
Endoscopic Vacuum Therapy (EVT) versus Self-Expandable Metal Stent (SEMS) for Anastomotic Leaks after Upper Gastrointestinal Surgery: Systematic Review and Meta-Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Outcomes
2.5. Risk of Bias
2.6. Data Analysis
3. Results
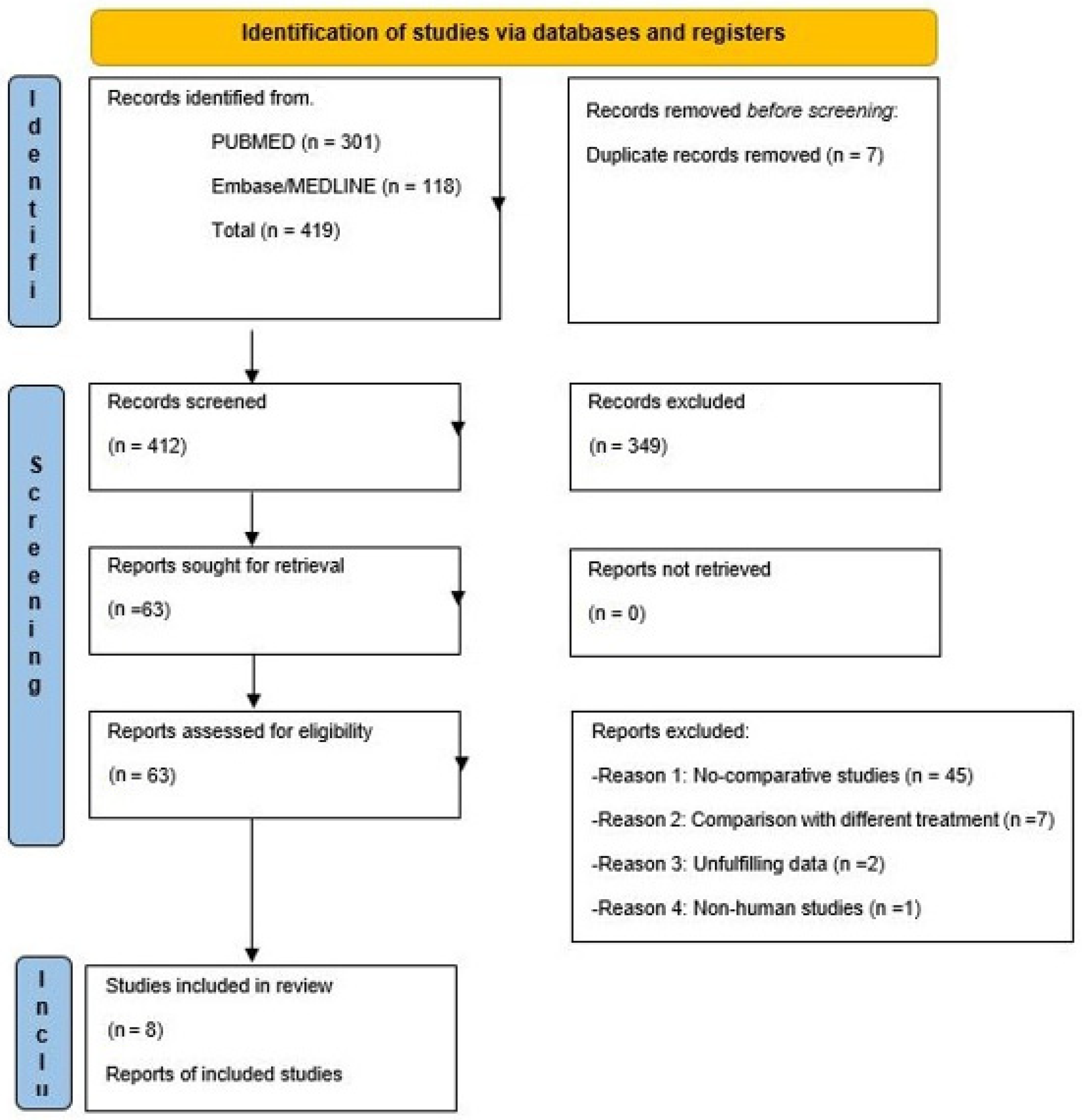
3.1. Study Selection
3.2. Study Assessment
3.3. Studies Description
3.4. Publication Bias
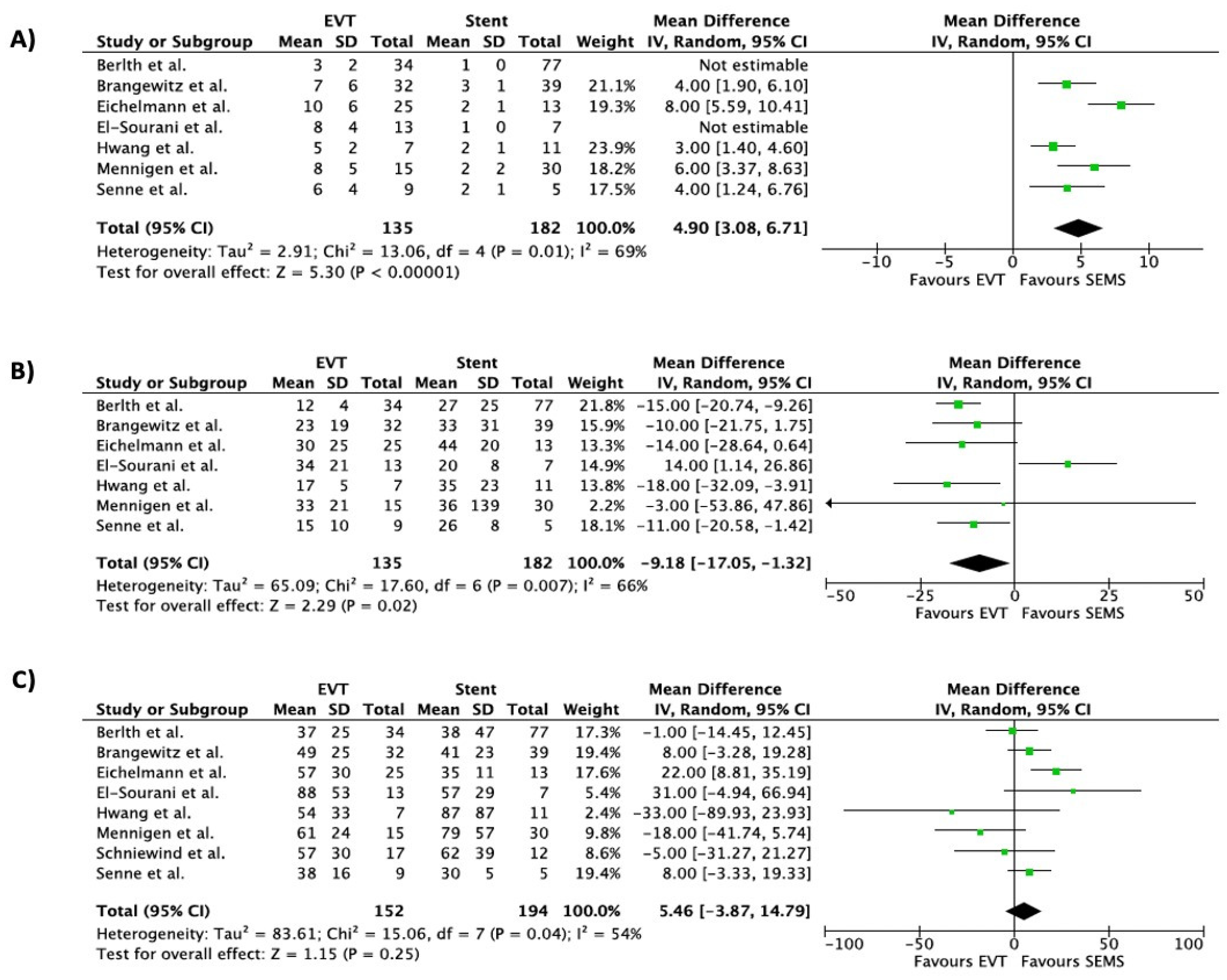
3.5. Overall Outcomes
3.6. Subgroup Analysis Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Busweiler, L.A.; Wijnhoven, B.P.; van Berge Henegouwen, M.I.; Henneman, D.; van Grieken, N.C.; Wouters, M.W.; van Hillegersberg, R.; van Sandick, J.W. Dutch Upper Gastrointestinal Cancer Audit (DUCA) Group. Early outcomes from the Dutch Upper Gastrointestinal Cancer Audit. Br. J. Surg. 2016, 103, 1855–1863. [Google Scholar] [PubMed]
- Li, B.; Xiang, J.; Zhang, Y.; Hu, H.; Sun, Y.; Chen, H. Factors Affecting Hospital Mortality in Patients with Esophagogastric Anastomotic Leak: A Retrospective Study. World J. Surg. 2016, 40, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Hulscher, J.B.; van Sandick, J.W.; de Boer, A.G.; Wijnhoven, B.P.; Tijssen, J.G.; Fockens, P.; Stalmeier, P.F.; ten Kate, F.J.; van Dekken, H.; Obertop, H.; et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N. Engl. J. Med 2002, 347, 1662–1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kähler, G. Anastomotic Leakage after Upper Gastrointestinal Surgery: Endoscopic Treatment. Visc. Med. 2017, 33, 202–206. [Google Scholar] [CrossRef]
- Lambertz, R.; Hölscher, A.H.; Bludau, M.; Leers, J.M.; Gutschow, C.; Schröder, W. Management of tracheo- or bronchoesophageal fstula after Ivor-Lewis esophagectomy. World J. Surg 2016, 40, 1680–1687. [Google Scholar] [CrossRef]
- Talavera-Urquijo, E.; Parise, P.; Carresi, A.; Cossu, A.; Barbieri, L.; Puccetti, F.; Elmore, U.; Rosati, R. Post-esophagectomy tracheobronchoesophageal fistula: Management and results of a tertiary referral center. Updates Surg. 2022; Epub ahead of print. [Google Scholar] [CrossRef]
- Low, D.E.; Kuppusamy, M.K.; Alderson, D.; Cecconello, I.; Chang, A.C.; Darling, G.; Davies, A.; D’Journo, X.B.; Gisbertz, S.S.; Griffin, S.M.; et al. Benchmarking Complications Associated with Esophagectomy. Ann. Surg. 2019, 269, 291–298. [Google Scholar] [CrossRef] [Green Version]
- Van Der Werf, L.R.; Busweiler, L.A.; Van Sandick, J.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P. Reporting National Outcomes After Esophagectomy and Gastrectomy According to the Esophageal Complications Consensus Group (ECCG). Ann. Surg. 2020, 271, 1095–1101. [Google Scholar] [CrossRef]
- Smith, E.A.; Daly, S.C.; Smith, B.; Hinojosa, M.; Nguyen, N.T. The Role of Endoscopic Stent in Management of Postesophagectomy Leaks. Am. Surg. 2020, 86, 1411–1417. [Google Scholar] [CrossRef]
- Mandarino, F.V.; Barchi, A.; Fanti, L.; D’Amico, F.; Azzolini, F.; Esposito, D.; Biamonte, P.; Lauri, G.; Danese, S. Endoscopic vacuum therapy for post-esophagectomy anastomotic dehiscence as rescue treatment: A single center case series. Esophagus 2022, 19, 417–425. [Google Scholar] [CrossRef]
- Dasari, B.V.; Neely, D.; Kennedy, A.; Spence, G.; Rice, P.; Mackle, E.; Epanomeritakis, E. The role of esophageal stents in the management of esophageal anastomotic leaks and benign esophageal perforations. Ann. Surg. 2014, 259, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Mandarino, F.V.; Esposito, D.; Spelta, G.N.E.; Cavestro, G.M.; Rosati, R.; Parise, P.; Gemma, M.F.; Fanti, L. Double layer stent for the treatment of leaks and fistula after upper gastrointestinal oncologic surgery: A retrospective study. Updates Surg. 2022, 74, 1055–1062. [Google Scholar] [CrossRef]
- Weidenhagen, R.; Gruetzner, K.U.; Wiecken, T.; Spelsberg, F.; Jauch, K.W. Endoluminal vacuum therapy for the treatment of anastomotic leakage after anterior rectal resection. Rozhl. Chir. 2008, 87, 397–402. [Google Scholar] [PubMed]
- Zhang, C.C.; Liesenfeld, L.; Klotz, R.; Koschny, R.; Rupp, C.; Schmidt, T.; Diener, M.K.; Müller-Stich, B.P.; Hackert, T.; Sauer, P.; et al. Feasibility, effectiveness, and safety of endoscopic vacuum therapy for intrathoracic anastomotic leakage following transthoracic esophageal resection. BMC Gastroenterol. 2021, 21, 72. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Open Med. 2009, 3, e123–e130. [Google Scholar] [PubMed]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. PROSPERO: An International Prospective Register of Systematic Reviews [Internet]. York: The University of York. Available online: https://www.york.ac.uk/media/crd/PROSPERO_EQUATOR_poster.pdf (accessed on 25 June 2020).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 January 2020).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Salmeri, N.; Villanacci, R.; Ottolina, J.; Bartiromo, L.; Cavoretto, P.; Dolci, C.; Candiani, M. Maternal Arsenic Exposure and Gestational Diabetes: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3094. [Google Scholar] [CrossRef]
- Berlth, F.; Bludau, M.; Plum, P.S.; Herbold, T.; Christ, H.; Alakus, H.; Kleinert, R.; Bruns, C.J.; Hölscher, A.H.; Chon, S.H.H. Self-Expanding Metal Stents versus Endoscopic Vacuum Therapy in Anastomotic Leak Treatment After Oncologic Gastroesophageal Surgery. J. Gastrointest. Surg. 2019, 23, 67–75. [Google Scholar] [CrossRef]
- El-Sourani, N.; Miftode, S.; Bockhorn, M.; Arlt, A.; Meinhardt, C. Endoscopic Management of Anastomotic Leakage after Esophageal Surgery: Ten Year Analysis in a Tertiary University Center. Clin. Endosc. 2022, 55, 58–66. [Google Scholar] [CrossRef]
- Hwang, J.J.; Jeong, Y.S.; Park, Y.S.; Yoon, H.; Shin, C.M.; Kim, N.; Lee, D.H. Comparison of Endoscopic Vacuum Therapy and Endoscopic Stent Implantation With Self-Expandable Metal Stent in Treating Postsurgical Gastroesophageal Leakage. Medicine 2016, 95, e3416. [Google Scholar] [CrossRef]
- Senne, M.; Werner, C.R.; Schempf, U.; Thiel, K.; Königsrainer, A.; Wichmann, D. Comparison of Two Endoscopic Therapeutic Interventions as Primary Treatment for Anastomotic Leakages after Total Gastrectomy. Cancers 2022, 14, 2982. [Google Scholar] [CrossRef] [PubMed]
- Schniewind, B.; Schafmayer, C.; Voehrs, G.; Egberts, J.; von Schoenfels, W.; Rose, T.; Kurdow, R.; Arlt, A.; Ellrichmann, M.; Jürgensen, C.; et al. Endoscopic endoluminal vacuum therapy is superior to other regimens in managing anastomotic leakage after esophagectomy: A comparative retrospective study. Surg Endosc. 2013, 27, 3883–3890. [Google Scholar] [CrossRef] [PubMed]
- Brangewitz, M.; Voigtländer, T.; Helfritz, F.A.; Lankisch, T.O.; Winkler, M.; Klempnauer, J.; Manns, M.P.; Schneider, A.S.; Wedemeyer, J. Endoscopic closure of esophageal intrathoracic leaks: Stent versus endoscopic vacuum-assisted closure, a retrospective analysis. Endoscopy 2013, 45, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Mennigen, R.; Harting, C.; Lindner, K.; Vowinkel, T.; Rijcken, E.; Palmes, D.; Senninger, N.; Laukoetter, M.G. Comparison of Endoscopic Vacuum Therapy versus Stent for Anastomotic Leak After Esophagectomy. J. Gastrointest Surg. 2015, 19, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Eichelmann, A.K.; Ismail, S.; Merten, J.; Slepecka, P.; Palmes, D.; Laukötter, M.G.; Pascher, A.; Mardin, W.A. Economic Burden of Endoscopic Vacuum Therapy Compared to Alternative Therapy Methods in Patients with Anastomotic Leakage After Esophagectomy. J. Gastrointest. Surg. 2021, 25, 2447–2454. [Google Scholar] [CrossRef] [PubMed]
- Baltin, C.; Kron, F.; Urbanski, A.; Zander, T.; Kron, A.; Berlth, F.; Kleinert, R.; Hallek, M.; Hoelscher, A.H.; Chon, S.H. The economic burden of endoscopic treatment for anastomotic leaks following oncological Ivor Lewis esophagectomy. PLoS ONE 2019, 14, e0221406. [Google Scholar] [CrossRef] [Green Version]
- Scognamiglio, P.; Reeh, M.; Karstens, K.; Bellon, E.; Kantowski, M.; Schön, G.; Zapf, A.; Chon, S.H.; Izbicki, J.R.; Tachezy, M. Endoscopic vacuum therapy versus stenting for postoperative esophago-enteric anastomotic leakage: Systematic review and meta-analysis. Endoscopy 2020, 52, 632–642. [Google Scholar] [CrossRef]
- Gutschow, C.A.; Schlag, C.; Vetter, D. Endoscopic vacuum therapy in the upper gastrointestinal tract: When and how to use it. Langenbecks Arch. Surg. 2022, 407, 957–964. [Google Scholar] [CrossRef]
- do Monte Junior, E.S.; de Moura, D.T.H.; Ribeiro, I.B.; Hathorn, K.E.; Farias, G.F.A.; Turiani, C.V.; Medeiros, F.S.; Bernardo, W.M.; de Moura, E.G.H. Endoscopic vacuum therapy versus endoscopic stenting for upper gastrointestinal transmural defects: Systematic review and meta-analysis. Dig. Endosc. 2021, 33, 892–902. [Google Scholar]
- Scognamiglio, P.; Reeh, M.; Melling, N.; Kantowski, M.; Eichelmann, A.-K.; Chon, S.-H.; El-Sourani, N.; Höller, A.; Izbicki, J.R.; Tachezy, M. Management of intra-thoracic anastomotic leakages after esophagectomy: Updated systematic review and meta-analysis of endoscopic vacuum therapy versus stenting. BMC Surg. 2022, 22, 309. [Google Scholar] [CrossRef]
- Jung, D.H.; Huh, C.W.; Min, Y.W.; Park, J.C. Endoscopic vacuum therapy for the management of upper GI leaks and perforations: A multicenter retrospective study of factors associated with treatment failure (with video). Gastrointest. Endosc. 2022, 95, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.F.M.; Hallit, R.; Müller-Dornieden, A.; Calmels, M.; Goere, D.; Chaput, U.; Camus, M.; Gonzalez, J.M.; Barthet, M.; Jacques, J.; et al. Endoscopic internal drainage and low negative-pressure endoscopic vacuum therapy for anastomotic leaks after oncologic upper gastrointestinal surgery. Endoscopy 2022, 54, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Hallit, R.; Calmels, M.; Chaput, U.; Lorenzo, D.; Becq, A.; Camus, M.; Dray, X.; Gonzalez, J.M.; Barthet, M.; Jacques, J.; et al. Endoscopic management of anastomotic leak after esophageal or gastric resection for malignancy: A multicenter experience. Therap. Adv. Gastroenterol. 2021, 14, 17562848211032823. [Google Scholar] [CrossRef] [PubMed]
- Mandarino, F.V.; Barchi, A.; Biamonte, P.; Esposito, D.; Azzolini, F.; Fanti, L.; Danese, S. The prophylactic use of endoscopic vacuum therapy for anastomotic dehiscence after rectal anterior resection: Is it feasible for redo surgery? Tech. Coloproctol. 2022, 26, 319–320. [Google Scholar] [CrossRef]
- Richter, F.; Hendricks, A.; Schniewind, B.; Hampe, J.; Heits, N.; von Schönfels, W.; Reichert, B.; Eberle, K.; Ellrichmann, M.; Baumann, P.; et al. Eso-Sponge® for anastomotic leakage after oesophageal resection or perforation: Outcomes from a national, prospective multicentre registry. BJS Open 2022, 6, zrac030. [Google Scholar] [CrossRef]
- Tachezy, M.; Chon, S.H.; Rieck, I.; Kantowski, M.; Christ, H.; Karstens, K.; Gebauer, F.; Goeser, T.; Rösch, T.; Izbicki, J.R.; et al. Endoscopic vacuum therapy versus stent treatment of esophageal anastomotic leaks (ESOLEAK): Study protocol for a prospective randomized phase 2 trial. Trials 2021, 22, 377. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Publication Year | Country | Study Design | Treatment | Patients (n) | Male, n (%) | Age, Median (Range) | Oncologic Resection n (%) | Neoadjuvant Therapy n (%) | Esophagectomies n (%) | Histology | Resection Rate | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ADK | SCC | Other | R0 | R1 | |||||||||||
| Berlth et al. [21] | 2018 | Germany | Retrospective | 111 | |||||||||||
| EVT | 34 | 29 (85) | 65 (43–84) | 34 (100) | 26 (76.4) | 25 (73.5) | 28 (82.4) | 5 (14.7) | 1 (2.9) | N/A | N/A | ||||
| SEMS | 77 | 63 (82) | 64 (43–88) | 77 (100) | 50 (64.9) | 68 (77.9) | 46 (59.7) | 29 (37.7) | 2 (2.1) | N/A | N/A | ||||
| Brangewitz et al. [26] | 2013 | Germany | Retrospective | 71 | |||||||||||
| EVT | 32 | 28 (88) | 65 (45–84) | 28 (87.5) | 18 (56.2) | 14 (43.7) | N/A | N/A | N/A | N/A | N/A | ||||
| SEMS | 39 | 30 (77) | 62 (32–78) | 29 (74.3) | 6 (15.3) | 27 (69.2) | N/A | N/A | N/A | N/A | N/A | ||||
| El Sourani et al. [22] | 2021 | Germany | Retrospective | 20 | |||||||||||
| EVT | 13 | N/A | N/A | 13 (100) | N/A | 13 (100) | N/A | N/A | N/A | N/A | N/A | ||||
| SEMS | 7 | N/A | N/A | 7 (100) | N/A | 7 (100) | N/A | N/A | N/A | N/A | N/A | ||||
| Hwang et al. [23] | 2016 | Korea | Retrospective | 18 | |||||||||||
| EVT | 7 | 5 (71) | 71.1 (63–78) | 7 (100) | N/A | 5 (71.4) | N/A | N/A | N/A | N/A | N/A | ||||
| SEMS | 11 | 9 (82) | 67.3 (55–81) | 11 (100) | N/A | 4 (36.3) | N/A | N/A | N/A | N/A | N/A | ||||
| Menningen et al. [27] | 2015 | Germany | Retrospective | 45 | |||||||||||
| EVT | 15 | 14 (93) | 65.5 (40–92) | 15 (100) | 11 (73.3) | 15 (100) | 8 (53.3) | 5 (33.3) | 2 (13.3) | N/A | N/A | ||||
| SEMS | 30 | 21 (70) | 56 (42–76) | 28 (93) | 13 (43.3) | 30 (100) | 21 (70.0) | 7 (23.3) | 5 (33.3) | N/A | N/A | ||||
| Schniewind et al. [25] | 2013 | Germany | Retrospective | 35 * | |||||||||||
| EVT | 17 | N/A | N/A | 17 (100) | N/A | 17 (100) | N/A | N/A | N/A | N/A | N/A | ||||
| SEMS | 12 | N/A | N/A | 12 (100) | N/A | 12 (100) | N/A | N/A | N/A | N/A | N/A | ||||
| Senne et al. [24] | 2022 | Germany | Retrospective | 14 | |||||||||||
| EVT | 9 | 5 (56) | 60 (36–79) | 9 (100) | 7 (77.7) | 6 (66.6) | N/A | N/A | N/A | 6 (66.6) | 3 (33.3) | ||||
| SEMS | 5 | 4 (80) | 61 (21–79) | 5 (100) | 3 (60.0) | 4 (80.0) | N/A | N/A | N/A | 5 (100) | 0 (0) | ||||
| Eichelmann et al. [28] | 2021 | Germany | Retrospective | 42 * | |||||||||||
| EVT | 25 | 22 (88) | 60 (42–78) | 25 (100) | 20 (80.0) | 25 (100) | 20 (80) | 4 (16) | 1 (4) | 21 (84) | 3 (12) | ||||
| SEMS | 13 | 10 (77) | 65 (37–88) | 13 (100) | 8 (61.5) | 13 (100) | 10 (77) | 2 (15) | 1 (8) | 11 (85) | 2 (15) | ||||
| Author | Treatment | Patients (n) | Definition of Success | Success, n (%) | Number of Device, Median (Range) | Treatment Duration (Days), Median (Range) | Duration of Hospitalization (Days), Median (Range) | Dislocation, n (%) | Short-Term Complications, n (%) | Time in ICU (Days), Median (Range) | In-Hospital Mortality, n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Berlth et al. [21] | 111 | Endoscopical closure of leak, without signs of persistent dehiscence | |||||||||
| EVT | 34 | 24 (71) | 3 (1–9) | 12 (3–58) | 37 (19–118) | 4 (15) | 0 (0) | 6 (0–60) | 3 (9) | ||
| SEMS | 77 | 49 (64) | 1 (1–3) | 27 (1–152) | 38 (13–296) | 14 (20) | 4 (20) | 9 (0–295) | 11 (14) | ||
| Brangewitz et al. [26] | 71 | Radiological and endoscopic closure of leak, without clinical signs of persistent leakage, no leaks recurrence at follow-up | |||||||||
| EVT | 32 | 27 (84) | 7 (5–28) | 23 (9–86) | 48.5 (21–122) | 5 (16) | 3 (9) | N/A | 5 (16) | ||
| SEMS | 39 | 21 (54) | 3 (2–6) | 33 (9–132) | 41 (2–93) | 6 (15) | 9 (23) | N/A | 11 (28) | ||
| El Sourani et al. [22] | 20 | Complete closure of leak (assessment method not defined) | |||||||||
| EVT | 13 | 12 (92) | 5 (4–18) | 24.5 (8–80) | 74 (9–193) | 0 (0) | 0 | 38 (9–193) | 5 (38) | ||
| SEMS | 7 | 6 (86) | 1 (1–2) | 22 (3–31) | 41 (22–123) | 0 (0) | 1 | 20 (16–57) | 1 (14) | ||
| Hwang et al. [23] | 18 | Complete healing of leak, confirmed by EGD and X-ray | |||||||||
| EVT | 7 | 7 (100) | 4.3 (2–10) | 19.5 (5–21) | 37.1 (13–128) | 0 (0) | 0 | N/A | 0 (0) | ||
| SEMS | 11 | 7 (86) | 1.6 (1–4) | 27 (3–84) | 87.3 (17–366) | 3 (27) | 3 (27) | N/A | 0 (0) | ||
| Menningen et al. [27] | 45 | Healing of anastomosis at endoscopic and X-ray evaluation | |||||||||
| EVT | 15 | 14/15 (93) | 6.5 (1–18) | 26.5 (3–75) | 58 (23–106) | N/A | N/A | N/A | 1 (7) | ||
| SEMS | 30 | 19/30 (63) | 1 (1–6) | 36 (1–560) | 53 (13–195) | N/A | N/A | N/A | 8 (27) | ||
| Schniewind et al. [25] | 35 * | N/A | |||||||||
| EVT | 17 | N/A | N/A | N/A | 57 ± 30 (mean ± SD) | N/A | N/A | 26 ± 19 (mean ± SD) | 2 (12) | ||
| SEMS | 12 | N/A | N/A | N/A | 62 ± 39 (mean ± SD) | N/A | N/A | 38 ± 32 (mean ± SD) | 5 (42) | ||
| Senne et al. [24] | 14 | Endoscopic healing of dehiscence | |||||||||
| EVT | 9 | 8 (89) | 6 ± 3.5 (mean ± SD) | 14.8 ± 9.7 (mean ± SD) | 38 ± 16 (mean ± SD) | 0 | 0 (0) | 4.8 ± 6.8 (mean ± SD) | 0 (0) | ||
| SEMS | 5 | 5 (100) | 2.4 ± 0.5 (mean ± SD) | 26 ± 7.6 (mean ± SD) | 30 ± 5 (mean ± SD) | 1 (20) | 0 (0) | 5 ± 7.6 (mean ± SD) | 0 (0) | ||
| Eichelmann et al. [28] | 42 | Defected cavity lined with surface epithelium at endoscopy and no leakage at X-ray | |||||||||
| EVT | 25 | N/A | 7.4 (1–25) | 23 (3–101) | 47 (14–119) | N/A | N/A | 4 (1–37) | N/A | ||
| SEMS | 13 | N/A | 1.5 (1–3) | 44 (11–68) | 34 (17–56) | N/A | N/A | 2 (1–26) | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mandarino, F.V.; Barchi, A.; D’Amico, F.; Fanti, L.; Azzolini, F.; Viale, E.; Esposito, D.; Rosati, R.; Fiorino, G.; Bemelman, W.A.; et al. Endoscopic Vacuum Therapy (EVT) versus Self-Expandable Metal Stent (SEMS) for Anastomotic Leaks after Upper Gastrointestinal Surgery: Systematic Review and Meta-Analysis. Life 2023, 13, 287. https://doi.org/10.3390/life13020287
Mandarino FV, Barchi A, D’Amico F, Fanti L, Azzolini F, Viale E, Esposito D, Rosati R, Fiorino G, Bemelman WA, et al. Endoscopic Vacuum Therapy (EVT) versus Self-Expandable Metal Stent (SEMS) for Anastomotic Leaks after Upper Gastrointestinal Surgery: Systematic Review and Meta-Analysis. Life. 2023; 13(2):287. https://doi.org/10.3390/life13020287
Chicago/Turabian StyleMandarino, Francesco Vito, Alberto Barchi, Ferdinando D’Amico, Lorella Fanti, Francesco Azzolini, Edi Viale, Dario Esposito, Riccardo Rosati, Gionata Fiorino, Willem Adrianus Bemelman, and et al. 2023. "Endoscopic Vacuum Therapy (EVT) versus Self-Expandable Metal Stent (SEMS) for Anastomotic Leaks after Upper Gastrointestinal Surgery: Systematic Review and Meta-Analysis" Life 13, no. 2: 287. https://doi.org/10.3390/life13020287
APA StyleMandarino, F. V., Barchi, A., D’Amico, F., Fanti, L., Azzolini, F., Viale, E., Esposito, D., Rosati, R., Fiorino, G., Bemelman, W. A., Elmore, U., Barbieri, L., Puccetti, F., Testoni, S. G. G., & Danese, S. (2023). Endoscopic Vacuum Therapy (EVT) versus Self-Expandable Metal Stent (SEMS) for Anastomotic Leaks after Upper Gastrointestinal Surgery: Systematic Review and Meta-Analysis. Life, 13(2), 287. https://doi.org/10.3390/life13020287