrossRef]
- Trickey, A.; Fajardo, E.; Alemu, D.; Artenie, A.A.; Easterbrook, P. Impact of hepatitis C virus point-of-care RNA viral load testing compared with laboratory-based testing on uptake of RNA testing and treatment, and turnaround times: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2023, 8, 253–270. [Google Scholar] [CrossRef]
- Bahoussi, A.N.; Wang, P.-H.; Guo, Y.-Y.; Rabbani, N.; Wu, C.; Xing, L. Global Distribution and Natural Recombination of Hepatitis D Virus: Implication of Kyrgyzstan Emerging HDVs in the Clinical Outcomes. Viruses 2022, 14, 1467. [Google Scholar] [CrossRef]
- Sagnelli, C.; Sagnelli, E.; Russo, A.; Pisaturo, M.; Occhiello, L.; Coppola, N. HBV/HDV Co-Infection: Epidemiological and Clinical Changes, Recent Knowledge and Future Challenges. Life 2021, 11, 169. [Google Scholar] [CrossRef] [PubMed]
- Farci, P.; Niro, G. Clinical Features of Hepatitis D. Semin. Liver Dis. 2012, 32, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Roca Suarez, A.A.; Batbold, E.; Bartosch, B.; Dashdorj, N.; Testoni, B.; Zoulim, F. Emerging Anti-HDV Drugs and HBV Cure Strategies with Anti-HDV Activity. Liver Int. 2023, 43, 87–95. [Google Scholar] [CrossRef]
- Lempp, F.A.; Roggenbach, I.; Nkongolo, S.; Sakin, V.; Schlund, F.; Schnitzler, P.; Wedemeyer, H.; Le Gal, F.; Gordien, E.; Yurdaydin, C.; et al. A Rapid Point-of-Care Test for the Serodiagnosis of Hepatitis Delta Virus Infection. Viruses 2021, 13, 2371. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Shen, X.; Lu, J.; Zhang, L. Development of a Reverse Transcription-Loop-Mediated Isothermal Amplification (RT-LAMP) System for Rapid Detection of HDV Genotype 1. Lett. Appl. Microbiol. 2013, 56, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.B.; Simmonds, P.; members of the International Committee on the Taxonomy of Viruses Study Group; Jameel, S.; Emerson, S.U.; Harrison, T.J.; Meng, X.-J.; Okamoto, H.; Van Der Poel, W.H.M.; Purdy, M.A. Consensus Proposals for Classification of the Family Hepeviridae. J. Gen. Virol. 2014, 95, 2223–2232. [Google Scholar] [CrossRef]
- Zhang, W.; Ami, Y.; Suzaki, Y.; Kataoka, M.; Takeda, N.; Muramatsu, M.; Li, T. A Cross-Species Transmission of a Camel-Derived Genotype 8 Hepatitis E Virus to Rabbits. Pathogens 2021, 10, 1374. [Google Scholar] [CrossRef] [PubMed]
- Adlhoch, C.; Avellon, A.; Baylis, S.A.; Ciccaglione, A.R.; Couturier, E.; De Sousa, R.; Epštein, J.; Ethelberg, S.; Faber, M.; Fehér, Á.; et al. Hepatitis E Virus: Assessment of the Epidemiological Situation in Humans in Europe, 2014/15. J. Clin. Virol. 2016, 82, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Boccia, D.; Guthmann, J.-P.; Klovstad, H.; Hamid, N.; Tatay, M.; Ciglenecki, I.; Nizou, J.-Y.; Nicand, E.; Guerin, P.J. High Mortality Associated with an Outbreak of Hepatitis E among Displaced Persons in Darfur, Sudan. Clin. Infect. Dis. 2006, 42, 1679–1684. [Google Scholar] [CrossRef]
- Fujiwara, S.; Yokokawa, Y.; Morino, K.; Hayasaka, K.; Kawabata, M.; Shimizu, T. Chronic Hepatitis E: A Review of the Literature. J. Viral Hepat. 2014, 21, 78–89. [Google Scholar] [CrossRef]
- Peron, J.-M.; Larrue, H.; Izopet, J.; Buti, M. The Pressing Need for a Global HEV Vaccine. J. Hepatol. 2023, 79, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Pischke, S.; Hardtke, S.; Bode, U.; Birkner, S.; Chatzikyrkou, C.; Kauffmann, W.; Bara, C.L.; Gottlieb, J.; Wenzel, J.; Manns, M.P.; et al. Ribavirin Treatment of Acute and Chronic Hepatitis E: A Single-Centre Experience. Liver Int. 2013, 33, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Aslan, A.T.; Balaban, H.Y. Hepatitis E Virus: Epidemiology, Diagnosis, Clinical Manifestations, and Treatment. World J. Gastroenterol. 2020, 26, 5543–5560. [Google Scholar] [CrossRef] [PubMed]
- Chandra, N.S.; Sharma, A.; Malhotra, B.; Rai, R.R. Dynamics of HEV Viremia, Fecal Shedding and Its Relationship with Transaminases and Antibody Response in Patients with Sporadic Acute Hepatitis E. Virol. J. 2010, 7, 213. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Lu, Y.; Howard, T.; Anderson, D.; Fong, P.Y.; Hu, W.-P.; Chia, C.P.; Guan, M. Comparison of a New Immunochromatographic Test to Enzyme-Linked Immunosorbent Assay for Rapid Detection of Immunoglobulin M Antibodies to Hepatitis E Virus in Human Sera. Clin. Diagn. Lab. Immunol. 2005, 12, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Chionne, P.; Madonna, E.; Pisani, G.; Taffon, S.; La Rosa, G.; Candido, A.; Dettori, S.; Tritarelli, E.; Equestre, M.; Bruni, R.; et al. Evaluation of Rapid Tests for Diagnosis of Acute Hepatitis E. J. Clin. Virol. 2016, 78, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Myint, K.S.A.; Guan, M.; Chen, H.Y.; Lu, Y.; Anderson, D.; Howard, T.; Noedl, H.; Mammen, M.P. Evaluation of a New Rapid Immunochromatographic Assay for Serodiagnosis of Acute Hepatitis E Infection. Am. J. Trop. Med. Hyg. 2005, 73, 942–946. [Google Scholar] [CrossRef]
- Legrand-Abravanel, F.; Thevenet, I.; Mansuy, J.-M.; Saune, K.; Vischi, F.; Peron, J.-M.; Kamar, N.; Rostaing, L.; Izopet, J. Good Performance of Immunoglobulin M Assays in Diagnosing Genotype 3 Hepatitis E Virus Infections. Clin. Vaccine Immunol. 2009, 16, 772–774. [Google Scholar] [CrossRef]
- Al-Absi, E.S.; Al-Sadeq, D.W.; Younis, M.H.; Yassine, H.M.; Abdalla, O.M.; Mesleh, A.G.; Hadwan, T.A.; Amimo, J.O.; Thalib, L.; Nasrallah, G.K. Performance Evaluation of Five Commercial Assays in Assessing Seroprevalence of HEV Antibodies among Blood Donors. J. Med. Microbiol. 2018, 67, 1302–1309. [Google Scholar] [CrossRef]
- Ying, D.; Hong, C.; Wen, G.; Tang, Z.; Wang, S.; Zhang, X.; Liu, C.; Ge, S.; Zheng, Z.; Xia, N. Development and Evaluation of a Rapid Point-of-Care Test for Detecting the Hepatitis E Virus Antigen. Clin. Biochem. 2018, 55, 89–92. [Google Scholar] [CrossRef]
- Lan, X.; Yang, B.; Li, B.Y.; Yin, X.P.; Li, X.R.; Liu, J.X. Reverse Transcription-Loop-Mediated Isothermal Amplification Assay for Rapid Detection of Hepatitis E Virus. J. Clin. Microbiol. 2009, 47, 2304–2306. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Yuan, L.; Wan, J.; Chen, Y.; Du, C. Colorimetric Detection of Hepatitis E Virus Based on Reverse Transcription Loop Mediated Isothermal Amplification (RT-LAMP) Assay. J. Virol. Methods 2014, 197, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Li, D.; Liu, Y.; Zha, E.; Wang, S.; Li, Y.; Zhou, T.; Yue, X. Development and Evaluation of a RT-LAMP Assay for Rapid Detection of Hepatitis E Virus from Shellfish. Int. J. Food Microbiol. 2016, 220, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.-Q.; Zhao, F.-R.; Liu, Z.-G.; Kong, W.-L.; Wang, H.; Ouyang, Y.; Liang, H.-B.; Zhang, C.-Y.; Qi, H.-T.; Huang, C.-L.; et al. Simple and Rapid Detection of Swine Hepatitis E Virus by Reverse Transcription Loop-Mediated Isothermal Amplification. Arch. Virol. 2012, 157, 2383–2388. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wang, J.; Zhou, C.; Sun, X.; Liu, L.; Xu, X.; Wang, J. Rapid and Direct Detection of Hepatitis E Virus in Raw Pork Livers by Recombinase Polymerase Amplification Assays. Front. Cell. Infect. Microbiol. 2022, 12, 958990. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.; Salvador, D.; Brandão, J.; Ahmed, W.; Sadowsky, M.J.; Valério, E. Environmental and Adaptive Changes Necessitate a Paradigm Shift for Indicators of Fecal Contamination. Microbiol. Spectr. 2020, 8. [Google Scholar] [CrossRef]
- Guerrero-Latorre, L.; Carratala, A.; Rodriguez-Manzano, J.; Calgua, B.; Hundesa, A.; Girones, R. Occurrence of Water-Borne Enteric Viruses in Two Settlements Based in Eastern Chad: Analysis of Hepatitis E Virus, Hepatitis A Virus and Human Adenovirus in Water Sources. J. Water Health 2011, 9, 515–524. [Google Scholar] [CrossRef]
- Tripathy, A.S.; Sharma, M.; Deoshatwar, A.R.; Babar, P.; Bharadwaj, R.; Bharti, O.K. Study of a Hepatitis E Virus Outbreak Involving Drinking Water and Sewage Contamination in Shimla, India, 2015–2016. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 789–796. [Google Scholar] [CrossRef]
- Aguado, D.; Fores, E.; Guerrero-Latorre, L.; Rusiñol, M.; Martínez-Puchol, S.; Codony, F.; Girones, R.; Bofill-Mas, S. VirWaTest, A Point-of-Use Method for the Detection of Viruses in Water Samples. J. Vis. Exp. 2019, e59463. [Google Scholar] [CrossRef]
- Keahey, P.A.; Simeral, M.L.; Schroder, K.J.; Bond, M.M.; Mtenthaonnga, P.J.; Miros, R.H.; Dube, Q.; Richards-Kortum, R.R. Point-of-Care Device to Diagnose and Monitor Neonatal Jaundice in Low-Resource Settings. Proc. Natl. Acad. Sci. USA 2017, 114, E10965–E10971. [Google Scholar] [CrossRef]
- Jain, S.; Rajasingham, R.; Noubary, F.; Coonahan, E.; Schoeplein, R.; Baden, R.; Curry, M.; Afdhal, N.; Kumar, S.; Pollock, N.R. Performance of an Optimized Paper-Based Test for Rapid Visual Measurement of Alanine Aminotransferase (ALT) in Fingerstick and Venipuncture Samples. PLoS ONE 2015, 10, e0128118. [Google Scholar] [CrossRef] [PubMed]
- Howell, J.; Van, H.; Pham, M.D.; Sawhney, R.; Li, F.; Bhat, P.; Lubel, J.; Kemp, W.; Bloom, S.; Majumdar, A.; et al. Validation of a Novel Point-of-care Test for Alanine Aminotransferase Measurement: A Pilot Cohort Study. Liver Int. 2023, 43, 989–999. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Virus | Marker | Interpretation |
|---|---|---|
| HAV | IgG anti-HAV | past HAV infection or HAV vaccination |
| IgM anti-HAV | current or recent HAV infection | |
| HAV RNA | current HAV infection | |
| HAV capsid antigen | current HAV infection | |
| HBV | IgM anti-HBc | acute HBV infection |
| total anti-HBc | current or resolved HBV infection | |
| anti-HBs | resolved HBV infection or HBV vaccination | |
| anti-HBe | partial immune control of HBV infection | |
| HBV DNA | current HBV infection | |
| HBsAg | current HBV infection | |
| HBeAg | early-stage or chronic pre-seroconversion HBV infection | |
| HCV | anti-HCV | current or resolved HCV infection |
| HCV RNA | current HCV infection | |
| cAg | current HCV infection | |
| HDV | anti-HDV | current or resolved HDV infection |
| HDV RNA | current HDV infection | |
| HDAg | current HDV infection | |
| HEV | IgG anti-HEV | past HEV infection or HEV vaccination |
| IgM anti-HEV | current or recent HEV infection | |
| HEV RNA | current HEV infection | |
| HEV capsid antigen | current HEV infection |
| Test Analyte | Test Name (Company) | Sample Types | Time (min.) |
|---|---|---|---|
| HBsAg | Determine HBsAg 2 (Alere Medical, Waltham, MA, USA) | venous or capillary blood, plasma, or serum | 15–30 |
| HBsAg | Bioline HBsAg (Abbott Diagnostics, Abbott Park, Il, USA) | venous blood, plasma, or serum | 20 |
| anti-HCV | Rapid Anti-HCV Test (InTec Products, Xiamen, China) | venous or capillary blood, plasma, or serum | 15–20 |
| anti-HCV | Standard Q HCV Ab Test (SD Biosensor, Suwan, Republic of Korea) | venous or capillary blood, plasma, or serum | 5–20 |
| anti-HCV | OraQuick HCV Rapid Antibody Test (OraSure Technologies, Bethlehem, PA, USA) | venous or capillary blood, plasma, serum, or oral fluids | 20–40 |
| anti-HCV | Bioline HCV (Abbott Diagnostics, Abbott Park, IL, USA) | venous or capillary blood, plasma, or serum | 5–20 |
| HCV RNA | Genedrive HCV ID kit (Genedrive, Manchester, United Kingdom) | plasma and serum | 90 |
| HCV RNA | Xpert HCV Viral Load (Cepheid, Sunnyvale, CA, USA) | plasma or serum | 105 |
| HCV RNA | Xpert HCV VL Fingerstick (Cepheid, Sunnyvale, CA, USA) | venous or capillary blood | 60–75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pauly, M.D.; Ganova-Raeva, L. Point-of-Care Testing for Hepatitis Viruses: A Growing Need. Life 2023, 13, 2271. https://doi.org/10.3390/life13122271
Pauly MD, Ganova-Raeva L. Point-of-Care Testing for Hepatitis Viruses: A Growing Need. Life. 2023; 13(12):2271. https://doi.org/10.3390/life13122271
Chicago/Turabian StylePauly, Matthew D., and Lilia Ganova-Raeva. 2023. "Point-of-Care Testing for Hepatitis Viruses: A Growing Need" Life 13, no. 12: 2271. https://doi.org/10.3390/life13122271
APA StylePauly, M. D., & Ganova-Raeva, L. (2023). Point-of-Care Testing for Hepatitis Viruses: A Growing Need. Life, 13(12), 2271. https://doi.org/10.3390/life13122271