
A Meta-Analysis of Sampled Maximal Aerobic Capacity Data for Boys Aged 11 Years Old or Less Obtained by Cycle Ergometry

Abstract
:1. Introduction
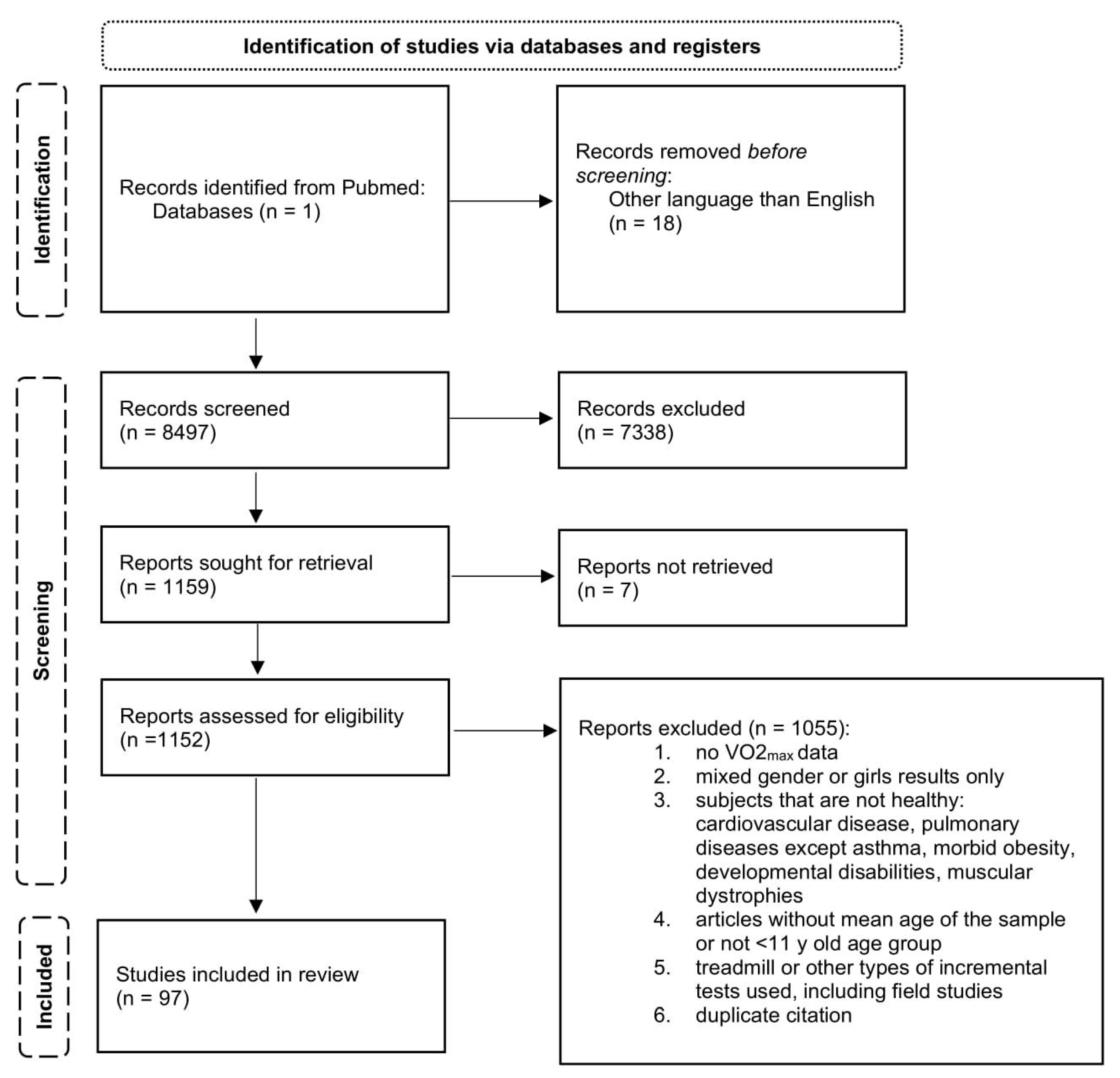
2. Materials and Methods
2.1. Design
2.2. Population
2.3. Intervention
2.4. Comparator
2.5. Outcomes
2.6. Study Design
2.7. Statistical Analysis
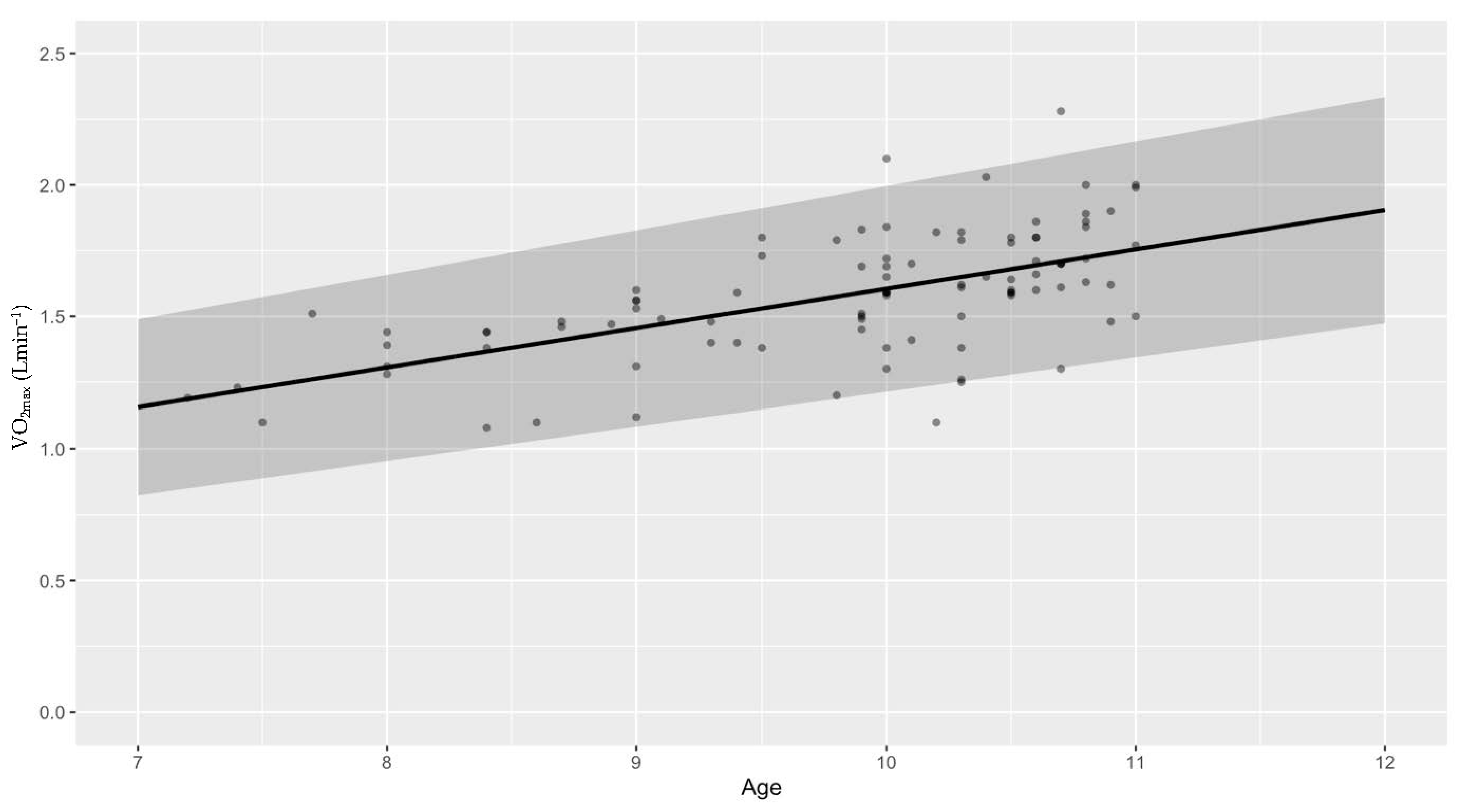
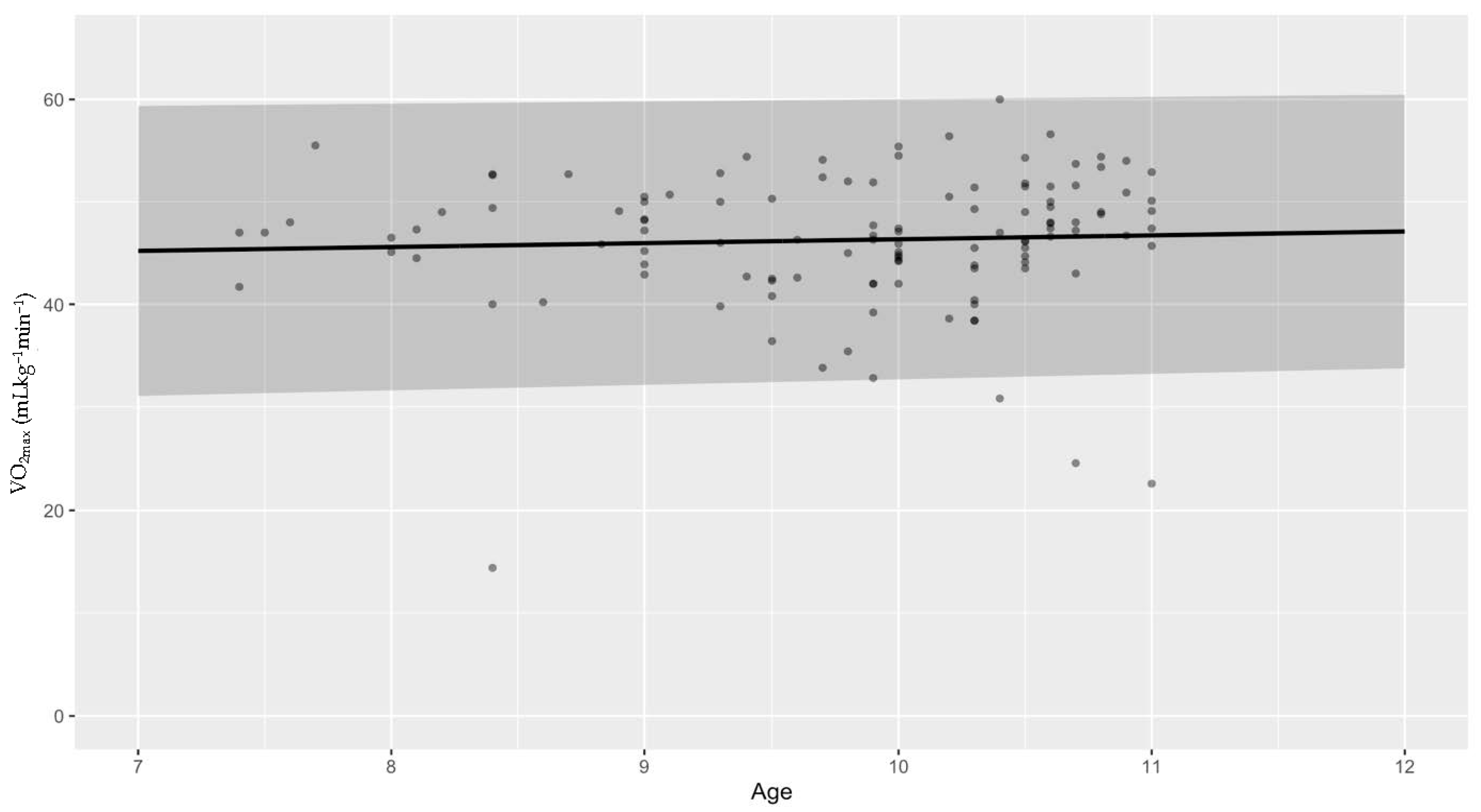
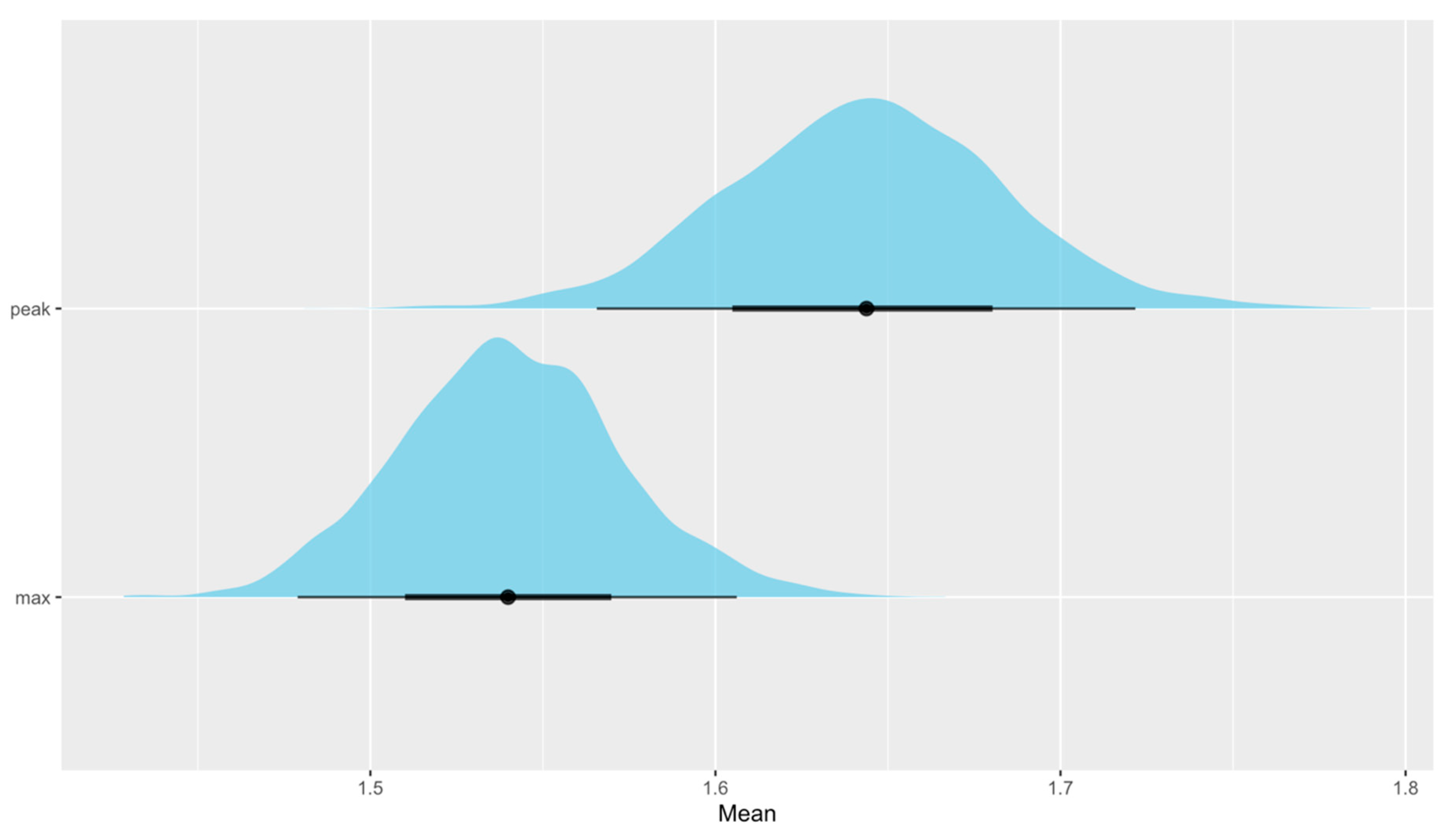
3. Results
3.1. Is There Any Difference between Boys and Girls?
3.2. Models in Practice
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takken, T.; Bongers, B.C.; van Brussel, M.; Haapala, E.A.; Hulzebos, E.H.J. Cardiopulmonary Exercise Testing in Pediatrics. Ann. Am. Thorac. Soc. 2017, 14 (Suppl. S1), S123–S128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balady, G.J.; Arena, R.; Sietsema, K.; Myers, J.; Coke, L.; Fletcher, G.F.; Forman, D.; Franklin, B.; Guazzi, M.; Gulati, M.; et al. Clinician’s Guide to Cardiopulmonary Exercise Testing in Adults: A Scientific Statement from the American Heart Association. Circulation 2010, 122, 191–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palange, P.; Laveneziana, P.; Neder, J.A.; Ward, S.A. Clinical Exercise Testing; Palange, P., Laveneziana, P., Neder, J.A., Ward, S.A., Eds.; European Respiratory Society: Sheffield, UK, 2018. [Google Scholar]
- Forbregd, T.R.; Aloyseus, M.A.; Berg, A.; Greve, G. Cardiopulmonary Capacity in Children During Exercise Testing: The Differences Between Treadmill and Upright and Supine Cycle Ergometry. Front. Physiol. 2019, 10, 1440. [Google Scholar] [CrossRef]
- Bergh, U.; Kanstrup, I.L.; Ekblom, B. Maximal Oxygen Uptake during Exercise with Various Combinations of Arm and Leg Work. J. Appl. Physiol. 1976, 41, 191–196. [Google Scholar] [CrossRef] [PubMed]
- LeMura, L.M.; von Duvillard, S.P.; Cohen, S.L.; Root, C.J.; Chelland, S.A.; Andreacci, J.; Hoover, J.; Weatherford, J. Treadmill and Cycle Ergometry Testing in 5- to 6-Year-Old Children. Eur. J. Appl. Physiol. 2001, 85, 472–478. [Google Scholar] [CrossRef]
- Armstrong, N. Aerobic Fitness and Physical Activity in Children. Pediatr. Exerc. Sci. 2013, 25, 548–560. [Google Scholar] [CrossRef]
- Whiting, S.; Buoncristiano, M.; Gelius, P.; Abu-Omar, K.; Pattison, M.; Hyska, J.; Duleva, V.; Musić Milanović, S.; Zamrazilová, H.; Hejgaard, T.; et al. Physical Activity, Screen Time, and Sleep Duration of Children Aged 6–9 Years in 25 Countries: An Analysis within the WHO European Childhood Obesity Surveillance Initiative (COSI) 2015–2017. Obes. Facts 2021, 14, 32. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Rosenkranz, R.R.; Dzewaltowski, D. Physical Activity Levels among Children Attending After-School Programs. Med. Sci. Sports Exerc. 2008, 40, 622–629. [Google Scholar] [CrossRef]
- Hinkley, T.; Crawford, D.; Salmon, J.; Okely, A.D.; Hesketh, K. Preschool Children and Physical Activity. A Review of Correlates. Am. J. Prev. Med. 2008, 34, 435–441. [Google Scholar] [CrossRef]
- Bailey, R.C.; Olson, J.; Pepper, S.L.; Porszasz, J.; Barstow, T.J.; Cooper, D.M. The Level and Tempo of Children’s Physical Activities: An Observational Study. Med. Sci. Sports Exerc. 1995, 27, 1033–1041. [Google Scholar] [CrossRef]
- Pate, R.R.; O’Neill, J.R.; Liese, A.D.; Janz, K.F.; Granberg, E.M.; Colabianchi, N.; Harsha, D.W.; Condrasky, M.M.; O’Neil, P.M.; Lau, E.Y.; et al. Factors Associated with Development of Excessive Fatness in Children and Adolescents: A Review of Prospective Studies. Obes. Rev. 2013, 14, 645–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, N.; Welsman, J.R. Assessment and Interpretation of Aerobic Fitness in Children and Adolescents. Exerc. Sport Sci. Rev. 1994, 22, 435–476. [Google Scholar] [CrossRef] [PubMed]
- Crisp, N.A.; Guelfi, K.J.; Licari, M.K.; Braham, R.; Fournier, P.A. Does Exercise Duration Affect Fat Max in Overweight Boys? Eur. J. Appl. Physiol. 2012, 112, 2557–2564. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.A.; Paterson, D.H.; Blimkie, C.J.R.; Donner, A.P. Development of Cardiorespiratory Function in Circumpubertal Boys: A Longitudinal Study. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1984, 56, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Welsh, L.; Roberts, R.G.D.; Kemp, J.G. Fitness and Physical Activity in Children with Asthma. Sport. Med. 2004, 34, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Stan Development Team RStan: The R Interface to Stan. Available online: https://mc-stan.org/ (accessed on 5 May 2022).
- Field, A.P. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2018; p. 368. [Google Scholar]
- Odor, P.M.; Bampoe, S.; Cecconi, M. Cardiac Output Monitoring: Validation Studies–How Results Should Be Presented. Curr. Anesthesiol. Rep. 2017, 7, 410–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agbaje, A.O.; Haapala, E.A.; Lintu, N.; Viitasalo, A.; Barker, A.R.; Takken, T.; Tompuri, T.; Lindi, V.; Lakka, T.A. Peak Oxygen Uptake Cut-Points to Identify Children at Increased Cardiometabolic Risk–The PANIC Study. Scand. J. Med. Sci. Sports 2019, 29, 16–24. [Google Scholar] [CrossRef]
- Andersen, K.L.; Ghesquiere, J. Sex Differences in Maximal Oxygen Uptake, Heart Rate and Oxygen Pulse at 10 and 14 Years in Norwegian Children. Hum. Biol. 1972, 44, 413–431. [Google Scholar]
- Arngrímsson, S.Á.; Sveinsson, T.; Jóhannsson, E. Peak Oxygen Uptake in Children: Evaluation of an Older Prediction Method and Development of a New One. Pediatr. Exerc. Sci. 2008, 20, 62–73. [Google Scholar] [CrossRef]
- Crisp, N.A.; Fournier, P.A.; Licari, M.K.; Braham, R.; Guelfi, K.J. Adding Sprints to Continuous Exercise at the Intensity That Maximises Fat Oxidation: Implications for Acute Energy Balance and Enjoyment. Metabolism 2012, 61, 1280–1288. [Google Scholar] [CrossRef]
- Davies, C.T.; Barnes, C.; Godfrey, S. Body Composition and Maximal Exercise Performance in Children. Hum. Biol. 1972, 44, 195–214. [Google Scholar] [PubMed]
- de Jonge, R. Effect of Anthropometric Characteristics and Socio-Economic Status on Physical Performances of Pre-Pubertal Children Living in Bolivia at Low Altitude. Eur. J. Appl. Physiol. Occup. Physiol. 1996, 74, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Del Corral, P.; Mahon, A.D.; Duncan, G.E.; Howe, C.A.; Craig, B.W. The Effect of Exercise on Serum and Salivary Cortisol in Male Children. Med. Sci. Sports Exerc. 1994, 26, 1297–1301. [Google Scholar] [CrossRef] [PubMed]
- Docherty, D.; Gaul, C.A. Relationship of Body Size, Physique, and Composition to Physical Performance in Young Boys and Girls. Int. J. Sports Med. 1991, 12, 525–532. [Google Scholar] [CrossRef]
- Dunstheimer, D.; Hebestreit, H.; Staschen, B.; Starßburg, H.M.; Jeschke, R. Bilateral Deficit during Short-Term, High-Intensity Cycle Ergometry in Girls and Boys. Eur. J. Appl. Physiol. 2001, 84, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Dzurenkova, D.; Marcek, T.; Hajkova, M. Specialities of Assessment of Endurance Capabilities in Sport Active Children. Bratisl. Lek. Listy 2001, 102, 432–433. [Google Scholar]
- Farr, C.; Middlebrooke, A.R.; Armstrong, N.; Barker, A.R.; Fulford, J.; Mawson, D.M.; McManus, A.M. Objectively Measured Aerobic Fitness Is Not Related to Vascular Health Outcomes and Cardiovascular Disease Risk in 9-10 Year Old Children. J. Sports Sci. Med. 2019, 18, 513–522. [Google Scholar] [PubMed]
- Fawkner, S.G.; Armstrong, N. Sex Differences in the Oxygen Uptake Kinetic Response to Heavy-Intensity Exercise in Prepubertal Children. Eur. J. Appl. Physiol. 2004, 93, 210–216. [Google Scholar] [CrossRef]
- Friberg, S.; Bevegård, S.; Graff-Lonnevig, V.; Hallbäck, I. Asthma from Childhood to Adulthood-A Follow-up Study of 20 Subjects with Special Reference to Work Capacity and Pulmonary Gas Exchange. J. Allergy Clin. Immunol. 1989, 84, 183–190. [Google Scholar] [CrossRef]
- Gaisl, G.; Buchberger, J. Determination of the Aerobic and Anaerobic Thresholds of 10-11-Year-Old Boys Using Blood-Gas Analysis; Berg, W., Eriksson, B.O., Eds.; University Park Press: Baltimore, MD, USA, 1980. [Google Scholar]
- Gilliam, T.B.; Katch, V.L.; Thorland, W.; Weltman, A. Prevalence of Coronary Heart Disease Risk Factors in Active Children, 7 to 12 Years of Age. Med. Sci. Sports Exerc. 1977, 9, 21–25. [Google Scholar] [CrossRef]
- Hansen, H.S.; Froberg, K.; Nielsen, J.R.; Hyldebrandt, N. A New Approach to Assessing Maximal Aerobic Power in Children: The Odense School Child Study. Eur. J. Appl. Physiol. Occup. Physiol. 1989, 58, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Hermansen, L.; Oseid, S. Direct and Indirect Estimation of Maximal Oxygen Uptake in Pre-Pubertal Boys. Acta Paediatr. Scand. Suppl. 1971, 217, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Ikai, M.; Kitagawa, K. Maximum Oxygen Uptake of Japanese Related to Sex and Age. Med. Sci. Sports Exerc. 1972, 4, 127–131. [Google Scholar] [CrossRef]
- Inbar, O.; Bar-Or, O. The Effects of Intermittent Warm-up on 7-9 Year-Old Boys. Eur. J. Appl. Physiol. Occup. Physiol. 1975, 34, 81–89. [Google Scholar] [CrossRef]
- Janz, K.F.; Burns, T.L.; Witt, J.D.; Mahoney, L.T. Longitudinal Analysis of Scaling VO2 for Differences in Body Size during Puberty: The Muscatine Study. Med. Sci. Sports Exerc. 1998, 30, 1436–1444. [Google Scholar] [CrossRef]
- Janz, K.F.; Dawson, J.D.; Mahoney, L.T. Tracking Physical Fitness and Physical Activity from Childhood to Adolescence: The Muscatine Study. Med. Sci. Sports Exerc. 2000, 32, 1250–1257. [Google Scholar] [CrossRef] [Green Version]
- Kolle, E.; Steene-Johannessen, J.; Andersen, L.B.; Anderssen, S.A. Objectively Assessed Physical Activity and Aerobic Fitness in a Population-Based Sample of Norwegian 9- and 15-Year-Olds. Scand. J. Med. Sci. Sports 2010, 20, e41–e47. [Google Scholar] [CrossRef]
- Kowaluk, A.; Woźniewski, M. Peak Oxygen Uptake and Exercise Capacity of Children Undergoing Leukemia Treatment. Int. J. Environ. Res. Public Health 2020, 17, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Lange Andersen, K.; Seliger, V.; Rutenfranz, J.; Skrobak-Kaczynski, J. Physical Performance Capacity of Children in Norway-Part IV. The Rate of Growth in Maximal Aerobic Power and the Influence of Improved Physical Education of Children in a Rural Community-Population Parameters in a Rural Community. Eur. J. Appl. Physiol. Occup. Physiol. 1976, 35, 49–58. [Google Scholar] [CrossRef]
- Lange Andersen, K.; Seliger, V.; Rutenfranz, J.; Mocellin, R. Physical Performance Capacity of Children in Norway-Part I. Population Parameters in a Rural Inland Community with Regard to Maximal Aerobic Power. Eur. J. Appl. Physiol. Occup. Physiol. 1974, 33, 177–195. [Google Scholar] [CrossRef]
- Lazzer, S.; Molin, M.; Stramare, D.; Facchini, S.; Francescato, M.P. Effects of an Eight-Month Weight-Control Program on Body Composition and Lipid Oxidation Rate during Exercise in Obese Children. J. Endocrinol. Invest. 2008, 31, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Lintu, N.; Viitasalo, A.; Tompuri, T.; Veijalainen, A.; Hakulinen, M.; Laitinen, T.; Savonen, K.; Lakka, T.A. Cardiorespiratory Fitness, Respiratory Function and Hemodynamic Responses to Maximal Cycle Ergometer Exercise Test in Girls and Boys Aged 9–11 Years: The PANIC Study. Eur. J. Appl. Physiol. 2015, 115, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.D.; Bar-Yoseph, R.; Radom-Aizik, S.; Cooper, D.M. A New Approach to Estimate Aerobic Fitness Using the NHANES Dataset. Scand. J. Med. Sci. Sports 2019, 29, 1392–1401. [Google Scholar] [CrossRef] [PubMed]
- Mahon, A.D.; Stephens, B.R.; Cole, A.S. Exercise Responses in Boys with Attention Deficit/Hyperactivity Disorder: Effects of Stimulant Medication. J. Atten. Disord. 2008, 12, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Massicotte, D.R.; Gauthier, R.; Markon, P. Prediction of VO2max from the Running Performance in Children Aged 10-17 Years. J. Sport. Med. Phys. Fit. 1985, 25, 10–17. [Google Scholar]
- McManus, A.M.; Cheng, C.H.; Leung, M.P.; Yung, T.C.; Macfarlane, D.J. Improving Aerobic Power in Primary School Boys: A Comparison of Continuous and Interval Training. Int. J. Sports Med. 2005, 26, 781–786. [Google Scholar] [CrossRef]
- McMurray, R.G.; Harrell, J.S.; Bradley, C.; Deng, S.; Bangdiwala, S.I. Predicted Maximal Aerobic Power in Youth Is Related to Gender, Ethnicity, and Body Composition. Med. Sci. Sports Exerc. 2001, 33, S31. [Google Scholar] [CrossRef]
- McNarry, M.A.; Farr, C.; Middlebrooke, A.; Welford, D.; Breese, B.; Armstrong, N.; Barker, A.R. Aerobic Function and Muscle Deoxygenation Dynamics during Ramp Exercise in Children. Med. Sci. Sports Exerc. 2015, 47, 1877–1884. [Google Scholar] [CrossRef] [Green Version]
- Nourry, C.; Fabre, C.; Bart, F.; Grosbois, J.M.; Berthoin, S.; Mucci, P. Evidence of Exercise-Induced Arterial Hypoxemia in Prepubescent Trained Children. Pediatr. Res. 2004, 55, 674–681. [Google Scholar] [CrossRef] [Green Version]
- Ortega, F.B.; Ruiz, J.R.; Hurtig-Wennlöf, A.; Vicente-Rodríguez, G.; Rizzo, N.S.; Castillo, M.J.; Sjöström, M. Cardiovascular Fitness Modifies the Associations between Physical Activity and Abdominal Adiposity in Children and Adolescents: The European Youth Heart Study. Br. J. Sports Med. 2010, 44, 256–262. [Google Scholar] [CrossRef] [Green Version]
- Peralta-Huertas, J.; Livingstone, K.; Banach, A.; Klentrou, P.; O’Leary, D. Differences in Left Ventricular Mass between Overweight and Normal-Weight Preadolescent Children. Appl. Physiol. Nutr. Metab. 2008, 33, 1172–1180. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Brown, A.M.; Alvarez, M.; Rodríguez-Santana, J.R.; Benetti, P.J. Anaerobic Power and Achievement of VO2 Plateau in Pre-Pubertal Boys. Int. J. Sports Med. 2001, 22, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Robertson, R.J.; Goss, F.L.; Boer, N.; Gallagher, J.D.; Thompkins, T.; Bufalino, K.; Balasekaran, G.; Meckes, C.; Pintar, J.; Williams, A. OMNI Scale Perceived Exertion at Ventilatory Breakpoint in Children: Response Normalized. Med. Sci. Sports Exerc. 2001, 33, 1946–1952. [Google Scholar] [CrossRef] [PubMed]
- Rowland, T.W.; Rambusch, J.M.; Staab, J.S.; Unnithan, V.B.; Siconolfi, S.F. Accuracy of Physical Working Capacity (PWC170) in Estimating Aerobic Fitness in Children. J. Sport. Med. Phys. Fit. 1993, 33, 184–188. [Google Scholar]
- Rowland, T.W. The Development of Aerobic Fitness in Children; Armstrong, N., Ed.; E & FN Spon.: London, UK, 1997. [Google Scholar]
- Rowland, T.W. Does Peak VO2 Reflect VO2max in Children?: Evidence from Supramaximal Testing. Med. Sci. Sports Exerc. 1993, 25, 689–693. [Google Scholar] [CrossRef]
- Rutenfranz, J.; Andersen, K.L.; Seliger, V.; Klimmer, F.; Berndt, I.; Ruppel, M. Maximum Aerobic Power and Body Composition during the Puberty Growth Period: Similarities and Differences between Children of Two European Countries. Eur. J. Pediatr. 1981, 136, 123–133. [Google Scholar] [CrossRef]
- Mandigout, S.; Lecoq, A.; Courteix, D.; Guenon, P.; Obert, P. Effect of Gender in Response to an Aerobic Training Programme in Prepubertal Children. Acta Paediatr. 2001, 90, 9–15. [Google Scholar] [CrossRef]
- Sockolov, R.; Irwin, B.; Dressendorfer, R.H.; Bernauer, E.M. Exercise Performance in 6 to 11 Year Old Boys with Duchenne Muscular Dystrophy. Arch. Phys. Med. Rehabil. 1977, 58, 195–201. [Google Scholar]
- Sunnegårdh, J.; Bratteby, L.E. Maximal Oxygen Uptake, Anthropometry and Physical Activity in a Randomly Selected Sample of 8 and 13 Year Old Children in Sweden. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 266–272. [Google Scholar] [CrossRef]
- Swain, K.E.; Rosenkranz, S.K.; Beckman, B.; Harms, C.A. Expiratory Flow Limitation during Exercise in Prepubescent Boys and Girls: Prevalence and Implications. J. Appl. Physiol. 2010, 108, 1267–1274. [Google Scholar] [CrossRef] [Green Version]
- Tolfrey, K.; Campbell, I.G.; Batterham, A.M. Aerobic Trainability of Prepubertal Boys and Girls. Pediatr. Excercise Sci. 1998, 10, 248–263. [Google Scholar] [CrossRef]
- Tompuri, T.; Lintu, N.; Savonen, K.; Laitinen, T.; Laaksonen, D.; Jääskeläinen, J.; Lakka, T.A. Measures of Cardiorespiratory Fitness in Relation to Measures of Body Size and Composition among Children. Clin. Physiol. Funct. Imaging 2015, 35, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Turley, K.R.; Rogers, D.M.; Harper, K.M.; Kujawa, K.I.; Wilmore, J.H. Maximal Treadmill versus Cycle Ergometry Testing in Children: Differences, Reliability, and Variability of Responses. Pediatr. Exerc. Sci. 1995, 7, 49–60. [Google Scholar] [CrossRef]
- Turley, K.R.; Wilmore, J.H. Cardiovascular Responses to Submaximal Exercise in 7- to 9-Yr-Old Boys and Girls. Med. Sci. Sports Exerc. 1997, 29, 824–832. [Google Scholar] [CrossRef]
- Van Praagh, E.; Bedu, M.; Falgairette, G.; Fellmann, N.; Coudert, J. Comparaison Entre over VO2 Max Direct et Indirect Chez l’enfant de 7 et 12 Ans. Validation d’une Épreuve de Terrain. Sci. Sports 1988, 3, 327–332. [Google Scholar] [CrossRef]
- Vandekerckhove, K.; Coomans, I.; Moerman, A.; De Wolf, D.; Boone, J. Characterizing Cerebral and Locomotor Muscle Oxygenation to Incremental Ramp Exercise in Healthy Children: Relationship with Pulmonary Gas Exchange. Eur. J. Appl. Physiol. 2016, 116, 2345–2355. [Google Scholar] [CrossRef] [PubMed]
- Vinet, A.; Mandigout, S.; Nottin, S.; Nguyen, L.D.; Lecoq, A.M.; Courteix, D.; Obert, P. Influence of Body Composition, Hemoglobin Concentration, and Cardiac Size and Function of Gender Differences in Maximal Oxygen Uptake in Prepubertal Children. Chest 2003, 124, 1494–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Washington, R.L.; van Gundy, J.C.; Cohen, C.; Sondheimer, H.M.; Wolfe, R.R. Normal Aerobic and Anaerobic Exercise Data for North American School-Age Children. J. Pediatr. 1988, 112, 223–233. [Google Scholar] [CrossRef]
- Weber, G.; Kartodihardjo, W.; Klissouras, V. Growth and Physical Training with Reference to Heredity. J. Appl. Physiol. 1976, 40, 211–215. [Google Scholar] [CrossRef]
- Weinstein, Y.; Kamerman, T.; Berry, E.; Falk, B. Mechanical Efficiency of Normal-Weight Prepubertal Boys Predisposed to Obesity. Med. Sci. Sports Exerc. 2004, 36, 567–573. [Google Scholar] [CrossRef]
- Welsman, J.; Bywater, K.; Farr, C.; Welford, D.; Armstrong, N. Reliability of Peak VO2 and Maximal Cardiac Output Assessed Using Thoracic Bioimpedance in Children. Eur. J. Appl. Physiol. 2005, 94, 228–234. [Google Scholar] [CrossRef]
- Winsley, R.J.; Fulford, J.; Roberts, A.C.; Welsman, J.R.; Armstrong, N. Sex Difference in Peak Oxygen Uptake in Prepubertal Children. J. Sci. Med. Sport 2009, 12, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Yamaji, K.; Miyashita, M. Oxygen Transport System during Exhaustive Exercise in Japanese Boys. Eur. J. Appl. Physiol. Occup. Physiol. 1977, 36, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Zebrowska, A.; Zwierzchowska, A. Spirometric Values and Aerobic Efficency of Children and Adolescents with Hearing Loss. J. Physiol. Pharmacol. 2006, 57, 443–447. [Google Scholar] [PubMed]
- Aandstad, A.; Berntsen, S.; Hageberg, R.; Klasson-Heggebø, L.; Anderssen, S.A. A Comparison of Estimated Maximal Oxygen Uptake in 9 and 10 Year Old Schoolchildren in Tanzania and Norway. Br. J. Sports Med. 2006, 40, 287–292. [Google Scholar] [CrossRef]
- Adegboye, A.R.A.; Anderssen, S.A.; Froberg, K.; Sardinha, L.B.; Heitmann, B.L.; Steene-Johannessen, J.; Kolle, E.; Andersen, L.B. Recommended Aerobic Fitness Level for Metabolic Health in Children and Adolescents: A Study of Diagnostic Accuracy. Br. J. Sports Med. 2011, 45, 722–728. [Google Scholar] [CrossRef]
- Barkley, J.E.; Roemmich, J.N. Validity of the CALER and OMNI-Bike Ratings of Perceived Exertion. Med. Sci. Sports Exerc. 2008, 40, 760–766. [Google Scholar] [CrossRef]
- Birat, A.; Bourdier, P.; Piponnier, E.; Blazevich, A.J.; Maciejewski, H.; Duché, P.; Ratel, S. Metabolic and Fatigue Profiles Are Comparable between Prepubertal Children and Well-Trained Adult Endurance Athletes. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Boissière, J.; Maufrais, C.; Baquet, G.; Schuster, I.; Dauzat, M.; Doucende, G.; Obert, P.; Berthoin, S.; Nottin, S. Specific Left Ventricular Twist-Untwist Mechanics during Exercise in Children. J. Am. Soc. Echocardiogr. 2013, 26, 1298–1305. [Google Scholar] [CrossRef]
- Cooper, D.M.; Weiler-Ravell, D.; Whipp, B.J.; Wasserman, K. Aerobic Parameters of Exercise as a Function of Body Size during Growth in Children. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1984, 56, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, D.A.; Telford, P.; Swart, G.T. The Cardiopulmonary Capacities of Young Hockey Players: Age 10. Med. Sci. Sports Exerc. 1976, 8, 23–25. [Google Scholar] [CrossRef]
- Danielson, A.; Thorsson, O.; Karlsson, M.K.; Wollmer, P.; Andersen, L.B.; Dencker, M. School-Based Study Found That Physical Activity and Aerobic Fitness Predicted Increases in Total Body Fat and Abdominal Fat at a Mean Age of 9.8 Years. Acta Paediatr. Int. J. Paediatr. 2018, 107, 1810–1817. [Google Scholar] [CrossRef] [PubMed]
- Dencker, M.; Thorsson, O.; Karlsson, M.K.; Lindén, C.; Svensson, J.; Wollmer, P.; Andersen, L.B. Daily Physical Activity and Its Relation to Aerobic Fitness in Children Aged 8-11 Years. Eur. J. Appl. Physiol. 2006, 96, 587–592. [Google Scholar] [CrossRef] [Green Version]
- DeStefano, R.A.; Caprio, S.; Fahey, J.T.; Tamborlane, W.V.; Goldberg, B. Changes in Body Composition after a 12-Wk Aerobic Exercise Program in Obese Boys. Pediatr. Diabetes 2000, 1, 61–65. [Google Scholar] [CrossRef]
- Dotan, R.; Falk, B.; Raz, A. Intensity Effect of Active Recovery from Glycolytic Exercise on Decreasing Blood Lactate Concentration in Prepubertal Children. Med. Sci. Sports Exerc. 2000, 32, 564–570. [Google Scholar] [CrossRef]
- Falgairette, G.; Bedu, M.; Fellmann, N.; Van-Praagh, E.; Coudert, J. Bio-Energetic Profile in 144 Boys Aged from 6 to 15 Years with Special Reference to Sexual Maturation. Eur. J. Appl. Physiol. Occup. Physiol. 1991, 62, 151–156. [Google Scholar] [CrossRef]
- Falk, B.; Bar-Or, O. Longitudinal Changes in Peak Aerobic and Anaerobic Mechanical Power of Circumpubertal Boys. Pediatr. Exerc. Sci. 1993, 5, 318–331. [Google Scholar] [CrossRef]
- Fellmann, N.; Beaune, B.; Coudert, J. Blood Lactate after Maximal and Supramaximal Exercise in 10- to 12-Year-Old Bolivian Boys Effects of Altitude and Socioeconomic Status. Int. J. Sports Med. 1994, 15, S90–S95. [Google Scholar] [CrossRef]
- Foraita, R.; Brandes, M.; Günther, F.; Bammann, K.; Pigeot, I.; Ahrens, W. The Influence of Aerobic Fitness on Obesity and Its Parent-Offspring Correlations in a Cross-Sectional Study among German Families. BMC Public Health 2015, 15, 638. [Google Scholar] [CrossRef] [Green Version]
- García-Prieto, J.C.; Martinez-Vizcaino, V.; García-Hermoso, A.; Sánchez-López, M.; Arias-Palencia, N.; Fonseca, J.F.O.; Mora-Rodriguez, R. Energy Expenditure in Playground Games in Primary School Children Measured by Accelerometer and Heart Rate Monitors. Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 467–474. [Google Scholar] [CrossRef]
- Guerrero, L.; Naranjo, J.; Carranza, M.D. Influence of Gender on Ventilatory Efficiency during Exercise in Young Children. J. Sports Sci. 2008, 26, 1455–1457. [Google Scholar] [CrossRef] [PubMed]
- Haapala, E.A.; Gao, Y.; Hartikainen, J.; Rantalainen, T.; Finni, T. Associations of Fitness, Motor Competence, and Adiposity with the Indicators of Physical Activity Intensity during Different Physical Activities in Children. Sci. Rep. 2021, 11, 12521. [Google Scholar] [CrossRef]
- Herman, K.M.; Chaput, J.P.; Sabiston, C.M.; Mathieu, M.E.; Tremblay, A.; Paradis, G. Combined Physical Activity/Sedentary Behavior Associations with Indices of Adiposity in 8- to 10-Year-Old Children. J. Phys. Act. Health 2015, 12, 20–29. [Google Scholar] [CrossRef]
- Inbar, O.; Bar-Or, O.; Dotan, R.; Gutin, B. Conditioning versus Exercise in Heat as Methods for Acclimatizing 8- to 10-Yr-Old Boys to Dry Heat. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1981, 50, 406–411. [Google Scholar] [CrossRef]
- Petzl, D.H.; Haber, P.; Schuster, E.; Popow, C.; Haschke, F. Reliability of Estimation of Maximum Performance Capacity on the Basis of Submaximum Ergometric Stress Tests in Children 10-14 Years Old. Eur. J. Pediatr. 1988, 147, 174–178. [Google Scholar] [CrossRef]
- Rivas, E.; Huynh, H.; Galassetti, P.R. Obesity Affects Submaximal Oxygen Uptake-Heart Rate Relationship and Exercise Economy Differently in Pre- and Post-Pubescent Boys and Girls. Int. J. Exerc. Sci. 2019, 12, 748–763. [Google Scholar]
- Rutenfranz, J.; Máček, M.; Lange Andersen, K.; Bell, R.D.; Vávra, J.; Radvanský, J.; Klimmer, F.; Kylian, H. The Relationship between Changing Body Height and Growth Related Changes in Maximal Aerobic Power. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 60, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Schöffl, I.; Ehrlich, B.; Stanger, S.; Rottermann, K.; Dittrich, S.; Schöffl, V. Exercise Field Testing in Children: A New Approach for Age-Appropriate Evaluation of Cardiopulmonary Function. Pediatr. Cardiol. 2020, 41, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Springer, C.; Barstow, T.J.; Wasserman, K.; Cooper, D.M. Oxygen Uptake and Heart Rate Responses during Hypoxic Exercise in Children and Adults. Med. Sci. Sports Exerc. 1991, 23, 71–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steene-Johannessen, J.; Anderssen, S.A.; Kolle, E.; Andersen, L.B. Low Muscle Fitness Is Associated with Metabolic Risk in Youth. Med. Sci. Sports Exerc. 2009, 41, 1361–1367. [Google Scholar] [CrossRef]
- van der Steeg, G.E.; Takken, T. Reference Values for Maximum Oxygen Uptake Relative to Body Mass in Dutch/Flemish Subjects Aged 6–65 Years: The LowLands Fitness Registry. Eur. J. Appl. Physiol. 2021, 121, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Wedderkopp, N.; Froberg, K.; Hansen, H.S.; Riddoch, C.; Andersen, L.B. Cardiovascular Risk Factors Cluster in Children and Adolescents with Low Physical Fitness: The European Youth Heart Study (EYHS). Pediatr. Exerc. Sci. 2003, 15, 419–427. [Google Scholar] [CrossRef]
- Yoshizawa, S. A Comparative Study of Aerobic Work Capacity in Urban and Rural Adolescents. J. Hum. Ergol. 1972, 1, 45–65. [Google Scholar]
- Zunquin, G.; Theunynck, D.; Sesboüé, B.; Arhan, P.; Bouglé, D. Evolution of Fat Oxidation during Exercise in Obese Pubertal Boys: Clinical Implications. J. Sports Sci. 2009, 27, 315–318. [Google Scholar] [CrossRef]
- Langer, R.D.; da Costa, K.G.; Bortolotti, H.; Fernandes, G.A.; de Jesus, R.S.; Gonçalves, E.M. Phase Angle Is Associated with Cardiorespiratory Fitness and Body Composition in Children Aged between 9 and 11 Years. Physiol. Behav. 2020, 215. [Google Scholar] [CrossRef]
- Leclair, E.; Berthoin, S.; Borel, B.; Thevenet, D.; Carter, H.; Baquet, G.; Mucci, P. Faster Pulmonary Oxygen Uptake Kinetics in Children vs Adults Due to Enhancements in Oxygen Delivery and Extraction. Scand. J. Med. Sci. Sports 2013, 23, 705–712. [Google Scholar] [CrossRef]
- Leclair, E.; Mucci, P.; Borel, B.; Baquet, G.; Carter, H.; Berthoin, S. Time to Exhaustion and Time Spent at a High Percentage of Vo2max in Severe Intensity Domain in Children and Adults. J. Strength Cond. Res. 2011, 25, 1151–1158. [Google Scholar] [CrossRef]
- Mahon, A.D.; Anderson, C.S.; Hipp, M.J.; Hunt, K.A. Heart Rate Recovery from Submaximal Exercise in Boys and Girls. Med. Sci. Sports Exerc. 2003, 35, 2093–2097. [Google Scholar] [CrossRef] [Green Version]
- Martin, R.; Hautier, C.; Bedu, M. Effect of Age and Pedalling Rate on Cycling Efficiency and Internal Power in Humans. Eur. J. Appl. Physiol. 2002, 86, 245–250. [Google Scholar] [CrossRef]
- Obert, P.; Mandigouts, S.; Nottin, S.; Vinet, A.; N’Guyen, L.D.; Lecoq, A.M. Cardiovascular Responses to Endurance Training in Children: Effect of Gender. Eur. J. Clin. Invest. 2003, 33, 199–208. [Google Scholar] [CrossRef]
- Bongers, B.C.; Hulzebos, E.H.J.; van Brussel, M.; Takken, T. Pediatric Norms for Cardiopulmonary Exercise Testing: In Relation to Gender and Age; Uitgeverij BOXPRESS: ’s-Hertogenbosch, The Netherlands, 2012; p. 129. [Google Scholar]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, Regional, and National Prevalence of Overweight and Obesity in Children and Adults during 1980–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Johansson, L.; Brissman, M.; Morinder, G.; Westerståhl, M.; Marcus, C. Reference Values and Secular Trends for Cardiorespiratory Fitness in Children and Adolescents with Obesity. Acta Paediatr. Int. J. Paediatr. 2020, 109, 1665–1671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical Fitness in Childhood and Adolescence: A Powerful Marker of Health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghuveer, G.; Hartz, J.; Lubans, D.R.; Takken, T.; Wiltz, J.L.; Mietus-Snyder, M.; Perak, A.M.; Baker-Smith, C.; Pietris, N.; Edwards, N.M. Cardiorespiratory Fitness in Youth: An Important Marker of Health: A Scientific Statement From the American Heart Association. Circulation 2020, 142, E101–E118. [Google Scholar] [CrossRef]
- Aadland, E.; Kvalheim, O.M.; Rajalahti, T.; Skrede, T.; Resaland, G.K. Aerobic Fitness and Metabolic Health in Children: A Clinical Validation of Directly Measured Maximal Oxygen Consumption versus Performance Measures as Markers of Health. Prev. Med. Rep. 2017, 7, 74–76. [Google Scholar] [CrossRef]
- Högström, G.; Nordström, A.; Nordström, P. High Aerobic Fitness in Late Adolescence Is Associated with a Reduced Risk of Myocardial Infarction Later in Life: A Nationwide Cohort Study in Men. Eur. Heart J. 2014, 35, 3133–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin-Rincon, M.; Calbet, J.A.L. Progress Update and Challenges on VO2max Testing and Interpretation. Front. Physiol. 2020, 11, 1070. [Google Scholar] [CrossRef]
- Howley, E.T.; Bassett, D.R.; Welch, H.G. Criteria for Maximal Oxygen Uptake: Review and Commentary. Med. Sci. Sports Exerc. 1995, 27, 1292–1301. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | 4–5 | 5–6 | 6–7 | 7–8 | 8–9 | 9–10 | 10–11 |
|---|---|---|---|---|---|---|---|
| VO2max/peak (mLkg−1min−1) | 44.29 ± 7.28 | 44.67 ± 7.20 | 45.04 ± 7.12 | 45.41 ± 7.04 | 45.79 ± 6.96 | 46.16 ± 6.88 | 46.54 ± 6.80 |
| Body mass (kg) | 16.43 ± 3.58 | 19.96 ± 4.16 | 23.50 ± 4.75 | 27.03 ± 5.34 | 30.56 ± 5.93 | 34.09 ± 6.51 | 37.62 ± 7.10 |
| VO2max/peak (Lmin−1) | 0.78 ± 0.14 | 0.93 ± 0.15 | 1.08 ± 0.16 | 1.23 ± 0.17 | 1.38 ± 0.18 | 1.53 ± 0.19 | 1.68 ± 0.20 |
| Body mass (kg) | 16.37 ± 3.01 | 19.68 ± 3.24 | 22.99 ± 3.47 | 26.31 ± 3.71 | 29.62 ± 3.94 | 32.93 ± 4.18 | 36.24 ± 4.41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurov, I.; Demšar, J.; McCurdy, T. A Meta-Analysis of Sampled Maximal Aerobic Capacity Data for Boys Aged 11 Years Old or Less Obtained by Cycle Ergometry. Life 2023, 13, 276. https://doi.org/10.3390/life13020276
Jurov I, Demšar J, McCurdy T. A Meta-Analysis of Sampled Maximal Aerobic Capacity Data for Boys Aged 11 Years Old or Less Obtained by Cycle Ergometry. Life. 2023; 13(2):276. https://doi.org/10.3390/life13020276
Chicago/Turabian StyleJurov, Iva, Jure Demšar, and Thomas McCurdy. 2023. "A Meta-Analysis of Sampled Maximal Aerobic Capacity Data for Boys Aged 11 Years Old or Less Obtained by Cycle Ergometry" Life 13, no. 2: 276. https://doi.org/10.3390/life13020276
APA StyleJurov, I., Demšar, J., & McCurdy, T. (2023). A Meta-Analysis of Sampled Maximal Aerobic Capacity Data for Boys Aged 11 Years Old or Less Obtained by Cycle Ergometry. Life, 13(2), 276. https://doi.org/10.3390/life13020276